
Vitamin D and Insulin-Dependent Diabetes: A Systematic Review of Clinical Trials

 ,
,
Abstract
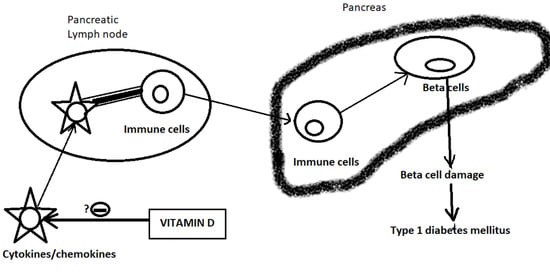
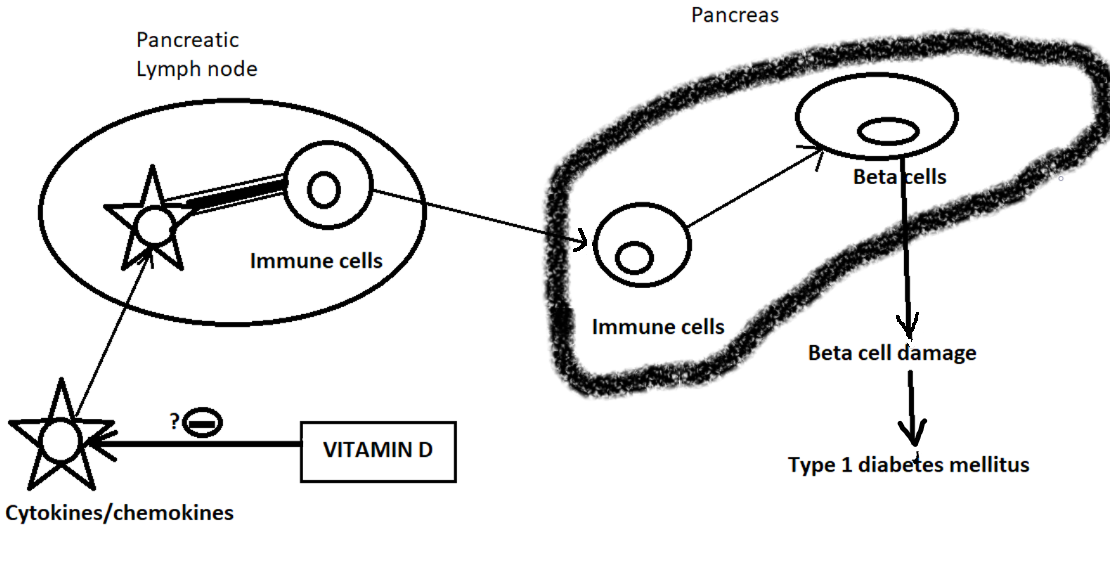
1. Introduction
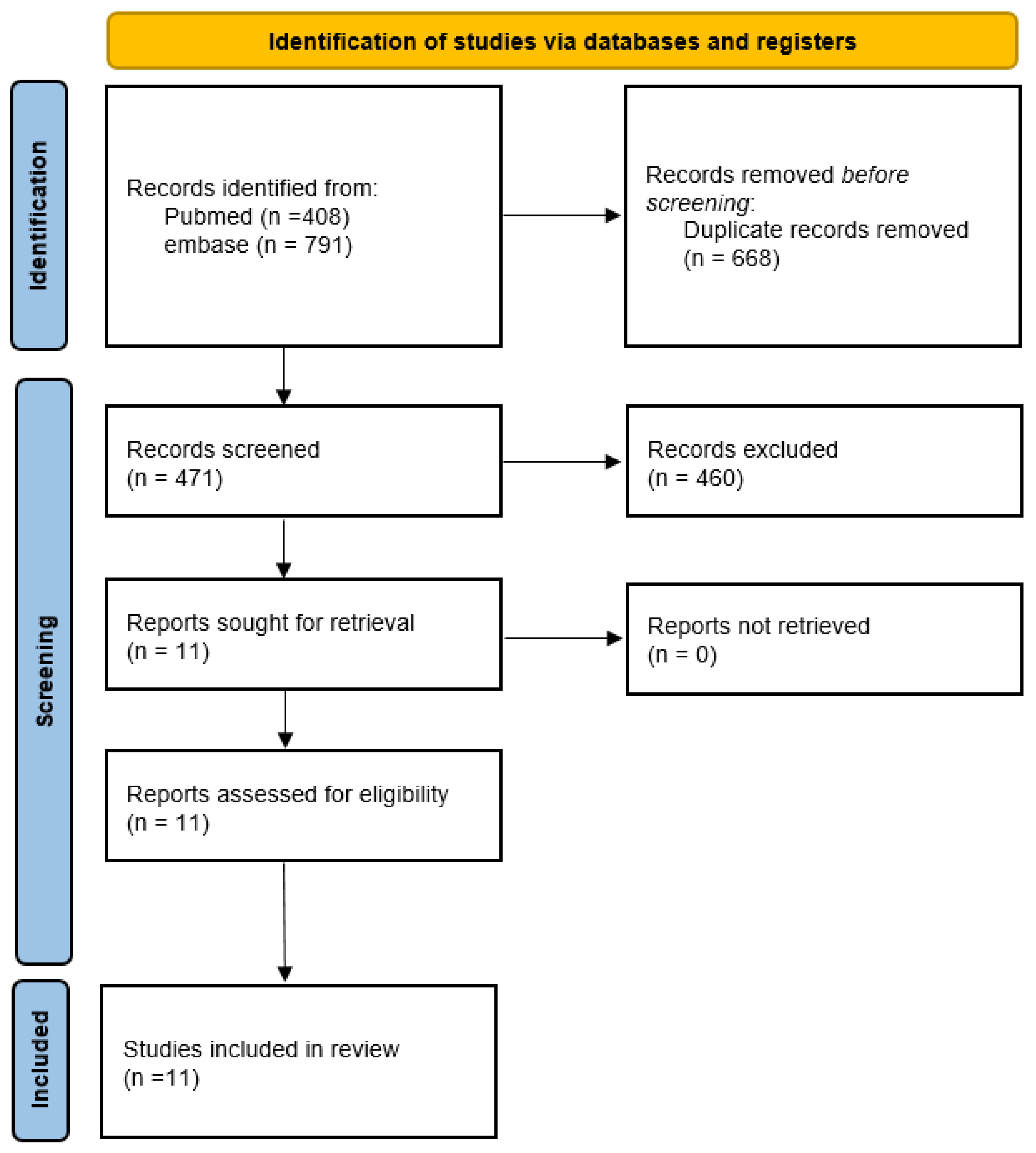
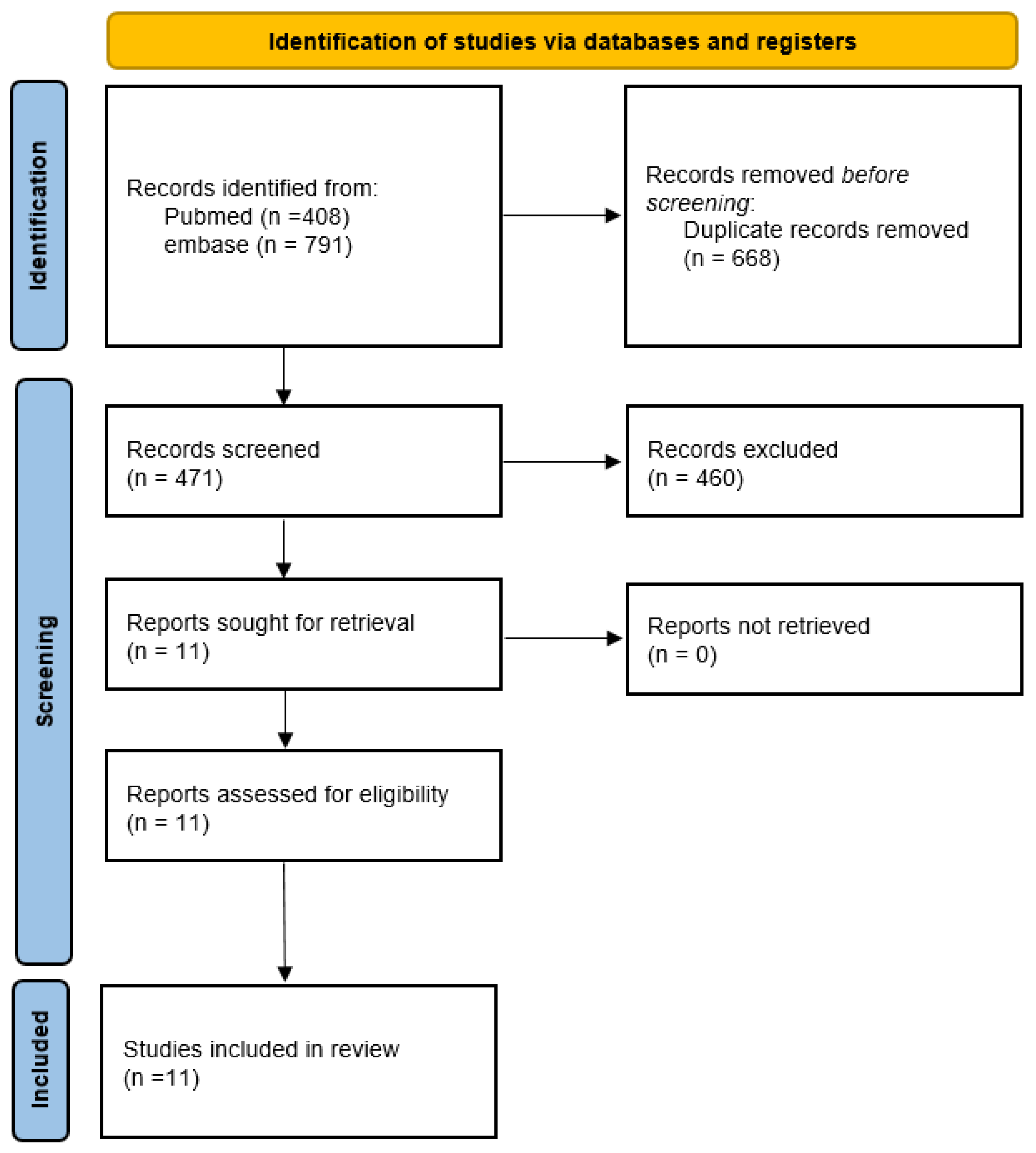
2. Methods
2.1. Search Strategy
2.2. Data Collection
3. Results
Types of Intervention
4. Discussion
5. Conclusions and Suggestions for Future Research
Author Contributions
Funding
Conflicts of Interest
References
- Adams, J.S.; Hewison, M. Unexpected actions of vitamin D: New perspectives on the regulation of innate and adaptive immunity. Nat. Clin. Pract. Endocrinol. Metab. 2008, 4, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Penna, G.; Roncari, A.; Amuchastegui, S.; Daniel, K.C.; Berti, E.; Colonna, M.; Adorini, L. Expression of the inhibitory receptor ILT3 on dendritic cells is dispensable for induction of CD4+Foxp3+ regulatory T cells by 1,25-dihydroxyvitamin D3. Blood 2005, 106, 3490–3497. [Google Scholar] [CrossRef] [PubMed]
- Brehm, J.M.; Celedón, J.C.; Soto-Quiros, M.E.; Avila, L.; Hunninghake, G.M.; Forno, E.; Laskey, D.; Sylvia, J.S.; Hollis, B.W.; Weiss, S.T.; et al. Serum vitamin D levels and markers of severity of childhood asthma in Costa Rica. Am. J. Respir. Crit. Care Med. 2009, 179, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Black, P.N.; Scragg, R. Relationship between serum 25-hydroxyvitamin d and pulmonary function in the third national health and nutrition examination survey. Chest 2005, 128, 3792–3798. [Google Scholar] [CrossRef] [PubMed]
- Baeke, F.; Takiishi, T.; Korf, H.; Gysemans, C.; Mathieu, C. Vitamin D: Modulator of the immune system. Curr. Opin. Pharmacol. 2010, 10, 482–496. [Google Scholar] [CrossRef] [PubMed]
- Chinellato, I.; Piazza, M.; Sandri, M.; Peroni, D.; Piacentini, G.; Boner, A.L. Vitamin D serum levels and markers of asthma control in Italian children. J. Pediatr. 2011, 158, 437–441. [Google Scholar] [CrossRef]
