
Sex-Specific Association between Sodium Intake Estimated by 24-Hour Urinary Sodium Excretion and Nonalcoholic Fatty Liver Disease: The Community-Based Prospective Cohort Study


Abstract
1. Introduction
2. Materials and Methods
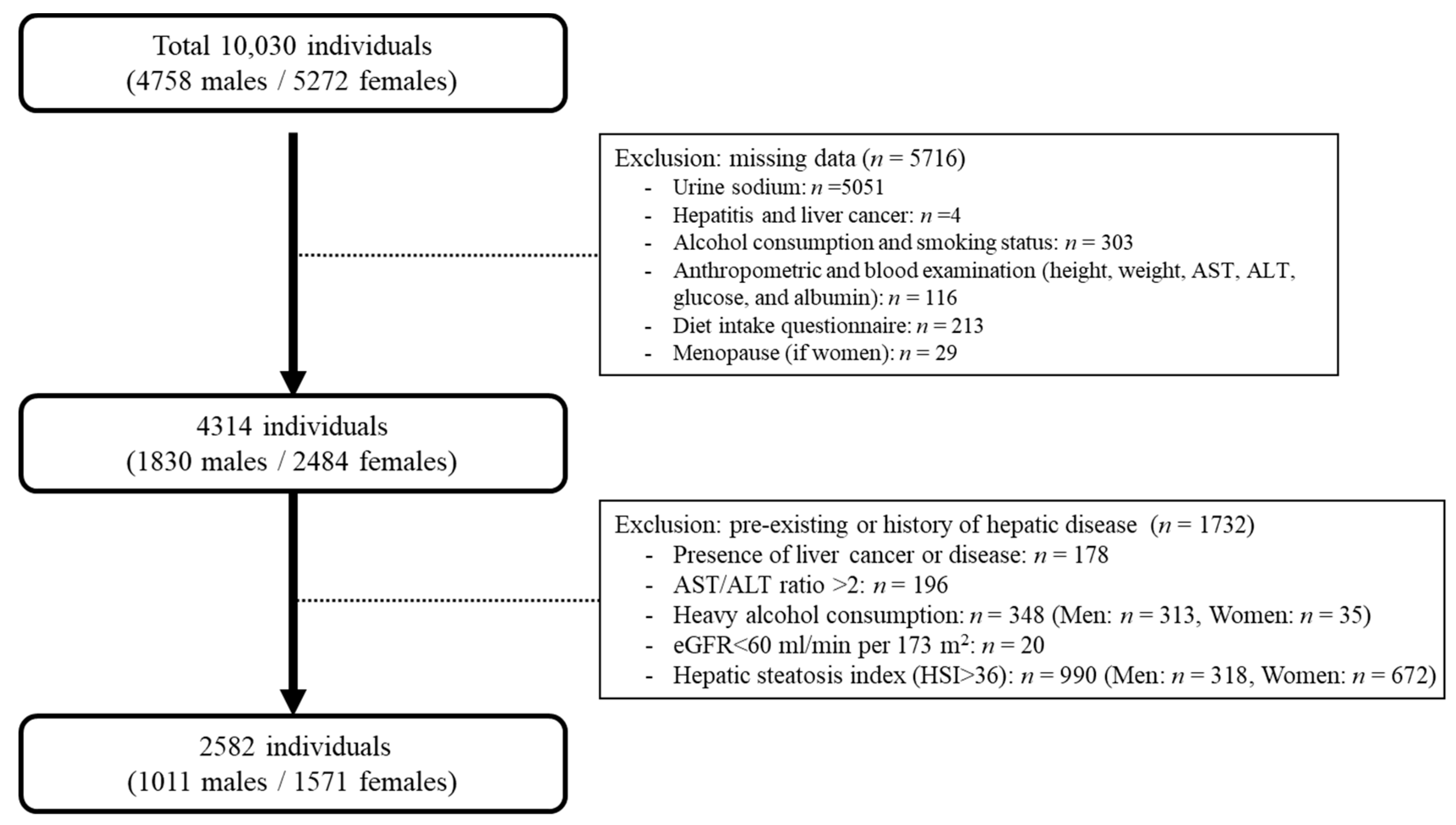
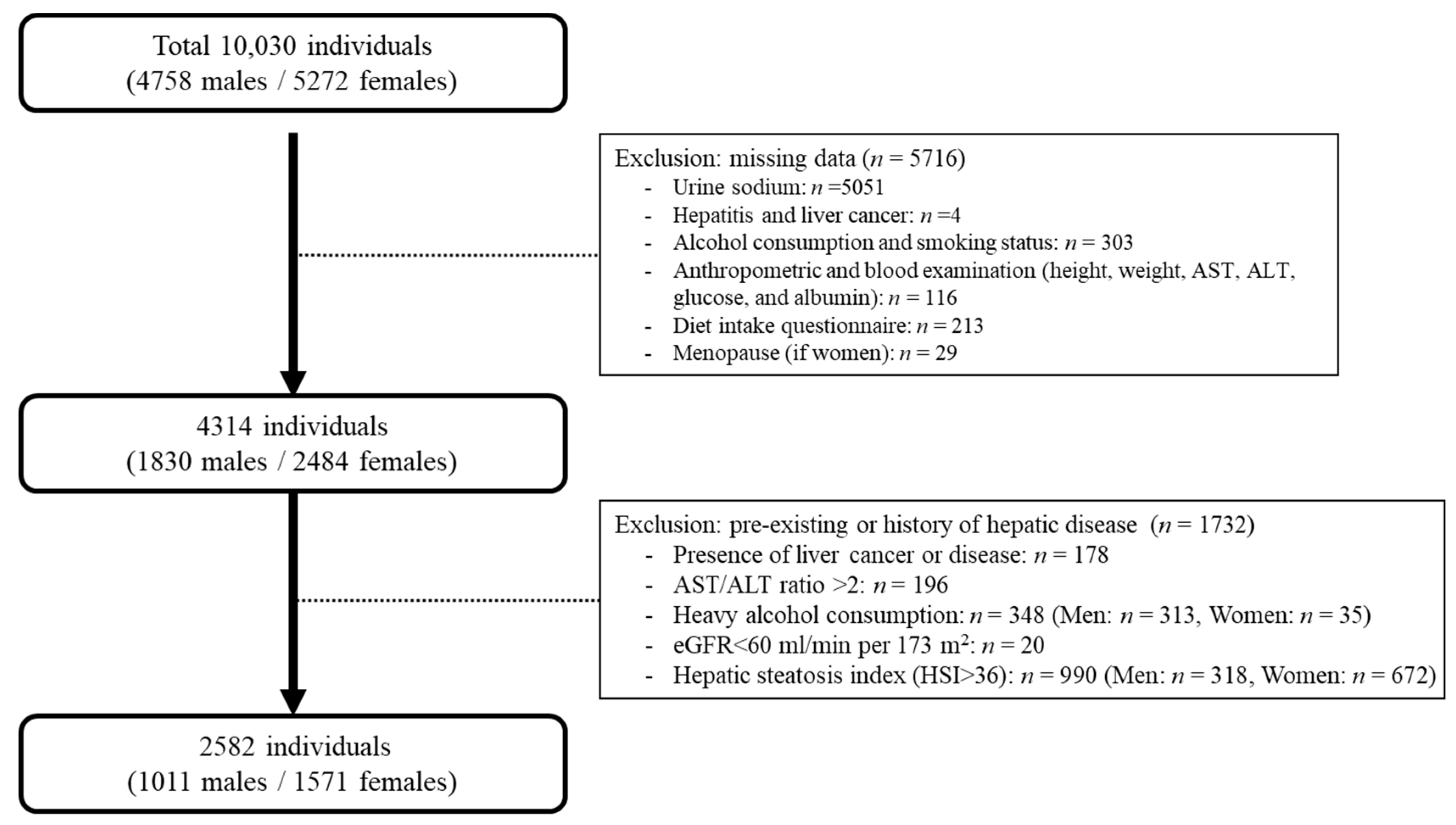
2.1. Study Design and Participants
2.2. Estimation of 24-Hour Sodium Excretion
2.3. Determination of NAFLD Based on Hepatic Steatosis Index (HSI)
2.4. Determination of Hepatic Fibrosis Based on Fibrosis-4 (FIB-4)
2.5. Covariates
2.6. Statistical Analysis
3. Results
3.1. The Distribution of Estimated 24-Hour Urinary Sodium Levels
3.2. Baseline Characteristics of Study Population
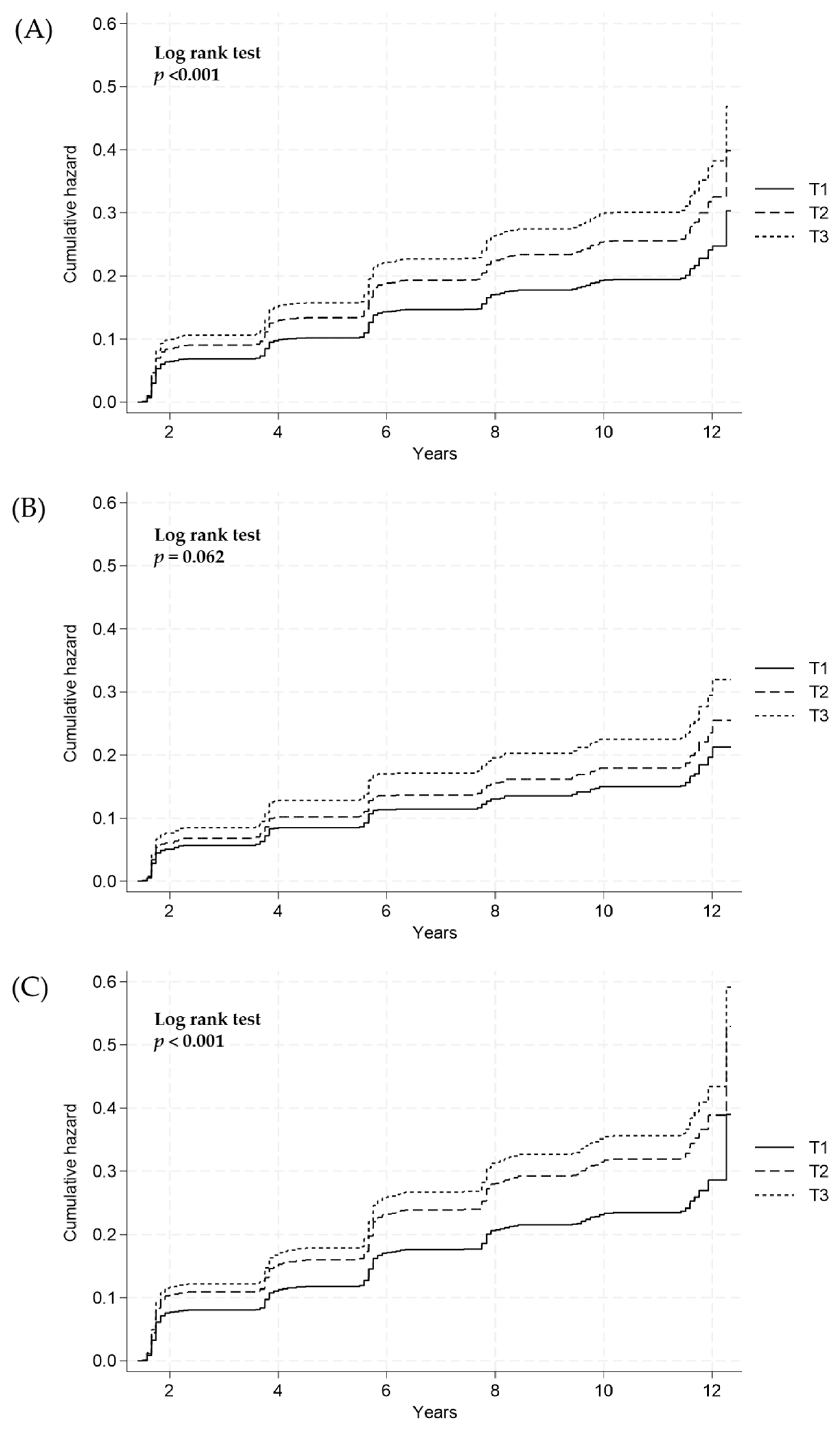
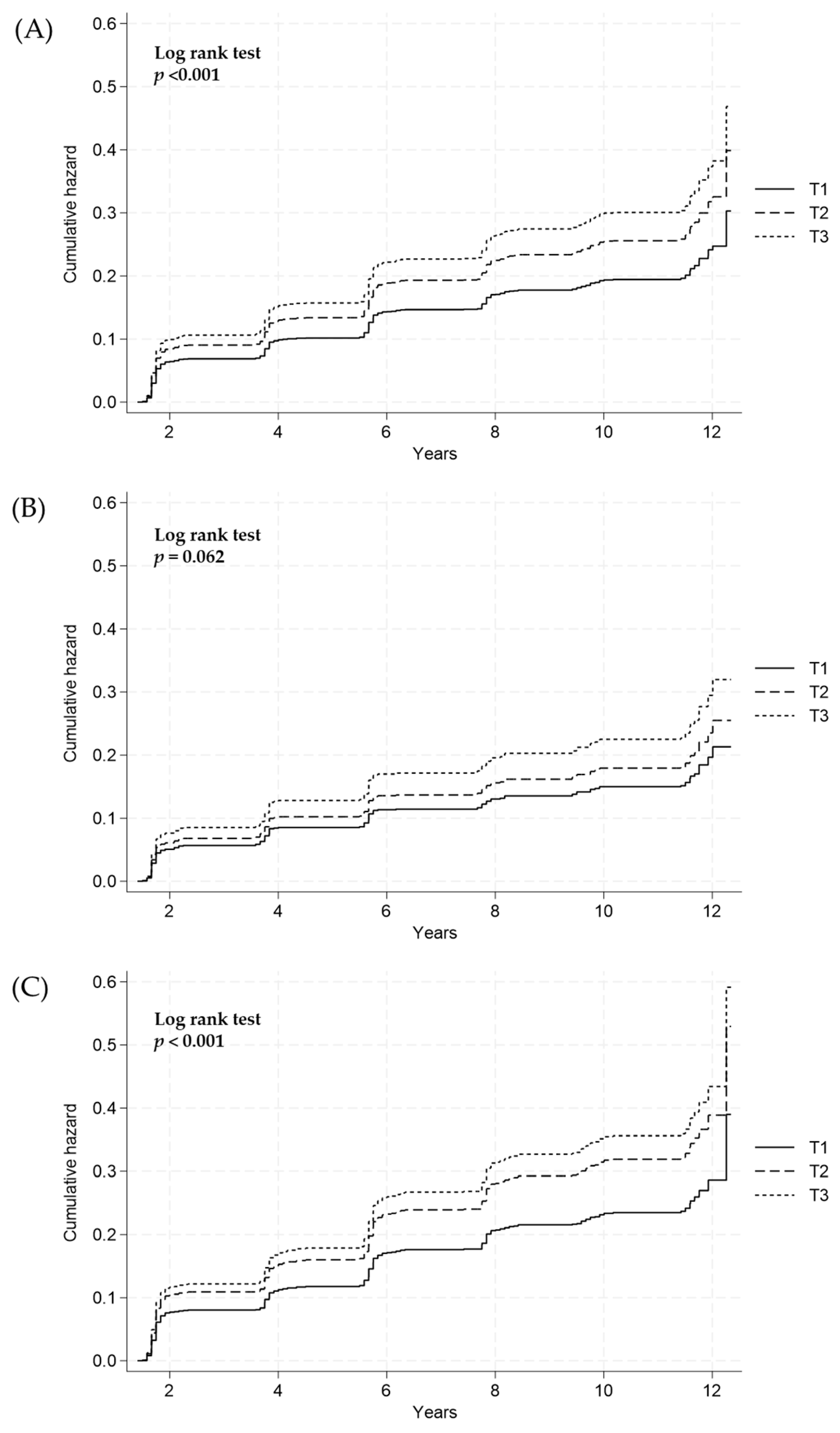
3.3. Longitudinal Relationship between Estimated 24-Hour Urinary Sodium Excretion and Incidence of NAFLD
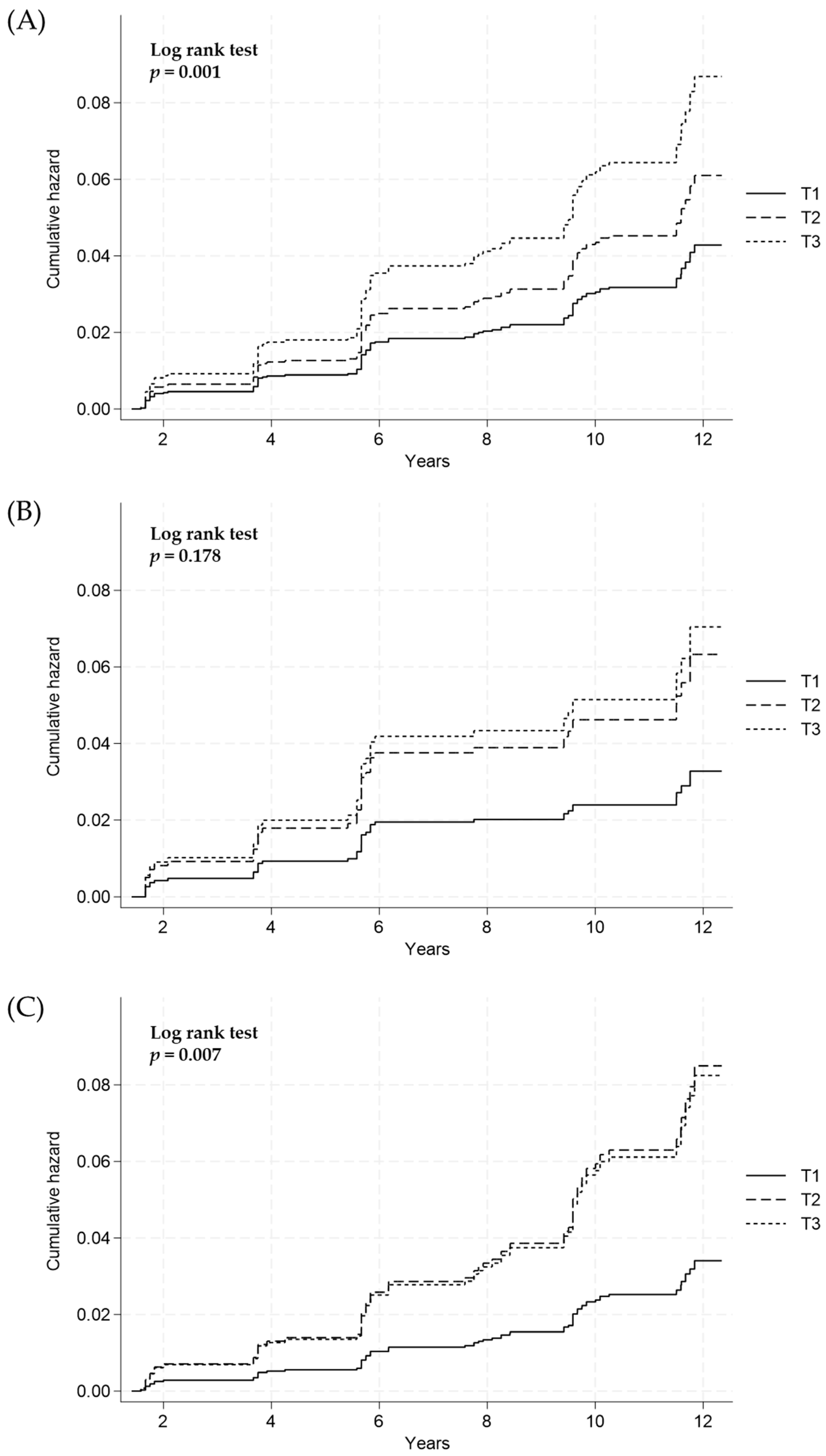
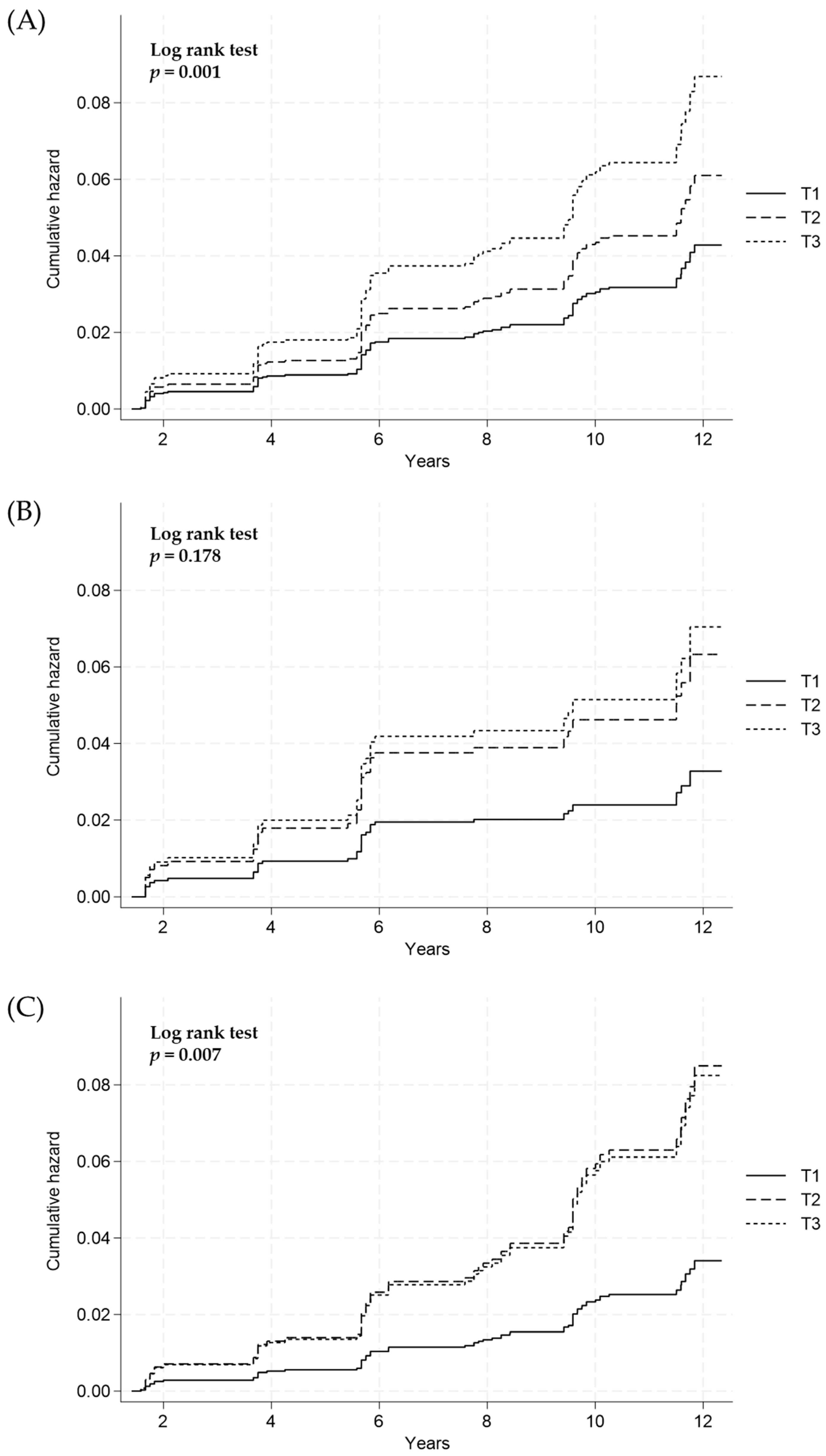
3.4. Longitudinal Relationship between Estimated 24-Hour Urinary Sodium Excretion and Incidence of Hepatic Fibrosis in Subjects with NAFLD
4. Dishcussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pafili, K.; Maltezos, E.; Papanas, N. Ipragliflozin and sodium glucose transporter 2 inhibitors to reduce liver fat: Will the prize we sought be won? Expert. Opin. Pharmacother. 2018, 19, 185–187. [Google Scholar] [CrossRef] [PubMed]
- Cusi, K. Treatment of patients with type 2 diabetes and non-alcoholic fatty liver disease: Current approaches and future directions. Diabetologia 2016, 59, 1112–1120. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Pafili, K.; Roden, M. Nonalcoholic fatty liver disease (NAFLD) from pathogenesis to treatment concepts in humans. Mol. Metab. 2021, 50, 101122. [Google Scholar] [CrossRef] [PubMed]
- Rinella, M.E. Nonalcoholic fatty liver disease: A systematic review. JAMA 2015, 313, 2263–2273. [Google Scholar] [CrossRef] [PubMed]
- Weiss, J.; Rau, M.; Geier, A. Non-alcoholic fatty liver disease: Epidemiology, clinical course, investigation, and treatment. Dtsch. Arztebl. Int. 2014, 111, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Dongiovanni, P.; M Anstee, Q.; Valenti, L. Genetic predisposition in NAFLD and NASH: Impact on severity of liver disease and response to treatment. Curr. Pharm. Des. 2013, 19, 5219–5238. [Google Scholar] [CrossRef]
