
Vitamin D Status, VDR, and TLR Polymorphisms and Pulmonary Tuberculosis Epidemiology in Kazakhstan

 , , ,
, , ,  and
and
Abstract
1. Introduction
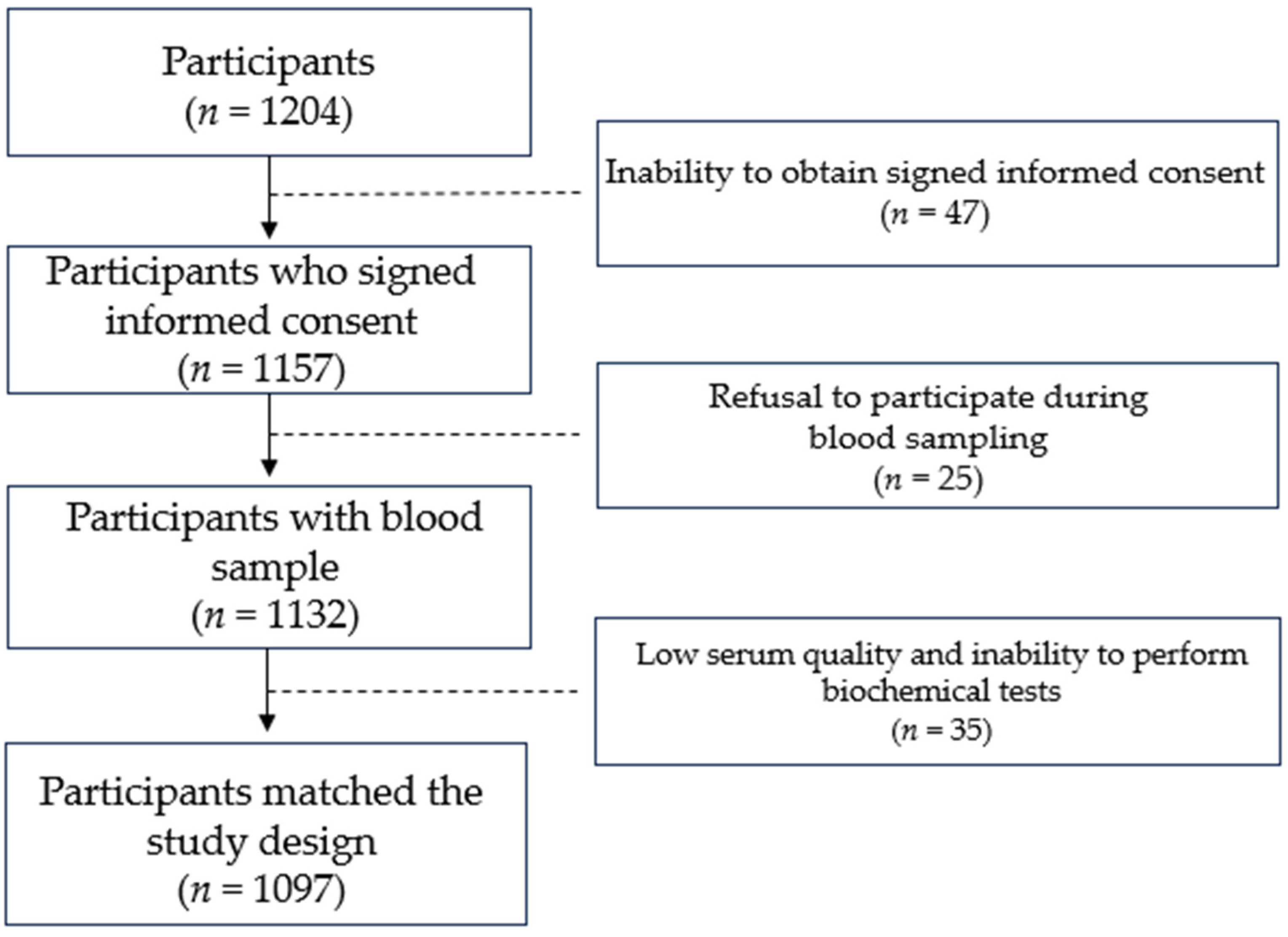
2. Materials and Methods
3. Results
3.1. Epidemiology of Pulmonary TB in Kazakhstan
3.2. Genetics of Pulmonary Tuberculosis in Kazakhstan
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Tuberculosis Report 2018. 2018. Available online: https://www.who.int/publications-detail-redirect/9789241565646 (accessed on 9 January 2024).
