
Depressive Symptoms among Bariatric Surgery Candidates: Associations with Stigmatization and Weight and Shape Concern

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Measures
2.2.1. Predictor Variable: Experienced Stigmatization
2.2.2. Outcome Variable: Depressive Symptoms
2.2.3. Mediator Variable: Weight Bias Internalization
2.2.4. Moderator Variable: Weight and Shape Concern
2.2.5. Control Variables
2.3. Data Analysis
3. Results
3.1. Sample Characteristics
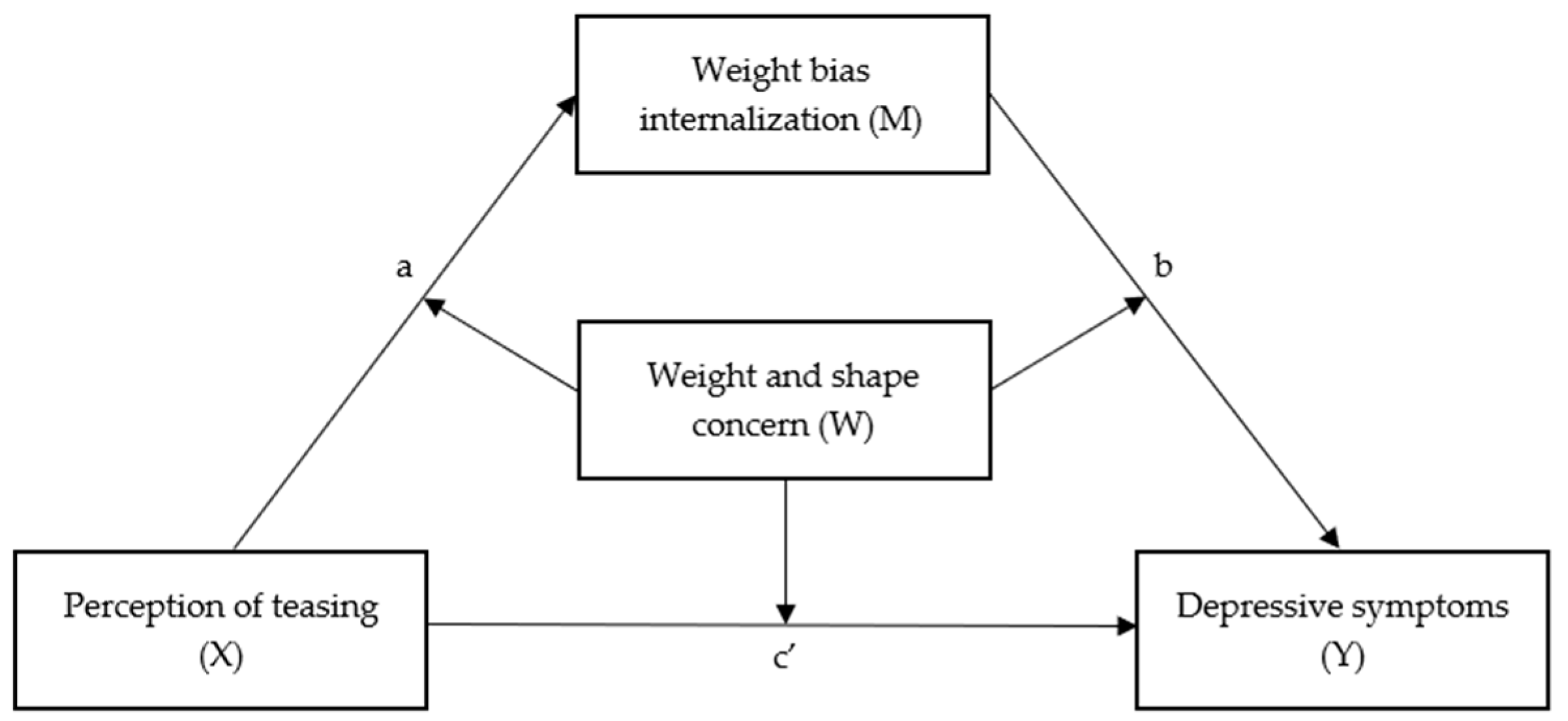
3.2. Mediation
