
Association between Homocysteine and Vitamin D Levels in Asymptomatic Korean Adults


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Laboratory Measurements
2.3. Other Variables
2.4. Statistical Analyses
3. Results
3.1. Characteristics of the Study Participants
3.2. Correlations between Homocysteine Levels and Clinical Variables
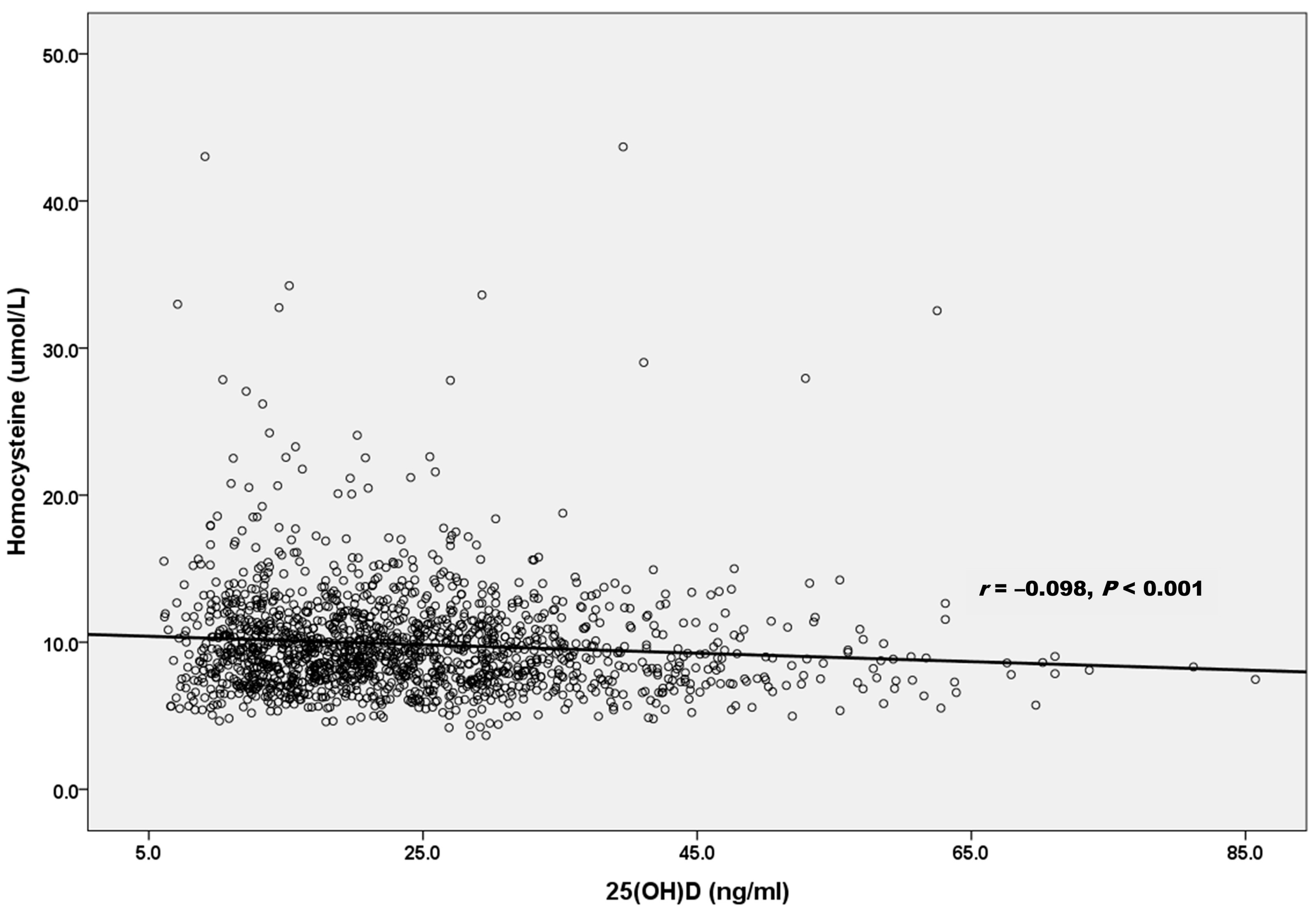
3.3. Associations between Serum Levels of Homocysteine and Vitamin D
3.4. Multiple Linear Regression Analysis of Homocysteine Levels and Clinical Variables
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Crider, K.S.; Zhu, J.H.; Hao, L.; Yang, Q.H.; Yang, T.P.; Gindler, J.; Maneval, D.R.; Quinlivan, E.P.; Li, Z.; Bailey, L.B.; et al. MTHFR 677C->T genotype is associated with folate and homocysteine concentrations in a large, population-based, double-blind trial of folic acid supplementation. Am. J. Clin. Nutr. 2011, 93, 1365–1372. [Google Scholar] [CrossRef] [PubMed]
- Jhee, K.H.; Kruger, W.D. The role of cystathionine beta-synthase in homocysteine metabolism. Antioxid. Redox Signal. 2005, 7, 813–822. [Google Scholar] [CrossRef] [PubMed]
- Gospodarczyk, A.; Marczewski, K.; Gospodarczyk, N.; Widuch, M.; Tkocz, M.; Zalejska-Fiolka, J. Homocysteine and cardiovascular disease—A current review. Wiad. Lek. 2022, 75, 2862–2866. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, P.; Tatarkova, Z.; Sivonova, M.K.; Racay, P.; Lehotsky, J. Homocysteine and Mitochondria in Cardiovascular and Cerebrovascular Systems. Int. J. Mol. Sci. 2020, 21, 7698. [Google Scholar] [CrossRef] [PubMed]
- Lentz, S.R. Mechanisms of homocysteine-induced atherothrombosis. J. Thromb. Haemost. 2005, 3, 1646–1654. [Google Scholar] [CrossRef]
- Wald, D.S.; Law, M.; Morris, J.K. Homocysteine and cardiovascular disease: Evidence on causality from a meta-analysis. BMJ 2002, 325, 1202. [Google Scholar] [CrossRef] [PubMed]
- Den Heijer, M.; Lewington, S.; Clarke, R. Homocysteine, MTHFR and risk of venous thrombosis: A meta-analysis of published epidemiological studies. J. Thromb. Haemost. 2005, 3, 292–299. [Google Scholar] [CrossRef]
- McIlroy, S.P.; Dynan, K.B.; Lawson, J.T.; Patterson, C.C.; Passmore, A.P. Moderately elevated plasma homocysteine, methylenetetrahydrofolate reductase genotype, and risk for stroke, vascular dementia, and Alzheimer disease in Northern Ireland. Stroke 2002, 33, 2351–2356. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Lu, Y.; Deng, Y.; Xu, J.; Zhang, X. Homocysteine level is positively and independently associated with serum creatinine and urea nitrogen levels in old male patients with hypertension. Sci. Rep. 2020, 10, 18050. [Google Scholar] [CrossRef] [PubMed]
