

Does the Composition of Breast Milk in the First Week Postpartum Differ Due to Maternal Factors or Neonatal Birth Weight and Percent Fat Body Mass?


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Material
2.2. Body Composition Analysis
2.3. Breast Milk Analysis
2.4. Software
2.5. Statistics
2.6. Ethics
3. Results
3.1. Demographic and Medical Data in the Primary Study Groups
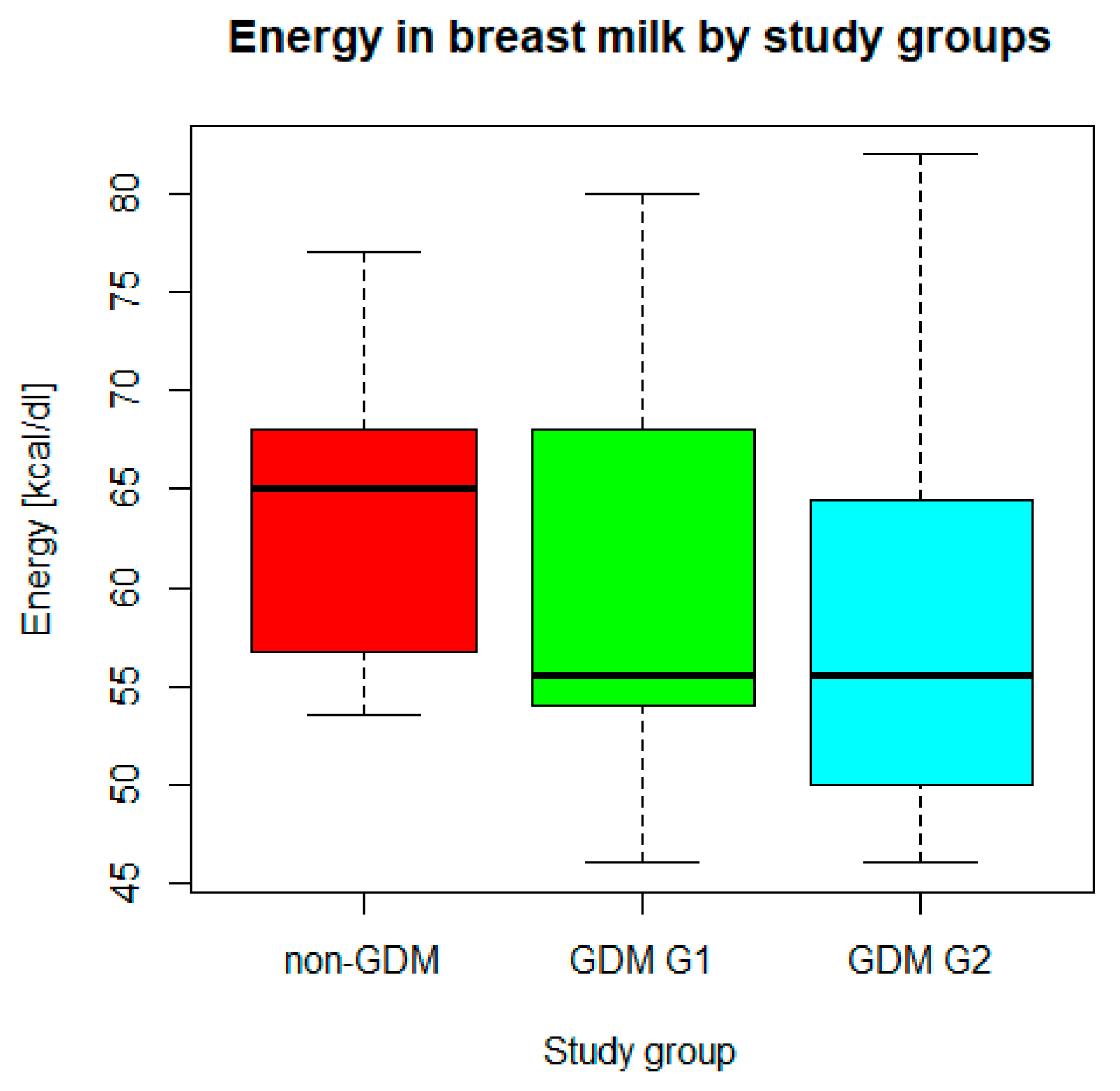
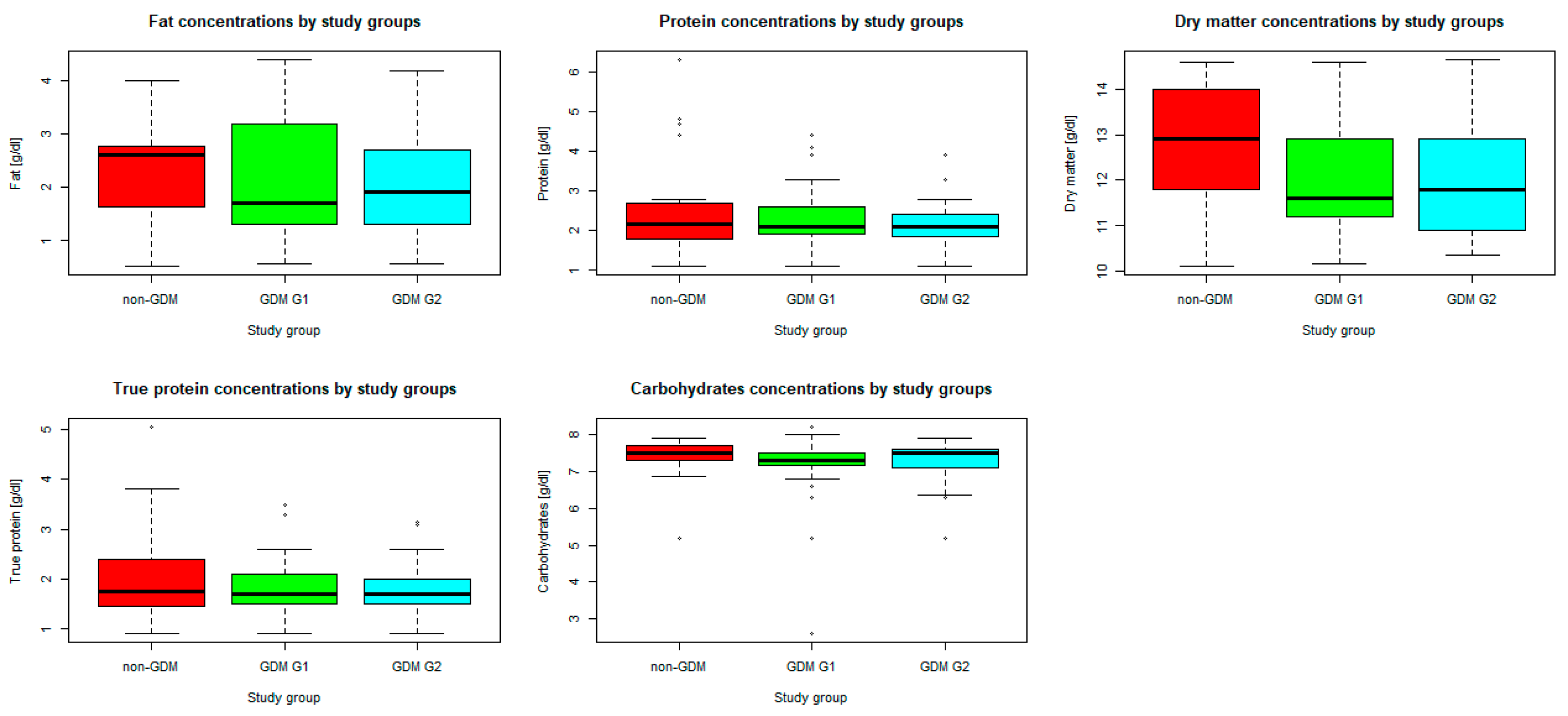
3.2. Analysis of Breast Milk Composition
3.3. Cluster Analysis
3.4. Influence of Neonatal Birth Weight (BW) and Body Fat Mass Percent (%FBM) on Maternal Milk Composition
3.5. Other Maternal Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kim, S.Y.; Yi, D.Y. Components of human breast milk: From macronutrient to microbiome and microRNA. Clin. Exp. Pediatr. 2020, 63, 301–309. [Google Scholar] [CrossRef] [PubMed]