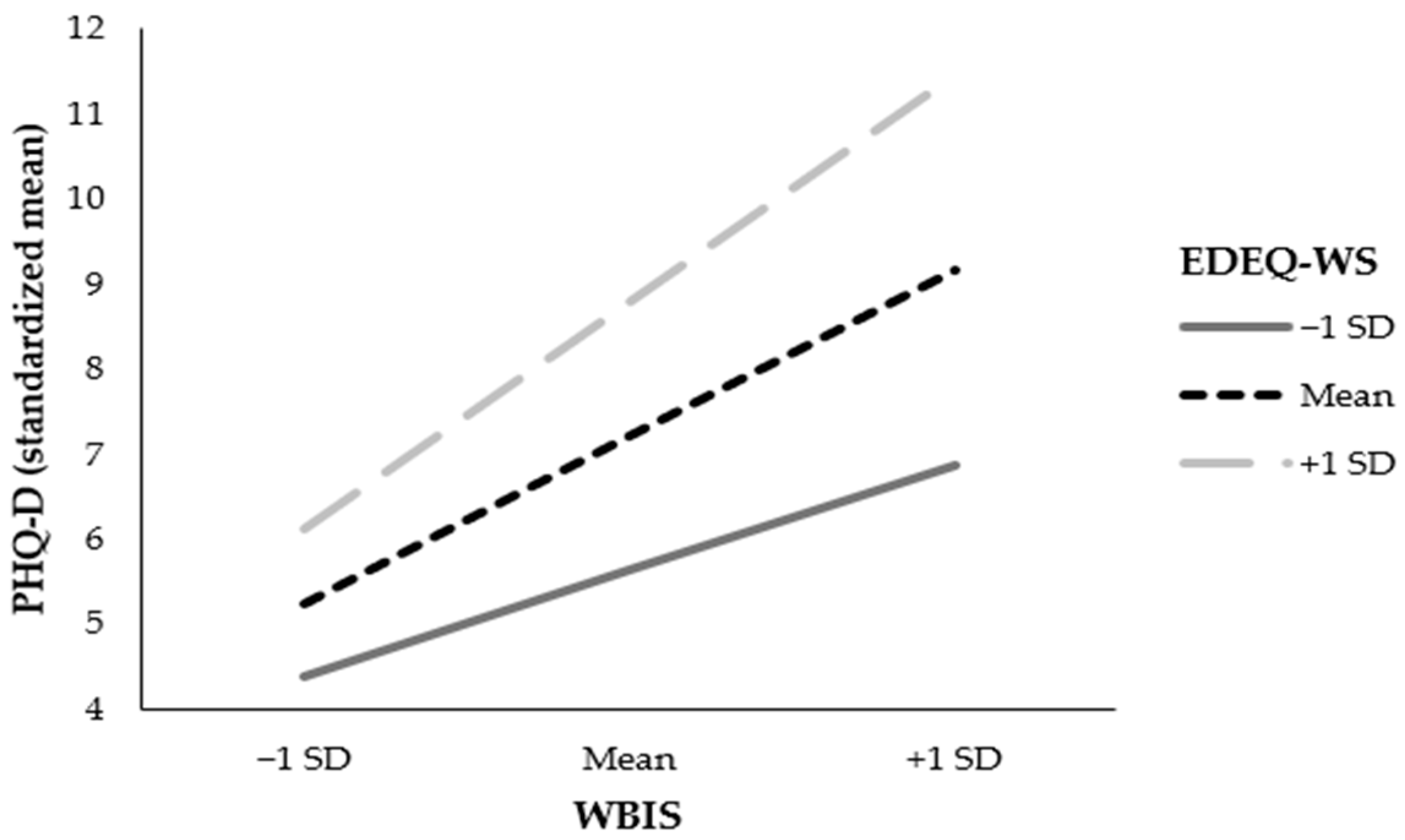
3.3. Moderated Mediation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef]
- The GBD 2015 Obesity Collaborators. Health effects of overweight and obesity in 195 countries over 25 years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration (NCD-RisC). Trends in adult body-mass index in 200 countries from 1975 to 2014: A pooled analysis of 1698 population-based measurement studies with 19.2 million participants. Lancet 2016, 387, 1377–1396. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 2 September 2022).