- Škovierová, H.; Vidomanová, E.; Mahmood, S.; Sopková, J.; Drgová, A.; Červeňová, T.; Halašová, E.; Lehotský, J. The Molecular and Cellular Effect of Homocysteine Metabolism Imbalance on Human Health. Int. J. Mol. Sci. 2016, 17, 1733. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, W.; Herrmann, M.; Obeid, R. Hyperhomocysteinaemia: A critical review of old and new aspects. Curr. Drug Metab. 2007, 8, 17–31. [Google Scholar] [CrossRef]
- Pusceddu, I.; Herrmann, W.; Kleber, M.E.; Scharnagl, H.; Hoffmann, M.M.; Winklhofer-Roob, B.M.; März, W.; Herrmann, M. Subclinical inflammation, telomere shortening, homocysteine, vitamin B6, and mortality: The Ludwigshafen Risk and Cardiovascular Health Study. Eur. J. Nutr. 2020, 59, 1399–1411. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Norman, P.E.; Powell, J.T. Vitamin D and cardiovascular disease. Circ. Res. 2014, 114, 379–393. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin D status: Measurement, interpretation, and clinical application. Ann. Epidemiol. 2009, 19, 73–78. [Google Scholar] [CrossRef] [PubMed]
- Glueck, C.J.; Jetty, V.; Rothschild, M.; Duhon, G.; Shah, P.; Prince, M.; Lee, K.; Goldenberg, M.; Kumar, A.; Goldenberg, N.; et al. Associations between Serum 25-hydroxyvitamin D and Lipids, Lipoprotein Cholesterols, and Homocysteine. N. Am. J. Med. Sci. 2016, 8, 284–290. [Google Scholar] [CrossRef] [PubMed]
- Mao, X.; Xing, X.; Xu, R.; Gong, Q.; He, Y.; Li, S.; Wang, H.; Liu, C.; Ding, X.; Na, R.; et al. Folic Acid and Vitamins D and B12 Correlate with Homocysteine in Chinese Patients With Type-2 Diabetes Mellitus, Hypertension, or Cardiovascular Disease. Medicine 2016, 95, e2652. [Google Scholar] [CrossRef] [PubMed]
- Verdoia, M.; Nardin, M.; Gioscia, R.; Saghir Afifeh, A.M.; Viglione, F.; Negro, F.; Marcolongo, M.; De Luca, G. Association between vitamin D deficiency and serum Homocysteine levels and its relationship with coronary artery disease. J. Thromb. Thrombolysis 2021, 52, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Pham, T.M.; Ekwaru, J.P.; Mastroeni, S.S.; Mastroeni, M.F.; Loehr, S.A.; Veugelers, P.J. The Effect of Serum 25-Hydroxyvitamin D on Elevated Homocysteine Concentrations in Participants of a Preventive Health Program. PLoS ONE 2016, 11, e0161368. [Google Scholar] [CrossRef] [PubMed]