- Choi, H.; Yoo, J.E.; Han, K.; Choi, W.; Rhee, S.Y.; Lee, H.; Shin, D.W. Body Mass Index, Diabetes, and Risk of Tuberculosis: A Retrospective Cohort Study. Front. Nutr. 2021, 8, 739766. [Google Scholar] [CrossRef]
- Ockenga, J.; Fuhse, K.; Chatterjee, S.; Malykh, R.; Rippin, H.; Pirlich, M.; Yedilbayev, A.; Wickramasinghe, K.; Barazzoni, R. Tuberculosis and malnutrition: The European perspective. Clin. Nutr. 2023, 42, 486–492. [Google Scholar] [CrossRef]
- Jackson, P.; Muyanja, S.Z.; Siddharthan, T. Health Equity and Respiratory Diseases in Low- and Middle-Income Countries. Clin. Chest Med. 2023, 44, 623–634. [Google Scholar] [CrossRef]
- Greenaway, C.; Castelli, F. Migration Medicine. Infect. Dis. Clin. N. Am. 2019, 33, 265–287. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Factsheet. Tuberculosis. 2017. Available online: https://www.cdc.gov/tb/default.htm (accessed on 7 January 2024).
- Ministry of Healthcare of the Republic of Kazakhstan. Order DCM-214/2020 Dated November 30, 2020 “On Approval of the Rules for Carrying Out Measures to Prevent Tuberculosis”; Ministry of Healthcare of the Republic of Kazakhstan: Astana, Kazakhstan, 2020.
- Ravesloot-Chávez, M.M.; Van Dis, E.; Stanley, S.A. The Innate Immune Response to Mycobacterium tuberculosis Infection. Annu. Rev. Immunol. 2021, 39, 611–637. [Google Scholar] [CrossRef]
- Flynn, J.L.; Chan, J. Immune cell interactions in tuberculosis. Cell 2022, 185, 4682–4702. [Google Scholar] [CrossRef]
- Wani, B.A.; Shehjar, F.; Shah, S.; Koul, A.; Yusuf, A.; Farooq, M.; Mir, M.I.; Singh, R.; Afroze, D. Role of genetic variants of Vitamin D receptor, Toll-like receptor 2 and Toll-like receptor 4 in extrapulmonary tuberculosis. Microb. Pathog. 2021, 156, 104911. [Google Scholar] [CrossRef]
- Bikle, D.D. Vitamin D metabolism, mechanism of action, and clinical applications. Chem. Biol. 2014, 21, 319–329. [Google Scholar] [CrossRef]
- Gallagher, J.C.; Rosen, C.J. Vitamin D: 100 years of discoveries, yet controversy continues. Lancet Diabetes Endocrinol. 2023, 11, 362–374. [Google Scholar] [CrossRef]
- Ismailova, A.; White, J.H. Vitamin D, infections and immunity. Rev. Endocr. Metab. Disord. 2022, 23, 265–277. [Google Scholar] [CrossRef]
- Chen, C.; Liu, Q.; Zhu, L.; Yang, H.; Lu, W. Vitamin D receptor gene polymorphisms on the risk of tuberculosis, a meta-analysis of 29 case-control studies. PLoS ONE 2013, 8, e83843. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Liu, M.; Mijiti, X.; Liu, H.; Wang, Q.; Yin, C.; Anwaierjiang, A.; Xu, M.; Li, M.; Deng, L.; et al. Association of Single-Nucleotide Polymorphisms in the VDR Gene with Tuberculosis and Infection of Beijing Genotype Mycobacterium tuberculosis. Infect. Drug Resist. 2023, 16, 3157–3169. [Google Scholar] [CrossRef]
- Sadykov, M.; Azizan, A.; Kozhamkulov, U.; Akilzhanova, A.; Yerezhepov, D.; Salfinger, M.; Chan, C.K. Association of genetic variations in the vitamin D pathway with susceptibility to tuberculosis in Kazakhstan. Mol. Biol. Rep. 2020, 47, 1659–1666. [Google Scholar] [CrossRef]
- Duan, T.; Du, Y.; Xing, C.; Wang, H.Y.; Wang, R.F. Toll-Like Receptor Signaling and Its Role in Cell-Mediated Immunity. Front. Immunol. 2022, 13, 812774. [Google Scholar] [CrossRef] [PubMed]
- Varshney, D.; Singh, S.; Sinha, E.; Mohanty, K.K.; Kumar, S.; Kumar Barik, S.; Patil, S.A.; Katara, P. Systematic review and meta-analysis of human Toll-like receptors genetic polymorphisms for susceptibility to tuberculosis infection. Cytokine 2022, 152, 155791. [Google Scholar] [CrossRef]
- Sakko, Y.; Madikenova, M.; Kim, A.; Syssoyev, D.; Mussina, K.; Gusmanov, A.; Zhakhina, G.; Yerdessov, S.; Semenova, Y.; Crape, B.L.; et al. Epidemiology of tuberculosis in Kazakhstan: Data from the Unified National Electronic Healthcare System 2014–2019. BMJ Open 2023, 13, e074208. [Google Scholar] [CrossRef]
- Expand New Drug Markets for TB (endTB). Kazakhstan. Available online: https://endtb.org/Kazakhstan (accessed on 15 January 2024).