- Zelber-Sagi, S.; Ratziu, V.; Oren, R. Nutrition and physical activity in NAFLD: An overview of the epidemiological evidence. World J. Gastroenterol. 2011, 17, 3377–3389. [Google Scholar] [CrossRef]
- Mouzaki, M.; Allard, J.P. The role of nutrients in the development, progression, and treatment of nonalcoholic fatty liver disease. J. Clin. Gastroenterol. 2012, 46, 457–467. [Google Scholar] [CrossRef]
- Schwarz, J.M.; Noworolski, S.M.; Wen, M.J.; Dyachenko, A.; Prior, J.L.; Weinberg, M.E.; Herraiz, L.A.; Tai, V.W.; Bergeron, N.; Bersot, T.P.; et al. Effect of a High-Fructose Weight-Maintaining Diet on Lipogenesis and Liver Fat. J. Clin. Endocrinol. Metab. 2015, 100, 2434–2442. [Google Scholar] [CrossRef]
- Wijarnpreecha, K.; Thongprayoon, C.; Edmonds, P.J.; Cheungpasitporn, W. Associations of sugar- and artificially sweetened soda with nonalcoholic fatty liver disease: A systematic review and meta-analysis. QJM Int. J. Med. 2016, 109, 461–466. [Google Scholar] [CrossRef]
- Bansal, V.; Mishra, S.K. Reduced-sodium cheeses: Implications of reducing sodium chloride on cheese quality and safety. Compr. Rev. Food Sci. Food Saf. 2020, 19, 733–758. [Google Scholar] [CrossRef]
- Campbell, N.R.C.; Whelton, P.K.; Orias, M.; Wainford, R.D.; Cappuccio, F.P.; Ide, N.; Neal, B.; Cohn, J.; Cobb, L.K.; Webster, J.; et al. 2022 World Hypertension League, Resolve to Save Lives and International Society of Hypertension dietary sodium (salt) global call to action. J. Hum. Hypertens. 2023, 37, 428–437. [Google Scholar] [CrossRef]
- Jeong, Y.; Kim, E.S.; Lee, J.; Kim, Y. Trends in sodium intake and major contributing food groups and dishes in Korea: The Korea National Health and Nutrition Examination Survey 2013-2017. Nutr. Res. Pract. 2021, 15, 382–395. [Google Scholar] [CrossRef]
- WHO. Guideline: Sodium Intake for Adults and Children; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- Moosavian, S.P.; Haghighatdoost, F.; Surkan, P.J.; Azadbakht, L. Salt and obesity: A systematic review and meta-analysis of observational studies. Int. J. Food Sci. Nutr. 2017, 68, 265–277. [Google Scholar] [CrossRef] [PubMed]
