Abstract
Aim: To investigate the routine guidance provided by pediatricians concerning the timing of complementary feeding (CF) for both healthy infants and those at a heightened risk of allergies. Methods: A total of 233 pediatricians participated in an anonymous online survey that included questions about demographics and recommendations for CF. Specifically, they provided guidance on the types of foods, preparation methods, supplements, time intervals for introducing new foods to infants at low and high allergy risk, and delayed food introductions for high-risk cases. Results: The respondents advised introducing certain foods at specific ages: fruits, starchy non-gluten grains, vegetables, olive oil, and meat were appropriate at 6 months; gluten-rich grains at 7 months; yogurt, hard-boiled eggs, and legumes at 8 months; fish at 8.5 months; and nuts at 9 months. Pediatricians, especially those with less than 15 years of practice, often introduced egg, seafood, gluten-rich grains, legumes, and nuts earlier for high-risk infants. Parenthood and male gender were associated with the earlier introduction of eggs and grains. Conclusions: Greek pediatricians follow a structured food introduction schedule for CF in infants. Interestingly, they tend to delay the introduction of common food allergens and recommend longer intervals between introducing new foods, particularly for high-risk infants. Key Notes: Despite recent evidence-based indications on healthy complementary feeding strategies for infants, discrepancies persist among pediatricians regarding food choices and the order and timing of food introduction, both for healthy infants and those at risk of allergy. Guidance on complementary feeding by pediatricians is influenced by their individual characteristics. Pediatricians tend to delay the introduction of common food allergens and recommend longer intervals between introducing new foods, particularly for high-risk infants.
1. Introduction
For infants, the transition from a milk-based diet to solid foods is important for healthy psychosomatic development [1,2,3,4,5] and plays a determining role in the future dietary variety of the child [6,7].
Complementary feeding (CF) in exclusively breastfed infants is recommended at approximately 6 months. In formula-fed infants, this should begin not before 17 weeks and not later than 26 weeks of age [4,8].
Delayed introduction of allergenic foods was recommended in the past based on the theory that the immature gut is more permeable, allowing food proteins to enter the bloodstream intact and potentially increasing the risk of developments of food allergy (FA) [9]. A recent shift towards earlier introduction, from 4 months onwards [10], followed the results of large-scale interventional studies in the general population [11] and in infants at high risk for allergy [12,13,14,15,16,17], although the results of both observational and interventional studies are conflicting [18,19,20,21].
Consequently, the specific time point for initiating CF remains an individual decision of pediatricians, one based on the overall development of the infant and the personal and family history of allergy [22,23,24,25,26].
Pronounced differences between pediatricians are reported regarding their guidance in terms of allergy prevention for both healthy infants and those at risk of allergy [27]. The period they recommend between the introduction of two new foods parallels the personal convictions of the pediatricians about allergy prevention, ranging from 2–3 days for healthy infants to more than 4 days for infants considered at high risk of allergy [1,2]. The Canadian Pediatric Society (CPS) recommends a flexible approach in which foods not included in the list of main allergens are introduced freely, with a time interval of a few days between new foods only observed for food allergens. Allergen-related foods should be introduced one at a time to identify more easily the causative food of a possible allergic reaction [28].
In this study, we aimed to investigate (a) the routine CF guidance for healthy infants provided by pediatricians practicing in different areas in Greece, (b) the differences in their recommendations for infants at high risk of allergy in terms of food introduction order, and (c) their recommended time period between the introduction of new foods.
2. Methods
2.1. Participants
Greek pediatricians registered with the Hellenic Pediatric Society (n~2000 members) were invited via e-mail to participate in this study from May to December 2022. A detailed introductory informative text regarding the scope of the study was provided, and online informed consent was provided by each participant. After this, they accessed the online study questionnaire using a personalized code.
The study was approved by the Education Department of the 6th Health Region of Greece (study ID 3111/18.03.2022) and conducted in accordance with the code of Ethics of the World Medical Association Declaration of Helsinki.
2.2. Questionnaire
A questionnaire was developed for the purposes of the study ([link to Supplementary material]) and responses were gathered online using a purpose-built web platform, hosted by the International Hellenic University, which secured on-premises collection and analysis of data. For inclusion in the analysis, pediatricians were required to confirm ongoing or completed pediatric training, and to complete the questionnaire up to and including the final question.
The questionnaire included anonymous demographic information on the participant: sex, age, pediatric subspecialty, years of experience, place of work, marital status, and parental status.
The main questionnaire was divided into three sections with user-friendly multi-part ranking questions. In these, participants were asked to select foods from each food category (Section 1), as well as different cooking methods (Section 2) and food supplements (Section 3), and arrange them in the order that they usually recommend for introduction into the infant’s diet, proceeding according to month of age, given from birth to 18 months.
Each section was followed by an open-ended question for adding food items, cooking methods and food supplements not included in the list, respectively.
The time period between the introduction of new foods was explored for infants at both low and high risk of allergies, and an open-ended question recorded the foods for which introduction was delayed for infants at high risk of allergy. Completion of all sections and questions of the questionnaire was mandatory.
The questionnaire was piloted with a small number of pediatricians (n = 23) to ensure that the requested information was clearly formulated and that the responses were appropriate. The average time required for completion, based on the piloting data, was 18 min.
2.3. Statistical Analysis
The normality of distribution of continuous variables was assessed via the Kolmogorov–Smirnov test. Continuous variables were expressed as median (interquartile range), and comparisons were conducted using the non-parametric Mann–Whitney U test. Categorical variables were expressed as n (percentage %) and compared using the chi-square test or Fisher’s exact test. Univariate analysis was conducted on respondents’ dichotomous categorical data: sex (male, female), years of experience (<15 years, ≥15 years), location of practice (urban, rural/semi-urban), parenthood (yes, no), and subspecialty (yes, no), and the time of introduction (months of age) of each food.