- Chu, D.-T.; Minh Nguyet, N.T.; Dinh, T.C.; Thai Lien, N.V.; Nguyen, K.-H.; Nhu Ngoc, V.T.; Tao, Y.; Le Son, H.; Le, D.-H.; Nga, V.B.; et al. An update on physical health and economic consequences of overweight and obesity. Diabetes Metab. Syndr. 2018, 12, 1095–1100. [Google Scholar] [CrossRef]
- Avila, C.; Holloway, A.C.; Hahn, M.K.; Morrison, K.M.; Restivo, M.; Anglin, R.; Taylor, V.H. An overview of links between obesity and mental health. Curr. Obes. Rep. 2015, 4, 303–310. [Google Scholar] [CrossRef]
- Lehnert, T.; Sonntag, D.; Konnopka, A.; Riedel-Heller, S.; König, H.-H. Economic costs of overweight and obesity. Best Practice & Research. Clin. Endocrinol. Metab. 2013, 27, 105–115. [Google Scholar] [CrossRef]
- LeBlanc, E.S.; Patnode, C.D.; Webber, E.M.; Redmond, N.; Rushkin, M.; O’Connor, E.A. Behavioral and pharmacotherapy weight loss interventions to prevent obesity-related morbidity and mortality in adults: Updated evidence report and systematic review for the US Preventive Services Task Force. JAMA 2018, 320, 1172–1191. [Google Scholar] [CrossRef] [PubMed]
- Wadden, T.A.; Bailey, T.S.; Billings, L.K.; Davies, M.; Frias, J.P.; Koroleva, A.; Lingvay, I.; O’Neil, P.M.; Rubino, D.M.; Skovgaard, D.; et al. Effect of subcutaneous semaglutide vs placebo as an adjunct to intensive behavioral therapy on body weight in adults with overweight or obesity: The STEP 3 randomized clinical trial. JAMA 2021, 325, 1403–1413. [Google Scholar] [CrossRef]
- Wolfe, B.M.; Kvach, E.; Eckel, R.H. Treatment of obesity: Weight loss and bariatric surgery. Circ. Res. 2016, 118, 1844–1855. [Google Scholar] [CrossRef]
- Hilbert, A.; Staerk, C.; Strömer, A.; Mansfeld, T.; Sander, J.; Seyfried, F.; Kaiser, S.; Dietrich, A.; Mayr, A. Nonnormative eating behaviors and eating disorders and their associations with weight loss and quality of life during 6 years following obesity surgery. JAMA Netw. Open 2022, 5, e2226244. [Google Scholar] [CrossRef]
- Duarte-Guerra, L.S.; Coêlho, B.M.; Santo, M.A.; Wang, Y.-P. Psychiatric disorders among obese patients seeking bariatric surgery: Results of structured clinical interviews. Obes. Surg. 2015, 25, 830–837. [Google Scholar] [CrossRef]
- Fischer, L.; Wekerle, A.-L.; Sander, J.; Nickel, F.; Billeter, A.T.; Zech, U.; Bruckner, T.; Müller-Stich, B.P. Is there a reason why obese patients choose either conservative treatment or surgery? Obes. Surg. 2017, 27, 1684–1690. [Google Scholar] [CrossRef]
- Tylka, T.L.; Annunziato, R.A.; Burgard, D.; Daníelsdóttir, S.; Shuman, E.; Davis, C.; Calogero, R.M. The weight-inclusive versus weight-normative approach to health: Evaluating the evidence for prioritizing well-being over weight loss. J. Obes. 2014, 2014, 983495. [Google Scholar] [CrossRef] [PubMed]
- Forbes, Y.; Donovan, C. The role of internalised weight stigma and self-compassion in the psychological well-being of overweight and obese women. Aust. Psychol. 2019, 54, 471–482. [Google Scholar] [CrossRef]
- Pötzsch, A.; Rudolph, A.; Schmidt, R.; Hilbert, A. Two sides of weight bias in adolescent binge-eating disorder: Adolescents’ perceptions and maternal attitudes. Int. J. Eat. Disord. 2018, 51, 1339–1345. [Google Scholar] [CrossRef]
