
Using Participatory Narrative Inquiry to Assess Experiences and Self-Experimentation with Diet Interventions in Inflammatory Bowel Disease Patients

 ,
, 
Highlights
- The findings of this study demonstrate that Participatory Narrative Inquiry (PNI) can be used to collect patient stories about self-experimentation with lifestyle changes in IBD.
- Patients identified rest, psychological balance, and dietary changes as key factors that improved their quality of life, although food experiences varied among individuals.
- Our findings suggest that personalized dietary guidance is essential to effectively support individuals with IBD.
Abstract
1. Introduction
2. Materials and Methods
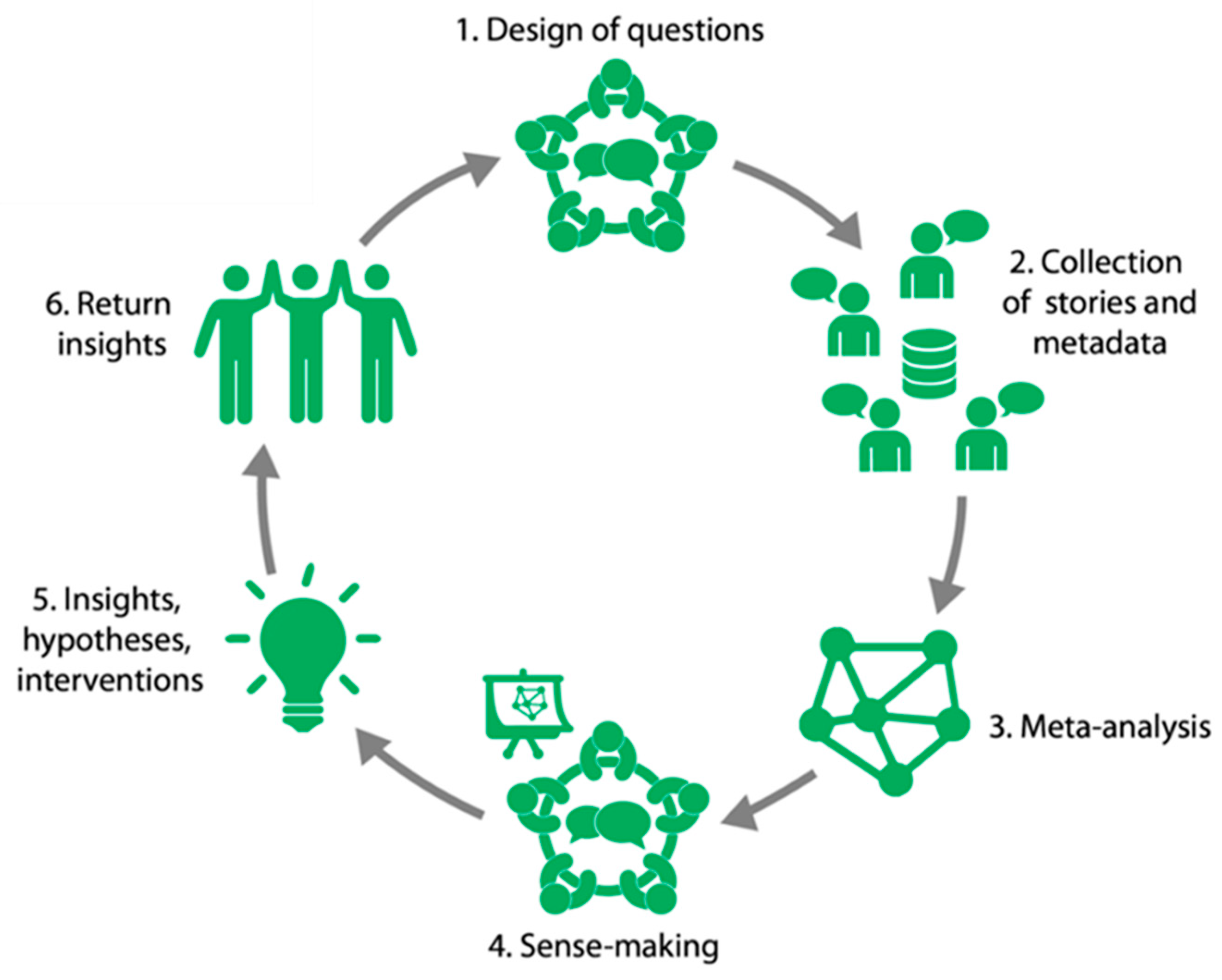
2.1. General Study Design
2.1.1. Design of Questions
Questions in Project Gut Feeling
| 1. Do you remember a time where you felt surprisingly good? What happened during that time? |
| 2. Could you tell something about a situation in which your symptoms were surprisingly less than usual? What happened during that time? |
| 3. Do you remember times where you changed something in your life that made you feel better, what happened? |