Multivariate logistic regression analysis was utilized to explore the association of the characteristics of the pediatricians with the time (early, late) of food introduction and the time period between the introduction of new foods for infants at low risk and high risk of allergy. Foods introduced late into the diet of infants at high risk of allergy were examined in the models, as follows: >7 months for wheat products and trahanas (frumenty); >8 months for hard-boiled egg, cream cheese, tomato, orange, kiwi or strawberry; >9 months for soft egg/omelet/fried egg; 10 months for cows-milk yogurt; and 12 months for all other foods [12,29,30,31]. The time period between introduction of new foods was considered low if ≤3 days and high if >4 days [27].
All tests were two-sided, and a p-value of <0.05 was considered statistically significant (alpha = 0.05). The data were analyzed using SPSS Statistics (IBM SPSS Statistics for Windows, Version 24.0, Armonk, NY, USA).
3. Results
3.1. Participants
Of the ~2000 pediatricians invited to participate, 348 submitted responses (response rate 17.4%), of which 233 questionnaires were fully completed and were included in the final data analysis (11.65%). Of the final participants, 75.96% were female, 44.63% were based in an urban area, and 85.83% were parents; 51.9% had working experience as pediatricians of ≥15 years, and a pediatric subspecialty had been attained by 25.32% (Supplementary Table S1).
3.2. Infant Feeding Practices: The Order of Introduction of Solid Food Recommended by the Pediatricians
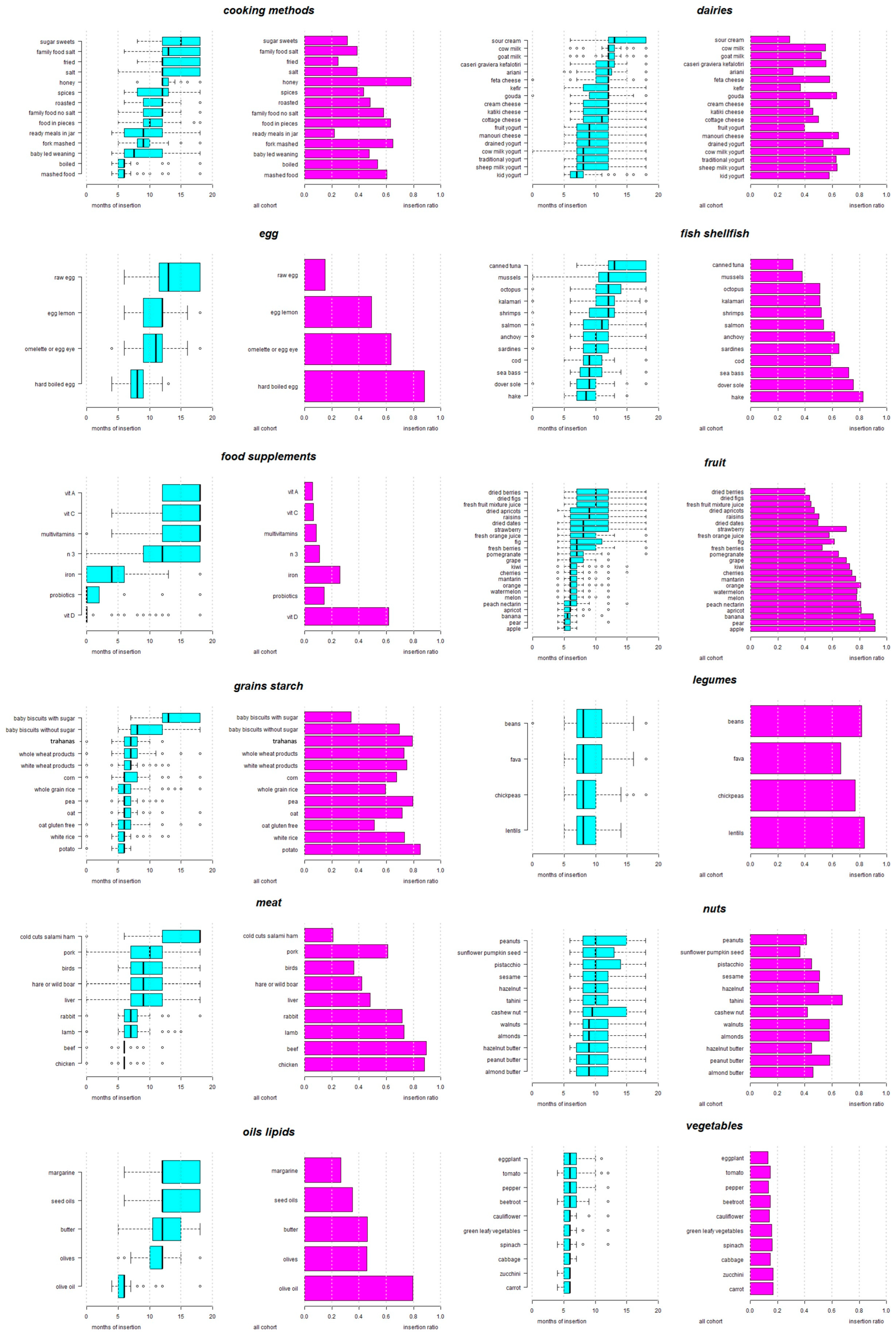
Figure 1 and Supplementary Table S2 present the responses of the pediatricians regarding the usual guidance for the CF of infants that they provide to parents. Fruits are the first food to be introduced into the infant’s diet, starting at 5 months with apple and pear, followed by banana, apricot, peach, and nectarine, and then by orange, melon, watermelon, and kiwi. Grapes, pomegranate, fresh berries, and figs follow, while strawberries, dried fruits and fresh juices are suggested after 8 months (Figure 1).
