
Conceptualizing an Integrative Multiple Myeloma Care: The Role of Nutrition, Supplements, and Complementary Modalities

Abstract
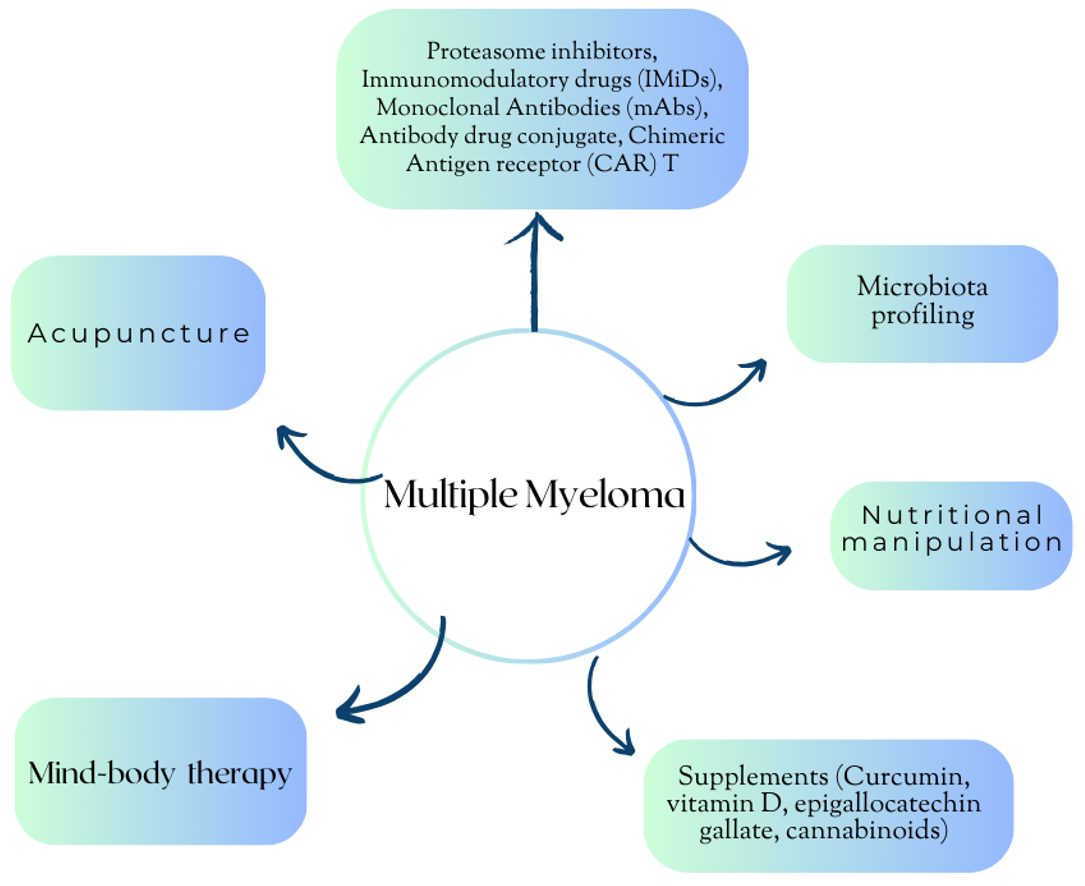
1. Introduction
2. Nutrition, Lifestyle Changes and Microbiota
2.1. Nutrition, Lifestyle Changes, and the Link with Pathogenesis and Progression of MM
2.2. Obesity, Sarcopenia, and MM
2.3. The Role of Microbiota in the Pathogenesis and Treatment of MM
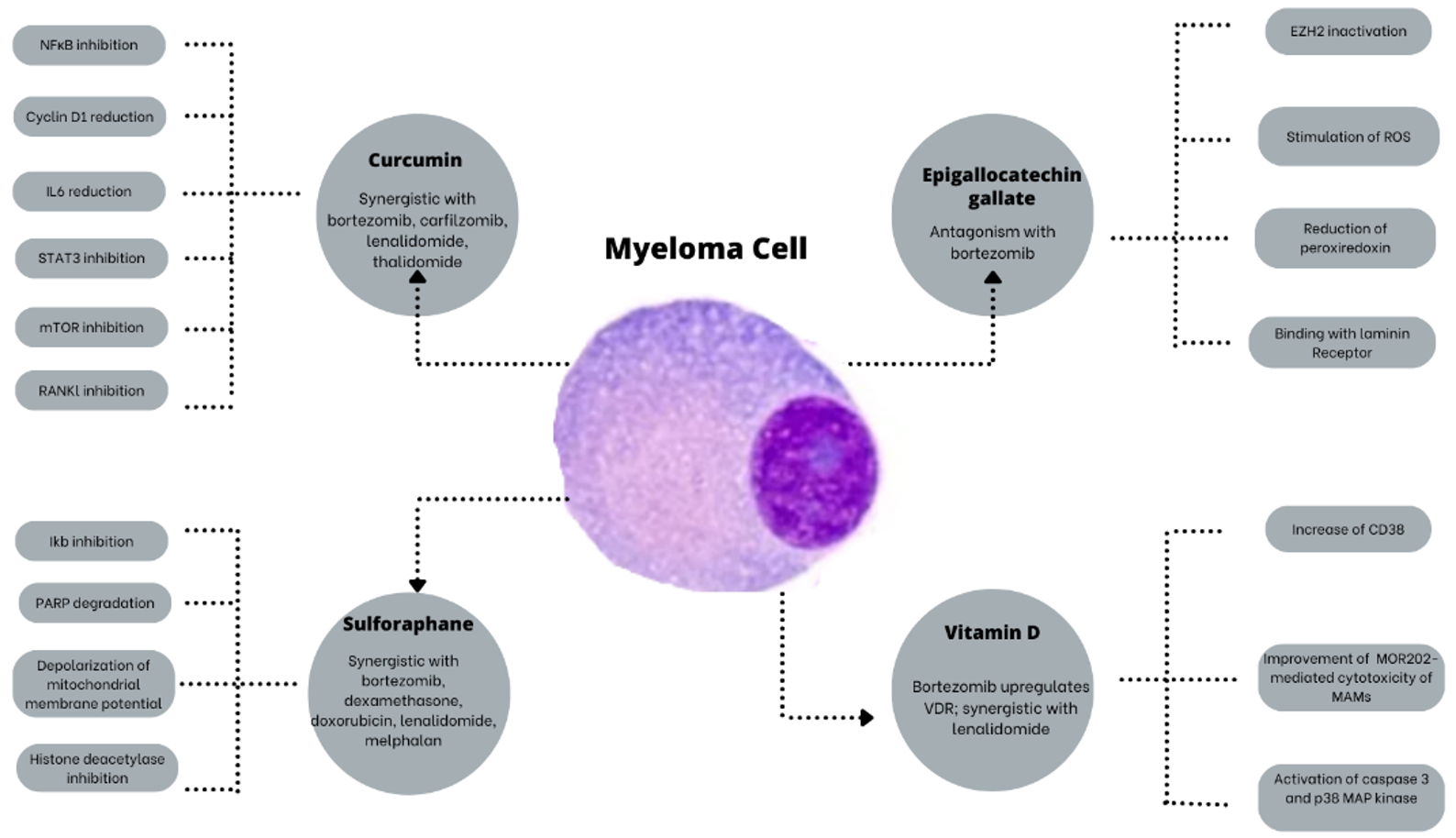
3. Natural Compounds and Vitamins: Their Potential Role in the Treatment of MM
3.1. Curcumin
3.2. Epigallocatechin Gallate (EGCG)
3.3. Vitamin D
3.4. Others
4. Acupuncture
5. Mind–Body Medicine
6. Discussion
7. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ASCO | American Society of Clinical Oncology |
| ASCT | Autologous stem cell transplantation |
| BIPN | Bortezomib-induced peripheral neuropathy |
| CAR-T | Chimeric Antigen Receptor T cell |
| CB1 | Cannabinoid type 1 receptors |
| CB2 | Cannabinoid type 2 receptors |
| CBD | Cannabidiol |
| CIPN | Chemotherapy-induced peripheral neuropathy |
| CRP | C-reactive Protein |
| CSCs | Cancer stem cells |
| DNMT | DNA methyltransferase |
| EGCG | Epigallocatechin 3 gallate |
| EZH2 | Enhancer of zeste homolog2 |
| IH | Integrative Hematology |
| IGF1 | Insulin-like growth factor 1 |
| IkB | NkB inhibitor |
| IL6 | Interleukin 6 |
| IL17 | Interleukin 17 |
| IMiDs | Immunomodulatory imide drugs |
| IO | Integrative Oncology |
| MAMs | Macrophages associated with myeloma |
| MBI | Mindfulness-based interventions |
| MDASI | MD Anderson Symptom Inventory |
| MGUS | Monoclonal gammopathy of unknown significance |
| MM | Multiple Myeloma |
| MMP2 | Matrix metalloproteinase-2 |
| MMP9 | Matrix metalloproteinase-9 |
| mTOR | Mammalian target of rapamycin |
| NCV | Nerve conduction velocity |
| NfkB | Nuclear factor kappa B |
| PI | Proteasome inhibitor |
| PIs | Proteasome inhibitors |
| QoL | Quality of life |
| RANKL | Receptor activator of nuclear factor kappa-Β ligand |
| RCT | Randomized-controlled trial |
| ROS | Reactive oxygen species |
| SIO | Society for Integrative Oncology |
| STAT3 | Signal transducer and activator of transcription 3 |
| THC | Delta-trans-9-tetrahydrocannabinol |
| TNFα | Tumor necrosis factor-α |
| TP53 | Tumor protein p53 |
| VEGF | Vascular endothelium growth factor |
| VDR | Vitamin D receptor |
References
- Palumbo, A.; Anderson, K. Multiple Myeloma. N. Engl. J. Med. 2011, 364, 1046–1060. [Google Scholar] [CrossRef]
- Cowan, A.J.; Green, D.J.; Kwok, M.; Lee, S.; Coffey, D.G.; Holmberg, L.A.; Tuazon, S.; Gopal, A.K.; Libby, E.N. Diagnosis and Management of Multiple Myeloma: A Review. JAMA 2022, 327, 464–477. [Google Scholar] [CrossRef] [PubMed]
- Bird, S.A.; Boyd, K. Multiple Myeloma: An Overview of Management. Palliat. Care Soc. Pract. 2019, 13, 1178224219868235. [Google Scholar] [CrossRef] [PubMed]
- Kvam, A.K.; Waage, A. Health-Related Quality of Life in Patients with Multiple Myeloma-Does It Matter? Haematologica 2015, 100, 704–705. [Google Scholar] [CrossRef] [PubMed]