| 4. Do you want to tell about a situation in which your symptoms first increased and subsequently decreased, what happened? |
Questions in the Dietary Inquiry
| 1. What was the best experience you have ever had regarding the effect of food and drinks on your physical condition and well-being? What food and drink were involved? |
| 2. What was the worst experience you have ever had regarding the effect of food and drinks on your physical condition and well-being? What food and drinks were involved? |
| 3. Do you remember a change in your diet (including drinks) which made you feel better. What happened around that time and of what consisted this change? |
| 4. Do you remember a change in your diet (including drinks) which made you feel worse. What happened around that time and of what consisted this change? |
2.1.2. Collection of Stories and Meta-Data
2.1.3. Meta-Analysis
2.1.4. Sense-Making
- A message for IBD patients;
- A message for gastroenterologists, specialized nurses, and dietitians;
- A message for researchers.
2.1.5. Insights, Hypotheses, and Interventions
2.1.6. Return Insights
3. Results
3.1. Gut Feeling
3.1.1. Meta-Data Demographics
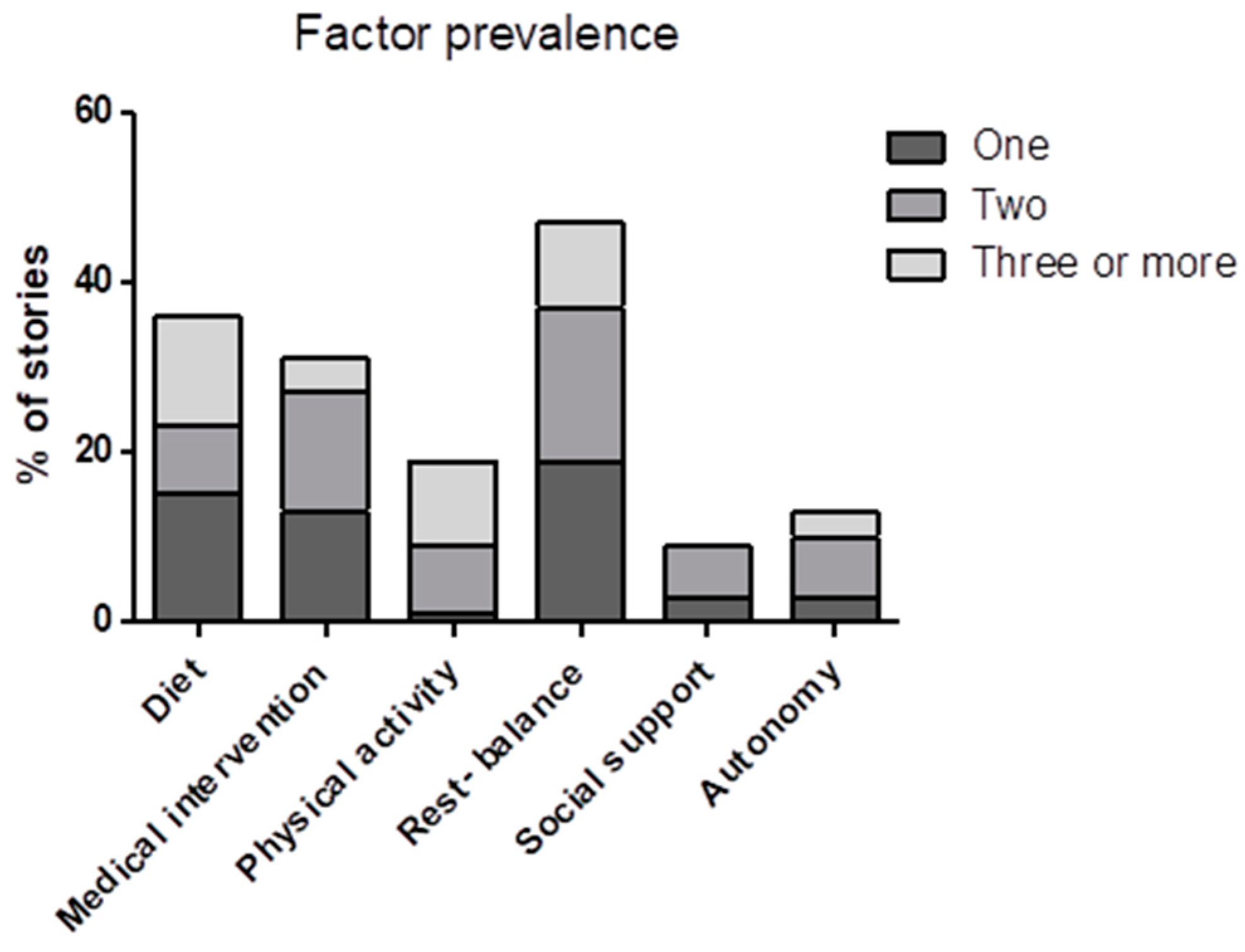
3.1.2. Prevalence of Factors in Patient Experiences
3.1.3. Meta-Data Patient Interpretation
3.1.4. Change in Diet and IBD
3.2. The Dietary Inquiry
3.2.1. Meta-Data Demographics
3.2.2. Prevalence of Dietary Factors in Patient Experiences
3.2.3. Participant Quotes
4. Discussion
4.1. Lessons Learned for Future Use of PNI
4.2. Messages That Emerged from the Stories
- The most frequent factors that were mentioned by participants when describing times when they experienced a better QoL were rest and (psychological) balance and a change in diet.
- Participants described the effects of dietary changes on the QoL they experienced in terms of a reduction in symptoms such as abdominal pain, fatigue, and defecation problems.
- The message to researchers is to conduct more research on the effects of the top five food products on IBD symptoms. When the possible effects on IBD symptoms are known, a patient, together with a dietician, can find an individual diet that suits his or her needs while still taking in sufficient essential nutrients and not overdosing on others.