- Devereux, G.; Wilson, A.; Avenell, A.; McNeill, G.; Fraser, W.D. A case-control study of vitamin D status and asthma in adults. Allergy 2010, 65, 666–667. [Google Scholar] [CrossRef]
- Eijkemans, M.; Mommers, M.; Draaisma, J.M.; Thijs, C.; Prins, M.H. Physical activity and asthma: A systematic review and meta-analysis. PLoS ONE 2012, 7, e50775. [Google Scholar] [CrossRef]
- Pitocco, D.; Crinò, A.; Di Stasio, E.; Manfrini, S.; Guglielmi, C.; Spera, S.; Anguissola, G.B.; Visalli, N.; Suraci, C.; Matteoli, M.C.; et al. The effects of calcitriol and nicotinamide on residual pancreatic beta-cell function in patients with recent-onset Type 1 diabetes (IMDIAB XI). Diabet. Med. 2006, 23, 920–923. [Google Scholar] [CrossRef]
- Walter, M.; Kaupper, T.; Adler, K.; Foersch, J.; Bonifacio, E.; Ziegler, A.G. No effect of the 1alpha,25-dihydroxyvitamin D3 on beta-cell residual function and insulin requirement in adults with new-onset type 1 diabetes. Diabetes Care 2010, 33, 1443–1448. [Google Scholar] [CrossRef]
- Bizzarri, C.; Pitocco, D.; Napoli, N.; Di Stasio, E.; Maggi, D.; Manfrini, S.; Suraci, C.; Cavallo, M.G.; Cappa, M.; Ghirlanda, G.; et al. No protective effect of calcitriol on beta-cell function in recent-onset type 1 diabetes: The IMDIAB XIII trial. Diabetes Care 2010, 33, 1962–1963. [Google Scholar] [CrossRef] [PubMed]
- Nitzan, I.; Mimouni, F.B.; Nun, A.B.; Kasirer, Y.; Mendlovic, J. Vitamin D and Asthma: A Systematic Review of Clinical Trials. Curr. Nutr. Rep. 2022, 11, 311–317. [Google Scholar] [CrossRef]
- Gabbay, M.A.; Sato, M.N.; Finazzo, C.; Duarte, A.J.; Dib, S.A. Effect of cholecalciferol as adjunctive therapy with insulin on protective immunologic profile and decline of residual β-cell function in new-onset type 1 diabetes mellitus. Arch. Pediatr. Adolesc. Med. 2012, 166, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Ataie-Jafari, A.; Loke, S.C.; Rahmat, A.B.; Larijani, B.; Abbasi, F.; Leow, M.K.; Yassin, Z. A randomized placebo-controlled trial of alphacalcidol on the preservation of beta cell function in children with recent onset type 1 diabetes. Clin. Nutr. 2013, 32, 911–917. [Google Scholar] [CrossRef]