- Gromova, O.; Doschanova, A.; Lokshin, V.; Tuletova, A.; Grebennikova, G.; Daniyarova, L.; Kaishibayeva, G.; Nurpeissov, T.; Khan, V.; Semenova, Y.; et al. Vitamin D deficiency in Kazakhstan: Cross-Sectional study. J. Steroid Biochem. Mol. Biol. 2020, 199, 105565. [Google Scholar] [CrossRef]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Hassan Murad, M.; Weaver, C.M. Evaluation, Treatment, and Prevention of Vitamin D Deficiency: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef]
- Furin, J.; Cox, H.; Pai, M. Tuberculosis. Lancet 2019, 393, 1642–1656. [Google Scholar] [CrossRef]
- Wikimedia Foundation. Kazakhstan. 2023. Available online: https://en.wikipedia.org/wiki/Kazakhstan (accessed on 17 January 2024).
- Wulan, S.N.; Westerterp, K.R.; Plasqui, G. Ethnic differences in body composition and the associated metabolic profile: A comparative study between Asians and Caucasians. Maturitas 2010, 65, 315–319. [Google Scholar] [CrossRef]
- Biswas, M.; Jinda, P.; Sukasem, C. Pharmacogenomics in Asians: Differences and similarities with other human populations. Expert Opin. Drug Metab. Toxicol. 2023, 19, 27–41. [Google Scholar] [CrossRef]
- Sedgwick, P. Bias in observational study designs: Case-control studies. BMJ 2015, 350, 560. [Google Scholar] [CrossRef]
- Galea, S.; Tracy, M. Participation rates in epidemiologic studies. Ann. Epidemiol. 2007, 17, 643–653. [Google Scholar] [CrossRef]
- Tenny, S.; Kerndt, C.C.; Hoffman, M.R. Case Control Studies; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Statistics of the Regions of the Republic of Kazakhstan. Available online: https://stat.gov.kz/en/region/ (accessed on 17 January 2024).
- Költringer, F.A.; Annerstedt, K.S.; Boccia, D.; Carter, D.J.; Rudgard, W.E. The social determinants of national tuberculosis incidence rates in 116 countries: A longitudinal ecological study between 2005–2015. BMC Public Health 2023, 23, 337. [Google Scholar] [CrossRef]
- Miele, K.; Bamrah Morris, S.; Tepper, N.K. Tuberculosis in Pregnancy. Obstet. Gynecol. 2020, 135, 1444–1453. [Google Scholar] [CrossRef]
- Nordholm, A.C.; Andersen, A.B.; Wejse, C.; Norman, A.; Ekstrøm, C.T.; Andersen, P.H.; Koch, A.; Lillebaek, T. Social determinants of tuberculosis: A nationwide case-control study, Denmark, 1990–2018. Int. J. Epidemiol. 2022, 51, 1446–1456. [Google Scholar] [CrossRef]
- Lu, P.; Zhang, Y.; Liu, Q.; Ding, X.; Kong, W.; Zhu, L.; Lu, W. Association of BMI, diabetes, and risk of tuberculosis: A population-based prospective cohort. Int. J. Infect. Dis. 2021, 109, 168–173. [Google Scholar] [CrossRef]
- Snow, K.J.; Sismanidis, C.; Denholm, J.; Sawyer, S.M.; Graham, S.M. The incidence of tuberculosis among adolescents and young adults: A global estimate. Eur. Respir. J. 2018, 51, 1702352. [Google Scholar] [CrossRef]
- Cui, A.; Zhang, T.; Xiao, P.; Fan, Z.; Wang, H.; Zhuang, Y. Global and regional prevalence of vitamin D deficiency in population-based studies from 2000 to 2022: A pooled analysis of 7.9 million participants. Front. Nutr. 2023, 10, 1070808. [Google Scholar] [CrossRef]
- Autier, P.; Boniol, M.; Pizot, C.; Mullie, P. Vitamin D status and ill health: A systematic review. Lancet Diabetes Endocrinol. 2014, 2, 76–89. [Google Scholar] [CrossRef]
- Costenbader, K.H. Vitamin D and fish oil supplements and risk of autoimmune disease. BMJ 2022, 376, e066452. [Google Scholar] [CrossRef]
- Zhou, A.; Selvanayagam, J.B.; Hyppönen, E. Non-linear Mendelian randomization analyses support a role for vitamin D deficiency in cardiovascular disease risk. Eur. Heart J. 2022, 43, 1731–1739. [Google Scholar] [CrossRef]