- A considerable number of food products were experienced as beneficial by one person and detrimental by another. This is shown in Supplementary Table S1, and results in the message that personalized dietary guidance is needed that supports the individual.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| PNI | Participatory Narrative Inquiry |
| QoL | Quality of Life |
References
- Knowles, S.R.; Graff, L.A.; Wilding, H.; Hewitt, C.; Keefer, L.; Mikocka-Walus, A. Quality of Life in Inflammatory Bowel Disease: A Systematic Review and Meta-analyses-Part I. Inflamm. Bowel Dis. 2018, 24, 742–751. [Google Scholar] [CrossRef] [PubMed]
- Knowles, S.R.; Keefer, L.; Wilding, H.; Hewitt, C.; Graff, L.A.; Mikocka-Walus, A. Quality of Life in Inflammatory Bowel Disease: A Systematic Review and Meta-analyses-Part II. Inflamm. Bowel Dis. 2018, 24, 966–976. [Google Scholar] [CrossRef] [PubMed]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.C.E.; Parkes, G.C.; Selinger, C.; et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 2019, 68 (Suppl. 3), s1–s106. [Google Scholar] [CrossRef] [PubMed]
- Krzystek-Korpacka, M.; Kempinski, R.; Bromke, M.; Neubauer, K. Biochemical Biomarkers of Mucosal Healing for Inflammatory Bowel Disease in Adults. Diagnostics 2020, 10, 367. [Google Scholar] [CrossRef]
- Sagami, S.; Kobayashi, T.; Miyatani, Y.; Okabayashi, S.; Yamazaki, H.; Takada, T.; Kinoshita, K.; Allocca, M.; Kunisaki, R.; Ramaswamy, P.K.; et al. Accuracy of Ultrasound for Evaluation of Colorectal Segments in Patients With Inflammatory Bowel Diseases: A Systematic Review and Meta-analysis. Clin. Gastroenterol. Hepatol. 2021, 19, 908–921.e6. [Google Scholar] [CrossRef]
- Huber, M.; Knottnerus, J.A.; Green, L.; Horst, H.V.D.; Jadad, A.R.; Kromhout, D.; Leonard, B.; Lorig, K.; Loureiro, M.I.; Meer, J.W.M.V.D.; et al. How should we define health? BMJ 2011, 343, d4163. [Google Scholar] [CrossRef]
- Sudhakar, P.; Wellens, J.; Verstockt, B.; Ferrante, M.; Sabino, J.; Vermeire, S. Holistic healthcare in inflammatory bowel disease: Time for patient-centric approaches? Gut 2023, 72, 192–204. [Google Scholar] [CrossRef]
- Hou, J.K.; Lee, D.; Lewis, J. Diet and inflammatory bowel disease: Review of patient-targeted recommendations. Clin. Gastroenterol. Hepatol. 2014, 12, 1592–1600. [Google Scholar] [CrossRef] [PubMed]
- Levine, A.; Wine, E.; Assa, A.; Boneh, R.S.; Shaoul, R.; Kori, M.; Cohen, S.; Peleg, S.; Shamaly, H.; On, A.; et al. Crohn’s Disease Exclusion Diet Plus Partial Enteral Nutrition Induces Sustained Remission in a Randomized Controlled Trial. Gastroenterology 2019, 157, 440–450.e8. [Google Scholar] [CrossRef]
- Limketkai, B.N.; Iheozor-Ejiofor, Z.; Gjuladin-Hellon, T.; Parian, A.; Matarese, L.E.; Bracewell, K.; MacDonald, J.K.; Gordon, M.; Mullin, G.E. Dietary interventions for induction and maintenance of remission in inflammatory bowel disease. Cochrane Database Syst. Rev. 2019, 2, CD012839. [Google Scholar] [CrossRef] [PubMed]
- Khalili, H.; Chan, S.S.M.; Lochhead, P.; Ananthakrishnan, A.N.; Hart, A.R.; Chan, A.T. The role of diet in the aetiopathogenesis of inflammatory bowel disease. Nat. Rev. Gastroenterol. Hepatol. 2018, 15, 525–535. [Google Scholar] [CrossRef] [PubMed]