- Golan, Y.; Assaraf, Y.G. Genetic and Physiological Factors Affecting Human Milk Production and Composition. Nutrients 2020, 12, 1500. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (US) Committee on Nutritional Status During Pregnancy and Lactation. Nutrition During Lactation; Milk Composition; National Academies Press (US): Washington, DC, USA, 1991; Volume 6. Available online: https://www.ncbi.nlm.nih.gov/books/NBK235590/ (accessed on 1 December 2023).
- Samuel, T.M.; Zhou, Q.; Giuffrida, F.; Munblit, D.; Verhasselt, V.; Thakkar, S.K. Nutritional and Non-nutritional Composition of Human Milk Is Modulated by Maternal, Infant, and Methodological Factors. Front. Nutr. 2020, 7, 576133. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y. The Impact of Gestational Diabetes Mellitus on the Composition of Breast Milk: A Systematic Review. HSET 2023, 30, 143–155. [Google Scholar] [CrossRef]
- Lopes, F.O.; Soares, F.V.M.; Silva, D.A.D.; Moreira, M.E.L. Do Thyroid Diseases during Pregnancy and Lactation Affect the Nutritional Composition of Human Milk? As doenças da tireoide durante a gestação e lactação afetam a composição nutricional do leite humano? Rev. Bras. Ginecol. Obstet. 2020, 42, 752–758. [Google Scholar] [CrossRef] [PubMed]
- Hashemi Javaheri, F.S.; Karbin, K.; Senobari, M.A.; Hakim, H.G.; Hashemi, M. The association between maternal body mass index and breast milk composition: A systematic review. Nutr. Rev. 2024. [Google Scholar] [CrossRef] [PubMed]
- Meek, J.Y.; Noble, L. Section on Breastfeeding; Policy Statement: Breastfeeding and the Use of Human Milk. Pediatrics 2022, 150, e2022057988. [Google Scholar] [CrossRef] [PubMed]
- Horta, B.L.; Victora, C.G.; World Health Organization. Long-Term Effects of Breastfeeding: A Systematic Review. Available online: http://www.who.int/iris/handle/10665/79198 (accessed on 19 July 2024).
