
Association of Korean Healthy Eating Index and Sleep Duration with Obesity in Korean Adults: Based on the 7th Korea National Health and Nutrition Examination Survey 2016–2018



Abstract
1. Introduction
2. Materials and Methods
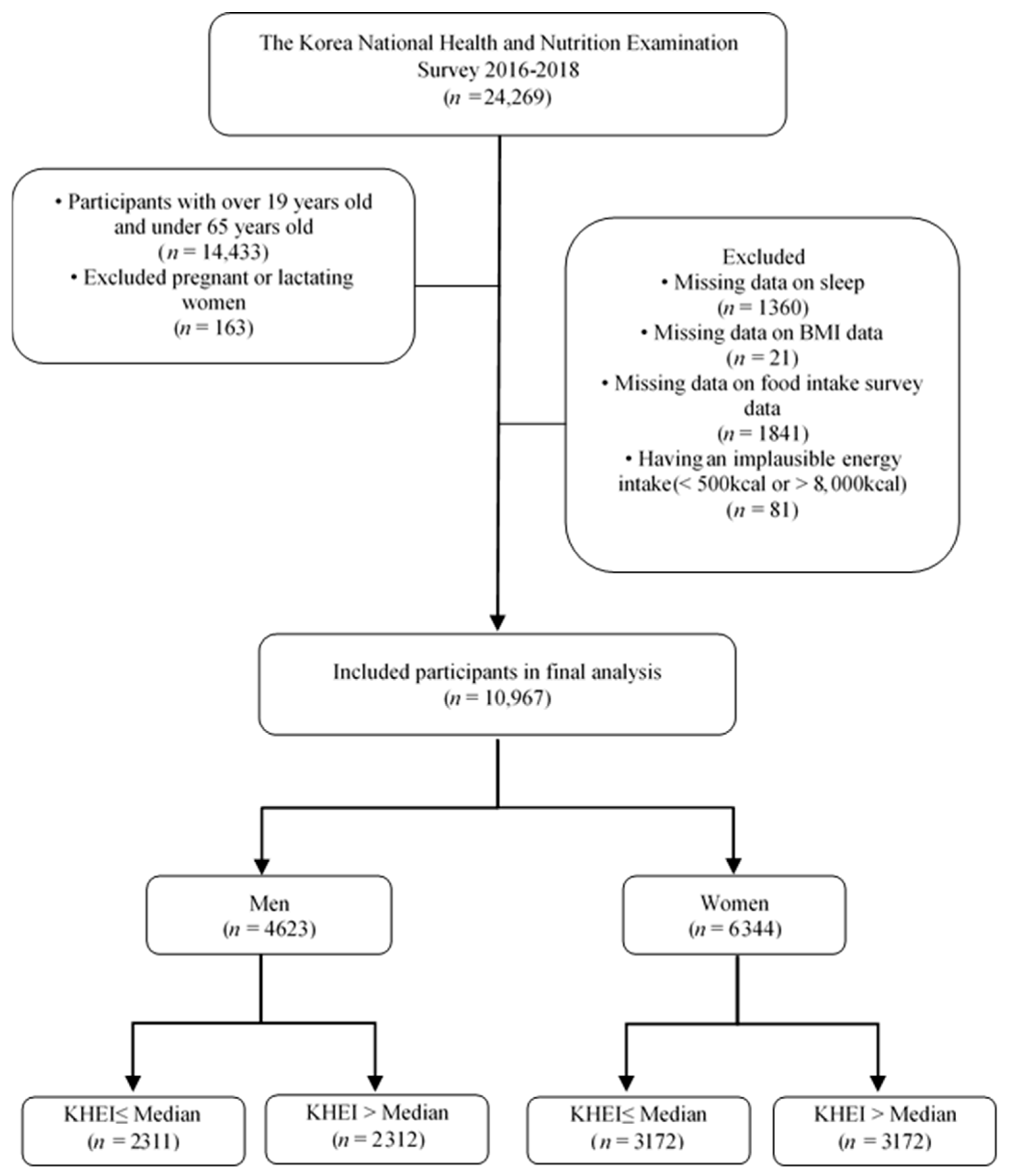
2.1. Participants
2.2. General and Socioeconomic Characteristics
2.3. Anthropometric Measurements
2.4. Assessment of Sleep Duration
2.5. Assessment of Diet Quality
2.5.1. Macronutrient Intake
2.5.2. KHEI
2.6. Statistical Analysis
3. Results
3.1. General Characteristics of the Participants According to BMI Status
3.2. Sleep Duration According to BMI Status
3.3. Diet Quality (KHEI) According to BMI Status
3.4. Macronutrient Intake According to the Median KHEI Score
3.5. Association between Sleep Duration and Obesity According to the Median KHEI Score
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- UN General Assembly. Political Declaration of the Third High-Level Meeting of the General Assembly on the Prevention and Control of Non-Communicable Diseases. 2018. Available online: https://digitallibrary.un.org/record/1648984?ln=en (accessed on 10 August 2023).