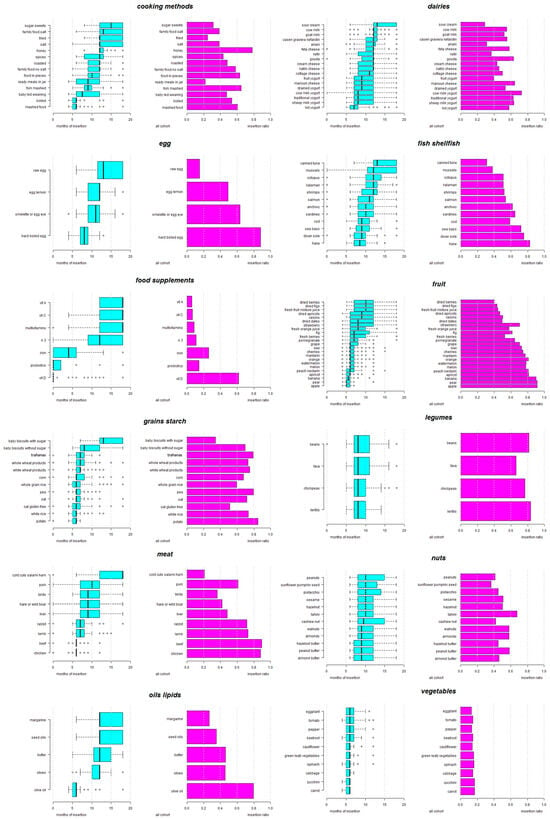
Figure 1.
Usual guidance on complementary feeding provided by pediatricians. Months of age that the study pediatricians usually recommend for the insertion of the respective food into the infant’s diet. Insertion ratio represents the rate of respondents that selected the specific food in relation to the overall study pediatricians.
Starchy gluten-free products are recommended at 5–6 months in the form of potato, white rice and gluten-free oats, followed by oats without a gluten-free indication, whole-grain rice, peas, and corn. White-wheat (gluten-rich) products are recommended at 6–7 months, and whole-wheat products and trahanas (frumenty) at 6–8 months.
A variety of vegetables, including carrot, zucchini, cabbage, spinach, green leafy vegetables, cauliflower and beetroot, are introduced at 5–6 months, and peppers, tomato, and eggplant are included slightly later.
Olive oil is introduced at 5–6 months, and olives, seed oils and margarine after 12 months. Regarding animal products, chicken and beef are recommended at 6 months, followed by lamb and rabbit. Then liver, hare, wild boar and game birds, and finally pork, are included at 7–12 months, and processed meats (cold cuts, salami and ham) are suggested at 12–18 months.
Regarding dairy products, pediatricians suggest kids’ yogurt at 6–8 months, traditional or sheep’s or cow’s milk yogurt at 7–12 months, manouri (soft) cheese at 7.25–12 months, cottage cheese at 8–12 months, and other cheese types and butter after 12 months.
Hard-boiled egg is introduced at 8 months, while other forms of egg follow later, with soft egg/omelet/fried egg and egg-lemon sauce at 9–12 months and raw egg at 11.5–18 months.
Among legumes, lentils and chickpeas are introduced first (7–10 months), with fava and regular beans slightly later.
Regarding fish, hake is introduced at 7–10 months, followed by other fish species. Shellfish are suggested after the 12th month, with canned tuna at 12–18 months.
Nuts are introduced first in the form of almond, peanut, or hazelnut butter at 7–12 months, followed by ground nuts and seeds, such as almonds, walnuts, sesame, pistachios, sunflower/pumpkin seeds, and peanuts, after 10 months.
Regarding cooking and preparation methods, the pediatricians recommend that food should be consumed first boiled and mashed at 5–6 months, followed by fork-mashed food at 8–10 months, and food in pieces at 9–12 months. Baby-led weaning (BLW) is recommended by some at 6–12 months. Sharing family food without salt is suggested at 9–12 months, and with salt at 12–18 months, and with roasted or fried food, salt and spices included in the infant’s diet after 12 months, in addition to honey, sugar and other sweet substances.
3.3. The Influence of Years of Pediatric Practice on the Order of Food Introduction
Pediatricians with more years of practice (≥15 years) introduce certain food items, including raisins, fresh mixed fruit juice and white rice, and food supplements, such as omega-3, vitamin C and multivitamins, earlier. Conversely, pediatricians with <15 years of practice introduce earlier various types of meat products (rabbit, beef and pork), soft and raw egg, cow’s milk and yogurt, legumes, and various fish and shellfish species (anchovy, calamari and octopus) (Table 1).

Table 1.
Month of age of recommendation of complementary food introduction according to the years of pediatric experience.
3.4. The Influence of Sex of the Pediatrician on the Order of Food Introduction
Male pediatricians recommend the earlier introduction of certain fruit (kiwi, pomegranate and raisins), dairy products (yogurt, Greek soft cheese and ariani), and baby biscuits with sugar. Female pediatricians suggest the earlier introduction of soft egg, olive oil and boiled and mashed food into the infant’s diet (Table 2).
Table 2.
Month of age of recommendation of complementary food introduction according to the sex of the pediatrician.
3.5. The Influence of the Area of Practice on the Order of Food Introduction
Pediatricians practicing in rural and semi-urban areas introduce rabbit, ariani, hazelnut, and iron supplements earlier, while they delay the introduction of hard yellow cheese (kasseri/graviera/kefalotyri) in comparison to those practicing in urban areas (Supplementary Table S3).
3.6. The Influence of Parenthood on the Order of Food Introduction
Pediatricians with children of their own are more likely to recommend the earlier introduction of certain fruits, such as cherries and fresh orange juice, whole-wheat and white-wheat products and fork-mashed food, but to delay BLW and the introduction of cottage cheese, in comparison to non-parents (Supplementary Table S4).
3.7. Differences in Recommendations of Pediatricians on Food Introduction, according to High and Low Risk of Allergy
For infants at high risk of allergy, some pediatricians reported that they recommend delaying the introduction of certain items, specifically, orange (16%), kiwi (21%), strawberry (43%), gluten-rich wheat products (12%), milk and dairy products (49%), all forms of egg (59%), peanuts (57%), tree-nuts (62%), legumes (62%), fish and shellfish (48%), beef (0.4%), and soya (0.4%).
Regression models, created to explore the characteristics of the pediatricians that may predict the earlier introduction of the above-mentioned foods, showed that a shorter period of practice in pediatrics, lack of a subspecialty, parenthood and sex all differentiated the age of recommended introduction of the above foods (Table 3).
Table 3.
Regression model of the factors that contribute to earlier recommendation by the pediatrician of introduction of specific foods in the infant’s diet.