- Baudrand, R.; Campino, C.; Carvajal, C.A.; Olivieri, O.; Guidi, G.; Faccini, G.; Vohringer, P.A.; Cerda, J.; Owen, G.; Kalergis, A.M.; et al. High sodium intake is associated with increased glucocorticoid production, insulin resistance and metabolic syndrome. Clin. Endocrinol. 2014, 80, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Subasinghe, A.K.; Arabshahi, S.; Busingye, D.; Evans, R.G.; Walker, K.Z.; Riddell, M.A.; Thrift, A.G. Association between salt and hypertension in rural and urban populations of low to middle income countries: A systematic review and meta-analysis of population based studies. Asia Pac. J. Clin. Nutr. 2016, 25, 402–413. [Google Scholar] [CrossRef]
- Hu, G.; Jousilahti, P.; Peltonen, M.; Lindstrom, J.; Tuomilehto, J. Urinary sodium and potassium excretion and the risk of type 2 diabetes: A prospective study in Finland. Diabetologia 2005, 48, 1477–1483. [Google Scholar] [CrossRef]
- Ha, S.K. Dietary salt intake and hypertension. Electrolyte Blood Press. 2014, 12, 7–18. [Google Scholar] [CrossRef]
- D’Elia, L.; Rossi, G.; Ippolito, R.; Cappuccio, F.P.; Strazzullo, P. Habitual salt intake and risk of gastric cancer: A meta-analysis of prospective studies. Clin. Nutr. 2012, 31, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Huh, J.H.; Lee, K.J.; Lim, J.S.; Lee, M.Y.; Park, H.J.; Kim, M.Y.; Kim, J.W.; Chung, C.H.; Shin, J.Y.; Kim, H.S.; et al. High Dietary Sodium Intake Assessed by Estimated 24-h urinary sodium Excretion Is Associated with NAFLD and Hepatic Fibrosis. PLoS ONE 2015, 10, e0143222. [Google Scholar] [CrossRef]
- Choi, Y.; Lee, J.E.; Chang, Y.; Kim, M.K.; Sung, E.; Shin, H.; Ryu, S. Dietary sodium and potassium intake in relation to non-alcoholic fatty liver disease. Br. J. Nutr. 2016, 116, 1447–1456. [Google Scholar] [CrossRef] [PubMed]
- Han, E.; Kim, M.K.; Im, S.S.; Kim, H.S.; Kwon, T.K.; Jang, B.K. High Sodium Intake, as Assessed by Urinary sodium Excretion, Is Associated with Nonalcoholic Fatty Liver Disease or Sarcopenia. Gut Liver 2023, 17, 456–465. [Google Scholar] [CrossRef]