- Rahe, C.; Czira, M.E.; Teismann, H.; Berger, K. Associations between poor sleep quality and different measures of obesity. Sleep Med. 2015, 16, 1225–1228. [Google Scholar] [CrossRef]
- Krističević, T.; Štefan, L.; Sporiš, G. The associations between sleep duration and sleep quality with body-mass index in a large sample of young adults. Int. J. Environ. Res. Public Health 2018, 15, 758. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Q.; Arem, H.; Moore, S.C.; Hollenbeck, A.R.; Matthews, C.E. A large prospective investigation of sleep duration, weight change, and obesity in the NIH-AARP Diet and Health Study cohort. Am. J. Epidemiol. 2013, 178, 1600–1610. [Google Scholar] [CrossRef] [PubMed]
- Chaput, J.P.; McNeil, J.; Després, J.P.; Bouchard, C.; Tremblay, A. Short sleep duration as a risk factor for the development of the metabolic syndrome in adults. Prev. Med. 2013, 57, 872–877. [Google Scholar] [CrossRef] [PubMed]
- Guo, X.; Zheng, L.; Wang, J.; Zhang, X.; Zhang, X.; Li, J.; Sun, Y. Epidemiological evidence for the link between sleep duration and high blood pressure: A systematic review and meta-analysis. Sleep Med. 2013, 14, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Knutson, K.L.; Van Cauter, E.; Rathouz, P.J.; Yan, L.L.; Hulley, S.B.; Liu, K.; Lauderdale, D.S. Association between sleep and blood pressure in midlife: The CARDIA sleep study. Arch. Intern. Med. 2009, 169, 1055–1061. [Google Scholar] [CrossRef] [PubMed]
- Iftikhar, I.H.; Donley, M.A.; Mindel, J.; Pleister, A.; Soriano, S.; Magalang, U.J. Sleep duration and metabolic syndrome. An updated dose–risk metaanalysis. Ann. Am. Thorac. Soc. 2015, 12, 1364–1372. [Google Scholar] [CrossRef] [PubMed]
- Taheri, S.; Lin, L.; Austin, D.; Young, T.; Mignot, E. Short sleep duration is associated with reduced leptin, elevated ghrelin, and increased body mass index. PLoS Med. 2004, 1, e62. [Google Scholar] [CrossRef]
- Chaput, J.P.; Després, J.P.; Bouchard, C.; Tremblay, A. Short sleep duration is associated with reduced leptin levels and increased adiposity: Results from the Quebec family study. Obesity 2007, 15, 253–261. [Google Scholar] [CrossRef]
- Gangwisch, J.E.; Heymsfield, S.B.; Boden-Albala, B.; Buijs, R.M.; Kreier, F.; Pickering, T.G.; Rundle, A.G.; Zammit, G.K.; Malaspina, D. Sleep duration as a risk factor for diabetes incidence in a large US sample. Sleep 2007, 30, 1667–1673. [Google Scholar] [CrossRef]
- Wu, Y.; Zhai, L.; Zhang, D. Sleep duration and obesity among adults: A meta-analysis of prospective studies. Sleep Med. 2014, 15, 1456–1462. [Google Scholar] [CrossRef]
- Patel, S.R.; Hu, F.B. Short sleep duration and weight gain: A systematic review. Obesity 2008, 16, 643–653. [Google Scholar] [CrossRef]
- Bixler, E. Sleep and society: An epidemiological perspective. Sleep Med. 2009, 10, S3–S6. [Google Scholar] [CrossRef] [PubMed]
- Magee, L.; Hale, L. Longitudinal associations between sleep duration and subsequent weight gain: A systematic review. Sleep Med. Rev. 2012, 16, 231–241. [Google Scholar] [CrossRef] [PubMed]
- Omisade, A.; Buxton, O.M.; Rusak, B. Impact of acute sleep restriction on cortisol and leptin levels in young women. Physiol. Behav. 2010, 99, 651–656. [Google Scholar] [CrossRef]
- Spiegel, K.; Leproult, R.; L’hermite-Balériaux, M.; Copinschi, G.; Penev, P.D.; Van Cauter, E. Leptin levels are dependent on sleep duration: Relationships with sympathovagal balance, carbohydrate regulation, cortisol, and thyrotropin. J. Clin. Endocrinol. Metab. 2004, 89, 5762–5771. [Google Scholar] [CrossRef]