- Olson, K.L.; Mensinger, J.L. Weight-related stigma mediates the relationship between weight status and bodily pain: A conceptual model and call for further research. Body Image 2019, 30, 159–164. [Google Scholar] [CrossRef]
- Hayward, L.E.; Vartanian, L.R.; Pinkus, R.T. Weight stigma predicts poorer psychological well-being through internalized weight bias and maladaptive coping responses. Obesity 2018, 26, 755–761. [Google Scholar] [CrossRef] [PubMed]
- Carr, D.; Friedman, M.A. Is obesity stigmatizing? Body weight, perceived discrimination, and psychological well-being in the United States. J. Health Soc. Behav. 2005, 46, 244–259. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R.M.; Himmelstein, M.S.; Quinn, D.M. Internalizing weight stigma: Prevalence and sociodemographic considerations in US adults. Obesity 2018, 26, 167–175. [Google Scholar] [CrossRef]
- Braun, T.D.; Gorin, A.A.; Puhl, R.M.; Stone, A.; Quinn, D.M.; Ferrand, J.; Abrantes, A.M.; Unick, J.; Tishler, D.; Papasavas, P. Shame and self-compassion as risk and protective mechanisms of the internalized weight bias and emotional eating link in individuals seeking bariatric surgery. Obes. Surg. 2021, 31, 3177–3187. [Google Scholar] [CrossRef]
- Luck-Sikorski, C.; Bernard, M. Stigmatisierung und Diskriminierung von Patient*innen mit Adipositas. Psychotherapeut 2021, 66, 28–34. [Google Scholar] [CrossRef]
- Alimoradi, Z.; Golboni, F.; Griffiths, M.D.; Broström, A.; Lin, C.-Y.; Pakpour, A.H. Weight-related stigma and psychological distress: A systematic review and meta-analysis. Clin. Nutr. 2020, 39, 2001–2013. [Google Scholar] [CrossRef]
- Crockett, K.B.; Borgatti, A.; Tan, F.; Tang, Z.; Dutton, G. Weight discrimination experienced prior to enrolling in a behavioral obesity intervention is associated with treatment response among black and white adults in the Southeastern U.S. Int. J. Behav. Med. 2022, 29, 152–159. [Google Scholar] [CrossRef]
- Duan, W.; Wang, Z. Mindfulness capability mediates the association between weight-based stigma and negative emotion symptoms. Mindfulness 2019, 10, 1074–1081. [Google Scholar] [CrossRef]
- Emmer, C.; Bosnjak, M.; Mata, J. The association between weight stigma and mental health: A meta-analysis. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2020, 21, e12935. [Google Scholar] [CrossRef] [PubMed]
- Pearl, R.L.; Puhl, R.M. Weight bias internalization and health: A systematic review. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2018, 19, 1141–1163. [Google Scholar] [CrossRef] [PubMed]
- Spahlholz, J.; Pabst, A.; Riedel-Heller, S.G.; Luck-Sikorski, C. Coping with perceived weight discrimination: Testing a theoretical model for examining the relationship between perceived weight discrimination and depressive symptoms in a representative sample of individuals with obesity. Int. J. Obes. 2016, 40, 1915–1921. [Google Scholar] [CrossRef] [PubMed]
- Pearl, R.L.; Hernandez, M.; Bach, C.; Groshon, L.; Wadden, T.A. Prevalence of diagnosed psychiatric disorders among adults who have experienced and internalized weight stigma. Obes. Sci. Pract. 2023, 9, 681–687. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, K.; Paczkowska, A.; Bryl, W.; Marzec, K.; Raakow, J.; Pross, M.; Berghaus, R.; Nowakowska, E.; Kus, K.; Michalak, M. Comparison of perceived weight discrimination between Polish and German patients underwent bariatric surgery or endoscopic method versus conservative treatment for morbid obesity: An International Multicenter Study. Nutrients 2022, 14, 2775. [Google Scholar] [CrossRef] [PubMed]