3.8. Factors Associated with Recommendation of a Longer Time Period between Introduction of New Foods
Applying the regression model on the factors influencing the recommended time period between the introduction of new foods (Table 4) showed that male pediatricians recommended a longer time period between introduction of new foods (>4 days) in infants at low risk of allergy. For infants at high risk of allergy, a lack of a subspecialty and practicing in a rural/semi-urban area were predictors of a longer time period between the introduction of new foods, as shown in Table 4.
Table 4.
Regression model of the factors that contribute to a longer time period (>4 days) between the introduction of new foods in the infant’s diet.
4. Discussion
Knowledge accumulated from a variety of studies provides evidence of the benefits of healthy CF strategies in infancy for the promotion of balanced, lifelong dietary habits [32], with avoidance of obesity [33] and malnutrition [34], and a reduction in food allergies (FAs) [35,36]. In several countries, including Greece, practicing pediatricians play an important role in choosing the most suitable CF approach for guiding parents in the introduction of new foods into their infants’ diets [25]. This study is the first to our knowledge to evaluate the typical guidance on CF strategies provided by practicing pediatricians in relation to their individual characteristics. The findings reveal that the recommendations of the Greek pediatricians show similarities with the Italian infant feeding practices [37,38], in proposing that fruits, cereals, and vegetables should be introduced first. Conversely, in a US study, cereals were reported to be the first CF [27]. Notably, the Greek pediatricians show variation, and according to their individual characteristics, they may delay the introduction of several common food allergens into the diet of infants at both low and high risk of allergy and may increase the time period between the introduction of new foods for infants at high risk of allergy.
The variations do not always conform with current guidelines; specifically, Greek pediatricians suggest the introduction of gluten-containing products at around the 7th month, although the WHO guidelines [1,2,3] recommend inclusion between the 4th and the 7th months in small portions. It is also proposed that breastfed infants should continue breastfeeding for at least 2–3 weeks [8,39], while gluten consumption must be continuous up to the 1st year, in predisposed individuals [4], to reduce the risk of celiac disease [40,41], although one randomized trial suggested that the late introduction of gluten-rich foods might not increase the risk of celiac disease [41].
Among the gluten-rich foods, Greek pediatricians recommend introduction into the infant diet of trahanas (frumenty), a traditional fermented food produced from cracked wheat and milk [42]. The fermentation of dairy products has been proposed as a method of reducing allergenicity [43] and has been used effectively to increase tolerance in children with milk allergy [44]. Koksal and colleagues have proposed that pregnant and lactating mothers should consume trahanas and other fermented dairy products to protect their infants from cow’s milk allergy [45]. Greek pediatricians practicing in urban areas tended to delay slightly the introduction of other fermented dairy products, such as traditional yogurt, suggesting their introduction at around the 1st year of age for low-risk infants, or even later for infants at high risk of allergy.
Pediatricians practicing in rural/semi-urban areas recommend the earlier introduction of local dairy products, such as ariani—a fermentation product known to benefit the gut microflora and the immune system [46]. This group of pediatricians also recommends the early introduction of meat from domestic animals, such as rabbit, and game meat, as well as sesame, tree nuts, seafood, legumes and tomato, probably because of their local availability [47,48]. Residency in rural/semi-urban environments has thus been proposed as a factor that increases adherence to traditional dietary patterns and provides wider food diversity in comparison to urban environments [49].
Practicing in rural/semi-urban areas, however, along with lack of a subspecialty, were correlated with recommendation by the pediatricians of a longer time period between the introduction of new foods for infants at high risk for allergy. Studies on extended time periods between new foods suggested by pediatricians have emphasized the possible detrimental effects of delays in food introduction on dietary diversity in infancy [27], and its possible relationship with an increased risk of pediatric asthma and allergies [50,51,52,53].
Greek pediatricians in this study recommend the early introduction of sources of highly bioavailable iron into the infants’ diet at 6 months, such as red- and white-meat products. These are crucial to covering their iron needs [3] and preventing iron deficiency in exclusively breastfed infants [54].
They suggest delaying the introduction of ultra-processed meats, such as cold cuts and salami, until 18 months. Increased consumption of ultra-processed foods (UPF) has been correlated with wheezing [55], raised IgE levels, current asthma, and eczema during childhood [56]. In their responses, the female pediatricians paid more attention to food processing and cooking methods, while the male professionals suggested earlier introduction of fresh fruits and dairy products. In a relevant US study, male pediatricians provided more specific guidance than females to parents regarding healthy eating, including avoidance of sugar, enhancing fruit and vegetable variety, and exposure to many tastes and textures, while the females focused more on overall healthy eating and living [57].
Male sex emerged as a predictor for recommendation of longer time periods (>4 days) between new foods for infants at low risk of allergy. In line with our findings, female pediatricians [58] and those with less years of practice appeared, in previous studies, better informed regarding the implementation of guidelines on the appropriate timing of introduction of known allergens to prevent food allergy [59]. In this study, we found that female pediatricians recommended wider food variety earlier, including common food allergens, and foods considered to be triggers of symptoms in children with atopic dermatitis, such as kiwi, strawberry, and tomato [35,60,61]. On the other hand, pediatricians with more years of practice recommended fresh fruits and white rice earlier, in line with past standard recommendations [62].
Pediatricians’ decisions regarding CF are undoubtedly influenced by their own family habits [63,64], traditional approaches [65,66], and new trends, including BLW weaning [7,24,67,68]. Parenthood was correlated with earlier recommendation by the pediatricians to introduce cow’s milk, delay introduction of wheat products, and implement BLW. BLW was an early feeding method, more often promoted by pediatricians with fewer years of practice and non-parents. Although BLW has been proposed as a method for reducing food fussiness and increasing food enjoyment and satiety responsiveness [69], it should be accompanied by appropriate education of the parents, as it may increase the risk of dietary deficiencies in important nutrients, such as zinc [70], or pose a choking hazard [71].
5. Limitations
The current study has certain limitations. The data are based on self-reported responses, a mode of assessment that can increase response bias, which we tried to minimize by ensuring the anonymity of the respondents. The response rate was 17.4%, with only 11.65% fully completed questionnaires. This rate was similar to that in other research studies conducted by distributing the questionnaire via e-mail [27,72], but carries the risk of respondent bias. Finally, due to the nature of our study, which focused on general recommendations, specific information pertaining to individual infants and their interactions with pediatricians was not collected. Subsequent research could explore the specific guidance provided in a dyad mode, investigating the nuanced interactions between pediatricians and individual infants to enhance our understanding of tailored recommendations.