- Optimizing support for breastfeeding as part of obstetric practice. ACOG Committee Opinion No. 756. American College of Obstetricians and Gynecologists. Obstet. Gynecol. 2018, 132, e187–e196. [CrossRef]
- Nommsen, L.A.; Lovelady, C.A.; Heinig, M.J.; Lönnerdal, B.; Dewey, K.G. Determinants of energy, protein, lipid, and lactose concentrations in human milk during the first 12 months of lactation: The DARLING Study. Am. J. Clin. Nutr. 1991, 53, 457–465. [Google Scholar] [CrossRef]
- Lagström, H.; Rautava, S.; Ollila, H.; Kaljonen, A.; Turta, O.; Mäkelä, J.; Yonemitsu, C.; Gupta, J.; Bode, L. Associations between human milk oligosaccharides and growth in infancy and early childhood. Am. J. Clin. Nutr. 2020, 111, 769–778. [Google Scholar] [CrossRef]
- Butte, N.F.; Garza, C.; Smith, E.O.; Nichols, B.L. Human milk intake and growth in exclusively breast-fed infants. J. Pediatr. 1984, 104, 187–195. [Google Scholar] [CrossRef] [PubMed]
- Karcz, K.; Czosnykowska-Lukacka, M.; Krolak-Olejnik, B. Impact of gestational diabetes and other maternal factors on neonatal body composition in the first week of life: A case-control study. Ginekol. Pol. 2023, 94, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Marczewski, E.; Steinhaus, H. On a certain distance of sets and the corresponding distance of functions. Colloq. Math. 1958, 6, 319–327. Available online: http://matwbn.icm.edu.pl/ksiazki/cm/cm6/cm6141.pdf (accessed on 19 July 2024). [CrossRef]
- Zhai, C.X. A Note on the Expectation-Maximization (EM) Algorithm; Department of Computer Science, University of Illinois at Urbana-Champaign: Chicago, IL, USA, 2007; Available online: https://citeseerx.ist.psu.edu/document?repid=rep1&type=pdf&doi=8c3e7708aa78ba89ce85df96f17de3125def7d4c (accessed on 19 July 2024).
- Sims, C.R.; Lipsmeyer, M.E.; Turner, D.E.; Andres, A. Human milk composition differs by maternal BMI in the first 9 months postpartum. Am. J. Clin. Nutr. 2020, 112, 548–557. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Borràs-Novell, C.; Herranz Barbero, A.; Balcells Esponera, C.; López-Abad, M.; Aldecoa Bilbao, V.; Izquierdo Renau, M.; Iglesias Platas, I. Influence of maternal and perinatal factors on macronutrient content of very preterm human milk during the first weeks after birth. J. Perinatol. 2023, 43, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Leghi, G.E.; Netting, M.J.; Middleton, P.F.; Wlodek, M.E.; Geddes, D.T.; Muhlhausler, A.B.S. The impact of maternal obesity on human milk macronutrient composition: A systematic review and meta-analysis. Nutrients 2020, 12, 934. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dugas, C.; Laberee, L.; Perron, J.; St-Arnaud, G.; Richard, V.; Perreault, V.; Leblanc, N.; Marc, I.; Di Marzo, V.; Doyen, A.; et al. Gestational Diabetes Mellitus, Human Milk Composition, and Infant Growth. Breastfeed. Med. 2023, 18, 14–22. [Google Scholar] [CrossRef] [PubMed]