- Zhou, L.; Yang, Y.; Feng, Y.; Zhao, X.; Fan, Y.; Rong, J.; Zhao, L.; Yu, Y. Association between dietary sodium intake and non-alcoholic fatty liver disease in the US population. Public Health Nutr. 2021, 24, 993–1000. [Google Scholar] [CrossRef]
- Kim, Y.; Han, B.G.; Ko, G.E.S.g. Cohort Profile: The Korean Genome and Epidemiology Study (KoGES) Consortium. Int. J. Epidemiol. 2017, 46, e20. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, T.; Okamura, T.; Miura, K.; Kadowaki, T.; Ueshima, H.; Nakagawa, H.; Hashimoto, T. A simple method to estimate populational 24-h urinary sodium and potassium excretion using a casual urine specimen. J. Hum. Hypertens. 2002, 16, 97–103. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, D.; Kim, H.J.; Lee, C.H.; Yang, J.I.; Kim, W.; Kim, Y.J.; Yoon, J.H.; Cho, S.H.; Sung, M.W.; et al. Hepatic steatosis index: A simple screening tool reflecting nonalcoholic fatty liver disease. Dig. Liver Dis. 2010, 42, 503–508. [Google Scholar] [CrossRef] [PubMed]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, S.M.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef]
- Levey, A.S.; Coresh, J.; Greene, T.; Stevens, L.A.; Zhang, Y.L.; Hendriksen, S.; Kusek, J.W.; Van Lente, F.; Chronic Kidney Disease Epidemiology, C. Using standardized serum creatinine values in the modification of diet in renal disease study equation for estimating glomerular filtration rate. Ann. Intern. Med. 2006, 145, 247–254. [Google Scholar] [CrossRef]
- Lefebvre, P.; Staels, B. Hepatic sexual dimorphism—Implications for non-alcoholic fatty liver disease. Nat. Rev. Endocrinol. 2021, 17, 662–670. [Google Scholar] [CrossRef]
- Ballestri, S.; Nascimbeni, F.; Baldelli, E.; Marrazzo, A.; Romagnoli, D.; Lonardo, A. NAFLD as a Sexual Dimorphic Disease: Role of Gender and Reproductive Status in the Development and Progression of Nonalcoholic Fatty Liver Disease and Inherent Cardiovascular Risk. Adv. Ther. 2017, 34, 1291–1326. [Google Scholar] [CrossRef]
- Lonardo, A.; Suzuki, A. Sexual Dimorphism of NAFLD in Adults. Focus on Clinical Aspects and Implications for Practice and Translational Research. J. Clin. Med. 2020, 9, 1278. [Google Scholar] [CrossRef]