- Sinopoulou, V.; Gordon, M.; Akobeng, A.K.; Gasparetto, M.; Sammaan, M.; Vasiliou, J.; Dovey, T.M. Interventions for the management of abdominal pain in Crohn’s disease and inflammatory bowel disease. Cochrane Database Syst. Rev. 2021, 11, CD013531. [Google Scholar] [CrossRef] [PubMed]
- de Vries, J.H.M.; Dijkhuizen, M.; Tap, P.; Witteman, B.J.M. Patient’s Dietary Beliefs and Behaviours in Inflammatory Bowel Disease. Dig. Dis. 2019, 37, 131–139. [Google Scholar] [CrossRef] [PubMed]
- Limdi, J.K.; Aggarwal, D.; McLaughlin, J.T. Dietary Practices and Beliefs in Patients with Inflammatory Bowel Disease. Inflamm. Bowel Dis. 2016, 22, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Zallot, C.; Quilliot, D.; Chevaux, J.-B.; Peyrin-Biroulet, C.; Guéant-Rodriguez, R.M.; Freling, E.; Collet-Fenetrier, B.; Williet, N.; Ziegler, O.; Bigard, M.-A.; et al. Dietary beliefs and behavior among inflammatory bowel disease patients. Inflamm. Bowel Dis. 2013, 19, 66–72. [Google Scholar] [CrossRef]
- Velde, A.A.T.; Bezema, T.; van Kampen, A.H.C.; Kraneveld, A.D.; Hart, B.A.; van Middendorp, H.; Hack, E.C.; van Montfrans, J.M.; Belzer, C.; Jans-Beken, L.; et al. Embracing Complexity beyond Systems Medicine: A New Approach to Chronic Immune Disorders. Front. Immunol. 2016, 7, 587. [Google Scholar] [CrossRef]
- Woods, A. The limits of narrative: Provocations for the medical humanities. Med. Humanit. 2011, 37, 73–78. [Google Scholar] [CrossRef]
- Fioretti, C.; Mazzocco, K.; Riva, S.; Oliveri, S.; Masiero, M.; Pravettoni, G. Research studies on patients’ illness experience using the Narrative Medicine approach: A systematic review. BMJ Open 2016, 6, e011220. [Google Scholar] [CrossRef]
- Kurtz, C. Working with Stories in Your Community or Organization: Participatory Narrative Inquiry, 3rd ed.; Kurtz-Fernhout Publishing: New York, NY, USA, 2014. [Google Scholar]
- Huber, M.; van Vliet, M.; Giezenberg, M.; Winkens, B.; Heerkens, Y.; Dagnelie, P.C.; Knottnerus, J.A. Towards a ‘patient-centred’ operationalisation of the new dynamic concept of health: A mixed methods study. BMJ Open 2016, 6, e010091. [Google Scholar] [CrossRef]
- Sturmberg, J.P.; Picard, M.; Aron, D.C.; Bennett, J.M.; Bircher, J.; Dehaven, M.J.; Gijzel, S.M.W.; Heng, H.H.; Marcum, J.A.; Martin, C.M.; et al. Health and Disease-Emergent States Resulting from Adaptive Social and Biological Network Interactions. Front. Med. 2019, 6, 59. [Google Scholar] [CrossRef]
- de Jong, M.J.; Huibregtse, R.; Masclee, A.A.M.; Jonkers, D.; Pierik, M.J. Patient-Reported Outcome Measures for Use in Clinical Trials and Clinical Practice in Inflammatory Bowel Diseases: A Systematic Review. Clin. Gastroenterol. Hepatol. 2018, 16, 648–663.e3. [Google Scholar] [CrossRef]
- Calvino-Suarez, C.; Ferreiro-Iglesias, R.; Baston-Rey, I.; Barreiro-de Acosta, M. Role of Quality of Life as Endpoint for Inflammatory Bowel Disease Treatment. Int. J. Environ. Res. Public Health 2021, 18, 7159. [Google Scholar] [CrossRef] [PubMed]
- Sturmberg, J.P. Evidence-based medicine-Not a panacea for the problems of a complex adaptive world. J. Eval. Clin. Pract. 2019, 25, 706–716. [Google Scholar] [CrossRef] [PubMed]