- Mailhot, G.; White, J.H. Vitamin D and immunity in infants and children. Nutrients 2020, 12, 1233. [Google Scholar] [CrossRef]
- Jolliffe, D.A.; Camargo, C.A.; Sluyter, J.D.; Martineau, A.R. Vitamin D supplementation to prevent acute respiratory infections: A systematic review and meta-analysis of aggregate data from randomized controlled trials. Lancet Diabetes Endocrinol. 2021, 9, 276–292. [Google Scholar] [CrossRef]
- Pereira, M.; Dantas Damascena, A.; Galvão Azevedo, L.M.; de Almeida Oliveira, T.; da Mota Santana, J. Vitamin D deficiency aggravates COVID-19: Systematic review and meta-analysis. Crit. Rev. Food Sci. Nutr. 2020, 62, 1308–1316. [Google Scholar] [CrossRef] [PubMed]
- Brighenti, S.; Bergman, P.; Martineau, A.R. Vitamin D and tuberculosis: Where next? J. Intern. Med. 2018, 284, 145–162. [Google Scholar] [CrossRef]
- Kafle, S.; Basnet, A.K.; Karki, K.; Thapa Magar, M.; Shrestha, S.; Yadav, R.S. Association of Vitamin D Deficiency with Pulmonary Tuberculosis: A Systematic Review and Meta-Analysis. Cureus 2021, 13, e17883. [Google Scholar] [CrossRef] [PubMed]
- Nugmanova, Z.; Patel, N.; Akhmetova, G.M.; Kurmangalieva, G.S.; Abdumananova, M.K.; Akanov, A.A.; Kovtunenko, N.G.; Mc Nutt, L.A. Relationship between vitamin D and human immunodeficiency virus (HIV) viral load among HIV-infected patients in Kazakhstan. J. Infect. Dev. 2015, 9, 1277–1283. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Algazina, T.; Touir, G.; Pshembayeva, S.; Jetpisbayeva, Z.; Batpenova, G. The role of vitamin D in the development of psoriasis and acne. Georgian Med. News 2019, 290, 96–100. [Google Scholar]
- Markabayeva, A.; Bauer, S.; Pivina, L.; Bjorklund, S.; Chirumbolo, S.; Kerimkulova, A.; Semenova, Y.; Belikhina, T. Increased prevalence of essential hypertension in areas previously exposed to fallout due to nuclear weapons testing at the Semipalatinsk Test Site, Kazakhstan. Environ. Res. 2018, 167, 129–135. [Google Scholar] [CrossRef]
- Semenova, Y.; Pivina, L.; Manatova, A.; Bjorklund, G.; Glushkova, N.; Belikhina, T.; Dauletyarova, M.; Zhunussova, T. Mental distress in the rural Kazakhstani population exposed and non-exposed to radiation from the Semipalatinsk Nuclear Test Site. J. Environ. Radioact. 2019, 203, 39–47. [Google Scholar] [CrossRef]
- Protas, V.V.; Pogossyan, G.P.; Li, K.G.; Zhumina, A.G.; Bisseneva, A.K.; Shaikina, D.N. Plasma 25-Hydroxyvitamin D Level and VDR Gene Single Nucleotide Polymorphism rs2228570 Influence on COVID-19 Susceptibility among the Kazakh Ethnic Group—A Pilot Study. Nutrients 2023, 15, 1781. [Google Scholar] [CrossRef]
- Zhumina, A.G.; Li, K.; Konovalova, A.A.; Li, Y.A.; Ishmuratova, M.Y.; Pogossyan, G.P.; Danilenko, M. Plasma 25-Hydroxyvitamin D Levels and VDR Gene Expression in Peripheral Blood Mononuclear Cells of Leukemia Patients and Healthy Subjects in Central Kazakhstan. Nutrients 2020, 12, 1229. [Google Scholar] [CrossRef]
- Bikle, D.D. Vitamin D and the skin: Physiology and pathophysiology. Rev. Endocr. Metab. Disord. 2012, 13, 3–19. [Google Scholar] [CrossRef]
- Wielders, J.P.; Wijnberg, F.A. Preanalytical stability of 25(OH)-vitamin D3 in human blood or serum at room temperature: Solid as a rock. Clin. Chem. 2009, 55, 1584–1585. [Google Scholar] [CrossRef]
- Abraham, R.A.; Rana, G.; Agrawal, P.K.; Johnston, R.; Sarna, A.; Ramesh, S.; Acharya, R.; Khan, N.; Porwal, A.; Kurundkar, S.B.; et al. The Effects of a Single Freeze-Thaw Cycle on Concentrations of Nutritional, Noncommunicable Disease, and Inflammatory Biomarkers in Serum Samples. J. Lab. Physicians 2021, 13, 6–13. [Google Scholar] [CrossRef]