- Lee, H.S.; Duffey, K.J.; Popkin, B.M. Sodium and potassium intake patterns and trends in South Korea. J. Hum. Hypertens. 2013, 27, 298–303. [Google Scholar] [CrossRef]
- Shen, X.; Jin, C.; Wu, Y.; Zhang, Y.; Wang, X.; Huang, W.; Li, J.; Wu, S.; Gao, X. Prospective study of perceived dietary salt intake and the risk of non-alcoholic fatty liver disease. J. Hum. Nutr. Diet. 2019, 32, 802–809. [Google Scholar] [CrossRef]
- Van den Berg, E.H.; Gruppen, E.G.; Blokzijl, H.; Bakker, S.J.L.; Dullaart, R.P.F. Higher Sodium Intake Assessed by 24 Hour Urinary sodium Excretion Is Associated with Non-Alcoholic Fatty Liver Disease: The PREVEND Cohort Study. J. Clin. Med. 2019, 8, 2157. [Google Scholar] [CrossRef]
- De Melo Portela, C.L.; de Carvalho Sampaio, H.A.; Pereira de Melo, M.L.; Ferreira Carioca, A.A.; Maia Pinto, F.J.; Machado Arruda, S.P. Nutritional Status, Diet and Non-Alcoholic Fatty Liver Disease in Elders. Nutr. Hosp. 2015, 32, 2038–2045. [Google Scholar] [CrossRef]
- Park, S.H.; Jeon, W.K.; Kim, S.H.; Kim, H.J.; Park, D.I.; Cho, Y.K.; Sung, I.K.; Sohn, C.I.; Keum, D.K.; Kim, B.I. Prevalence and risk factors of non-alcoholic fatty liver disease among Korean adults. J. Gastroenterol. Hepatol. 2006, 21, 138–143. [Google Scholar] [CrossRef] [PubMed]
- Eguchi, Y.; Hyogo, H.; Ono, M.; Mizuta, T.; Ono, N.; Fujimoto, K.; Chayama, K.; Saibara, T.; Jsg, N. Prevalence and associated metabolic factors of nonalcoholic fatty liver disease in the general population from 2009 to 2010 in Japan: A multicenter large retrospective study. J. Gastroenterol. 2012, 47, 586–595. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, J.; Fisher, B.M.; Jaap, A.J.; Stanley, A.; Paterson, K.; Sattar, N. Effects of HRT on liver enzyme levels in women with type 2 diabetes: A randomized placebo-controlled trial. Clin. Endocrinol. 2006, 65, 40–44. [Google Scholar] [CrossRef]
- Grillo, A.; Salvi, L.; Coruzzi, P.; Salvi, P.; Parati, G. Sodium Intake and Hypertension. Nutrients 2019, 11, 1970. [Google Scholar] [CrossRef] [PubMed]