- Hsieh, S.D.; Muto, T.; Murase, T.; Tsuji, H.; Arase, Y. Association of short sleep duration with obesity, diabetes, fatty liver and behavioral factors in Japanese men. Intern. Med. 2011, 50, 2499–2502. [Google Scholar] [CrossRef][Green Version]
- Park, S.E.; Kim, H.M.; Kim, D.H.; Kim, J.; Cha, B.S.; Kim, D.J. The association between sleep duration and general and abdominal obesity in Koreans: Data from the Korean National Health and Nutrition Examination Survey, 2001 and 2005. Obesity 2009, 17, 767–771. [Google Scholar] [CrossRef]
- Bayon, V.; Leger, D.; Gomez-Merino, D.; Vecchierini, M.F.; Chennaoui, M. Sleep debt and obesity. Ann. Med. 2014, 46, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Kjeldsen, J.S.; Hjorth, M.F.; Andersen, R.; Michaelsen, K.F.; Tetens, I.; Astrup, A.; Chaput, J.P.; Sjödin, A. Short sleep duration and large variability in sleep duration are independently associated with dietary risk factors for obesity in Danish school children. Int. J. Obes. 2014, 38, 32–39. [Google Scholar] [CrossRef]
- Kracht, C.L.; Chaput, J.P.; Martin, C.K.; Champagne, C.M.; Katzmarzyk, P.T.; Staiano, A.E. Associations of sleep with food cravings, diet, and obesity in adolescence. Nutrients 2019, 11, 2899. [Google Scholar] [CrossRef]
- Poggiogalle, E.; Lubrano, C.; Gnessi, L.; Marocco, C.; Di Lazzaro, L.; Polidoro, G.; Luisi, F.; Merola, G.; Mariani, S.; Migliaccio, S. Reduced sleep duration affects body composition, dietary intake and quality of life in obese subjects. Eat Weight Disord. 2016, 21, 501–505. [Google Scholar] [CrossRef]
- Dashti, H.S.; Follis, J.L.; Smith, C.E.; Tanaka, T.; Cade, B.E.; Gottlieb, D.J.; Hruby, A.; Jacques, P.F.; Lamon-Fava, S.; Richardson, K.; et al. Habitual sleep duration is associated with BMI and macronutrient intake and may be modified by CLOCK genetic variants. Am. J. Clin. Nutr. 2015, 101, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Haghighatdoost, F.; Karimi, G.; Esmaillzadeh, A.; Azadbakht, L. Sleep deprivation is associated with lower diet quality indices and higher rate of general and central obesity among young female students in Iran. Nutrition 2012, 28, 1146–1150. [Google Scholar] [CrossRef] [PubMed]
- Hur, S.; Oh, B.; Kim, H.; Kwon, O. Associations of diet quality and sleep quality with obesity. Nutrients 2021, 13, 3181. [Google Scholar] [CrossRef]
- Krebs-Smith, S.M.; Pannucci, T.E.; Subar, A.F.; Kirkpatrick, S.I.; Lerman, J.L.; Tooze, J.A.; Wilson, M.M.; Reedy, J. Update of the healthy eating index: HEI-2015. J. Acad. Nutr. Diet. 2018, 118, 1591–1602. [Google Scholar] [CrossRef] [PubMed]
- Yun, S.; Park, S.; Yook, S.M.; Kim, K.; Shim, J.E.; Hwang, J.Y.; Oh, K. Development of the Korean healthy eating index for adults, based on the Korea National Health and Nutrition Examination Survey. Nutr. Res. Pract. 2022, 16, 233–247. [Google Scholar] [CrossRef]
- Guo, X.; Warden, B.A.; Paeratakul, S.; Bray, G.A. Healthy eating index and obesity. Eur. J. Clin. Nutr. 2004, 58, 1580–1586. [Google Scholar] [CrossRef]
- Tande, D.L.; Magel, R.; Strand, B.N. Healthy Eating Index and abdominal obesity. Public Health Nutr. 2010, 13, 208–214. [Google Scholar] [CrossRef]
- Jansen, E.C.; Prather, A.; Leung, C.W. Associations between sleep duration and dietary quality: Results from a nationally-representative survey of US adults. Appetite 2020, 153, 104748. [Google Scholar] [CrossRef]