6. Conclusions
This study of pediatricians revealed that, in their routine practice, they appear to follow a food introduction schedule when providing guidance for CF of infants. They tend to delay the introduction of known food allergens, and to recommend a longer time period between introduction of new foods for infants at high risk of allergy. In view of the reported benefits of healthy CF for infants at both low and high risk of allergy, pediatricians should keep well informed of research outcomes and implement relevant guidelines effectively.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/nu16020239/s1, Table S1: Demographic characteristics of the study participants; Table S2; Age of Introduction of Solid Food as Recommended by the Pediatricians; Table S3: Differences based on location of practice; Table S4: Differences based on parentship; Table S5: DEPENDENT VARIABLE: ALMONDS/ALMOND BUTTER; Table S6: Multivariate regression Analysis to evaluate the association of different factors with the time and the waiting period for food introduction of various foods in low- and high-risk children. Questionare.
Author Contributions
E.V. conception, design, investigation, interpretation of the results, wrote the first draft; E.V., S.T., G.F., I.P., G.P.M., C.A., N.D., Z.E. and E.S.: data collection and interpretation; D.R., J.L., Z.E.: data interpretation and analysis; All: edit and approve final manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Education Department of the 6th Health Region of Greece (study ID 3111/18.03.2022, 18 March 2022).
Informed Consent Statement
Participants provided informed consent before completing the online questionnaire.
Data Availability Statement
Data is contained within the article (and supplementary materials).
Acknowledgments
We would like to express our gratitude to the Greek Paediatric Allergy Society Executive Committee for their support to spread the questionnaire to potential participants.
Conflicts of Interest
The authors have no conflicts of interest to disclose.
References
- World Health Organization. Complementary Feeding. 2023. Available online: https://www.who.int/health-topics/complementary-feeding#tab=tab_1 (accessed on 10 September 2023).
- CDC (Centers for Disease Control and Prevention). Weaning. Nutrition. Available online: https://www.cdc.gov/nutrition/InfantandToddlerNutrition/breastfeeding/weaning.html (accessed on 10 September 2023).
- Greek Ministry of Health. Recommendations for the Introduction of Solid Foods in the 1st Year of Life. 2018. Available online: https://www.moh.gov.gr/articles/health/dieythynsh-dhmosias-ygieinhs/metadotika-kai-mh-metadotika-noshmata/c388-egkyklioi/5750-systaseis-gia-thn-eisagwgh-sterewn-trofwn-ston-1o-xrono-ths-zwhs (accessed on 10 September 2023).
- Agostoni, C.; Decsi, T.; Fewtrell, M.; Goulet, O.; Kolacek, S.; Koletzko, B.; Michaelsen, K.F.; Moreno, L.; Puntis, J.; Rigo, J.; et al. Complementary feeding: A commentary by the espghan committee on nutrition. J. Pediatr. Gastroenterol. Nutr. 2008, 46, 99–110. [Google Scholar] [CrossRef] [PubMed]
- Lutter, C.K.; Grummer-Strawn, L.; Rogers, L. Complementary feeding of infants and young children 6 to 23 months of age. Nutr. Rev. 2021, 79, 825–846. [Google Scholar] [CrossRef] [PubMed]
- Alvisi, P.; Congiu, M.; Ficara, M.; De Gregorio, P.; Ghio, R.; Spisni, E.; Di Saverio, P.; Labriola, F.; Lacorte, D.; Lionetti, P. Complementary feeding in italy: From tradition to innovation. Children 2021, 8, 638. [Google Scholar] [CrossRef] [PubMed]
- D’Auria, E.; Bergamini, M.; Staiano, A.; Banderali, G.; Pendezza, E.; Penagini, F.; Zuccotti, G.V.; Peroni, D.G. Baby-led weaning: What a systematic review of the literature adds on. Ital. J. Pediatr. 2018, 44, 49. [Google Scholar] [CrossRef]
- Fewtrell, M.; Bronsky, J.; Campoy, C.; Domellöf, M.; Embleton, N.; Mis, N.F.; Hojsak, I.; Hulst, J.M.; Indrio, F.; Lapillonne, A.; et al. Complementary feeding: A position paper by the european society for paediatric gastroenterology, hepatology, and nutrition (espghan) committee on nutrition. J. Pediatr. Gastroenterol. Nutr. 2017, 64, 119–132. [Google Scholar] [CrossRef]
- Devonshire, A.L.; Robison, R.G. Prevention of food allergy. Allergy Asthma Proc. 2019, 40, 450–452. [Google Scholar] [CrossRef]
- Prescott, S.L.; Smith, P.; Tang, M.; Palmer, D.J.; Sinn, J.; Huntley, S.J.; Cormack, B.; Heine, R.G.; Gibson, R.A.; Makrides, M. The importance of early complementary feeding in the development of oral tolerance: Concerns and controversies. Pediatr. Allergy Immunol. 2008, 19, 375–380. [Google Scholar] [CrossRef]
- Perkin, M.R.; Logan, K.; Tseng, A.; Raji, B.; Ayis, S.; Peacock, J.; Brough, H.; Marrs, T.; Radulovic, S.; Craven, J.; et al. Randomized trial of introduction of allergenic foods in breast-fed infants. N. Engl. J. Med. 2016, 374, 1733–1743. [Google Scholar] [CrossRef]