- Zaleta, A.K.; Miller, M.F.; Olson, J.S.; Yuen, E.Y.N.; LeBlanc, T.W.; Cole, C.E.; McManus, S.; Buzaglo, J.S. Symptom Burden, Perceived Control, and Quality of Life among Patients Living with Multiple Myeloma. JNCCN J. Natl. Compr. Cancer Netw. 2020, 18, 1087–1095. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, E.K.; Shapiro, Y.N.; Yee, A.J.; Nadeem, O.; Hu, B.Y.; Laubach, J.P.; Branagan, A.R.; Anderson, K.C.; Mo, C.C.; Munshi, N.C.; et al. Quality of Life, Psychological Distress, and Prognostic Perceptions in Patients with Multiple Myeloma. Cancer 2022, 128, 1996–2004. [Google Scholar] [CrossRef] [PubMed]
- Osborne, T.R.; Ramsenthaler, C.; de Wolf-Linder, S.; Schey, S.A.; Siegert, R.J.; Edmonds, P.M.; Higginson, I.J. Understanding What Matters Most to People with Multiple Myeloma: A Qualitative Study of Views on Quality of Life. BMC Cancer 2014, 14, 496. [Google Scholar] [CrossRef]
- Cenzer, I.; Berger, K.; Rodriguez, A.M.; Ostermann, H.; Covinsky, K.E. Patient-Reported Measures of Well-Being in Older Multiple Myeloma Patients: Use of Secondary Data Source. Aging Clin. Exp. Res. 2020, 32, 1153–1160. [Google Scholar] [CrossRef]
- Shapiro, Y.N.; Peppercorn, J.M.; Yee, A.J.; Branagan, A.R.; Raje, N.S.; Donnell, E.K.O. Lifestyle Considerations in Multiple Myeloma. Blood Cancer J. 2021, 11, 172. [Google Scholar] [CrossRef]
- Bonucci, M.; Andreazzoli, F. New approach of Integration: Integrative Hematology. Br. J. Res. 2017, 4, 6. [Google Scholar]
- Witt, C.M.; Balneaves, L.G.; Cardoso, M.J.; Cohen, L.; Greenlee, H.; Johnstone, P.; Kucuk, O.; Mailman, J.; Mao, J.J. A Comprehensive Definition for Integrative Oncology. J. Natl. Cancer Inst. Monogr. 2017, 2017, lgx012. [Google Scholar] [CrossRef] [PubMed]
- Okolo, O.; Wertheim, B.C.; Larsen, A.; Sweeney, N.W.; Ahlstrom, J.M.; Gowin, K. Integrative Medicine in Multiple Myeloma and Plasma Cell Disorders. Complement. Ther. Med. 2023, 73, 102939. [Google Scholar] [CrossRef] [PubMed]
- Roydhouse, J.K.; Bhatnagar, V.; Berman, T.; Menapace, L.A.; Agarwal, R.; Fiero, M.H.; Kluetz, P. Botanical Product Use Among Multiple Myeloma Patients in Commercial Drug Trials. Blood 2019, 134 (Suppl. S1), 4769. [Google Scholar] [CrossRef]
- Jogdand, R.P.; Singh, A.; Khumbhare, U.; Parameshwar; Nagaratna, R. Impact of Integrative Therapy in Remission of Multiple Myloma: A Case Study. Integr. Med. Case Rep. 2022, 3, 25. [Google Scholar] [CrossRef]
- Korde, N.; Tavitian, E.; Mastey, D.; Lengfellner, J.; Hevroni, G.; Zarski, A.; Salcedo, M.; Mailankody, S.; Hassoun, H.; Smith, E.L.; et al. Association of Patient Activity Bio-Profiles with Health-Related Quality of Life in Patients with Newly Diagnosed Multiple Myeloma: A Prospective Observational Cohort Study. Lancet 2023, 57, 101854. [Google Scholar] [CrossRef]
- Yu, C.C.; Li, Y.; Cheng, Z.J.; Wang, X.; Mao, W.; Zhang, Y.W. Active Components of Traditional Chinese Medicinal Material for Multiple Myeloma: Current Evidence and Future Directions. Front. Pharmacol. 2022, 13, 818179. [Google Scholar] [CrossRef]
- Shah, U.A.; Parikh, R.; Castro, F.; Bellone, M.; Lesokhin, A.M. Dietary and microbiome evidence in multiple myeloma and other plasma cell disorders. Leukemia 2023, 37, 964–980. [Google Scholar] [CrossRef]