- Amer, M.; Qayyum, R. The relationship between 25-hydroxyvitamin D and homocysteine in asymptomatic adults. J. Clin. Endocrinol. Metab. 2014, 99, 633–638. [Google Scholar] [CrossRef] [PubMed]
- Al-Bayyari, N.; Hailat, R.; Subih, H.; Alkhalidy, H.; Eaton, A. Vitamin D(3) reduces risk of cardiovascular and liver diseases by lowering homocysteine levels: Double-blinded, randomised, placebo-controlled trial. Br. J. Nutr. 2021, 125, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Kriebitzsch, C.; Verlinden, L.; Eelen, G.; van Schoor, N.M.; Swart, K.; Lips, P.; Meyer, M.B.; Pike, J.W.; Boonen, S.; Carlberg, C.; et al. 1,25-dihydroxyvitamin D3 influences cellular homocysteine levels in murine preosteoblastic MC3T3-E1 cells by direct regulation of cystathionine β-synthase. J. Bone Miner. Res. 2011, 26, 2991–3000. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Wu, P.; Zhou, L.; Shen, Y.; Li, Y.; Song, H. Relationship between increase of serum homocysteine caused by smoking and oxidative damage in elderly patients with cardiovascular disease. Int. J. Clin. Exp. Med. 2015, 8, 4446–4454. [Google Scholar]
- O’Callaghan, P.; Meleady, R.; Fitzgerald, T.; Graham, I. Smoking and plasma homocysteine. Eur. Heart J. 2002, 23, 1580–1586. [Google Scholar] [CrossRef] [PubMed]
- Haj Mouhamed, D.; Ezzaher, A.; Neffati, F.; Douki, W.; Najjar, M.F. Effect of cigarette smoking on plasma homocysteine concentrations. Clin. Chem. Lab. Med. 2011, 49, 479–483. [Google Scholar] [CrossRef] [PubMed]
- Michael Pittilo, R. Cigarette smoking, endothelial injury and cardiovascular disease. Int. J. Exp. Pathol. 2000, 81, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Francis, M.E.; Eggers, P.W.; Hostetter, T.H.; Briggs, J.P. Association between serum homocysteine and markers of impaired kidney function in adults in the United States. Kidney Int. 2004, 66, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Sabanayagam, C.; Shankar, A. Association between plasma homocysteine and microalbuminuria in persons without hypertension, diabetes mellitus, and cardiovascular disease. Clin. Exp. Nephrol. 2011, 15, 92–99. [Google Scholar] [CrossRef]
- van Guldener, C.; Robinson, K. Homocysteine and renal disease. Semin. Thromb. Hemost. 2000, 26, 313–324. [Google Scholar] [CrossRef] [PubMed]