- Du Toit, G.; Roberts, G.; Sayre, P.H.; Bahnson, H.T.; Radulovic, S.; Santos, A.F.; Brough, H.A.; Phippard, D.; Basting, M.; Feeney, M.; et al. Randomized trial of peanut consumption in infants at risk for peanut allergy. N. Engl. J. Med. 2015, 372, 803–813. [Google Scholar] [CrossRef]
- Bellach, J.; Schwarz, V.; Ahrens, B.; Trendelenburg, V.; Aksünger, Ö.; Kalb, B.; Niggemann, B.; Keil, T.; Beyer, K. Randomized placebo-controlled trial of hen’s egg consumption for primary prevention in infants. J. Allergy Clin. Immunol. 2017, 139, 1591–1599.e2. [Google Scholar] [CrossRef]
- Palmer, D.J.; Metcalfe, J.; Makrides, M.; Gold, M.S.; Quinn, P.; West, C.E.; Loh, R.; Prescott, S.L. Early regular egg exposure in infants with eczema: A randomized controlled trial. J. Allergy Clin. Immunol. 2013, 132, 387–392.e1. [Google Scholar] [CrossRef] [PubMed]
- Palmer, D.J.; Sullivan, T.R.; Gold, M.S.; Prescott, S.L.; Makrides, M. Randomized controlled trial of early regular egg intake to prevent egg allergy. J. Allergy Clin. Immunol. 2017, 139, 1600–1607.e2. [Google Scholar] [CrossRef] [PubMed]
- Tan, W.-L.; Valerio, C.; Barnes, E.H.; Turner, P.J.; Van Asperen, P.A.; Kakakios, A.M.; Campbell, D.E. A randomized trial of egg introduction from 4 months of age in infants at risk for egg allergy. J. Allergy Clin. Immunol. 2017, 139, 1621–1628.e8. [Google Scholar] [CrossRef]
- Natsume, O.; Kabashima, S.; Nakazato, J.; Yamamoto-Hanada, K.; Narita, M.; Kondo, M.; Saito, M.; Kishino, A.; Takimoto, T.; Inoue, E.; et al. Two-step egg introduction for prevention of egg allergy in high-risk infants with eczema (petit): A randomised, double-blind, placebo-controlled trial. Lancet 2017, 389, 276–286. [Google Scholar] [CrossRef]
- Hesselmar, B.; Saalman, R.; Rudin, A.; Adlerberth, I.; Wold, A. Early fish introduction is associated with less eczema, but not sensitization, in infants. Acta Paediatr. 2010, 99, 1861–1867. [Google Scholar] [CrossRef] [PubMed]
- Papamichael, M.M.; Shrestha, S.K.; Itsiopoulos, C.; Erbas, B. The role of fish intake on asthma in children: A meta-analysis of observational studies. Pediatr. Allergy Immunol. 2018, 29, 350–360. [Google Scholar] [CrossRef] [PubMed]
- Ierodiakonou, D.; Garcia-Larsen, V.; Logan, A.; Groome, A.; Cunha, S.; Chivinge, J.; Robinson, Z.; Geoghegan, N.; Jarrold, K.; Reeves, T.; et al. Timing of allergenic food introduction to the infant diet and risk of allergic or autoimmune disease: A systematic review and meta-analysis. JAMA 2016, 316, 1181–1192. [Google Scholar] [CrossRef]
- Scarpone, R.; Kimkool, P.; Ierodiakonou, D.; Leonardi-Bee, J.; Garcia-Larsen, V.; Perkin, M.R.; Boyle, R.J. Timing of allergenic food introduction and risk of immunoglobulin e–mediated food allergy: A systematic review and meta-analysis. JAMA Pediatr. 2023, 177, 489–497. [Google Scholar] [CrossRef]
- Venter, C.; Pereira, B.; Voigt, K.; Grundy, J.; Clayton, C.B.; Higgins, B.; Arshad, S.H.; Dean, T. Factors associated with maternal dietary intake, feeding and weaning practices, and the development of food hypersensitivity in the infant. Pediatr. Allergy Immunol. 2009, 20, 320–327. [Google Scholar] [CrossRef]
- Sellen, D.W. Evolution of infant and young child feeding: Implications for contemporary public health. Annu. Rev. Nutr. 2007, 27, 123–148. [Google Scholar] [CrossRef]
- Borowitz, S.M. First bites-why, when, and what solid foods to feed infants. Front. Pediatr. 2021, 9, 654171. [Google Scholar] [CrossRef]
- Nuzzi, G.; Gerini, C.; Comberiati, P.; Peroni, D.G. The weaning practices: A new challenge for pediatricians? Pediatr. Allergy Immunol. 2022, 33 (Suppl. S27), 44–46. [Google Scholar] [CrossRef] [PubMed]
- King, C. An evidence based guide to weaning preterm infants. Paediatr. Child Health 2009, 19, 405–414. [Google Scholar] [CrossRef]
- Samady, W.; Campbell, E.; Aktas, O.N.; Jiang, J.; Bozen, A.; Fierstein, J.L.; Joyce, A.H.; Gupta, R.S. Recommendations on complementary food introduction among pediatric practitioners. JAMA Netw. Open 2020, 3, e2013070. [Google Scholar] [CrossRef] [PubMed]
- Grueger, B. Weaning from the breast. Paediatr. Child Health 2013, 18, 210–211. [Google Scholar] [CrossRef] [PubMed]
- Koplin, J.J.; Osborne, N.J.; Wake, M.; Martin, P.E.; Gurrin, L.C.; Robinson, M.N.; Tey, D.; Slaa, M.; Thiele, L.; Miles, L.; et al. Can early introduction of egg prevent egg allergy in infants? A population-based study. J. Allergy Clin. Immunol. 2010, 126, 807–813. [Google Scholar] [CrossRef]
- de Lauzon-Guillain, B.; Jones, L.; Oliveira, A.; Moschonis, G.; Betoko, A.; Lopes, C.; Moreira, P.; Manios, Y.; Papadopoulos, N.G.; Emmett, P.; et al. The influence of early feeding practices on fruit and vegetable intake among preschool children in 4 european birth cohorts. Am. J. Clin. Nutr. 2013, 98, 804–812. [Google Scholar] [CrossRef] [PubMed]
- Romero-Velarde, E.; Villalpando-carrion, S.; Pérez-Lizaur, A.B.; Iracheta-Gerez, M.D.L.L.; Alonso-Rivera, C.G.; López-Navarrete, G.E.; García-Contreras, A.A.; Ochoa-Ortiz, E.; Zárate-mondragón, F.; López-Pérez, G.T.; et al. Guidelines for complementary feeding in healthy infants. Boletín Médico Hosp. Infant. México 2016, 73, 338–356. [Google Scholar] [CrossRef]