- Malik, M.A.; Sweeney, N.W.; Jafri, M.; Derkach, A.; Chmielewski, C.; Adintori, P.A.; Mailankody, S.; Korde, N.; Tan, C.R.; Hassoun, H.; et al. Nutrition perceptions, needs and practices among patients with plasma cell disorders. Blood Cancer J. 2022, 12, 70. [Google Scholar] [CrossRef]
- Key, T.J.; Appleby, P.N.; Crowe, F.L.; Bradbury, K.E.; Schmidt, J.A.; Travis, R.C. Cancer in British vegetarians: Updated analyses of 4998 incident cancers in a cohort of 32,491 meat eaters, 8612 fish eaters, 18,298 vegetarians, and 2246 vegans. Am. J. Clin. Nutr. 2014, 100, 378s–385s. [Google Scholar] [CrossRef]
- Brown, L.M.; Gridley, G.; Pottern, L.M.; Baris, D.; Swanson, C.A.; Silverman, D.T.; Hayes, R.B.; Greenberg, R.S.; Swanson, G.M.; Schoenberg, J.B.; et al. Diet and nutrition as risk factors for multiple myeloma among blacks and whites in the United States. Cancer Causes Control CCC 2001, 12, 117–125. [Google Scholar] [CrossRef]
- Fritschi, L.; Ambrosini, G.L.; Kliewer, E.V.; Johnson, K.C. Dietary fish intake and risk of leukaemia, multiple myeloma, and non-Hodgkin lymphoma. Cancer epidemiology, biomarkers & prevention: A publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive. Oncology 2004, 13, 532–537. [Google Scholar]
- Wang, Y.Z.; Wu, Q.J.; Zhu, J.; Wu, L. Fish consumption and risk of myeloma: A meta-analysis of epidemiological studies. Cancer Causes Control CCC 2015, 26, 1307–1314. [Google Scholar] [CrossRef]
- Parolini, C. Effects of Fish n-3 PUFAs on Intestinal Microbiota and Immune System. Mar. Drugs 2019, 17, 374. [Google Scholar] [CrossRef] [PubMed]
- Vlajinac, H.D.; Pekmezović, T.D.; Adanja, B.J.; Marinković, J.M.; Kanazir, M.S.; Suvajdzić, N.D.; Colović, M.D. Case-control study of multiple myeloma with special reference to diet as risk factor. Neoplasma 2003, 50, 79–83. [Google Scholar]
- Thordardottir, M.; Lindqvist, E.K.; Lund, S.H.; Costello, R.; Burton, D.; Steingrimsdottir, L.; Korde, N.; Mailankody, S.; Eiriksdottir, G.; Launer, L.J.; et al. Dietary intake is associated with risk of multiple myeloma and its precursor disease. PLoS ONE 2018, 13, e0206047. [Google Scholar] [CrossRef] [PubMed]
- Hosgood, H.D., 3rd; Baris, D.; Zahm, S.H.; Zheng, T.; Cross, A.J. Diet and risk of multiple myeloma in Connecticut women. Cancer Causes Control CCC 2007, 18, 1065–1076. [Google Scholar] [CrossRef]
- Bieghs, L.; Johnsen, H.E.; Maes, K.; Menu, E.; Van Valckenborgh, E.; Overgaard, M.T.; Nyegaard, M.; Conover, C.A.; Vanderkerken, K.; De Bruyne, E. The insulin-like growth factor system in multiple myeloma: Diagnostic and therapeutic potential. Oncotarget 2016, 7, 48732–48752. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.H.; Fung, T.T.; Tabung, F.K.; Marinac, C.R.; Devore, E.E.; Rosner, B.A.; Ghobrial, I.M.; Colditz, G.A.; Giovannucci, E.L.; Birmann, B.M. Prediagnosis dietary pattern and survival in patients with multiple myeloma. Int. J. Cancer 2020, 147, 1823–1830. [Google Scholar] [CrossRef]
- Santo, L.; Liao, L.M.; Andreotti, G.; Purdue, M.P.; Hofmann, J.N. Alcohol consumption and risk of multiple myeloma in the NIH-AARP Diet and Health Study. Int. J. Cancer 2019, 144, 43–48. [Google Scholar] [CrossRef]