- Stern, J.H.; Grant, A.S.; Thomson, C.A.; Tinker, L.; Hale, L.; Brennan, K.M.; Woods, N.F.; Chen, Z. Short sleep duration is associated with decreased serum leptin, increased energy intake and decreased diet quality in postmenopausal women. Obesity 2014, 22, E55–E61. [Google Scholar] [CrossRef]
- World Health Organization. Regional office for the Western Pacific. The Asia-Pacific Perspective: Redefining Obesity and Its Treatment. Sydney: Health Communications Australia; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Kim, B.Y.; Kang, S.M.; Kang, J.H.; Kang, S.Y.; Kim, K.K.; Kim, K.B.; Kim, B.; Kim, S.J.; Kim, Y.H.; Kim, J.H.; et al. 2020 Korean Society for the Study of Obesity guidelines for the management of obesity in Korea. J. Obes. Metab. Syndr. 2021, 30, 81. [Google Scholar] [CrossRef]
- Kant, A.K.; Graubard, B.I. Association of self-reported sleep duration with eating behaviors of American adults: NHANES 2005–2010. Am. J. Clin. Nutr. 2014, 100, 938–947. [Google Scholar] [CrossRef]
- Xiao, R.S.; Moore Simas, T.A.; Pagoto, S.L.; Person, S.D.; Rosal, M.C.; Waring, M.E. Sleep duration and diet quality among women within 5 years of childbirth in the United States: A cross-sectional study. Matern. Child Health J. 2016, 20, 1869–1877. [Google Scholar] [CrossRef]
- Han, D.H.; Kim, M.S.; Kim, S.; Yoo, J.W.; Shen, J.J. Sleep time and duration are associated with periodontitis in a representative sample of Koreans. J. Periodontol. 2022, 93, 210–219. [Google Scholar] [CrossRef]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Katz, E.S.; Kheirandish-Gozal, L.; et al. National Sleep Foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2015, 1, 40–43. [Google Scholar] [CrossRef]
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea national health and nutrition examination survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Gao, S.K.; Beresford, S.A.; Frank, L.L.; Schreiner, P.J.; Burke, G.L.; Fitzpatrick, A.L. Modifications to the Healthy Eating Index and its ability to predict obesity: The Multi-Ethnic Study of Atherosclerosis. Am. J. Clin. Nutr. 2008, 88, 64–69. [Google Scholar] [CrossRef] [PubMed]
- González-Treviño, I.M.; Arrona-Palacios, A.; Núñez-Rocha, G.M.; Jansen, E.C. Association between self-reported sleep duration and dietary quality in Mexican school-aged children. Appetite 2022, 178, 106177. [Google Scholar] [CrossRef] [PubMed]
- Dashti, H.S.; Scheer, F.A.; Jacques, P.F.; Lamon-Fava, S.; Ordovás, J.M. Short sleep duration and dietary intake: Epidemiologic evidence, mechanisms, and health implications. Adv. Nutr. 2015, 6, 648–659. [Google Scholar] [CrossRef] [PubMed]
- Doo, M.; Kim, Y. Association between sleep duration and obesity is modified by dietary macronutrients intake in Korean. Obes. Res. Clin. Pract. 2016, 10, 424–431. [Google Scholar] [CrossRef]
- Beebe, D.; Chang, J.J.; Kress, K.; Mattfeldt-Beman, M. Diet quality and sleep quality among day and night shift nurses. J. Nurs. Manag. 2017, 25, 549–557. [Google Scholar] [CrossRef]
- Mossavar-Rahmani, Y.; Weng, J.; Wang, R.; Shaw, P.A.; Jung, M.; Sotres-Alvarez, D.; Castañeda, S.F.; Gallo, L.C.; Gellman, M.D.; Qi, Q.; et al. Actigraphic sleep measures and diet quality in the Hispanic Community Health Study/Study of Latinos Sueño ancillary study. J. Sleep Res. 2017, 26, 739–746. [Google Scholar] [CrossRef]
- Spiegel, K.; Tasali, E.; Penev, P.; Van Cauter, E. Brief communication: Sleep curtailment in healthy young men is associated with decreased leptin levels, elevated ghrelin levels, and increased hunger and appetite. Ann. Intern. Med. 2004, 141, 846–850. [Google Scholar] [CrossRef]