- Scaglioni, S.; De Cosmi, V.; Ciappolino, V.; Parazzini, F.; Brambilla, P.; Agostoni, C. Factors influencing children’s eating behaviours. Nutrients 2018, 10, 706. [Google Scholar] [CrossRef]
- Mameli, C.; Mazzantini, S.; Zuccotti, G.V. Nutrition in the first 1000 days: The origin of childhood obesity. Int. J. Environ. Res. Public Health 2016, 13, 838. [Google Scholar] [CrossRef]
- Ajmal, S.; Ajmal, L.; Ajmal, M.; Nawaz, G. Association of malnutrition with weaning practices among infants in pakistan. Cureus 2022, 14, e31018. [Google Scholar] [CrossRef] [PubMed]
- Trogen, B.; Jacobs, S.; Nowak-Wegrzyn, A. Early introduction of allergenic foods and the prevention of food allergy. Nutrients 2022, 14, 2565. [Google Scholar] [CrossRef] [PubMed]
- Ferraro, V.; Zanconato, S.; Carraro, S. Timing of food introduction and the risk of food allergy. Nutrients 2019, 11, 1131. [Google Scholar] [CrossRef] [PubMed]
- Giovannini, M.; Riva, E.; Banderali, G.; Scaglioni, S.; Veehof, S.; Sala, M.; Radaelli, G.; Agostoni, C. Feeding practices of infants through the first year of life in italy. Acta Paediatr. 2004, 93, 492–497. [Google Scholar] [CrossRef] [PubMed]
- Caroli, M.; Mele, R.M.; Tomaselli, M.A.; Cammisa, M.; Longo, F.; Attolini, E. Complementary feeding patterns in europe with a special focus on italy. Nutr. Metab. Cardiovasc. Dis. 2012, 22, 813–818. [Google Scholar] [CrossRef] [PubMed]
- Guandalini, S. The influence of gluten: Weaning recommendations for healthy children and children at risk for celiac disease. Nestle Nutr. Workshop Ser. Pediatr. Program. 2007, 60, 139–155. [Google Scholar] [CrossRef]
- Logan, K.; Perkin, M.R.; Marrs, T.; Radulovic, S.; Craven, J.; Flohr, C.; Bahnson, H.T.; Lack, G. Early gluten introduction and celiac disease in the eat study: A prespecified analysis of the eat randomized clinical trial. JAMA Pediatr. 2020, 174, 1041–1047. [Google Scholar] [CrossRef]
- Hall, A.; Meisenheimer, E.S.; Marshall, R.C. Can early introduction of gluten reduce risk of celiac disease? J. Fam. Pract. 2022, 71, E4–E6. [Google Scholar] [CrossRef]
- Lazos, E.S.; Aggelousis, G.; Bratakos, M. The fermentation of trahanas: A milk-wheat flour combination. Plant Foods Hum. Human. Nutr. 1993, 44, 45–62. [Google Scholar] [CrossRef]
- El Mecherfi, K.-E.; Todorov, S.D.; de Albuquerque, M.A.C.; Denery-Papini, S.; Lupi, R.; Haertlé, T.; de Melo Franco, B.D.G.; Larré, C. Allergenicity of fermented foods: Emphasis on seeds protein-based products. Foods 2020, 9, 792. [Google Scholar] [CrossRef]
- Uncuoglu, A.; Yologlu, N.; Simsek, I.E.; Uyan, Z.S.; Aydogan, M. Tolerance to baked and fermented cow’s milk in children with ige-mediated and non-ige-mediated cow’s milk allergy in patients under two years of age. Allergol. Immunopathol. 2017, 45, 560–566. [Google Scholar] [CrossRef] [PubMed]
- Koksal, Z.G.; Uysal, P.; Mercan, A.; Bese, S.A.; Erge, D. Does maternal fermented dairy products consumption protect against cow’s milk protein allergy in toddlers? Ann. Allergy Asthma Immunol. 2023, 130, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Okoniewski, A.; Dobrzyńska, M.; Kusyk, P.; Dziedzic, K.; Przysławski, J.; Drzymała-Czyż, S. The role of fermented dairy products on gut microbiota composition. Fermentation 2023, 9, 231. [Google Scholar] [CrossRef]
- Bustillos, B.; Sharkey, J.R.; Anding, J.; McIntosh, A. Availability of more healthful food alternatives in traditional, convenience, and nontraditional types of food stores in two rural texas counties. J. Am. Diet. Assoc. 2009, 109, 883–889. [Google Scholar] [CrossRef] [PubMed]
- Pachón, H.; Simondon, K.B.; Fall, S.T.; Menon, P.; Ruel, M.T.; Hotz, C.; Creed-Kanashiro, H.; Arce, B.; Domínguez, M.R.; Frongillo, E.A.; et al. Constraints on the delivery of animal-source foods to infants and young children: Case studies from five countries. Food Nutr. Bull. 2007, 28, 215–229. [Google Scholar] [CrossRef]
- Casari, S.; Di Paola, M.; Banci, E.; Diallo, S.; Scarallo, L.; Renzo, S.; Gori, A.; Renzi, S.; Paci, M.; de Mast, Q.; et al. Changing dietary habits: The impact of urbanization and rising socio-economic status in families from burkina faso in sub-saharan africa. Nutrients 2022, 14, 1782. [Google Scholar] [CrossRef]
- Roduit, C.; Frei, R.; Depner, M.; Schaub, B.; Loss, G.; Genuneit, J.; Pfefferle, P.; Hyvärinen, A.; Karvonen, A.M.; Riedler, J.; et al. Increased food diversity in the first year of life is inversely associated with allergic diseases. J. Allergy Clin. Immunol. 2014, 133, 1056–1064. [Google Scholar] [CrossRef]
- Roduit, C.; Frei, R.; Loss, G.; Büchele, G.; Weber, J.; Depner, M.; Loeliger, S.; Dalphin, M.L.; Roponen, M.; Hyvärinen, A.; et al. Development of atopic dermatitis according to age of onset and association with early-life exposures. J. Allergy Clin. Immunol. 2012, 130, 130–136.e5. [Google Scholar] [CrossRef]