- Díaz, L.E.; Montero, A.; González-Gross, M.; Vallejo, A.I.; Romeo, J.; Marcos, A. Influence of alcohol consumption on immunological status: A review. Eur. J. Clin. Nutr. 2002, 56, S50–S53. [Google Scholar] [CrossRef]
- Marques-Mourlet, C.; Di Iorio, R.; Fairfield, H.; Reagan, M.R. Obesity and myeloma: Clinical and mechanistic contributions to disease progression. Front. Endocrinol. 2023, 14, 1118691. [Google Scholar] [CrossRef]
- Takeoka, Y.; Sakatoku, K.; Miura, A.; Yamamura, R.; Araki, T.; Seura, H.; Okamura, T.; Koh, H.; Nakamae, H.; Hino, M.; et al. Prognostic Effect of Low Subcutaneous Adipose Tissue on Survival Outcome in Patients with Multiple Myeloma. Clin. Lymphoma Myeloma Leuk. 2016, 16, 434–441. [Google Scholar] [CrossRef]
- Kamiya, T.; Ito, C.; Fujita, Y.; Ogura, S.; Mizuno, K.; Sakurai, A.; Aisa, Y.; Nakazato, T. The prognostic value of the controlling nutritional status score in patients with multiple myeloma. Leuk. Lymphoma 2020, 61, 1894–1900. [Google Scholar] [CrossRef] [PubMed]
- Capitão, C.; Coutinho, D.; Neves, P.M.; Capelas, M.L.; Pimenta, N.M.; Santos, T.; Mäkitie, A.; Ravasco, P. Protein intake and muscle mass maintenance in patients with cancer types with high prevalence of sarcopenia: A systematic review. Support. Care Cancer 2022, 30, 3007–3015. [Google Scholar] [CrossRef] [PubMed]
- Zhang, B.; Gu, J.; Liu, J.; Huang, B.; Li, J. Fecal microbiota taxonomic shifts in Chinese multiple myeloma patients analyzed by quantitative polimerase chain reaction (QPCR) and 16S rRNA high-throughput sequencing. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2019, 25, 8269–8280. [Google Scholar] [CrossRef] [PubMed]
- Antoine Pepeljugoski, C.; Morgan, G.; Braunstein, M. Analysis of intestinal microbiome in multiple myeloma reveals progressive dysbiosis compared to MGUS and healthy individuals. Blood 2019, 134, 3076. [Google Scholar] [CrossRef]
- Available online: https://clinicaltrials.gov/study/NCT05712967 (accessed on 30 November 2023).
- Jian, X.; Zhu, Y.; Ouyang, J.; Wang, Y.; Lei, Q.; Xia, J.; Guan, Y.; Zhang, J.; Guo, J.; He, Y.; et al. Alterations of gut microbiome accelerate multiple myeloma progression by increasing the relative abundances of nitrogen-recycling bacteria. Microbiome 2020, 8, 74. [Google Scholar] [CrossRef]
- Pianko, M.J.; Devlin, S.M.; Littmann, E.R.; Chansakul, A.; Mastey, D.; Salcedo, M.; Fontana, E.; Ling, L.; Tavitian, E.; Slingerland, J.B.; et al. Minimal residual disease negativity in multiple myeloma is associated with intestinal microbiota composition. Blood Adv. 2019, 3, 2040–2044. [Google Scholar] [CrossRef]
- Shah, U.A.; Maclachlan, K.H.; Derkach, A.; Salcedo, M.; Barnett, K.; Caple, J.; Blaslov, J.; Tran, L.; Ciardiello, A.; Burge, M.; et al. Sustained minimal residual disease negativity in multiple myeloma is associated with stool butyrate and healthier plant-based diets. Clin. Cancer Res. 2022, 28, 5149–5155. [Google Scholar] [CrossRef]
- Zhu, G.; Jin, L.; Shen, W.; Zhao, M.; Liu, N. Intratumor microbiota: Occult participants in the microenvironment of multiple myeloma. Biochim. Biophys. Acta Rev. Cancer 2023, 1878, 188959. [Google Scholar] [CrossRef]
- Available online: https://clinicaltrials.gov/study/NCT05640843 (accessed on 30 November 2023).