- Singh, M.; Drake, C.L.; Roehrs, T.; Hudgel, D.W.; Roth, T. The association between obesity and short sleep duration: A population-based study. J. Clin. Sleep Med. 2005, 1, 357–363. [Google Scholar] [CrossRef] [PubMed]
- Hasler, G.; Buysse, D.J.; Klaghofer, R.; Gamma, A.; Ajdacic, V.; Eich, D.; Rössler, W.; Angst, J. The association between short sleep duration and obesity in young adults: A 13-year prospective study. Sleep 2004, 27, 661–666. [Google Scholar] [CrossRef] [PubMed]
- Marshall, N.S.; Glozier, N.; Grunstein, R.R. Is sleep duration related to obesity? A critical review of the epidemiological evidence. Sleep Med. Rev. 2008, 12, 289–298. [Google Scholar] [CrossRef] [PubMed]
- Cappuccio, F.P.; Taggart, F.M.; Kandala, N.B.; Currie, A.; Peile, E.; Stranges, S.; Miller, M.A. Meta-analysis of short sleep duration and obesity in children and adults. Sleep 2008, 31, 619–626. [Google Scholar] [CrossRef] [PubMed]
- Zimberg, I.Z.; Dâmaso, A.; Del Re, M.; Carneiro, A.M.; de Sá Souza, H.; de Lira, F.S.; Tufik, S.; de Mello, M.T. Short sleep duration and obesity: Mechanisms and future perspectives. Cell Biochem. Funct. 2012, 30, 524–529. [Google Scholar] [CrossRef] [PubMed]
- Ikonte, C.J.; Mun, J.G.; Reider, C.A.; Grant, R.W.; Mitmesser, S.H. Micronutrient inadequacy in short sleep: Analysis of the NHANES 2005–2016. Nutrients 2019, 11, 2335. [Google Scholar] [CrossRef] [PubMed]
- Grandner, M.A.; Jackson, N.; Gerstner, J.R.; Knutson, K.L. Dietary nutrients associated with short and long sleep duration. Data from a nationally representative sample. Appetite 2013, 64, 71–80. [Google Scholar] [CrossRef] [PubMed]
- St-Onge, M.P.; O’Keeffe, M.; Roberts, A.L.; RoyChoudhury, A.; Laferrère, B. Short sleep duration, glucose dysregulation and hormonal regulation of appetite in men and women. Sleep 2012, 35, 1503–1510. [Google Scholar] [CrossRef] [PubMed]
- Simpson, N.S.; Banks, S.; Dinges, D.F. Sleep restriction is associated with increased morning plasma leptin concentrations, especially in women. Biol. Res. Nurs. 2010, 12, 47–53. [Google Scholar] [CrossRef]
- Cauley, J.A.; Gutai, J.P.; Kuller, L.H.; LeDonne, D.; Powell, J.G. The epidemiology of serum sex hormones in postmenopausal women. Am. J. Epidemiol. 1989, 129, 1120–1131. [Google Scholar] [CrossRef]
- Mezick, E.J.; Wing, R.R.; Mccaffery, J.M. Associations of self-reported and actigraphy-assessed sleep characteristics with body mass index and waist circumference in adults: Moderation by gender. Sleep Med. 2014, 15, 64–70. [Google Scholar] [CrossRef]
- Grandner, M.A.; Schopfer, E.A.; Sands-Lincoln, M.; Jackson, N.; Malhotra, A. Relationship between sleep duration and body mass index depends on age. Obesity 2015, 23, 2491–2498. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Men | Women | p-Value ** | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Total (n = 4623) | BMI < 25 kg/m2 (n = 2608) | BMI ≥ 25 kg/m2 (n = 2015) | p-Value * | Total (n = 6344) | BMI < 25 kg/m2 (n = 4682) | BMI ≥ 25 kg/m2 (n = 1662) | p-Value * | ||
| Age (years) | 41.28 ± 0.24 1 | 41.15 ± 0.31 | 41.43 ± 0.32 | 0.482 | 42.55 ± 0.21 | 41.53 ± 0.24 | 45.66 ± 0.37 | <0.001 | <0.001 |
| Height (cm) | 172.54 ± 0.11 | 172.62 ± 0.14 | 172.43 ± 0.16 | 0.367 | 159.43 ± 0.09 | 159.77 ± 0.10 | 158.39 ± 0.18 | <0.001 | <0.001 |