- Wagner, A.F.; Butt, M.; Rigby, A. Internalized weight bias in patients presenting for bariatric surgery. Eat. Behav. 2020, 39, 101429. [Google Scholar] [CrossRef] [PubMed]
- Pearl, R.L.; Puhl, R.M. The distinct effects of internalizing weight bias: An experimental study. Body Image 2016, 17, 38–42. [Google Scholar] [CrossRef]
- Szwimer, E.; Mougharbel, F.; Goldfield, G.S.; Alberga, A.S. The association between weight-based teasing from peers and family in childhood and depressive symptoms in childhood and adulthood: A systematic review. Curr. Obes. Rep. 2020, 9, 15–29. [Google Scholar] [CrossRef] [PubMed]
- Bidstrup, H.; Brennan, L.; Kaufmann, L.; La Piedad Garcia, X.D. Internalised weight stigma as a mediator of the relationship between experienced/perceived weight stigma and biopsychosocial outcomes: A systematic review. Int. J. Obes. 2022, 46, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Magallares, A.; Bolaños-Rios, P.; Ruiz-Prieto, I.; Benito de Valle, P.; Irles, J.A.; Jáuregui-Lobera, I. The mediational effect of weight self-stigma in the relationship between blatant and subtle discrimination and depression and anxiety. Span. J. Psychol. 2017, 20, E4. [Google Scholar] [CrossRef]
- Braun, T.D.; Quinn, D.M.; Stone, A.; Gorin, A.A.; Ferrand, J.; Puhl, R.M.; Sierra, J.; Tishler, D.; Papasavas, P. Weight bias, shame, and self-compassion: Risk/protective mechanisms of depression and anxiety in prebariatic surgery patients. Obesity 2020, 28, 1974–1983. [Google Scholar] [CrossRef]
- Gee, A.; Troop, N.A. Shame, depressive symptoms and eating, weight and shape concerns in a non-clinical sample. Eat. Weight Disord. EWD 2003, 8, 72–75. [Google Scholar] [CrossRef]
- Oliveira, S.; Pires, C.; Ferreira, C. Does Recall Caregiv. Eat. Messages Exacerbate Pathog. Impact Shame Eat. Weight-Relat. Difficulties? Eat. Weight Disord. EWD 2020, 25, 471–480. [Google Scholar] [CrossRef] [PubMed]
- Troop, N.A.; Allan, S.; Serpell, L.; Treasure, J.L. Shame in women with a history of eating disorders. Eur. Eat. Disord. Rev. J. Eat. Disord. Assoc. 2008, 16, 480–488. [Google Scholar] [CrossRef] [PubMed]
- Losekam, S.; Kraeling, S.; Goetzky, B.; Rief, W.; Hilbert, A. Evaluation of the German version of the Perception of Teasing Scale (POTS). Unveröff. Manuskript. Univ. Marburg, 2017; unpublished. [Google Scholar]
- Thompson, J.K.; Cattarin, J.; Fowler, B.; Fisher, E. The Perception of Teasing Scale (POTS): A revision and extension of the Physical Appearance Related Teasing Scale (PARTS). J. Personal. Assess. 1995, 65, 146–157. [Google Scholar] [CrossRef]
- Löwe, B.; Spitzer, R.L.; Zipfel, S.; Herzog, W. PHQ_D. Gesundheitsfragebogen für Patienten. Manual. Komplettversion und Kurzform: Autorisierte Deutsche Version des “Prime MD Patient Health Questionnaire (PHQ)”. 2nd ed.; 2002. Available online: https://www.klinikum.uni-heidelberg.de/fileadmin/psychosomatische_klinik/download/phq_manual1.pdf (accessed on 8 January 2024).