- Zoi, V.; Galani, V.; Lianos, G.D.; Voulgaris, S.; Kyritsis, A.P.; Alexiou, G.A. The Role of Curcumin in Cancer Treatment. Biomedicines 2021, 9, 1086. [Google Scholar] [CrossRef] [PubMed]
- Bai, Q.X.; Zhang, X.Y. Curcumin enhances cytotoxic effects of bortezomib in human multiple myeloma H929 cells: Potential roles of NF-κB/JNK. Int. J. Mol. Sci. 2012, 13, 4831–4838. [Google Scholar] [CrossRef] [PubMed]
- Allegra, A.; Speciale, A.; Molonia, M.S.; Guglielmo, L.; Musolino, C.; Ferlazzo, G.; Costa, G.; Saija, A.; Cimino, F. Curcumin ameliorates the in vitro efficacy of carfilzomib in human multiple myeloma U266 cells targeting p53 and NF-kappaB pathways. Toxicol. Vitr. 2018, 47, 186–194. [Google Scholar] [CrossRef]
- Gomez-Bougie, P.; Halliez, M.; Maïga, S.; Godon, C.; Kervoëlen, C.; Pellat-Deceunynck, C.; Moreau, P.; Amiot, M. Curcumin induces cell death of the main molecular myeloma subtypes, particularly the poor prognosis subgroups. Cancer Biol. Ther. 2015, 16, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Bharti, A.C.; Donato, N.; Aggarwal, B.B. Curcumin (diferuloylmethane) inhibits constitutive and IL-6-inducible STAT3 phosphorylation in human myeloma cells. J. Immunol. 2003, 171, 3863–3871. [Google Scholar] [CrossRef] [PubMed]
- Bashang, H.; Tamma, S. The use of curcumin as an effective adjuvant to cancer therapy: A short review. Biotechnol. Appl. Biochem. 2020, 67, 171–179. [Google Scholar] [CrossRef]
- Mekkawy, S.A.; Abdalla, M.S.; Omran, M.M.; Hassan, N.M.; Abdelfattah, R.; Abdel-Salam, I.M. Cancer Stem Cells as a Prognostic Biomarker and Therapeutic Target Using Curcumin/Piperine Extract for Multiple Myeloma. Asian Pac. J. Cancer Prev. APJCP 2022, 23, 3507–3515. [Google Scholar] [CrossRef]
- Chen, J.; Ying, Y.; Zhu, H.; Zhu, T.; Qu, C.; Jiang, J.; Fang, B. Curcumin-induced promoter hypermethylation of the mammalian target of rapamycin gene in multiple myeloma cells. Oncol. Lett. 2019, 17, 1108–1114. [Google Scholar] [CrossRef]
- Sung, B.; Kunnumakkara, A.B.; Sethi, G.; Anand, P.; Guha, S.; Aggarwal, B.B. Curcumin circumvents chemoresistance in vitro and potentiates the effect of thalidomide and bortezomib against human multiple myeloma in nude mice model. Mol. Cancer Ther. 2009, 8, 959–970. [Google Scholar] [CrossRef]
- Golombick, T.; Diamond, T.H.; Badmaev, V.; Manoharan, A.; Ramakrishna, R. The potential role of curcumin in patients with monoclonal gammopathy of undefined significance—Its effect on paraproteinemia and the urinary N-telopeptide of type I collagen bone turnover marker. Clin. Cancer Res. 2009, 15, 5917–5922. [Google Scholar] [CrossRef]
- Golombick, T.; Diamond, T.H.; Manoharan, A.; Ramakrishna, R. Monoclonal gammopathy of undetermined significance, smoldering multiple myeloma, and curcumin: A randomized, double-blind placebo-controlled cross-over 4g study and an open-label 8g extension study. Am. J. Hematol. 2012, 87, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, A.; Lai, M.; Cavenagh, J. Long-term stabilisation of myeloma with curcumin Case Reports. BMJ Case Rep. 2017, 2017, bcr2016218148. [Google Scholar] [CrossRef]
- Ramakrishna, R.; Diamond, T.H.; Alexander, W.; Manoharan, A.; Golombick, T. Use of Curcumin in Multiple Myeloma patients intolerant of steroid therapy. Clin. Case Rep. 2020, 8, 739–744. [Google Scholar] [CrossRef]
- Santosa, D.; Suharti, C.; Riwanto, I.; Dharmana, E.; Pangarsa, E.A.; Setiawan, B.; Suyono, S.; Tobing, M.L.; Suhartono, S.; Hadisapurto, S. Curcumin as adjuvant therapy to improve remission in myeloma patients: A pilot randomized clinical trial. Casp. J. Intern. Med. 2022, 13, 375–384. [Google Scholar]
- Shammas, M.A.; Neri, P.; Koley, H.; Batchu, R.B.; Bertheau, R.C.; Munshi, V.; Prabhala, R.; Fulciniti, M.; Tai, Y.T.; Treon, S.P.; et al. Specific killing of multiple myeloma cells by (−)-epigallocatechin-3-gallate extracted from green tea: Biologic activity and therapeutic implications. Blood 2006, 108, 2804–2810. [Google Scholar] [CrossRef]
- Zhou, C.G.; Hui, L.M.; Luo, J.M. Epigallocatechin gallate inhibits the proliferation and induces apoptosis of multiple myeloma cells via inactivating EZH2. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 2093–2098. [Google Scholar] [PubMed]
- Golden, E.B.; Lam, P.Y.; Kardosh, A.; Gaffney, K.J.; Cadenas, E.; Louie, S.G.; Petasis, N.A.; Chen, T.C.; Schönthal, A.H. Green tea polyphenols block the anticancer effects of bortezomib and other boronic acid-based proteasome inhibitors. Blood 2009, 113, 5927–5937. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Li, J.; Gu, J.; Huang, B.; Zhao, Y.; Zheng, D.; Ding, Y.; Zeng, L. Potentiation of (−)-epigallocatechin-3-gallate-induced apoptosis by bortezomib in multiple myeloma cells. Acta Biochim. Biophys. Sin. 2009, 41, 1018–1026. [Google Scholar] [CrossRef]
- Modernelli, A.; Naponelli, V.; Troglio, M.G.; Bonacini, M.; Ramazzina, I.; Bettuzzi, S.; Rizzi, F. EGCG antagonizes Bortezomib cytotoxicity in prostate cancer cells by an autophagic mechanism. Sci. Rep. 2015, 5, 15270. [Google Scholar] [CrossRef]