| Weight (kg) | 73.70 ± 0.19 | 66.66 ± 0.18 | 82.90 ± 0.26 | <0.001 | 58.49 ± 0.15 | 54.55 ± 0.10 | 70.52 ± 0.28 | <0.001 | <0.001 |
| BMI (kg/m2) | 24.72 ± 0.06 | 22.35 ± 0.05 | 27.83 ± 0.07 | <0.001 | 23.02 ± 0.06 | 21.37 ± 0.04 | 28.06 ± 0.08 | <0.001 | <0.001 |
| Education level | |||||||||
| ≤Elementary | 279 (4.24) | 183 (4.90) | 96 (3.37) | 0.011 | 590 (7.29) | 309 (5.18) | 281 (13.74) | <0.001 | <0.001 |
| ≤Middle school | 355 (5.86) | 212 (5.74) | 143 (6.02) | 581 (8.17) | 380 (7.08) | 201 (11.48) | |||
| ≥High school | 1694 (38.63) | 972 (39.87) | 722 (37.01) | 2355 (38.56) | 1709 (37.73) | 646 (41.10) | |||
| ≥College | 2292 (51.28) | 1239 (49.49) | 1053 (53.61) | 2816 (45.98) | 2283 (50.00) | 533 (33.68) | |||
| Marital status | |||||||||
| Married | 3357 (66.18) | 1839 (63.87) | 1518 (69.20) | 0.001 | 5242 (77.10) | 3776 (74.81) | 1466 (84.10) | <0.001 | <0.001 |
| Single | 1266 (33.82) | 769 (36.13) | 497 (30.80) | 1102 (22.90) | 906 (25.19) | 196 (15.90) | |||
| Occupation | |||||||||
| Yes | 3789 (81.12) | 2102 (79.85) | 1687 (82.80) | 0.035 | 3863 (60.00) | 2887 (60.81) | 976 (57.53) | 0.048 | <0.001 |
| No | 820 (18.88) | 500 (20.15) | 320 (17.20) | 2478 (40.00) | 1792 (39.19) | 686 (42.47) | |||
| Household income | |||||||||
| Low | 432 (8.97) | 264 (9.52) | 168 (8.24) | 0.430 | 601 (9.08) | 383 (8.12) | 218 (12.04) | <0.001 | 0.007 |
| Middle-low | 1017 (21.24) | 580 (21.49) | 437 (20.92) | 1553 (23.94) | 1064 (22.12) | 489 (29.53) | |||
| Middle-high | 1457 (31.89) | 794 (31.04) | 663 (32.99) | 1980 (31.57) | 1456 (31.16) | 524 (32.81) | |||
| High | 1712 (37.91) | 967 (37.95) | 745 (37.85) | 2202 (35.40) | 1773 (38.60) | 429 (25.63) | |||
| Drinking | |||||||||
| None | 586 (11.71) | 344 (12.51) | 242 (10.67) | 0.069 | 1642 (23.11) | 1150 (21.91) | 492 (26.77) | 0.005 | <0.001 |
| ≤1 drink/month | 1034 (23.89) | 592 (24.09) | 442 (23.62) | 2281(36.49) | 1697 (36.88) | 584 (35.32) | |||
| 2–4 drinks/month | 1303 (29.30) | 747 (30.14) | 556 (28.20) | 1531 (25.77) | 1180 (26.58) | 351 (23.30) | |||
| 2–3 drinks/week | 1183 (25.33) | 644 (23.94) | 539 (27.13) | 711 (11.65) | 531 (11.80) | 180 (11.17) | |||
| ≥4 drinks/week | 513 (9.77) | 279 (9.31) | 234 (10.38) | 173 (2.98) | 119 (2.83) | 54 (3.44) | |||
| Smoking | |||||||||
| Non-smoker | 1180 (27.79) | 691 (29.10) | 489 (26.07) | 0.095 | 5557 (86.82) | 4123 (87.08) | 1434 (86.00) | 0.602 | <0.001 |
| Past smoker | 1656 (33.78) | 916 (32.63) | 740 (35.28) | 410 (6.60) | 293 (6.52) | 117 (6.83) | |||
| Current smoker | 1781 (38.43) | 998 (38.26) | 783 (38.65) | 368 (6.59) | 260 (6.39) | 108 (7.17) | |||
| Physical activity | |||||||||
| Yes | 2297 (52.76) | 1276 (52.07) | 1021 (53.66) | 0.327 | 2894 (48.43) | 2191 (49.12) | 703 (46.31) | 0.080 | <0.001 |
| No | 2323 (47.24) | 1332 (47.93) | 991 (46.34) | 3444 (51.57) | 2487 (50.88) | 957 (53.69) | |||
| Dietary supplement | |||||||||
| Yes | 2127 (45.05) | 1238 (46.44) | 889 (43.25) | 0.058 | 3494 (53.48) | 2617 (53.69) | 877 (52.81) | 0.596 | <0.001 |
| No | 2496 (54.95) | 1370 (53.56) | 1126 (56.75) | 2850 (46.52) | 2065 (46.31) | 785 (47.19) | |||
| Postmenopausal | |||||||||
| Yes | 2299 (31.62) | 1555 (28.96) | 744 (39.75) | <0.001 | |||||
| No | 4045 (68.38) | 3127 (71.04) | 918 (60.25) | ||||||
| Men | Women | p-Value ** | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Total (n = 4623) | BMI < 25 kg/m2 (n = 2608) | BMI ≥ 25 kg/m2 (n = 2015) | p-Value * | Total (n = 6344) | BMI < 25 kg/m2 (n = 4682) | BMI ≥ 25 kg/m2 (n = 1662) | p-Value * | ||