- Abdel-Wareth, L.; Haq, A.; Turner, A.; Khan, S.; Salem, A.; Mustafa, F.; Hussein, N.; Pallinalakam, F.; Grundy, L.; Patras, G.; et al. Total Vitamin D Assay Comparison of the Roche Diagnostics “Vitamin D Total” Electrochemiluminescence Protein Binding Assay with the Chromsystems HPLC Method in a Population with both D2 and D3 forms of Vitamin D. Nutrients 2013, 5, 971–980. [Google Scholar] [CrossRef] [PubMed]
- Abreu, R.; Giri, P.; Quinn, F. Host-pathogen interaction as a novel target for host-directed therapies in tuberculosis. Front. Immunol. 2020, 11, 1553. [Google Scholar] [CrossRef] [PubMed]
- Yerezhepov, D.; Zhabagin, A.; Askapuli, A.; Rakhimova, S.; Nurkina, Z.; Abilmazhinova, A.; Akhmetova, A.; Molkenov, A.; Kairov, U.; Akilzhanova, A. Genetic Diversity of IFγ, IL1β, TLR2, and TLR8 Loci in Pulmonary Tuberculosis in Kazakhstan. Cent. Asian J. Glob. Health 2014, 3, 181. [Google Scholar] [CrossRef] [PubMed]
- Rai, V.; Abdo, J.; Agrawal, S.; Agrawal, D.K. Vitamin D Receptor Polymorphism and Cancer: An Update. Anticancer Res. Anticancer 2017, 37, 3991–4003. [Google Scholar] [CrossRef]
- Guo, Y.; Zhang, Y.; Tang, X.; Liu, X.; Xu, H. Association between Vitamin D receptor (VDR) gene polymorphisms and hypertensive disorders of pregnancy: A systematic review and meta-analysis. PeerJ 2023, 11, e15181. [Google Scholar] [CrossRef] [PubMed]
- Tizaoui, K.; Kaabachi, W.; Hamzaoui, A.; Hamzaoui, K. Contribution of VDR polymorphisms to type 1 diabetes susceptibility: Systematic review of case-control studies and meta-analysis. J. Steroid Biochem. Mol. Biol. 2014, 143, 240–249. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Shen, M. Associations between vitamin D receptor genetic variants and tuberculosis: A meta-analysis. Innate Immun. 2019, 25, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Ioana, M.; Ferwerda, B.; Plantinga, T.S.; Stappers, M.; Oosting, M.; McCall, M.; Cimpoeru, A.; Burada, F.; Panduru, N.; Sauerwein, R.; et al. Different patterns of Toll-like receptor 2 polymorphisms in populations of various ethnic and geographic origins. Infect. Immun. 2012, 80, 1917–1922. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Zhang, M. Associations between genetic polymorphisms of TLRs and susceptibility to tuberculosis: A meta-analysis. Innate Immun. 2020, 26, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Zhabagin, M.; Sarkytbayeva, A.; Tazhigulova, I.; Yerezhepov, D.; Li, S.; Akilzhanov, R.; Yeralinov, A.; Sabitov, Z.; Akilzhanova, A. Development of the Kazakhstan Y-chromosome haplotype reference database: Analysis of 27 Y-STR in Kazakh population. Int. J. Leg. Med. 2018, 133, 1029–1032. [Google Scholar] [CrossRef]
- Zhabagin, M.; Sabitov, Z.; Tarlykov, P.; Tazhigulova, I.; Junissova, Z.; Yerezhepov, D.; Akilzhanov, R.; Zholdybayeva, E.; Wei, L.H.; Akilzhanova, A.; et al. The medieval Mongolian roots of Y-chromosomal lineages from South Kazakhstan. BMC Genet. 2020, 21, 87. [Google Scholar] [CrossRef]
- Silva, C.A.; Fernandes, D.C.R.O.; Braga, A.C.O.; Cavalcante, G.C.; Sortica, V.A.; Hutz, M.H.; Leal, D.F.V.B.; Fernades, M.R.; Santana-da-Silva, M.N.; Lopes Valente, S.E.; et al. Investigation of genetic susceptibility to mycobacterium tuberculosis (VDR and IL10 genes) in a population with a high level of substructure in the Brazilian amazon region. Int. J. Infect. Dis. 2020, 98, 447–453. [Google Scholar] [CrossRef]
- Jetyata. Available online: https://en.wikipedia.org/wiki/Jetyata (accessed on 17 January 2024).