- Lastra, G.; Dhuper, S.; Johnson, M.S.; Sowers, J.R. Salt, aldosterone, and insulin resistance: Impact on the cardiovascular system. Nat. Rev. Cardiol. 2010, 7, 577–584. [Google Scholar] [CrossRef]
- Rinaldi, L.; Pafundi, P.C.; Galiero, R.; Caturano, A.; Morone, M.V.; Silvestri, C.; Giordano, M.; Salvatore, T.; Sasso, F.C. Mechanisms of Non-Alcoholic Fatty Liver Disease in the Metabolic Syndrome. A Narrative Review. Antioxidants 2021, 10, 270. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Lee, H.S.; Ahn, S.B.; Kwon, Y.J. Dairy protein intake is inversely related to development of non-alcoholic fatty liver disease. Clin. Nutr. 2021, 40, 5252–5260. [Google Scholar] [CrossRef] [PubMed]
- Nyblom, H.; Berggren, U.; Balldin, J.; Olsson, R. High AST/ALT ratio may indicate advanced alcoholic liver disease rather than heavy drinking. Alcohol Alcohol. 2004, 39, 336–339. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Mean | SD | Min | Percentile | Max | |||
|---|---|---|---|---|---|---|---|
| 25th | 50th | 75th | |||||
| All subjects (n = 2582) | 161.69 | 35.57 | 62.72 | 138.63 | 160.42 | 182.62 | 391.32 |
| Males (n = 1011) | 162.03 | 35.47 | 64.04 | 138.36 | 160.99 | 182.89 | 373.08 |
| Females (n = 1571) | 161.48 | 35.65 | 62.72 | 138.74 | 160.20 | 182.58 | 391.32 |
| Characteristics | Tertiles of 24-Hour Urinary Sodium Excretion (mmol/Day) | p-Value | ||
|---|---|---|---|---|
| T1 (n = 861) | T2 (n = 861) | T3 (n = 860) | ||
| 24-h urinary sodium, mmol/day | 129.11 (115.53–138.63) | 160.42 (152.95–167.25) | 192.76 (182.63–208.43) | <0.001 † |
| Age, yr | 49 (43–59) | 51 (44–61) | 53 (45–61) | <0.001 † |
| Gender (females), n (%) | 529 (61.44) | 531 (61.67) | 511 (59.42) | 0.574 |
| BMI, kg/m2 | 22.91 (21.41–24.61) | 23.53 (21.90–25.01) | 23.89 (22.39–25.34) | <0.001 † |
| Drinking status, n (%) | 0.783 | |||
| Never | 489 (56.79) | 472 (54.82) | 487 (56.63) | |
| Former | 58 (6.74) | 66 (7.67) | 54 (6.28) | |
| Current | 314 (36.47) | 323 (37.51) | 319 (37.09) | |
| Smoking status, n (%) | 0.002 | |||
| Never | 555 (64.46) | 585 (67.94) | 602 (70.00) | |
| Former | 82 (9.52) | 93 (10.80) | 102 (11.86) | |
| Current | 224 (26.02) | 183 (21.25) | 156 (18.14) | |