- Haller, M.J.; Wasserfall, C.H.; Hulme, M.A.; Cintron, M.; Brusko, T.M.; McGrail, K.M.; Wingard, J.R.; Theriaque, D.W.; Shuster, J.J.; Ferguson, R.J.; et al. Autologous umbilical cord blood infusion followed by oral docosahexaenoic acid and vitamin D supplementation for C-peptide preservation in children with Type 1 diabetes. Biol. Blood Marrow Transplant. 2013, 19, 1126–1129. [Google Scholar] [CrossRef] [PubMed]
- Treiber, G.; Prietl, B.; Fröhlich-Reiterer, E.; Lechner, E.; Ribitsch, A.; Fritsch, M.; Rami-Merhar, B.; Steigleder-Schweiger, C.; Graninger, W.; Borkenstein, M.; et al. Cholecalciferol supplementation improves suppressive capacity of regulatory T-cells in young patients with new-onset type 1 diabetes mellitus—A randomized clinical trial. Clin. Immunol. 2015, 161, 217–224. [Google Scholar] [CrossRef]
- Shih, E.M.; Mittelman, S.; Pitukcheewanont, P.; Azen, C.G.; Monzavi, R. Effects of vitamin D repletion on glycemic control and inflammatory cytokines in adolescents with type 1 diabetes. Pediatr. Diabetes 2016, 17, 36–43. [Google Scholar] [CrossRef]
- Sharma, S.; Biswal, N.; Bethou, A.; Rajappa, M.; Kumar, S.; Vinayagam, V. Does Vitamin D Supplementation Improve Glycaemic Control In Children With Type 1 Diabetes Mellitus?—A Randomized Controlled Trial. J. Clin. Diagn. Res. 2017, 11, SC15–SC17. [Google Scholar] [CrossRef]
- Kadhim, K.A.; Nafea, L.T.; Gasim, G.A.; al-Hameed, E.A.; Fawzi, H.A. Assessment of vitamin D therapy effect on inflammatory markers in pediatric patients with type 1 diabetic. Asian J. Pharm. Clin. Res. 2018, 11, 552–554. [Google Scholar] [CrossRef]
- Nwosu, B.U.; Parajuli, S.; Jasmin, G.; Fleshman, J.; Sharma, R.B.; Alonso, L.C.; Lee, A.F.; Barton, B.A. Ergocalciferol in New-onset Type 1 Diabetes: A Randomized Controlled Trial. J. Endocr. Soc. 2021, 6, bvab179. [Google Scholar] [CrossRef]