- Löwe, B.; Spitzer, R.L.; Zipfel, S.; Herzog, W. PHQ-D. Gesundheitsfragebogen Für Patienten. Z. Für Med. Psychol. 2003, 12, 90–95. [Google Scholar]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B. Validation and utility of a self-report version of PRIME-MD: The PHQ primary care study. Primary care evaluation of mental disorders. Patient Health Questionnaire. JAMA 1999, 282, 1737–1744. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; Text Revision (DSM-IV-TR); American Psychiatric Association: Arlington, VA, USA, 2000. [Google Scholar]
- Durso, L.E.; Latner, J.D. Understanding self-directed stigma: Development of the weight bias internalization scale. Obesity 2008, 16 (Suppl. 2), S80–S86. [Google Scholar] [CrossRef] [PubMed]
- Hilbert, A.; Baldofski, S.; Zenger, M.; Löwe, B.; Kersting, A.; Braehler, E. Weight bias internalization scale: Psychometric properties and population norms. PLoS ONE 2014, 9, e86303. [Google Scholar] [CrossRef] [PubMed]
- Pearl, R.L.; Puhl, R.M. Measuring internalized weight attitudes across body weight categories: Validation of the modified weight bias internalization scale. Body Image 2014, 11, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Schraven, S.; Hübner, C.; Eichler, J.; Mansfeld, T.; Sander, J.; Seyfried, F.; Kaiser, S.; Dietrich, A.; Schmidt, R.; Hilbert, A. Psychometric properties of the WBIS/-M in a representative prebariatric sample–Evidence for a 10-item version. Obes. Facts, 2023; submitted. [Google Scholar]
- Fairburn, C.G.; Beglin, S.J. Assessment of eating disorders: Interview or self-report questionnaire? Int. J. Eat. Disord. 1994, 16, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Hilbert, A.; Tuschen-Caffier, B.; Karwautz, A.; Niederhofer, H.; Munsch, S. Eating Disorder Examination-Questionnaire. Diagnostica 2007, 53, 144–154. [Google Scholar] [CrossRef]
- Hrabosky, J.I.; Masheb, R.M.; White, M.A.; Grilo, C.M. Overvaluation of shape and weight in binge eating disorder. J. Consult. Clin. Psychol. 2007, 75, 175–180. [Google Scholar] [CrossRef]
- Grilo, C.M.; Hrabosky, J.I.; White, M.A.; Allison, K.C.; Stunkard, A.J.; Masheb, R.M. Overvaluation of shape and weight in binge eating disorder and overweight controls: Refinement of a diagnostic construct. J. Abnorm. Psychol. 2008, 117, 414–419. [Google Scholar] [CrossRef]
- Fritz, M.S.; Mackinnon, D.P. Required sample size to detect the mediated effect. Psychol. Sci. 2007, 18, 233–239. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach (Methodology in the Social Sciences); The Guilford Press: New York, NY, USA, 2022. [Google Scholar]
- Godoy-Izquierdo, D.; Lara, R.; Ogallar, A.; Rodríguez-Tadeo, A.; Ramírez, M.J.; Navarrón, E.; Arbinaga, F. Psychosocial and diet-related lifestyle clusters in overweight and obesity. Int. J. Environ. Res. Public Health 2021, 18, 6414. [Google Scholar] [CrossRef]
- Lawson, J.L.; Schuh, L.M.; Creel, D.B.; Blackinton, R.M.; Giambrone, S.A.; Grilo, C.M.; Ivezaj, V. Examining weight bias and loss-of-control eating among individuals seeking bariatric surgery. Obes. Surg. 2021, 27, 105–115. [Google Scholar] [CrossRef] [PubMed]