- Peila, C.; Gazzolo, D.; Bertino, E.; Cresi, F.; Coscia, A. Influence of Diabetes during Pregnancy on Human Milk Composition. Nutrients 2020, 12, 185. [Google Scholar] [CrossRef] [PubMed]
- Şahin, Ö.N.; Di Renzo, G.C. Gestational Diabetes and Variety in the Composition of Breast Milk. In Breastfeeding and Metabolic Programming; Şahin, Ö.N., Briana, D.D., Di Renzo, G.C., Eds.; Springer: Cham, Switzerland, 2023. [Google Scholar] [CrossRef]
- de Fluiter, K.S.; Kerkhof, G.F.; van Beijsterveldt, I.A.L.P.; Breij, L.M.; van de Heijning, B.J.M.; Abrahamse-Berkeveld, M.; Hokken-Koelega, A.C.S. Longitudinal human milk macronutrients, body composition and infant appetite during early life. Clin. Nutr. 2021, 40, 3401–3408. [Google Scholar] [CrossRef]
- Much, D.; Brunner, S.; Vollhardt, C.; Schmid, D.; Sedlmeier, E.M.; Brüderl, M.; Heimberg, E.; Bartke, N.; Boehm, G.; Bader, B.L.; et al. Breast milk fatty acid profile in relation to infant growth and body composition: Results from the INFAT study. Pediatr. Res. 2013, 74, 230–237. [Google Scholar] [CrossRef]
- Simon Sarkadi, L.; Zhang, M.; Muránszky, G.; Vass, R.A.; Matsyura, O.; Benes, E.; Vari, S.G. Fatty Acid Composition of Milk from Mothers with Normal Weight, Obesity, or Gestational Diabetes. Life 2022, 12, 1093. [Google Scholar] [CrossRef] [PubMed]
- Rice, M.S.; Valentine, C.J. Neonatal Body Composition: Measuring Lean Mass as a Tool to Guide Nutrition Management in the Neonate. Nutr. Clin. Pract. 2015, 30, 625–632. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Macronutrients (g/dL; # Energy kcal/dL) | All Participants (n = 70) | Cluster 1 (n = 23) | Cluster 2 (n = 27) | Cluster 3 (n = 14) | Cluster 4 (n = 6) | p Value |
|---|---|---|---|---|---|---|
| Fat (Mean, SD) | 2.2, 1.02 | 2.2, 0.9 | 2.1, 1.2 | 2.2, 0.7 | 2.6, 0.9 | 0.762 |
| Total protein (Median, IQR) | 2.1, 1.8–2.5 | 2.1, 1.9–2.8 | 2.1, 1.8–2.5 | 2.4, 2.1–4.4 | 1.8, 1.7–1.9 | 0.051 |
| Carbohydrates (Mean, SD) | 7.2, 0.82 | 7.2, 1.1 | 7.2, 0.7 | 7.4, 0.3 | 7.3, 1.1 | 0.785 |
| Dry matter (Median, IQR) | 12.0, 11.2–13.3 | 11.8, 11.3–12.9 | 11.6, 10.7–13.3 | 12.0, 11.8–14.0 | 12.7, 11.6–13.3 | 0.089 |
| Energy (Mean, SD) # | 60.3, 9.6 | 59.4, 8.3 | 58.4, 1.4 | 63.4, 7.4 | 64.9, 8.0 | 0.246 |
| True protein (Median, IQR) | 1.7, 1.5–2.1 | 1.7, 1.5–2.0 | 1.7, 1.4–2.1 | 2.0, 1.7–3.15 | 1.45, 1.4–1.5 | 0.041 * |
| BW | %FBM | |||||
|---|---|---|---|---|---|---|
| Macronutrient | Coefficient | 95% CI | p Value | Coefficient | 95% CI | p Value |
| Fat | −0.090 | −0.590, 0.410 | 0.725 | 0.035 | −0.068, 0.138 | 0.508 |
| Total protein | 0.4234 | −0.035, 0.883 | 0.075 | 0.113 | 0.020, 0.206 | 0.020 * |
| Carbohydrates | 0.348 | −0.045, 0.741 | 0.880 | −0.036 | −0.118, 0.046 | 0.396 |
| Dry matter | 0.445 | −0.380, 0.869 | 0.245 | 0.128 | 0.003, 0.254 | 0.048 * |
| Energy | 2.244 | −2.424, 6.911 | 0.249 | 0.925 | −0.017, 1.867 | 0.060 |
| True protein | 0.256 | −0.128, 0.639 | 0.196 | 0.103 | 0.027, 0.179 | 0.010 * |