- Qiu, X.; Wu, X.; He, W. (−)-Epigallocatechin-3-gallate plays an antagonistic role in the antitumor effect of bortezomib in myeloma cells via activating Wnt/β-catenin signaling pathway. Adv. Clin. Exp. Med. 2022, 31, 789–794. [Google Scholar] [CrossRef]
- Li, C.; Feng, Y.; Wang, W.; Xu, L.; Zhang, M.; Yao, Y.; Wu, X.; Zhang, Q.; Huang, W.; Wang, X.; et al. Targeting Glutaminolysis to Treat Multiple Myeloma: An In Vitro Evaluation of Glutaminase Inhibitors Telaglenastat and Epigallocatechin-3-gallate. Anti-cancer Agents Med. Chem. 2023, 23, 779–785. [Google Scholar]
- Maier, G.S.; Horas, K.; Kurth, A.A.; Lazovic, D.; Seeger, J.B.; Maus, U. Prevalence of Vitamin D Deficiency in Patients with Bone Metastases and Multiple Myeloma. Anticancer Res. 2015, 35, 6281–6285. [Google Scholar] [PubMed]
- Rui, H.; Liu, Y.; Lin, M.; Zheng, X. Vitamin D receptor gene polymorphism is associated with multiple myeloma. J. Cell. Biochem. 2020, 121, 224–230. [Google Scholar] [CrossRef]
- Ng, A.C.; Kumar, S.K.; Rajkumar, S.V.; Drake, M.T. Impact of vitamin D deficiency on the clinical presentation and prognosis of patients with newly diagnosed multiple myeloma. Am. J. Hematol. 2009, 84, 397–400. [Google Scholar] [CrossRef]
- Wang, J.; Udd, K.A.; Vidisheva, A.; Swift, R.A.; Spektor, T.M.; Bravin, E.; Ibrahim, E.; Treisman, J.; Masri, M.; Berenson, J.R. Low serum vitamin D occurs commonly among multiple myeloma patients treated with bortezomib and/or thalidomide and isassociated with severe neuropathy. Support. Care Cancer 2016, 24, 3105–3110. [Google Scholar] [PubMed]
- Raoufinejad, K.; Shamshiri, A.R.; Pezeshki, S.; Chahardouli, B.; Hadjibabaie, M.; Jahangard-Rafsanjani, Z.; Gholami, K.; Rajabi, M.; Vaezi, M. Oral calcitriol in hematopoietic recovery and survival after autologous stem cell transplantation: A randomized clinical trial. DARU 2009, 27, 709–720. [Google Scholar] [CrossRef]
- Flamann, C.; Busch, L.; Mackensen, A.; Bruns, H. Combination of lenalidomide and vitamin D enhances MOR202-mediated cytotoxicity of macrophages: It takes three to tango. Oncotarget 2019, 10, 10–12. [Google Scholar] [CrossRef]
- Mirhosseini, N.; Psihogios, A.; McLaren, M.D.; Seely, D. Vitamin D and Multiple Myeloma: A Scoping Review. Curr. Oncol. 2023, 30, 3263–3276. [Google Scholar] [CrossRef]
- Perrone, G.; Hideshima, T.; Ikeda, H.; Okawa, Y.; Calabrese, E.; Gorgun, G.; Santo, L.; Cirstea, D.; Raje, N.; Chauhan, D.; et al. Ascorbic acid inhibits antitumor activity of bortezomib in vivo. Leukemia 2009, 23, 1679–1686. [Google Scholar] [CrossRef]
- Nakano, A.; Abe, M.; Oda, A.; Amou, H.; Hiasa, M.; Nakamura, S.; Miki, H.; Harada, T.; Fujii, S.; Kagawa, K.; et al. Delayed treatment with vitamin C and N-acetyl-l-cysteine protects Schwann cells without compromising the anti-myeloma activity of bortezomib. Int. J. Hematol. 2011, 93, 727–735. [Google Scholar] [CrossRef]
- Van Gorkom, G.N.Y.; Boerenkamp, L.S.; Gijsbers, B.L.M.G.; van Ojik, H.H.; Wodzig, W.K.W.H.; Wieten, L.; Van Elssen, C.H.M.J.; Bos, G.M.J. No Effect of Vitamin C Administration on Neutrophil Recovery in Autologous Stem Cell Transplantation for Myeloma or Lymphoma: A Blinded, Randomized Placebo-Controlled Trial. Nutrients 2022, 14, 4784. [Google Scholar] [CrossRef] [PubMed]
- Jakubikova, J.; Cervi, D.; Ooi, M.; Kim, K.; Nahar, S.; Klippel, S.; Cholujova, D.; Leiba, M.; Daley, J.F.; Delmore, J.; et al. Anti-tumor activity and signaling events triggered by the isothiocyanates, sulforaphane and phenethyl isothiocyanate, in multiple myeloma. Haematologica 2011, 96, 1170–1179. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, A.; Sethi, G.; Vadhan-Raj, S.; Bueso-Ramos, C.; Takada, Y.; Gaur, U.; Nair, A.S.; Shishodia, S.; Aggarwal, B.B. Resveratrol inhibits proliferation, induces apoptosis, and overcomes chemoresistance through down-regulation of STAT3 and nuclear factor-kappaB-regulated antiapoptotic and cell survival gene products in human multiple myeloma cells. Blood 2007, 109, 2293–2302. [Google Scholar] [CrossRef]
- Popat, R.; Plesner, T.; Davies, F.; Cook, G.; Cook, M.; Elliott, P.; Jacobson, E.; Gumbleton, T.; Oakervee, H.; Cavenagh, J. A phase 2 study of SRT501 (resveratrol) with bortezomib for patients with relapsed and or refractory multiple myeloma. Br. J. Haematol. 2013, 160, 714–717. [Google Scholar] [CrossRef] [PubMed]
- Bilbao, A.; Spanagel, R. Medical cannabinoids: A pharmacology-based systematic review and meta-analysis for all relevant medical indications. BMC Med. 2022, 20, 259. [Google Scholar] [CrossRef]
- Dariš, B.; Tancer Verboten, M.; Knez, Ž.; Ferk, P. Cannabinoids in cancer treatment: Therapeutic potential and legislation. Bosn. J. Basic Med. Sci. 2019, 19, 14–23. [Google Scholar] [CrossRef]
- Nabissi, M.; Morelli, M.B.; Offidani, M.; Amantini, C.; Gentili, S.; Soriani, A.; Cardinali, C.; Leoni, P.; Santoni, G. Cannabinoids synergize with carfilzomib, reducing multiple myeloma cells viability and migration. Oncotarget 2016, 7, 77543–77557. [Google Scholar] [CrossRef]
- Coluzzi, F.; Rolke, R.; Mercadante, S. Pain Management in Patients with Multiple Myeloma: An Update. Cancers 2019, 11, 2037. [Google Scholar] [CrossRef]
- Lu, W.; Rosenthal, D.S. Oncology Acupuncture for Chronic Pain in Cancer Survivors: A Reflection on the American Society of Clinical Oncology Chronic Pain Guideline. Hematol. Oncol. Clin. N. Am. 2018, 32, 519–533. [Google Scholar] [CrossRef]