- Dhaon, P.; Shah, V.N. Type 1 diabetes and osteoporosis: A review of literature. Indian J. Endocrinol. Metab. 2014, 18, 159–165. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Author (Year) | Location (Latitude) | Type | Daily Dose | Control (P/N/D) | Blinding | Ages Range | Age (Median) | Time from Diagnosis (mo) | Enrollment Period | FU (Year) | Sample Size | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Treatment | Control | |||||||||||
| Pitocco (2006) [9] | Rome, Italy (41.9 N) | 1,25 | 0.25 mcg qod | N | 0 | >5 | 13.6 | 1 | * | 1 | 34 | 33 |
| Walter (2010) [10] | Bavaria, Germany (48.8 N) | 1,25 | 0.25 mcg | P | 1 | 18 to 39 | * | 2 | November 2000–November 2006 | 1.5 | 25 | 18 |
| Bizzarri (2010) [11] | Rome, Italy (41.9 N) | 1,25 | 0.25 mcg | P | 1 | 11 to 35 | 18 | 3 | * | 2 | 15 | 12 |
| Gabbay (2012) [13] | San Paulo, Brazil (23.55 S) | D3 | 2000 | P | 1 | 7 to 30 | * | 6 | 10 March 2006–28 October 2010 | 1.5 | 17 | 18 |
| Ataie Jafari (2013) [14] | Teheran, Iran (35.7 N) | 1 alpha | 0.25 to 0.5 mcg | P | 1 | 8 to 15 | 10.7 | 2 | September–December 2010 | 0.5 | 29 | 25 |
| Haller (2013) [15] | Gainesville, FL, USA (29.65 N) | D3 | 2000 | DHA | 0 | 1 to 18 | 7.00 | 3.8 | 22 April 2009–31 August 2010 | 1 | 10 | 5 |
| Treiber (2015) [16] | Graz, Austria (47.4 N) | D3 | 70/kg | P | 1 | >6, 9.5 to 17.5 | 12.5 | 3 | * | 1 | 14 | 15 |
| Shih (2016) [17] | Los Angeles, CA, USA (34.1 N) | D3 | 2857 | P | 0 | 13 to 21 | 16.7 | 12 | October 2012–April 2013 | 1 | 12 (IT) | 13 (DT) |
| Sharma (2017) [18] | Puducherry, India (11.9 N) | D3 | 2000–4000 | Insulin only | 1 | 1 to 18 | 9.3 | 4.4 | August 2014–2015 | 0.5 | 26 | 26 |
| Kadhim (2018) [19] | Bagdad, Iraq (33.3 N) | D3 | 2000 | Insulin only | 0 | 4 to 12 | 8.5 | 12 | April 2015–May 2016 | 0.25 | 25 | 25 |
| Nwosu (2022) [20] | Worcester, MA, USA (42.3 N) | D2 | 7143 then 3571 | P | 1 | 10 to 21 | 13.8 | 3 | 19 October 2017–12 April 2021 | 1 | 18 | 18 |