{kind=link}
| Gene | Name | Reference Number | Context Sequence |
|---|---|---|---|
| VDR | FokI | rs2228570 | GGAAGTGCTGGCCGCCATTGCCTCC[A/G] TCCCTGTAAGAACAGCAAGCAGGCC |
| TaqI | rs731236 | TGGACAGGCGGTCCTGGATGGCCTC[A/G] ATCAGCGCGGCGTCCTGCACCCCAG | |
| BsmI | rs1544410 | GAGCAGAGCCTGAGTATTGGGAATG[T/C] GCAGGCCTGTCTGTGGCCCCAGGAA | |
| ApaI | rs7975232 | AAGGCACAGGAGCTCTCAGCTGGGC[A/C] CCTCACTGCTCAATCCCACCACCCC | |
| TLR2 | A-G | rs1898830 | ATAGTAAAATAAATCCAGAGAAATC[A/G] GAACAGGGGAAATAATAATATAAGA |
| TLR8 | A-G | rs3764880 | AATGAAAAATTAGAACAACAGAAAC[A/G] TGGTAAGCCACTTCTATTTCTTTAG |
| Details | All (n = 1097) | Case (n = 411) | Controls (n = 686) |
|---|---|---|---|
| Age, mean ± SD, years | 38.4 ± 13.8 | 35.0 ± 13.1 | 40.5 ± 13.9 |
| Height, mean ± SD, cm | 166.7 ± 8.5 | 166.6 ± 8.9 | 166.7 ± 8.3 |
| Weight, mean ± SD, kg | 64.0 ± 12.7 | 58.6 ± 10.9 | 67.2 ± 12.5 |
| BMI, mean ± SD, kg/m2 | 22.9 ± 4.1 | 21.0 ± 3.6 | 24.1 ± 4.0 |
| Gender, n (%) | |||
| Male | 527 (48) | 224 (54.5) | 303 (44.2) |
| Female | 570 (52) | 187 (45.5) | 383 (55.8) |
| Residence region, n (%) | |||
| North | 200 (18.2) | 80 (19.5) | 120 (60) |
| South-East | 457 (41.7) | 172 (41.8) | 285 (62.4) |
| South-West | 440 (40.1) | 159 (38.7) | 281 (63.9) |
| Risk factors, n (%) | |||
| Residence | |||
| Urban | 449 (40.9) | 169 (41.1) | 280 (40.8) |
| Rural | 648 (59.1) | 242 (58.9) | 406 (59.2) |
| Employment | |||
| Yes | 511 (46.6) | 121 (29.4) | 390 (56.9) |
| No | 586 (53.4) | 290 (70.6) | 296 (43.1) |
| Alcohol consumption | |||
| Yes | 12 (1.1) | 6 (1.5) | 6 (0.9) |
| No | 1085 (98.9) | 405 (98.5) | 608 (99.1) |
| BMI, kg/m2 | |||
| <24.99 | 769 (70.1) | 352 (85.6) | 417 (60.8) |
| >25.00 | 328 (29.9) | 59 (14.4) | 269 (39.2) |
| Diabetes | |||
| Yes | 35 (3.2) | 31 (7.5) | 4 (0.6) |
| No | 1062 (96.8) | 380 (92.5) | 682 (99.4) |
| Contact with TB | |||
| Yes | 28 (2.5) | 28 (6.8) | 0 |
| No | 1069 (97.5) | 383 (93.2) | 686 (100) |
| Smoking | |||
| Yes | 99 (9.0) | 40 (9.7) | 59 (8.6) |
| No | 998 (91.0) | 371 (92.3) | 682 (91.4) |
| Serum 25-(OH)D, mean ± SD, ng/mL | |||
| Serum 25-(OH)D overall | 20.4 ± 9.7 | 12.9 ± 3.8 | 24.8 ± 3.1 |
| Serum 25-(OH)D by regions | |||
| North | 16.0 ± 9.2 | 9.6 ± 3.4 | 20.3 ± 3.8 |
| South-East | 22.4 ± 10.1 | 14.3 ± 5.6 | 26.6 ± 3.1 |
| South-West | 20.3 ± 9.5 | 13.0 ± 2.1 | 23.4 ± 2.8 |
| Serum 25-(OH)D, ng/mL | |||
| >20.01 | 407 (37.1) | 21 (5.1) | 360 (56.3) |
| ≤20.00 | 690 (62.9) | 390 (94.9) | 326 (43.7) |
| Risk Factors | Case | Control | p-Value * | |
|---|---|---|---|---|
| Alcohol consumption | Yes | 6 | 6 | 0.6 |
| No | 405 | 680 | ||
| Diabetes | Yes | 31 | 4 | <0.001 |
| No | 380 | 682 | ||
| Smoking | Yes | 40 | 59 | 0.6 |
| No | 371 | 682 | ||
| BMI, kg/m2 | <24.99 | 352 | 417 | <0.001 |
| >25.00 | 59 | 269 | ||
| Contact with TB | Yes | 28 | 0 | <0.001 |
| No | 383 | 686 | ||
| Residence | Urban | 169 | 280 | 1.0 |
| Rural | 242 | 406 | ||
| Employment | Yes | 121 | 390 | <0.001 |