- Ling, F.; Qi, W.; Li, X.; Zhou, J.; Xiong, J.; Zhao, Y.; Zheng, Q.; Liang, F. Bibliometric Analysis of Acupuncture Therapy for Cancer Pain Over the Past 10 Years. J. Pain Res. 2023, 16, 985–1003. [Google Scholar] [CrossRef]
- Huang, L.; Zhao, Y.; Xiang, M. Knowledge Mapping of Acupuncture for Cancer Pain: A Scientometric Analysis (2000–2019). J. Pain Res. 2021, 14, 343–358. [Google Scholar] [CrossRef] [PubMed]
- Kutcher, A.M.; LeBaron, V.T. Evaluating Acupuncture for the Treatment of Chemotherapy-Induced Peripheral Neuropathy: An Integrative Review. West. J. Nurs. Res. 2022, 44, 169–179. [Google Scholar] [CrossRef]
- Ben-Arye, E.; Hausner, D.; Samuels, N.; Gamus, D.; Lavie, O.; Tadmor, T.; Gressel, O.; Agbarya, A.; Attias, S.; David, A.; et al. Impact of Acupuncture and Integrative Therapies on Chemotherapy-Induced Peripheral Neuropathy: A Multicentered, Randomized Controlled Trial. Cancer 2022, 128, 3641–3652. [Google Scholar] [CrossRef] [PubMed]
- Richardson, P.G.; Briemberg, H.; Jagannath, S.; Wen, P.Y.; Barlogie, B.; Berenson, J.; Singhal, S.; Siegel, D.S.; Irwin, D.; Schuster, M.; et al. Frequency, Characteristics, and Reversibility of Peripheral Neuropathy during Treatment of Advanced Multiple Myeloma with Bortezomib. J. Clin. Oncol. 2006, 24, 3113–3120. [Google Scholar] [CrossRef] [PubMed]
- Mandiroǧlu, S.; Cevik, C.; Ayli, M. Acupuncture for Neuropathic Pain Due to Bortezomib in a Patient with Multiple Myeloma. Acupunct. Med. 2014, 32, 194–196. [Google Scholar] [CrossRef]
- Bao, T.; Lao, L.; Medeiros, M.; Zhang, R.; Dorsey, S.G.; Badros, A. Improvement of Painful Bortezomib-Induced Peripheral Neuropathy Following Acupuncture Treatment in a Case Series of Multiple Myeloma Patients. Med. Acupunct. 2012, 24, 181–187. [Google Scholar] [CrossRef]
- Bao, T.; Goloubeva, O.; Pelser, C.; Porter, N.; Primrose, J.; Hester, L.; Sadowska, M.; Lapidus, R.; Medeiros, M.; Lao, L.; et al. A Pilot Study of Acupuncture in Treating Bortezomib-Induced Peripheral Neuropathy in Patients with Multiple Myeloma. Integr. Cancer Ther. 2014, 13, 396–404. [Google Scholar] [CrossRef]
- Zhi, W.I.; Ingram, E.; Li, S.Q.; Chen, P.; Piulson, L.; Bao, T. Acupuncture for Bortezomib-Induced Peripheral Neuropathy: Not Just for Pain. Integr. Cancer Ther. 2018, 17, 1079–1086. [Google Scholar] [CrossRef]
- Garcia, M.K.; Cohen, L.; Guo, Y.; Zhou, Y.; You, B.; Chiang, J.; Orlowski, R.Z.; Weber, D.; Shah, J.; Alexanian, R.; et al. Electroacupuncture for Thalidomide/Bortezomib-Induced Peripheral Neuropathy in Multiple Myeloma: A Feasibility Study. J. Hematol. Oncol. 2014, 7, 41. [Google Scholar] [CrossRef]
- Wang, L.; Xu, X.; Yao, L.; Huang, Y.; Zou, Q.; Wu, B.; Yin, D. Intervention Effect of Acupuncture and Moxibustion in Treatment of Chemotherapy-Induced Peripheral Neuropathy in Patients with Multiple Myeloma. J. Clin. Med. Pract. 2022, 26, 28–30. [Google Scholar]
- Han, X.; Wang, L.; Shi, H.; Zheng, G.; He, J.; Wu, W.; Shi, J.; Wei, G.; Zheng, W.; Sun, J.; et al. Acupuncture Combined with Methylcobalamin for the Treatment of Chemotherapy-Induced Peripheral Neuropathy in Patients with Multiple Myeloma. BMC Cancer 2017, 17, 40. [Google Scholar] [CrossRef] [PubMed]
- Deng, G.; Giralt, S.; Chung, D.J.; Landau, H.; Siman, J.; Search, B.; Coleton, M.; Vertosick, E.; Shapiro, N.; Chien, C.; et al. Acupuncture for Reduction of Symptom Burden in Multiple Myeloma Patients Undergoing Autologous Hematopoietic Stem Cell Transplantation: A Randomized Sham-Controlled Trial. Support. Care Cancer 2018, 26, 657–665. [Google Scholar] [CrossRef]
- Deng, G. Acupuncture as a Potential Opioid-Sparing Pain Management Intervention for Patients Undergoing Cancer Treatment. Med. Acupunct. 2020, 32, 394–395. [Google Scholar] [CrossRef]
- El Iskandarani, S.; Sun, L.; Li, S.Q.; Pereira, G.; Giralt, S.; Deng, G. Acupuncture Improves Certain Aspects of Sleep in Hematopoietic Stem Cell Transplantation Patients: A Secondary Analysis of a Randomized Controlled Trial. Acupunct. Med. 2023, 41, 319–326. [Google Scholar] [CrossRef]
- Deng, G.; Giralt, S.; Chung, D.J.; Landau, H.; Siman, J.; Li, Q.S.; Lapen, K.; Mao, J.J. Reduction of Opioid Use by Acupuncture in Patients Undergoing Hematopoietic Stem Cell Transplantation: Secondary Analysis of a Randomized, Sham-Controlled Trial. Pain Med. 2020, 21, 636–642. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Jiang, C. Effects of Heat-Sensitive Moxibustion plus Chinese Medication on the Expression of Serum Inflammatory Indicators and MicroRNAs in Patients with Multiple Myeloma after Chemotherapy. J. Acupunct. Tuina Sci. 2023, 21, 51–58. [Google Scholar] [CrossRef]
- Ke, M.; Qian, J.; Hao, F.; Li, X.; Wu, H.; Luo, X.; Xu, B.; Gu, C.; Yang, Y. Acupuncture Synergized with Bortezomib Improves Survival of Multiple Myeloma Mice via Decreasing Metabolic Ornithine. Front. Oncol. 2021, 11, 779562. [Google Scholar] [CrossRef]
- Lyu, J.; Wang, S.; Zhang, H.; Liu, S. Acupuncture-Exacerbated Pyoderma Gangrenosum Associated with IgG Multiple Myeloma. Wounds 2022, 34, e108–e111. [Google Scholar] [CrossRef]