- Nwaru, B.I.; Erkkola, M.; Ahonen, S.; Kaila, M.; Haapala, A.M.; Kronberg-Kippilä, C.; Salmelin, R.; Veijola, R.; Ilonen, J.; Simell, O.; et al. Age at the introduction of solid foods during the first year and allergic sensitization at age 5 years. Pediatrics 2010, 125, 50–59. [Google Scholar] [CrossRef]
- Nwaru, B.I.; Takkinen, H.M.; Niemelä, O.; Kaila, M.; Erkkola, M.; Ahonen, S.; Haapala, A.M.; Kenward, M.G.; Pekkanen, J.; Lahesmaa, R.; et al. Timing of infant feeding in relation to childhood asthma and allergic diseases. J. Allergy Clin. Immunol. 2013, 131, 78–86. [Google Scholar] [CrossRef]
- Palmeira, P.; Carneiro-Sampaio, M. Immunology of breast milk. Rev. Assoc. Med. Bras. 2016, 62, 584–593. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Galarraga, L.; Martín-Álvarez, I.; Fernández-Montero, A.; Rocha, B.S.; Barea, E.C.; Martín-Calvo, N. Consumption of ultra-processed products and wheezing respiratory diseases in children: The sendo project. Anales de Pediatría (Engl. Ed.) 2021, 95, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Kong, W.; Xie, Y.; Zhong, J.; Cao, C. Ultra-processed foods and allergic symptoms among children and adults in the united states: A population-based analysis of nhanes 2005–2006. Front. Public Health 2022, 10, 1038141. [Google Scholar] [CrossRef] [PubMed]
- Boundy, E.O.; Boyd, A.F.; Hamner, H.C.; Belay, B.; Liebhart, J.L.; Lindros, J.; Hassink, S.; Frintner, M.P. Us pediatrician practices on early nutrition, feeding, and growth. J. Nutr. Educ. Behav. 2020, 52, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.S.; Bilaver, L.A.; Johnson, J.L.; Hu, J.W.; Jiang, J.; Bozen, A.; Martin, J.; Reese, J.; Cooper, S.F.; Davis, M.M.; et al. Assessment of pediatrician awareness and implementation of the addendum guidelines for the prevention of peanut allergy in the united states. JAMA Netw. Open 2020, 3, e2010511. [Google Scholar] [CrossRef] [PubMed]
- Leo, S.; Dean, J.; Chan, E.S. What are the beliefs of pediatricians and dietitians regarding complementary food introduction to prevent allergy? Allergy Asthma Clin. Immunol. 2012, 8, 3. [Google Scholar] [CrossRef]
- Elbert, N.J.; Jong, J.C.K.-D.; Voortman, T.; Nijsten, T.E.C.; de Jong, N.W.; Jaddoe, V.W.V.; de Jongste, J.C.; van Wijk, R.G.; Duijts, L.; Pasmans, S.G.M.A. Allergenic food introduction and risk of childhood atopic diseases. PLoS ONE 2017, 12, e0187999. [Google Scholar] [CrossRef]
- Li, S.K.; Liu, Z.; Huang, C.K.; Wu, T.C.; Huang, C.F. Prevalence, clinical presentation, and associated atopic diseases of pediatric fruit and vegetable allergy: A population-based study. Pediatr. Neonatol. 2022, 63, 520–526. [Google Scholar] [CrossRef]
- Kleinman, R.E.; Coletta, F.A. Historical overview of transitional feeding recommendations and vegetable feeding practices for infants and young children. Nutr. Today 2016, 51, 7–13. [Google Scholar] [CrossRef]
- Baldassarre, M.E.; Palladino, V.; Amoruso, A.; Pindinelli, S.; Mastromarino, P.; Fanelli, M.; Di Mauro, A.; Laforgia, N. Rationale of probiotic supplementation during pregnancy and neonatal period. Nutrients 2018, 10, 1693. [Google Scholar] [CrossRef]
- Simeone, G.; Bergamini, M.; Verga, M.C.; Cuomo, B.; D’Antonio, G.; Iacono, I.D.; Mauro, D.D.; Mauro, F.D.; Mauro, G.D.; Leonardi, L.; et al. Do vegetarian diets provide adequate nutrient intake during complementary feeding? A systematic review. Nutrients 2022, 14, 3591. [Google Scholar] [CrossRef] [PubMed]
- Calamaro, C.J. Infant nutrition in the first year of life: Tradition or science? Pediatr. Nurs. 2000, 26, 211–215. [Google Scholar] [PubMed]
- Dembiński, Ł.; Banaszkiewicz, A.; Dereń, K.; Pituch-Zdanowska, A.; Jackowska, T.; Walkowiak, J.; Mazur, A. Exploring physicians’ perspectives on the introduction of complementary foods to infants and toddlers. Nutrients 2021, 13, 3559. [Google Scholar] [CrossRef] [PubMed]
- Białek-Dratwa, A.; Kowalski, O.; Szczepańska, E. Traditional complementary feeding or blw (baby led weaning) method?—A cross-sectional study of polish infants during complementary feeding. Front. Pediatr. 2022, 10, 992244. [Google Scholar] [CrossRef]
- Brown, A.; Jones, S.W.; Rowan, H. Baby-led weaning: The evidence to date. Curr. Nutr. Rep. 2017, 6, 148–156. [Google Scholar] [CrossRef]
- Boswell, N. Complementary feeding methods-a review of the benefits and risks. Int. J. Environ. Res. Public Health 2021, 18, 7165. [Google Scholar] [CrossRef]
- Białek-Dratwa, A.; Soczewka, M.; Grajek, M.; Szczepańska, E.; Kowalski, O. Use of the baby-led weaning (blw) method in complementary feeding of the infant-a cross-sectional study of mothers using and not using the blw method. Nutrients 2022, 14, 2372. [Google Scholar] [CrossRef]
- Committee on Injury, Violence, and Poison Prevention. Prevention of choking among children. Pediatrics 2010, 125, 601–607. [Google Scholar] [CrossRef]
- Golnik, A.; Ireland, M.; Borowsky, I.W. Medical homes for children with autism: A physician survey. Pediatrics 2009, 123, 966–971. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).