| No | 290 | 296 | ||
| Serum 25-(OH)D | >20 ng/mL | 21 | 417 | <0.001 |
| <20 ng/mL | 390 | 269 | ||
| Gene | Polymorphism | Reference Number | Genotype | Amount | % |
|---|---|---|---|---|---|
| VDR | FokI | rs2228570 | G/G | 477 | 0.43 |
| A/G | 488 | 0.44 | |||
| A/A | 132 | 0.12 | |||
| VDR | TaqI | rs731236 | A/A | 631 | 0.58 |
| A/G | 396 | 0.36 | |||
| G/G | 70 | 0.06 | |||
| VDR | BsmI | rs1544410 | C/C | 627 | 0.57 |
| C/T | 410 | 0.37 | |||
| T/T | 60 | 0.05 | |||
| VDR | ApaI | rs7975232 | A/A | 221 | 0.2 |
| C/A | 532 | 0.48 | |||
| C/C | 344 | 0.31 | |||
| TLR2 | G-A | rs1898830 | G/G | 1064 | 0.97 |
| G/A | 33 | 0.03 | |||
| - | - | - | |||
| TLR8 | G-A | rs3764880 | A/A | 175 | 0.16 |
| G/A | 379 | 0.35 | |||
| G/G | 543 | 0.49 |
| Polymorphisms | Geno-Type | Case | Control | C-OR (95% CI) | p-Value | A-OR * (95% CI) | p-Value |
|---|---|---|---|---|---|---|---|
| VDR FokI | G/G | 184 (44.8%) | 293 (42.7%) | 1.00 | 0.6 | 1.00 | 0.3 |
| A/G | 175 (42.6%) | 313 (45.6%) | 1.12 (0.87–1.46) | 1.17 (0.86–1.59) | |||
| A/A | 52 (12.7%) | 80 (11.7%) | 0.97 (0.65–1.43) | 0.82 (0.52–1.30) | |||
| VDR TaqI | A/A | 236 (57.4%) | 395 (57.6%) | 1.00 | 0.7 | 1.00 | 0.7 |
| A/G | 152 (37%) | 244 (35.6%) | 0.96 (0.74–1.24) | 0.97 (0.71–1.31) | |||
| G/G | 23 (5.6%) | 47 (6.8%) | 1.22 (0.72–2.06) | 1.19 (0.64–2.19) | |||
| VDR BsmI | C/C | 236 (57.4%) | 391 (57%) | 1.00 | 0.5 | 1.00 | 0.1 |
| C/T | 157 (38.2%) | 253 (36.9%) | 0.97 (0.75–1.26) | 1.04 (0.77–1.40) | |||
| T/T | 18 (4.4%) | 42 (6.1%) | 1.41 (0.79–2.50) | 1.99 (1.04–3.81) | |||
| VDR ApaI | C/C | 116 (28.2%) | 228 (33.2%) | 1.00 | 0.2 | 1.00 | 0.4 |
| A/C | 204 (49.6%) | 328 (47.8%) | 0.82 (0.62–1.09) | 0.83 (0.60–1.16) | |||
| A/A | 91 (22.1%) | 130 (18.9%) | 0.73 (0.51–1.03) | 0.76 (0.51–1.15) | |||
| TLR8 | G/G | 288 (70.1%) | 428 (62.4%) | 1.00 | 0.01 | 1.00 | 0.02 |
| A/G | 110 (26.8%) | 218 (31.8%) | 1.33 (1.01–1.75) | 1.18 (0.84–1.65) | |||
| A/A | 13 (3.2%) | 40 (5.8%) | 2.07 (1.09–3.94) | 2.56 (1.25–5.24) |
| Polymorphisms | Model | Genotype | Case | Control | C-OR (95% CI) | p-Value | A-OR * (95% CI) | p-Value |
|---|---|---|---|---|---|---|---|---|
| VDR FokI | Dominant | G/G | 184 (44.8%) | 293 (42.7%) | 1.00 | 0.5 | 1.00 | 0.6 |
| A/G-A/A | 227 (55.2%) | 393 (57.3%) | 1.09 (0.85–1.39) | 1.08 (0.81–1.45) | ||||
| Recessive | G/G-A/G | 359 (87.3%) | 606 (88.3%) | 1.00 | 0.6 | 1.00 | 0.2 | |
| A/A | 52 (12.7%) | 80 (11.7%) | 0.91 (0.63–1.32) | 0.76 (0.49–1.16) | ||||
| Overdominant | G/G-A/A | 236 (57.4%) | 373 (54.4%) | 1.00 | 0.3 | 1.00 | 0.2 | |
| A/G | 175 (42.6%) | 313 (45.6%) | 1.13 (0.88–1.45) | 1.23 (0.92–1.64) | ||||
| VDR TaqI | Dominant | A/A | 236 (57.4%) | 395 (57.6%) | 1.00 | 1.0 | 1.00 | 1.0 |
| A/G-G/G | 175 (42.6%) | 291 (42.4%) | 0.99 (0.78–1.27) | 1.00 (0.74–1.33) | ||||
| Recessive | A/A-A/G | 388 (94.4%) | 639 (93.2%) | 1.00 | 0.4 | 1.00 | 0.6 | |
| G/G | 23 (5.6%) | 47 (6.8%) | 1.24 (0.74–2.08) | 1.20 (0.66–2.20) | ||||