- Barros, V.J.d.S.; Severo, J.S.; Mendes, P.H.M.; da Silva, A.C.A.; de Oliveira, K.B.V.; Parente, J.M.L.; Lima, M.M.; Neto, E.M.M.; dos Santos, A.A.; Tolentino, M. Effect of dietary interventions on inflammatory biomarkers of inflammatory bowel diseases: A systematic review of clinical trials. Nutrition 2021, 91–92, 111457. [Google Scholar] [CrossRef] [PubMed]
- Lane, E.R.; Lee, D.; Suskind, D.L. Dietary Therapies in Pediatric Inflammatory Bowel Disease: An Evolving Inflammatory Bowel Disease Paradigm. Gastroenterol. Clin. N. Am. 2017, 46, 731–744. [Google Scholar] [CrossRef]
- Levine, A.; Rhodes, J.M.; Lindsay, J.O.; Abreu, M.T.; Kamm, M.A.; Gibson, P.R.; Gasche, C.; Silverberg, M.S.; Mahadevan, U.; Boneh, R.S.; et al. Dietary Guidance From the International Organization for the Study of Inflammatory Bowel Diseases. Clin. Gastroenterol. Hepatol. 2020, 18, 1381–1392. [Google Scholar] [CrossRef]
- Yanai, H.; Levine, A.; Hirsch, A.; Boneh, R.S.; Kopylov, U.; Eran, H.B.; Cohen, N.A.; Ron, Y.; Goren, I.; Leibovitzh, H.; et al. The Crohn’s disease exclusion diet for induction and maintenance of remission in adults with mild-to-moderate Crohn’s disease (CDED-AD): An open-label, pilot, randomised trial. Lancet Gastroenterol. Hepatol. 2021, 7, 49–59. [Google Scholar] [CrossRef]
- Boneh, R.S.; Van Limbergen, J.; Wine, E.; Assa, A.; Shaoul, R.; Milman, P.; Cohen, S.; Kori, M.; Peleg, S.; On, A.; et al. Dietary Therapies Induce Rapid Response and Remission in Pediatric Patients With Active Crohn’s Disease. Clin. Gastroenterol. Hepatol. 2021, 19, 752–759. [Google Scholar] [CrossRef]
- Peters, V.; Spooren, C.E.G.M.; Pierik, M.J.; Weersma, R.K.; van Dullemen, H.M.; Festen, E.A.M.; Visschedijk, M.C.; Masclee, A.A.M.; Hendrix, E.M.B.; Almeida, R.J.; et al. Dietary Intake Pattern is Associated with Occurrence of Flares in IBD Patients. J. Crohns Colitis 2021, 15, 1305–1315. [Google Scholar] [CrossRef]
- Castro, F.; de Souza, H.S.P. Dietary Composition and Effects in Inflammatory Bowel Disease. Nutrients 2019, 11, 1398. [Google Scholar] [CrossRef]
- Marion-Letellier, R.; Savoye, G.; Ghosh, S. IBD: In Food We Trust. J. Crohns Colitis 2016, 10, 1351–1361. [Google Scholar] [CrossRef] [PubMed]
- Sandys, O.; Te Velde, A. Raising the Alarm: Environmental Factors in the Onset and Maintenance of Chronic (Low-Grade) Inflammation in the Gastrointestinal Tract. Dig. Dis Sci. 2022, 67, 4355–4368. [Google Scholar] [CrossRef]
- Vissers, E.; Wellens, J.; Sabino, J. Ultra-processed foods as a possible culprit for the rising prevalence of inflammatory bowel diseases. Front. Med. 2022, 9, 1058373. [Google Scholar] [CrossRef] [PubMed]
- Godala, M.; Gaszynska, E.; Zatorski, H.; Malecka-Wojciesko, E. Dietary Interventions in Inflammatory Bowel Disease. Nutrients 2022, 14, 4261. [Google Scholar] [CrossRef]
- Wexler, A. Mapping the Landscape of Do-it-Yourself Medicine. Citiz Sci. 2022, 7, 38. [Google Scholar] [CrossRef] [PubMed]
- Anderson, C. Presenting and evaluating qualitative research. Am. J. Pharm. Educ. 2010, 74, 141. [Google Scholar] [CrossRef]