| Year | Author | 25OHD | HbA1C | Insulin Dose | FCP | Peak-CP | AUC CP | TNF Alpha | IL-4, IL-1β | IL-6 | IL-10 | Chemokine IL10 | IL-12 | CD4/CD8 | CRP | TREG |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2006 | Pitocco [9] | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 2010 | Walter [10] | 0 | 1 | 0 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 2010 | Bizzarri [11] | 0 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 2012 | Gabbay [13] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 1 |
| 2013 | Ataie Jafari [14] | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 2013 | Haller [15] | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 |
| 2015 | Treiber [16] | 0 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 1 |
| 2016 | Shih [17] | 1 | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 0 |
| 2017 | Sharma [18] | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 2018 | Kadhim [19] | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 2022 | Nwosu [20] | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dadon, Y.; Hecht Sagie, L.; Mimouni, F.B.; Arad, I.; Mendlovic, J. Vitamin D and Insulin-Dependent Diabetes: A Systematic Review of Clinical Trials. Nutrients 2024, 16, 1042. https://doi.org/10.3390/nu16071042
Dadon Y, Hecht Sagie L, Mimouni FB, Arad I, Mendlovic J. Vitamin D and Insulin-Dependent Diabetes: A Systematic Review of Clinical Trials. Nutrients. 2024; 16(7):1042. https://doi.org/10.3390/nu16071042
Chicago/Turabian StyleDadon, Yuval, Lior Hecht Sagie, Francis B. Mimouni, Iris Arad, and Joseph Mendlovic. 2024. "Vitamin D and Insulin-Dependent Diabetes: A Systematic Review of Clinical Trials" Nutrients 16, no. 7: 1042. https://doi.org/10.3390/nu16071042
APA StyleDadon, Y., Hecht Sagie, L., Mimouni, F. B., Arad, I., & Mendlovic, J. (2024). Vitamin D and Insulin-Dependent Diabetes: A Systematic Review of Clinical Trials. Nutrients, 16(7), 1042. https://doi.org/10.3390/nu16071042