| Average sleep duration (h/day) | 6.91 ± 0.02 1 | 6.95 ± 0.03 | 6.87 ± 0.03 | 0.070 | 6.99 ± 0.02 | 7.02 ± 0.02 | 6.89 ± 0.04 | 0.003 | 0.012 |
| Sleep duration < 7 h/day | 1898 (41.48) | 1039 (40.50) | 859 (42.77) | 0.175 | 2458 (40.29) | 1758 (39.11) | 700 (43.92) | 0.003 | 0.279 |
| Sleep duration ≥ 7 h/day | 2725 (58.52) | 1569 (59.50) | 1156 (57.23) | 3886 (59.71) | 2924 (60.89) | 962 (56.09) | |||
| Component of KHEI Score | Men | Women | p-Value ** | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Total (n = 4623) | BMI < 25 kg/m2 (n = 2608) | BMI ≥ 25 kg/m2 (n = 2015) | p-Value * | Total (n = 6344) | BMI < 25 kg/m2 (n = 4682) | BMI ≥ 25 kg/m2 (n = 1662) | p-Value * | ||
| Total KHEI score (0–100) | 59.96 ± 0.25 1 | 59.99 ± 0.33 | 59.92 ± 0.34 | 0.871 | 63.30 ± 0.22 | 63.59 ± 0.26 | 62.42 ± 0.39 | 0.009 | <0.001 |
| Adequacy (8) | |||||||||
| Have breakfast (0–10) | 6.46 ± 0.08 | 6.51 ± 0.10 | 6.40 ± 0.10 | 0.423 | 6.77 ± 0.07 | 6.72 ± 0.08 | 6.94 ± 0.12 | 0.100 | 0.001 |
| Mixed grains intake (0–5) | 1.73 ± 0.04 | 1.72 ± 0.05 | 1.73 ± 0.05 | 0.906 | 1.82 ± 0.03 | 1.81 ± 0.04 | 1.87 ± 0.06 | 0.350 | 0.022 |
| Total fruit intake (0–5) | 1.57 ± 0.03 | 1.63 ± 0.05 | 1.49 ± 0.05 | 0.038 | 2.43 ± 0.03 | 2.45 ± 0.04 | 2.36 ± 0.07 | 0.202 | <0.001 |
| Fresh fruit intake (0–5) | 1.78 ± 0.04 | 1.82 ± 0.05 | 1.71 ± 0.06 | 0.127 | 2.64 ± 0.04 | 2.66 ± 0.04 | 2.57 ± 0.07 | 0.206 | <0.001 |
| Total vegetable intake (0–5) | 3.70 ± 0.02 | 3.65 ± 0.03 | 3.77 ± 0.03 | 0.009 | 3.13 ± 0.02 | 3.10 ± 0.03 | 3.20 ± 0.04 | 0.073 | <0.001 |
| Vegetable intake, excluding kimchi and pickled vegetable intake (0–5) | 3.31 ± 0.03 | 3.25 ± 0.04 | 3.38 ± 0.04 | 0.014 | 2.93 ± 0.02 | 2.93 ± 0.03 | 2.93 ± 0.05 | 0.999 | <0.001 |
| Meat/fish/eggs/beans intake (0–5) | 7.58 ± 0.05 | 7.45 ± 0.07 | 7.74 ± 0.07 | 0.002 | 6.96 ± 0.05 | 7.05 ± 0.05 | 6.70 ± 0.10 | 0.002 | <0.001 |
| Milk/milk products intake (0–5) | 3.25 ± 0.08 | 3.30 ± 0.10 | 3.20 ± 0.11 | 0.476 | 3.76 ± 0.07 | 3.93 ± 0.08 | 3.25 ±0.12 | <0.001 | <0.001 |
| Moderation (3) | |||||||||
| Percentage of energy from saturated fatty acid (0–10) | 6.80 ± 0.07 | 6.84 ± 0.10 | 6.74 ± 0.11 | 0.509 | 6.94 ± 0.07 | 6.84 ± 0.07 | 7.22 ± 0.13 | 0.006 | 0.133 |
| Sodium intake (0–10) | 5.42 ± 0.06 | 5.50 ± 0.08 | 5.31 ± 0.09 | 0.096 | 7.61 ± 0.04 | 7.62 ± 0.05 | 7.56 ± 0.09 | 0.519 | <0.001 |
| Percentage of energy from sweets and beverages (0–10) | 9.04 ± 0.04 | 9.03 ± 0.06 | 9.06 ± 0.07 | 0.730 | 9.06 ± 0.04 | 9.05 ± 0.04 | 9.12 ± 0.07 | 0.414 | 0.639 |
| Energy balance (3) | |||||||||
| Percentage of energy from carbohydrate (0–5) | 2.77 ± 0.04 | 2.73 ± 0.05 | 2.83 ± 0.05 | 0.144 | 2.68 ± 0.03 | 2.74 ± 0.03 | 2.51 ± 0.06 | 0.001 | 0.047 |
| Percentage of energy intake from fat (0–5) | 3.55 ± 0.03 | 3.53 ± 0.04 | 3.59 ± 0.05 | 0.396 | 3.50 ± 0.03 | 3.55 ± 0.03 | 3.36 ± 0.06 | 0.004 | 0.215 |
| Energy intake (0–5) | 3.01 ± 0.04 | 3.04 ± 0.05 | 2.96 ± 0.06 | 0.265 | 3.06 ± 0.03 | 3.13 ± 0.04 | 2.85 ± 0.06 | <0.001 | 0.274 |
| KHEI ≤ median (%) 2 | 2311 (52.70) | 1313 (53.04) | 998 (52.25) | 0.621 | 3172 (52.47) | 2273 (51.31) | 899 (56.02) | 0.005 | 0.829 |
| Men | Women | p-Value ** | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Total (n = 4623) | KHEI ≤ Median † (n = 2311) | KHEI > Median (n = 2312) | p-Value * | Total (n = 6344) | KHE I ≤ Median (n = 3172) | KHEI > Median (n = 3172) | p-Value * | ||