- Cianciolo, G.; De Pascalis, A.; Di Lullo, L.; Ronco, C.; Zannini, C.; La Manna, G. Folic Acid and Homocysteine in Chronic Kidney Disease and Cardiovascular Disease Progression: Which Comes First? Cardiorenal Med. 2017, 7, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zhou, J.; Shao, Z.; Chen, X.; Yu, Z.; Zhao, W. Association between serum uric acid and homocysteine levels among adults in the United States: A cross-sectional study. BMC Cardiovasc. Disord. 2023, 23, 599. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Li, Y.; Hao, M.; Jiang, X.; Wang, J.; Jin, L.; Bao, Z.; Wang, X. Kidney function decline is associated with an accelerated increase in plasma homocysteine in older adults: A longitudinal study. Br. J. Nutr. 2022, 127, 993–999. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Men (n = 895) | Women (n = 480) | p-Value | |
|---|---|---|---|---|
| Age (y) | 53.23 ± 9.59 | 51.48 ± 10.48 | 0.002 | |
| Body mass index (kg/m2) | 25.32 ± 3.32 | 23.20 ± 3.62 | <0.001 | |
| Waist circumference (cm) | 88.49 ± 8.66 | 79.52 ± 9.65 | <0.001 | |
| SBP (mmHg) | 126.84 ± 13.21 | 120.71 ± 13.81 | <0.001 | |
| DBP (mmHg) | 79.29 ± 10.24 | 72.99 ± 9.88 | <0.001 | |
| Hypertension | <0.001 | |||
| Yes | 260 (29.1) | 76 (15.8) | ||
| No | 635 (70.9) | 404 (84.2) | ||
| Diabetes Mellitus | <0.001 | |||
| Yes | 119 (13.3) | 25 (5.2) | ||
| No | 776 (86.7) | 455 (94.8) | ||
| Dyslipidemia | 0.410 | |||
| Yes | 127 (14.2) | 60 (12.5) | ||
| No | 768 (85.8) | 420 (87.5) | ||
| Smoking | <0.001 | |||
| Non-smoker | 253 (28.3) | 459 (95.8) | ||
| Ex-smoker | 263 (29.4) | 14 (2.9) | ||
| Current-smoker | 378 (42.3) | 6 (1.3) | ||
| Alcohol | <0.001 | |||
| No (≤1/week) | 532 (59.5) | 403 (84.1) | ||
| Yes (>1/week) | 362 (40.5) | 76 (15.9) | ||
| Exercise | 0.037 | |||
| No | 167 (18.7) | 121 (25.2) | ||
| 1–3 times/week, irregular | 421 (47.0) | 191 (39.8) | ||
| 1–3 times/week, regular | 130 (14.5) | 75 (15.6) | ||
| ≥4 times/week | 173 (19.3) | 91 (19.0) | ||
| Fasting glucose (mg/dL) | 104.56 ± 26.85 | 95.54 ± 19.40 | <0.001 | |
| HbA1c (%) | 5.68 ± 0.87 | 5.47 ± 0.66 | <0.001 | |
| Triglycerides (mg/dL) | 130.94 ± 77.06 | 89.63 ± 48.84 | <0.001 | |
| HDL-cholesterol (mg/dL) | 51.32 ± 12.21 | 63.76 ± 14.09 | <0.001 | |
| LDL-cholesterol (mg/dL) | 118.09 ± 34.52 | 115.97 ± 29.74 | 0.233 | |
| Creatinine (mg/dL) | 0.89 ± 0.06 | 0.63 ± 0.11 | <0.001 | |
| Uric acid (mg/dL) | 6.15 ± 1.38 | 4.66 ± 1.01 | <0.001 | |
| Hs-CRP (mg/dL) | 0.14 ± 0.37 | 0.09 ± 0.13 | 0.001 | |
| TSH (μIU/mL) | 2.01 ± 1.36 | 2.45 ± 1.93 | <0.001 | |
| 25(OH)D (ng/mL) | 23.20 ± 10.66 | 25.02 ± 13.23 | 0.009 | |
| Homocysteine (μmol/L) | 10.99 ± 3.89 | 7.95 ± 2.26 | <0.001 |
| Variables | r | p-Value |
|---|---|---|
| Age (y) | 0.077 | 0.004 |
| Body mass index (kg/m2) | 0.110 | <0.001 |