| Overdominant | A/A-G/G | 259 (63%) | 442 (64.4%) | 1.00 | 0.6 | 1.00 | 0.7 | |
| A/G | 152 (37%) | 244 (35.6%) | 0.94 (0.73–1.21) | 0.95 (0.71–1.28) | ||||
| VDR BsmI | Dominant | C/C | 236 (57.4%) | 391 (57%) | 1.00 | 0.1 | 1.00 | 0.4 |
| C/T-T/T | 175 (42.6%) | 295 (43%) | 0.79 (0.60–1.03) | 1.13 (0.84–1.51) | ||||
| Recessive | C/C-C/T | 393 (95.6%) | 644 (93.9%) | 1.00 | 0.2 | 1.00 | 0.03 | |
| T/T | 18 (4.4%) | 42 (6.1%) | 0.82 (0.61–1.11) | 1.97 (1.04–3.72) | ||||
| Overdominant | C/C-T/T | 254 (61.8%) | 433 (63.1%) | 1.00 | 0.6 | 1.00 | 0.9 | |
| C/T | 157 (38.2%) | 253 (36.9%) | 0.93 (0.73–1.19) | 0.99 (0.73–1.33) | ||||
| VDR ApaI | Dominant | C/C | 116 (28.2%) | 228 (33.2%) | 1.00 | 0.9 | 1.00 | 0.2 |
| A/C-A/A | 295 (71.8%) | 458 (66.8%) | 1.02 (0.79–1.30) | 0.81 (0.60–1.10) | ||||
| Recessive | C/C-A/C | 320 (77.9%) | 556 (81%) | 1.00 | 0.2 | 1.00 | 0.38 | |
| A/A | 91 (22.1%) | 130 (18.9%) | 1.42 (0.81–2.51) | 0.85 (0.60–1.21) | ||||
| Overdominant | C/C-A/A | 207 (50.4%) | 358 (52.2%) | 1.00 | 0.7 | 1.00 | 0.6 | |
| A/C | 204 (49.6%) | 328 (47.8%) | 0.95 (0.73–1.22) | 0.93 (0.70–1.23) | ||||
| TLR8 | Dominant | G/G | 288 (70.1%) | 428 (62.4%) | 1.00 | 0.001 | 1.00 | 0.1 |
| A/G-A/A | 123 (29.9%) | 258 (37.6%) | 1.41 (1.09–1.83) | 1.34 (0.97–1.84) | ||||
| Recessive | G/G-A/G | 398 (96.8%) | 646 (94.2%) | 1.00 | 0.04 | 1.00 | 0.001 | |
| A/A | 13 (3.2%) | 40 (5.8%) | 1.90 (1.00–3.59) | 2.44 (1.20–4.98) | ||||
| Overdominant | G/G-A/A | 301 (73.2%) | 468 (68.2%) | 1.00 | 0.8 | 1.00 | 0.6 | |
| A/G | 110 (26.8%) | 218 (31.8%) | 1.27 (0.97–1.67) | 1.10 (0.79–1.54) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yerezhepov, D.; Gabdulkayum, A.; Akhmetova, A.; Kozhamkulov, U.A.; Rakhimova, S.E.; Kairov, U.Y.; Zhunussova, G.; Kalendar, R.N.; Akilzhanova, A. Vitamin D Status, VDR, and TLR Polymorphisms and Pulmonary Tuberculosis Epidemiology in Kazakhstan. Nutrients 2024, 16, 558. https://doi.org/10.3390/nu16040558
Yerezhepov D, Gabdulkayum A, Akhmetova A, Kozhamkulov UA, Rakhimova SE, Kairov UY, Zhunussova G, Kalendar RN, Akilzhanova A. Vitamin D Status, VDR, and TLR Polymorphisms and Pulmonary Tuberculosis Epidemiology in Kazakhstan. Nutrients. 2024; 16(4):558. https://doi.org/10.3390/nu16040558
Chicago/Turabian StyleYerezhepov, Dauren, Aidana Gabdulkayum, Ainur Akhmetova, Ulan A. Kozhamkulov, Saule E. Rakhimova, Ulykbek Y. Kairov, Gulnur Zhunussova, Ruslan N. Kalendar, and Ainur Akilzhanova. 2024. "Vitamin D Status, VDR, and TLR Polymorphisms and Pulmonary Tuberculosis Epidemiology in Kazakhstan" Nutrients 16, no. 4: 558. https://doi.org/10.3390/nu16040558
APA StyleYerezhepov, D., Gabdulkayum, A., Akhmetova, A., Kozhamkulov, U. A., Rakhimova, S. E., Kairov, U. Y., Zhunussova, G., Kalendar, R. N., & Akilzhanova, A. (2024). Vitamin D Status, VDR, and TLR Polymorphisms and Pulmonary Tuberculosis Epidemiology in Kazakhstan. Nutrients, 16(4), 558. https://doi.org/10.3390/nu16040558