| Energy intake (kcal)/day 2 | 2467.66 ± 18.02 1 | 2464.27 ± 28.84 | 2471.44 ± 18.85 | 0.830 | 1735.36 ± 10.77 | 1621.22 ± 16.34 | 1861.36 ± 11.44 | <0.001 | <0.001 |
| Percentage of macronutrient intake (kcal) (%)/day 3 | |||||||||
| Percentage of energy from carbohydrate (%)/day | 61.41± 0.20 | 59.36 ± 0.34 | 63.70 ± 0.21 | <0.001 | 63.29 ± 0.17 | 62.01 ± 0.28 | 64.70 ± 0.19 | <0.001 | <0.001 |
| Percentage of energy from protein (%)/day | 16.05 ± 0.09 | 15.91 ± 0.13 | 16.22 ± 0.11 | 0.070 | 15.07 ± 0.07 | 14.71 ± 0.11 | 15.45 ± 0.09 | <0.001 | <0.001 |
| Percentage of energy from fat (%)/day | 22.53 ± 0.16 | 24.73 ± 0.27 | 20.09 ± 0.16 | <0.001 | 21.65 ± 0.14 | 23.28 ± 0.23 | 19.84 ± 0.14 | <0.001 | <0.001 |
| Macronutrient intake (kcal)/day | |||||||||
| Carbohydrate intake (kcal)/day | 1356.07 ± 9.47 | 1249.59 ± 13.40 | 1474.71 ± 12.09 | <0.001 | 1057.51 ± 6.83 | 940.13 ± 9.10 | 1187.07 ± 8.39 | <0.001 | <0.001 |
| Protein intake (kcal)/day | 362.03 ± 3.17 | 351.51 ± 5.11 | 373.75 ± 3.62 | 0.001 | 252.91 ± 1.95 | 228.41 ± 2.82 | 279.94 ± 2.21 | <0.001 | <0.001 |
| Fat intake (kcal)/day | 532.17 ± 6.29 | 585.10 ± 10.82 | 473.21 ± 5.60 | <0.001 | 375.24 ± 3.76 | 383.49 ± 6.45 | 366.14 ± 3.63 | 0.020 | <0.001 |
| All 1 (n = 10,967) | 19–34 Years 2 (n = 2622) | 35–49 Years 3 (n = 4099) | 50–64 Years 4 (n = 4246) | |||||
|---|---|---|---|---|---|---|---|---|
| ≤Median | >Median | ≤Median | >Median | ≤Median | >Median | ≤Median | >Median | |
| OR (95% CI) * | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | OR (95% CI) | |
| Men | ||||||||
| Unadjusted | 1.024 (0.841–1.246) | 1.183 (0.984–1.423) | 0.820 (0.565–1.189) | 1.107 (0.788–1.555) | 0.926 (0.673–1.273) | 1.335 (0.999–1.784) | 1.318 (0.958–1.813) | 1.124 (0.824–1.531) |
| Model 1 | 1.015 (0.831–1.240) | 1.206 (0.999–1.457) | 0.812 (0.553–1.191) | 1.280 (0.892–1.836) | 0.943 (0.682–1.304) | 1.306 (0.968–1.764) | 1.272 (0.918–1.762) | 1.172 (0.847–1.621) |
| Women | ||||||||
| Unadjusted | 1.349 (1.134–1.605) | 1.087 (0.887–1.331) | 0.791 (0.503–1.245) | 1.346 (0.862–2.102) | 1.553 (1.150–2.095) | 0.860 (0.640–1.156) | 1.405 (1.070–1.846) | 1.007 (0.746–1.361) |
| Model 1 | 1.270 (1.058–1.525) | 1.032 (0.835–1.275) | 0.840 (0.523–1.350) | 1.410 (0.883–2.252) | 1.455 (1.059–2.000) | 0.777 (0.563–1.071) | 1.459 (1.103–1.930) | 0.988 (0.717–1.362) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Namgung, Y.; Jang, W.; Kwon, O.; Kim, H. Association of Korean Healthy Eating Index and Sleep Duration with Obesity in Korean Adults: Based on the 7th Korea National Health and Nutrition Examination Survey 2016–2018. Nutrients 2024, 16, 835. https://doi.org/10.3390/nu16060835
Namgung Y, Jang W, Kwon O, Kim H. Association of Korean Healthy Eating Index and Sleep Duration with Obesity in Korean Adults: Based on the 7th Korea National Health and Nutrition Examination Survey 2016–2018. Nutrients. 2024; 16(6):835. https://doi.org/10.3390/nu16060835
Chicago/Turabian StyleNamgung, Youngmin, Won Jang, Oran Kwon, and Hyesook Kim. 2024. "Association of Korean Healthy Eating Index and Sleep Duration with Obesity in Korean Adults: Based on the 7th Korea National Health and Nutrition Examination Survey 2016–2018" Nutrients 16, no. 6: 835. https://doi.org/10.3390/nu16060835
APA StyleNamgung, Y., Jang, W., Kwon, O., & Kim, H. (2024). Association of Korean Healthy Eating Index and Sleep Duration with Obesity in Korean Adults: Based on the 7th Korea National Health and Nutrition Examination Survey 2016–2018. Nutrients, 16(6), 835. https://doi.org/10.3390/nu16060835