- Leung, L. Validity, reliability, and generalizability in qualitative research. J. Fam. Med. Prim. Care 2015, 4, 324–327. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Blanck, H.M.; Garfield, K.M.; Wassung, A.; Petersen, R. A Food is Medicine approach to achieve nutrition security and improve health. Nat. Med. 2022, 28, 2238–2240. [Google Scholar] [CrossRef] [PubMed]
- Ogilvie, D.; Adams, J.; Bauman, A.; Gregg, E.W.; Panter, J.; Siegel, K.R.; Wareham, N.J.; White, M. Using natural experimental studies to guide public health action: Turning the evidence-based medicine paradigm on its head. J. Epidemiol. Community Health 2020, 74, 203–208. [Google Scholar] [CrossRef]
- Sandys, O.; Stokkers, P.C.F.; Te Velde, A. DAMP-ING IBD: Extinguish the fire and prevent smoldering. Dig. Dis. Sci. 2024. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Questions About the Participant | Questions About the Story |
|---|---|
| Age | Timeframe in which the effect was observed |
| Gender | Symptom(s) described |
| Disease type | Factors that changed |
| Habitat | Rural or urban |
| Use of medication | Yes/no |
| Questions About Participant | Questions About the Story |
|---|---|
| Age | Timeframe in which the effect of the food occurred |
| Gender | Symptom(s) described |
| Disease type | Dietary factors that changed |
| Comorbidities | Whether it contained improvement or deterioration |
| Category of the food products described | |
| Whether medication was changed; if yes, what the change consisted of |
| 1. Rest and psychological balance (45%) |
| 2. Change in diet (34%) |
| 3. Medical intervention (via treating physician) (32%) |
| 4. More physical activity (19%) |
| 5. Patient autonomy (12%) |
| 6. Social support (8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hos, C.; Tebbens, M.; Bezema, T.; Bosch, J.A.; Kraneveld, A.D.; Spooren, C.E.G.M.; de Haas, M.C.; Stokkers, P.C.F.; Duijvestein, M.; Bouma, G.; et al. Using Participatory Narrative Inquiry to Assess Experiences and Self-Experimentation with Diet Interventions in Inflammatory Bowel Disease Patients. Nutrients 2024, 16, 4027. https://doi.org/10.3390/nu16234027
Hos C, Tebbens M, Bezema T, Bosch JA, Kraneveld AD, Spooren CEGM, de Haas MC, Stokkers PCF, Duijvestein M, Bouma G, et al. Using Participatory Narrative Inquiry to Assess Experiences and Self-Experimentation with Diet Interventions in Inflammatory Bowel Disease Patients. Nutrients. 2024; 16(23):4027. https://doi.org/10.3390/nu16234027
Chicago/Turabian StyleHos, Celine, Merel Tebbens, Tjitske Bezema, Jos A. Bosch, Aletta D. Kraneveld, Corinne E. G. M. Spooren, Marie Claire de Haas, Pieter C. F. Stokkers, Marjolijn Duijvestein, Gerd Bouma, and et al. 2024. "Using Participatory Narrative Inquiry to Assess Experiences and Self-Experimentation with Diet Interventions in Inflammatory Bowel Disease Patients" Nutrients 16, no. 23: 4027. https://doi.org/10.3390/nu16234027
APA StyleHos, C., Tebbens, M., Bezema, T., Bosch, J. A., Kraneveld, A. D., Spooren, C. E. G. M., de Haas, M. C., Stokkers, P. C. F., Duijvestein, M., Bouma, G., & te Velde, A. A. (2024). Using Participatory Narrative Inquiry to Assess Experiences and Self-Experimentation with Diet Interventions in Inflammatory Bowel Disease Patients. Nutrients, 16(23), 4027. https://doi.org/10.3390/nu16234027