| Physical activity, MET-h/week | 17.00 (9.37–30.37) | 18.37 (9.62–34.25) | 19.12 (10.50–35.00) | 0.016 † |
| AST, IU/L | 21 (18–25) | 21 (18–25) | 21 (17–25) | 0.488 † |
| ALT, IU/L | 16 (12–21) | 16 (13–21) | 17 (13–21)) | 0.078 † |
| TG, mg/dL | 106 (77–151) | 111 (82–160) | 120 (86.5–176.5) | <0.001 † |
| T-Chol, mg/dL | 189 (167–214) | 192 (170–215) | 191 (171–214) | 0.097 † |
| Albumin, g/dL | 4.4 (4.2–4.6) | 4.4 (4.3–4.6)) | 4.4 (4.2–4.6) | 0.221 † |
| Urine potassium, mmol/L | 55 (35–82) | 43 (30–64) | 39 (27–55) | <0.001 † |
| HOMA-IR | 1.38 (1.02–1.95) | 1.45 (1.03–2.06) | 1.48 (1.05–2.08) | 0.005 † |
| eGFR, CKD-EPI, mL/min/1.73 m2 | 102.69 (93.11–110.03) | 103.37 (94.73–110.51) | 103.46 (95.80–109.84) | 0.053 † |
| Hypertension, n (%) | 202 (23.46) | 237 (27.53) | 296 (34.42) | <0.001 |
| Diabetes mellitus, n (%) | 30 (3.48) | 28 (3.25) | 42 (4.88) | 0.165 |
| Hyperlipidaemia, n (%) | 262 (29.31) | 257 (28.78) | 294 (32.92) | 0.117 |
| Postmenopausal, n (%) | 290 (33.68) | 312 (36.24) | 350 (40.70) | 0.005 |
| Total energy, kcal | 1796.7 (1484.2–2186.2) | 1883.9 (1515.9–2325.8) | 1930.1 (1592.8–2367.4) | <0.001 † |
| Protein, g | 58.92 (45.77–75.72) | 62.08 (46.54–78.76) | 63.77 (50.29–81.96) | <0.001 † |
| Fat, g | 27.04 (18.12–38.19) | 27.57 (17.89–38.91) | 29.05 (19.12–41.19) | 0.002 † |
| Carbohydrate, g | 325.75 (273.96–388.04) | 334.77 (280.48–405.66) | 343.05 (290.38–422.54) | <0.001 † |
| Hazard Ratio (95% CI) | p-Value | |||
|---|---|---|---|---|
| T1 | T2 | T3 | ||
| All (n = 2582) | 861 | 861 | 860 | |
| Incident case, n (%) | 139 (16.14) | 182 (21.13) | 203 (23.60) | <0.001 |
| Crude analysis | Ref | 1.32 (1.06, 1.65) | 1.55 (1.25, 1.92) | <0.001 * |
| Multivariate analysis | Ref | 1.31 (1.05–1.64) | 1.54 (1.24–1.92) | <0.001 * |
| Men (n = 1011) | 337 | 337 | 337 | |
| Incident case, n (%) | 49 (14.54) | 58 (17.21) | 66 (19.58) | 0.174 |
| Crude analysis | Ref | 1.18 (0.80, 1.72) | 1.41 (0.98, 2.04) | 0.064 * |
| Multivariate analysis | Ref | 1.19 (0.81, 1.75) | 1.50 (1.02, 2.19) | <0.001 * |
| Females (n = 1571) | 524 | 524 | 523 | |
| Incident case, n (%) | 90 (17.17) | 124 (23.66) | 137 (26.19) | 0.001 |
| Crude analysis | Ref | 1.40 (1.07, 1.84) | 1.62 (1.24, 2.12) | <0.001 * |