| Macronutrient [g/dL; # Energy kcal/dL] | Maternal Factor | |||
|---|---|---|---|---|
| History of Hypothyroidism | ||||
| Gestational (with Onset during Pregnancy) (n = 13) | Chronic (with Onset Before Pregnancy) (n = 20) | None (n = 37) | p Value | |
| Fat | 2.3, 1.3–2.8 | 1.5, 1.2–3.5 | 2.1, 1.6–2.7 | 0.665 |
| Total protein | 2.1, 1.9–2.5 | 1.9, 1.8–2.3 | 2.2, 1.9–2.8 | 0.062 |
| Carbohydrates | 7.4, 7.1–7.7 | 7.4, 7.2–7.5 | 7.5, 7.2–7.6 | 0.769 |
| Dry matter | 12.6, 11.6–12.9 | 11.3, 10.8–13.4 | 12.0, 11.6–12.9 | 0.364 |
| Energy # | 60.5, 55.0–67.5 | 55.0, 48.5–68.5 | 58.0, 55.0–67.5 | 0.308 |
| True protein | 1.7, 1.5–2.6 | 1.5, 1.4–1.8 | 1.8, 1.5–2.3 | 0.024 * |
| Pre-pregnancy BMI [kg/m2] | ||||
| Normal (n = 40) | Overweight (n = 16) | Obese (n = 14) | p value | |
| Fat | 2.1, 1.6–2.8 | 2.0, 1.4–3.3 | 1.5, 1.2–2.4 | 0.269 |
| Total protein | 2.1, 1.8–2.6 | 2.1, 1.8–2.2 | 2.4, 2.1–2.7 | 0.121 |
| Carbohydrates | 7.4, 7.1–7.6 | 7.5, 7.3–7.6 | 7.5, 7.3–7.6 | 0.699 |
| Dry matter | 12.3, 11.6–13.1 | 11.7, 10.6–13.2 | 12.1, 10.9–14.0 | 0.459 |
| Energy # | 57.5, 55.0–67.0 | 56.8, 50.0–71.7 | 59.3, 50.0–66.0 | 0.752 |
| True protein | 1.7, 1.4–2.3 | 1.7, 1.5–1.8 | 1.9, 1.7–3.1 | 0.086 |
| Gestational weight gain in reference to pre-gestational BMI | ||||
| Below recommendations (n = 18) | Within recommendations (n = 26) | Above recommendations (n = 26) | p value | |
| Fat | 1.9, 1.3–3.3 | 1.8, 1.3–2.9 | 2.1, 1.6–2.8 | 0.799 |
| Total protein | 2.1, 1.9–2.6 | 2.0, 1.8–2.3 | 2.2, 1.8–2.7 | 0.377 |
| Carbohydrates | 7.5, 7.3–7.6 | 7.4, 7.2–7.6 | 7.5, 7.1–7.7 | 0.690 |
| Dry matter | 12.3, 11.5–13.3 | 11.6, 10.9–12.6 | 12.6, 11.7–13.5 | 0.133 |
| Energy | 57.0, 54.0–68.0 | 55.5, 51.0–65.0 | 62.8, 55.5–68.0 | 0.241 |
| True protein | 1.7, 1.6–2.6 | 1.6, 1.4–2.0 | 1.8, 1.5–2.1 | 0.456 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karcz, K.; Gaweł, P.; Królak-Olejnik, B. Does the Composition of Breast Milk in the First Week Postpartum Differ Due to Maternal Factors or Neonatal Birth Weight and Percent Fat Body Mass? Nutrients 2024, 16, 3310. https://doi.org/10.3390/nu16193310
Karcz K, Gaweł P, Królak-Olejnik B. Does the Composition of Breast Milk in the First Week Postpartum Differ Due to Maternal Factors or Neonatal Birth Weight and Percent Fat Body Mass? Nutrients. 2024; 16(19):3310. https://doi.org/10.3390/nu16193310
Chicago/Turabian StyleKarcz, Karolina, Paulina Gaweł, and Barbara Królak-Olejnik. 2024. "Does the Composition of Breast Milk in the First Week Postpartum Differ Due to Maternal Factors or Neonatal Birth Weight and Percent Fat Body Mass?" Nutrients 16, no. 19: 3310. https://doi.org/10.3390/nu16193310
APA StyleKarcz, K., Gaweł, P., & Królak-Olejnik, B. (2024). Does the Composition of Breast Milk in the First Week Postpartum Differ Due to Maternal Factors or Neonatal Birth Weight and Percent Fat Body Mass? Nutrients, 16(19), 3310. https://doi.org/10.3390/nu16193310