- White, M.A.; Kalarchian, M.A.; Levine, M.D.; Masheb, R.M.; Marcus, M.D.; Grilo, C.M. Prognostic significance of depressive symptoms on weight loss and psychosocial outcomes following gastric bypass surgery: A prospective 24-month follow-up study. Obes. Surg. 2015, 25, 1909–1916. [Google Scholar] [CrossRef] [PubMed]
- Lent, M.R.; Napolitano, M.A.; Wood, G.C.; Argyropoulos, G.; Gerhard, G.S.; Hayes, S.; Foster, G.D.; Collins, C.A.; Still, C.D. Internalized weight bias in weight-loss surgery patients: Psychosocial correlates and weight loss outcomes. Obes. Surg. 2014, 24, 195–2199. [Google Scholar] [CrossRef] [PubMed]
- Kruseman, M.; Leimgruber, A.; Zumbach, F.; Golay, A. Dietary, weight, and psychological changes among patients with obesity, 8 years after gastric bypass. J. Am. Diet. Assoc. 2010, 110, 527–534. [Google Scholar] [CrossRef] [PubMed]
- Curll, S.L.; Brown, P.M. Weight stigma and psychological distress: A moderated mediation model of social identification and internalised bias. Body Image 2020, 35, 207–216. [Google Scholar] [CrossRef] [PubMed]
- Levy, M.; Nguyen, A.; Kakinami, L.; Alberga, A.S. Weight bias internalization: Relationships with mental health, physical activity, and sedentary behavior. Stigma Health 2021, 8, 453–461. [Google Scholar] [CrossRef]
- Pearl, R.L.; Puhl, R.M.; Himmelstein, M.S.; Pinto, A.M.; Foster, G.D. Weight stigma and weight-related health: Associations of self-report measures among adults in weight management. Ann. Behav. Med. A Publ. Soc. Behav. Med. 2020, 54, 904–914. [Google Scholar] [CrossRef]
- Pearl, R.L.; Wadden, T.A.; Bach, C.; Tronieri, J.S.; Berkowitz, R.I. Six-month follow-up from a randomized controlled trial of the Weight BIAS Program. Obesity 2020, 28, 1878–1888. [Google Scholar] [CrossRef]
- Selensky, J.C.; Carels, R.A. Weight stigma and media: An examination of the effect of advertising campaigns on weight bias, internalized weight bias, self-esteem, body image, and affect. Body Image 2021, 36, 95–106. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | n | M/n | SD/% | Min. | Max. |
|---|---|---|---|---|---|
| Sociodemographic variables | |||||
| Age | 854 | 46.8 | 11.6 | 18 | 74 |
| Sex | 854 | ||||
| Women | 547 | 67.2 | |||
| Men | 280 | 32.8 | |||
| Marital status | 832 | ||||
| Single | 154 | 18.5 | |||
| Partnership | 160 | 19.2 | |||
| Married | 430 | 51.7 | |||
| Divorced | 63 | 7.6 | |||
| Widowed | 25 | 3.0 | |||
| Educational level | 759 | ||||
| ≤10 school years | 180 | 23.7 | |||
| >10 school years | 579 | 76.3 | |||
| Anthropometrics | |||||
| BMI, kg/m2 | 854 | 48.7 | 8.0 | 35.0 | 97.3 |
| Obesity class 2 | 100 | 11.7 | |||
| Obesity class 3 | 754 | 88.3 | |||
| Psychological variables | |||||
| POTS, 6–30 | 854 | 16.0 | 7.9 | 6.0 | 30.0 |
| WBIS, 1–7 | 854 | 4.8 | 1.3 | 1.3 | 7.0 |
| PHQ-D, 0–27 | 854 | 7.8 | 5.2 | 0.0 | 26.0 |
| EDE-Q WS, 0–6 | 854 | 3.7 | 1.1 | 0.0 | 6.0 |
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
|---|---|---|---|---|---|---|---|
| − | ||||||
| −0.11 ** | − | |||||
| −0.14 *** | −0.03 | − | ||||
| 0.02 | 0.11 ** | −0.11 ** | − | |||
| −0.36 *** | 0.11 ** | 0.29 *** | −0.01 | − | ||
| −0.17 *** | 0.17 *** | 0.09 * | −0.03 | 0.38 *** | − | |
| 0.01 | 0.09 ** | 0.14 *** | −0.05 | 0.27 *** | 0.56 *** | − |
| −0.03 | 0.19 *** | 0.09 | 0.01 | 0.33 *** | 0.72 *** | 0.56 *** |