| Multivariate analysis | Ref | 1.35 (1.03, 1.78) | 1.51 (1.15, 1.98) | 0.003 * |
| Hazard Ratio (95% CI) | p-Value | |||
|---|---|---|---|---|
| T1 | T2 | T3 | ||
| All (n = 2582) | 861 | 861 | 860 | |
| Incident case, n (%) | 21 (2.43) | 48 (5.57) | 49 (5.69) | 0.001 |
| Crude analysis | Ref | 2.25 (1.35, 3.77) | 2.37 (1.42, 3.95) | 0.001 * |
| Multivariate analysis | Ref | 2.26 (1.35, 3.78) | 2.28 (1.36, 3.83) | 0.003 * |
| Men (n = 1011) | 337 | 337 | 337 | |
| Incident case, n (%) | 7 (2.07) | 17 (5.04) | 18 (5.34) | 0.178 |
| Crude analysis | Ref | 1.87 (0.83, 4.19) | 2.04 (0.91, 4.55) | 0.083 * |
| Multivariate analysis | Ref | 1.93 (0.85, 4.36) | 2.14 (0.95, 4.86) | 0.073 * |
| Females (n = 1571) | 524 | 524 | 523 | |
| Incident case, n (%) | 12 (1.90) | 31 (4.77) | 31 (5.73) | 0.007 |
| Crude analysis | Ref | 2.54 (1.30, 4.95) | 2.61 (1.34, 5.09) | 0.005 * |
| Multivariate analysis | Ref | 2.49 (1.27, 4.86) | 2.42 (1.23, 4.73) | 0.015 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.; Lee, J.-Y.; Yang, Y.-J. Sex-Specific Association between Sodium Intake Estimated by 24-Hour Urinary Sodium Excretion and Nonalcoholic Fatty Liver Disease: The Community-Based Prospective Cohort Study. Nutrients 2024, 16, 548. https://doi.org/10.3390/nu16040548
Lee J, Lee J-Y, Yang Y-J. Sex-Specific Association between Sodium Intake Estimated by 24-Hour Urinary Sodium Excretion and Nonalcoholic Fatty Liver Disease: The Community-Based Prospective Cohort Study. Nutrients. 2024; 16(4):548. https://doi.org/10.3390/nu16040548
Chicago/Turabian StyleLee, Jihye, Ju-Yeon Lee, and Yun-Jung Yang. 2024. "Sex-Specific Association between Sodium Intake Estimated by 24-Hour Urinary Sodium Excretion and Nonalcoholic Fatty Liver Disease: The Community-Based Prospective Cohort Study" Nutrients 16, no. 4: 548. https://doi.org/10.3390/nu16040548
APA StyleLee, J., Lee, J.-Y., & Yang, Y.-J. (2024). Sex-Specific Association between Sodium Intake Estimated by 24-Hour Urinary Sodium Excretion and Nonalcoholic Fatty Liver Disease: The Community-Based Prospective Cohort Study. Nutrients, 16(4), 548. https://doi.org/10.3390/nu16040548