| Waist circumference (cm) | 0.163 | <0.001 |
| SBP (mmHg) | 0.104 | <0.001 |
| DBP (mmHg) | 0.121 | <0.001 |
| Fasting glucose (mg/dL) | 0.076 | 0.005 |
| HbA1c (%) | 0.072 | 0.008 |
| Triglycerides (mg/dL) | 0.138 | <0.001 |
| HDL-cholesterol (mg/dL) | −0.142 | <0.001 |
| LDL-cholesterol (mg/dL) | 0.072 | 0.008 |
| Creatinine (mg/dL) | 0.473 | <0.001 |
| Uric acid (mg/dL) | 0.310 | <0.001 |
| Hs-CRP (mg/dL) | 0.088 | 0.001 |
| TSH (μIU/mL) | −0.037 | 0.175 |
| 25(OH)D (ng/mL) | −0.098 | <0.001 |
| β | p-Value | |
|---|---|---|
| Model 1 | −0.027 | 0.001 |
| Model 2 | −0.025 | 0.003 |
| Model 3 | −0.033 | <0.001 |
| Variables | β | p-Value | |
|---|---|---|---|
| Age (y) | 0.025 | 0.016 | |
| Sex (Women) | −0.767 | 0.014 | |
| Body mass index (kg/m2) | −0.038 | 0.438 | |
| Waist circumference(cm) | −0.019 | 0.298 | |
| SBP (mmHg) | −0.001 | 0.930 | |
| DBP (mmHg) | 0.003 | 0.794 | |
| Hypertension | 0.876 | <0.001 | |
| Diabetes Mellitus | 1.480 | <0.001 | |
| Dyslipidemia | 0.053 | 0.846 | |
| Smoking | |||
| Ex-smoker | 0.123 | 0.630 | |
| Current smoker | 0.892 | 0.001 | |
| Alcohol | −0.157 | 0.435 | |
| Exercise | |||
| 1–3 times/week, irregular | 0.044 | 0.879 | |
| 1–3 times/week, regular | −0.349 | 0.127 | |
| ≥4 times/week | −0.541 | 0.051 | |
| Fasting glucose (mg/dL) | −0.002 | 0.694 | |
| HbA1c (%) | −0.223 | 0.206 | |
| Triglycerides (mg/dL) | 0.001 | 0.646 | |
| HDL-cholesterol (mg/dL) | 0.014 | 0.059 | |
| LDL-cholesterol (mg/dL) | 0.009 | 0.002 | |
| Creatinine (mg/dL) | 6.788 | <0.001 | |
| Uric acid (mg/dL) | 0.245 | 0.002 | |
| Hs-CRP (mg/dL) | 0.687 | 0.016 | |
| TSH (μIU/mL) | 0.039 | 0.483 | |
| 25(OH)D (ng/mL) | −0.033 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.-A.; Kang, S.-G.; Song, S.-W.; Kim, S.-H. Association between Homocysteine and Vitamin D Levels in Asymptomatic Korean Adults. Nutrients 2024, 16, 1155. https://doi.org/10.3390/nu16081155
Lee Y-A, Kang S-G, Song S-W, Kim S-H. Association between Homocysteine and Vitamin D Levels in Asymptomatic Korean Adults. Nutrients. 2024; 16(8):1155. https://doi.org/10.3390/nu16081155
Chicago/Turabian StyleLee, Yun-Ah, Sung-Goo Kang, Sang-Wook Song, and Se-Hong Kim. 2024. "Association between Homocysteine and Vitamin D Levels in Asymptomatic Korean Adults" Nutrients 16, no. 8: 1155. https://doi.org/10.3390/nu16081155
APA StyleLee, Y.-A., Kang, S.-G., Song, S.-W., & Kim, S.-H. (2024). Association between Homocysteine and Vitamin D Levels in Asymptomatic Korean Adults. Nutrients, 16(8), 1155. https://doi.org/10.3390/nu16081155