- Kayo, T.; Suzuki, M.; Mitsuma, T.; Suzuki, M.; Ikeda, S.; Sukegawa, M.; Tsunoda, S.; Ohta, M. Bleeding Risk of Acupuncture for Patients with Hematological Malignancies Accompanying Thrombocytopenia: A Retrospective Chart Review. J. Integr. Complement. Med. 2023. ahead of print. [Google Scholar] [CrossRef]
- Mao, J.J.; Ismaila, N.; Bao, T.; Barton, D.; Ben-Arye, E.; Garland, E.L.; Greenlee, H.; Leblanc, T.; Lee, R.T.; Lopez, A.M.; et al. Integrative Medicine for Pain Management in Oncology: Society for Integrative Oncology-ASCO Guideline. J. Clin. Oncol. 2022, 40, 3998–4024. [Google Scholar] [CrossRef]
- Carlson, L.E.; Ismaila, N.; Addington, E.L.; Asher, G.N.; Atreya, C.; Balneaves, L.G.; Bradt, J.; Fuller-Shavel, N.; Goodman, J.; Hoffman, C.J.; et al. Integrative Oncology Care of Symptoms of Anxiety and Depression in Adults with Cancer: Society for Integrative Oncology-ASCO Guideline. J. Clin. Oncol. 2023, 41, 4562–4591. [Google Scholar] [CrossRef]
- Lamers, J.; Hartmann, M.; Goldschmidt, H.; Brechtel, A.; Hillengass, J.; Herzog, W. Psychosocial support in patients with multiple myeloma at time of diagnosis: Who wants what? Psychooncology 2013, 22, 2313–2320. [Google Scholar] [CrossRef] [PubMed]
- Pulgar, Á.; Garrido, S.; Alcalá, A.; Reyes del Paso, G.A. Psychosocial predictors of immune response following bone marrow transplantation. Behav. Med. 2012, 38, 12–18. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, M.R.; LeBlanc, T.W.; Yang, Q.; McLaughlin, J.; Irish, K.; Smith, S.K. A Mobile App to Support Self-Management in Patients with Multiple Myeloma or Chronic Lymphocytic Leukemia: Pilot Randomized Controlled Trial. JMIR Cancer 2023, 9, e44533. [Google Scholar] [CrossRef] [PubMed]
- Ng, D.L.; Gan, G.G.; Anuar, N.A.; Tung, Y.Z.; Lai, N.Z.; Tan, Y.W.; Said, S.N.M.; Madihie, A.; Chai, C.S.; Tan, S.B. The effect of a single session of 30-min mindful breathing in reducing fatigue among patients with haematological cancer—A randomised controlled trial. BMC Palliat. Care 2021, 20, 160. [Google Scholar] [CrossRef] [PubMed]
- Bates, D.; Bolwell, B.; Majhail, N.S.; Rybicki, L.; Yurch, M.; Abounader, D.; Kohuth, J.; Jarancik, S.; Koniarczyk, H.; McLellan, L.; et al. Music Therapy for Symptom Management After Autologous Stem Cell Transplantation: Results from a Randomized Study. Biol. Blood Marrow Transplant. 2017, 23, 1567–1572. [Google Scholar] [CrossRef]
- Saha, V.; Mallik, K.C. Psycho-socio-spiritual care in multiple myeloma: Are we lagging behind? Indian J. Cancer 2022, 59, 128–131. [Google Scholar]
- Sherman, A.C.; Plante, T.G.; Simonton, S.; Latif, U.; Anaissie, E.J. Prospective study of religious coping among patients undergoing autologous stem cell transplantation. J. Behav. Med. 2009, 32, 118–128. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Substance | Dose | Potential Chemotherapy Interaction | References |
|---|---|---|---|
| Vitamin D | To reach blood levels >30 ng/ml | Synergism with lenalidomide, pomalidomide, anti-CD38 | [67,68,69] |
| Curcumin | 6–8 g daily or liposomal formulation | Synergism with bortezomib, carfilzomib, thalidomide, melphalan | [44,45,51,52,53,54,55,56] |
| Epigallocatechin 3 gallate | 1 g daily | Antagonism with bortezomib | [61,62] |
| Vitamin C | 6–8 g daily | Antagonism with bortezomib | [71,72] |
| Cannabinoids | ? | Synergism with carfilzomib | [79] |
| Sulforaphane | To be found | Synergism with dexamethasone, doxorubicin, bortezomib, and melphalan | [74] |
| Resveratrol | To be found | Antagonism with bortezomib; possible side effects, not recommended | [75,76] |
| Indication | Description | Outcomes | Safety | References |
|---|---|---|---|---|
| CIPN | Ear and/or body points at least 1/week Electro Moxibustion | Improves sensory and motor symptoms. Improves QoL. Effect on NCV? | Avoid puncturing infected areas [37]. Safe for thrombo-cytopenia [38] | [87,88,89,90,91,92,93] |
| HSCT after conditioning regimen | 1/day for 5 days in ear and body points | Alleviates nausea. Improves appetite. Improves sleep quality. Decreases pain. Reduces opioid use. | [94,95,96,97] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Andreazzoli, F.; Levy Yurkovski, I.; Ben-Arye, E.; Bonucci, M. Conceptualizing an Integrative Multiple Myeloma Care: The Role of Nutrition, Supplements, and Complementary Modalities. Nutrients 2024, 16, 237. https://doi.org/10.3390/nu16020237
Andreazzoli F, Levy Yurkovski I, Ben-Arye E, Bonucci M. Conceptualizing an Integrative Multiple Myeloma Care: The Role of Nutrition, Supplements, and Complementary Modalities. Nutrients. 2024; 16(2):237. https://doi.org/10.3390/nu16020237
Chicago/Turabian StyleAndreazzoli, Francesca, Ilana Levy Yurkovski, Eran Ben-Arye, and Massimo Bonucci. 2024. "Conceptualizing an Integrative Multiple Myeloma Care: The Role of Nutrition, Supplements, and Complementary Modalities" Nutrients 16, no. 2: 237. https://doi.org/10.3390/nu16020237
APA StyleAndreazzoli, F., Levy Yurkovski, I., Ben-Arye, E., & Bonucci, M. (2024). Conceptualizing an Integrative Multiple Myeloma Care: The Role of Nutrition, Supplements, and Complementary Modalities. Nutrients, 16(2), 237. https://doi.org/10.3390/nu16020237