| Path | Independent Variable | Dependent Variable | t | p | Direct Effect [95% CI] | Indirect Effect [95% CI] |
|---|---|---|---|---|---|---|
| a | POTS | WBIS | 10.206 | <0.001 | 0.06 [0.05, 0.07] | |
| b | WBIS | PHQ-D | 18.018 | <0.001 | 2.23 [2.01, 2.52] | |
| c | POTS | PHQ-D | 7.931 | <0.001 | 0.19 [0.15, 0.25] | |
| c’ | POTS | PHQ-D | 2.841 | 0.005 | 0.06 [0.03, 0.12] | 0.13 [0.10, 0.16] |
| WBIS (Mediator) | PHQ-D (Outcome) | |||||
|---|---|---|---|---|---|---|
| Effect [95% CI] | t | p | Effect [95% CI] | t | p | |
| Path a | ||||||
| POTS | 0.02 [0.01, 0.03] | 4.97 | <0.001 | |||
| EDE-Q WS | 0.74 [0.68, 0.79] | 26.99 | <0.001 | |||
| POTS × EDE-Q WS | −0.01 [−0.02, −0.00] | −3.08 | 0.002 | |||
| POTS × EDE-Q WS (−1 SD) | 0.03 [0.02, 0.04] | 5.37 | <0.001 | |||
| POTS × EDE-Q WS (mean) | 0.02 [0.01, 0.03] | 4.97 | <0.001 | |||
| POTS × EDE-Q WS (+1 SD) | 0.01 [−0.00, 0.02] | 1.86 | 0.063 | |||
| Age | −0.01 [−0.02, −0.01] | −4.21 | <0.001 | |||
| Sex | −0.01 [−0.13, 0.13] | −0.18 | 0.860 | |||
| BMI | −0.01 [−0.01, 0.00] | −1.35 | 0.177 | |||
| Path b | ||||||
| WBIS | 1.55 [1.29, 1.94] | 9.57 | <0.001 | |||
| EDE-Q WS | 1.38 [0.98, 1.70] | 7.77 | <0.001 | |||
| WBIS × EDE-Q WS | 0.49 [0.32, 0.72] | 5.01 | <0.001 | |||
| WBIS × EDE-Q WS (−1 SD) | 0.99 [0.63, 1.41] | 5.17 | <0.001 | |||
| WBIS × EDE-Q WS (mean) | 1.55 [1.29, 1.94] | 9.57 | <0.001 | |||
| WBIS × EDE-Q WS (+1 SD) | 2.11 [1.80, 2.62] | 10.45 | <0.001 | |||
| Age | 0.05 [0.02, 0.08] | 3.75 | <0.001 | |||
| Sex | −0.25 [−0.99, 0.22] | −0.84 | 0.399 | |||
| BMI | 0.05 [0.01, 0.08] | 2.83 | 0.005 | |||
| Path c’ | ||||||
| POTS | 0.03 [−0.00, 0.08] | 1.53 | 0.127 | |||
| POTS × EDE-Q WS | 0.03 [−0.01, 0.06] | 1.39 | 0.164 | |||
| Overall moderated mediation | ||||||
| POTS × WBIS × EDE-Q WS (−1 SD) | 0.03 [0.01, 0.05] | |||||
| POTS × WBIS × EDE-Q WS (mean) | 0.03 [0.02, 0.05] | |||||
| POTS × WBIS × EDE-Q WS (+1 SD) | 0.02 [−0.00, 0.04] | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fabrig, A.; Schmidt, R.; Mansfeld, T.; Sander, J.; Seyfried, F.; Kaiser, S.; Stroh, C.; Dietrich, A.; Hilbert, A. Depressive Symptoms among Bariatric Surgery Candidates: Associations with Stigmatization and Weight and Shape Concern. Nutrients 2024, 16, 510. https://doi.org/10.3390/nu16040510
Fabrig A, Schmidt R, Mansfeld T, Sander J, Seyfried F, Kaiser S, Stroh C, Dietrich A, Hilbert A. Depressive Symptoms among Bariatric Surgery Candidates: Associations with Stigmatization and Weight and Shape Concern. Nutrients. 2024; 16(4):510. https://doi.org/10.3390/nu16040510
Chicago/Turabian StyleFabrig, Alexandra, Ricarda Schmidt, Thomas Mansfeld, Johannes Sander, Florian Seyfried, Stefan Kaiser, Christine Stroh, Arne Dietrich, and Anja Hilbert. 2024. "Depressive Symptoms among Bariatric Surgery Candidates: Associations with Stigmatization and Weight and Shape Concern" Nutrients 16, no. 4: 510. https://doi.org/10.3390/nu16040510
APA StyleFabrig, A., Schmidt, R., Mansfeld, T., Sander, J., Seyfried, F., Kaiser, S., Stroh, C., Dietrich, A., & Hilbert, A. (2024). Depressive Symptoms among Bariatric Surgery Candidates: Associations with Stigmatization and Weight and Shape Concern. Nutrients, 16(4), 510. https://doi.org/10.3390/nu16040510