Intestinal Anti-Endomysium Antibodies Are a Useful Tool for Diagnosing Celiac Disease in Pediatric and Adult Patients

 , , , , , ,
, , , , , ,  , , , ,
, , , ,
Abstract
1. Introduction
2. Materials and Methods
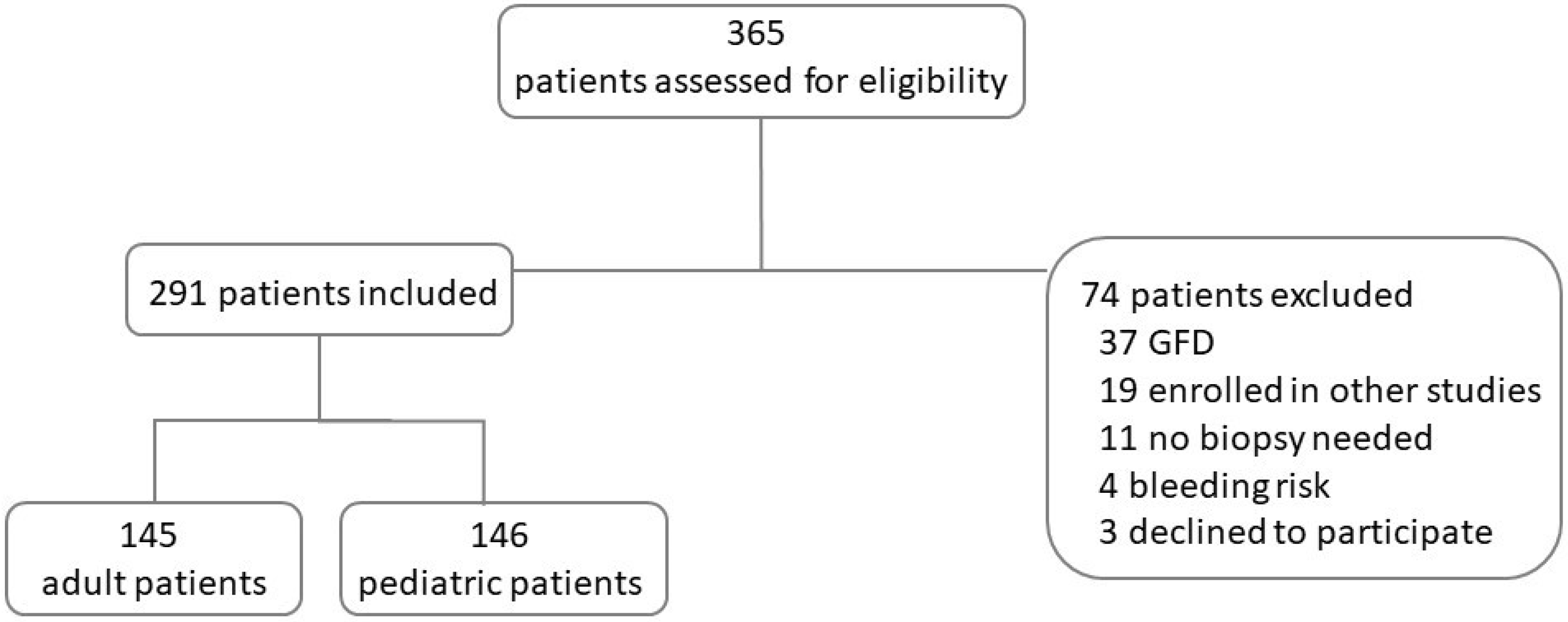
2.1. Study Design and Patient Population
2.2. Serology Tests
2.3. HLA Type Determination
2.4. Small Bowel Histology
2.5. Biopsy Culture Anti Endomysium Assay
2.6. Statistics
3. Results
3.1. Adult Subjects
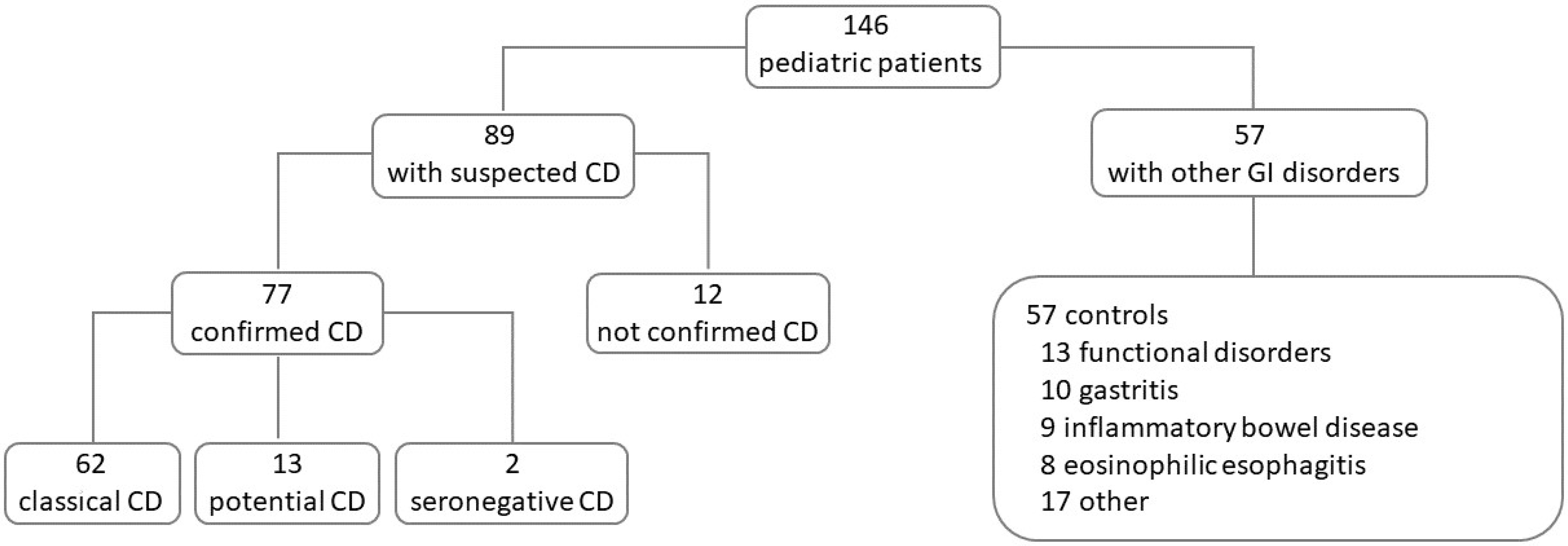
3.2. Pediatric Subjects
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AEA | Intestinal anti-endomysium antibodies |
| Anti-ttg | Anti-tissue transglutaminase |
| CD | Celiac disease CD |
| ESPGHAN | European Society for Pediatric Gastroenterology, Hepatology and Nutrition |
| GI | Gastro-intestinal |
| HLA | Human Leukocyte Antigens |
| NICE | National Institute for Health and Care Excellence |
| PPV | Positive predictive value |
References
- Singh, P.; Arora, A.; Strand, T.A.; Leffler, D.A.; Catassi, C.; Green, P.H.; Kelly, C.P.; Ahuja, V.; Makharia, G.K. Global Prevalence of Celiac Disease: Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2018, 16, 823–836.e2. [Google Scholar] [CrossRef] [PubMed]
- Gujral, N. Celiac Disease: Prevalence, Diagnosis, Pathogenesis and Treatment. World J. Gastroenterol. 2012, 18, 6036. [Google Scholar] [CrossRef]
- Caio, G.; Volta, U.; Sapone, A.; Leffler, D.A.; De Giorgio, R.; Catassi, C.; Fasano, A. Celiac Disease: A Comprehensive Current Review. BMC Med. 2019, 17, 142. [Google Scholar] [CrossRef] [PubMed]
- Catassi, C.; Verdu, E.F.; Bai, J.C.; Lionetti, E. Coeliac Disease. Lancet 2022, 399, 2413–2426. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, B.; Sanders, D.S.; Green, P.H.R. Coeliac Disease. Lancet 2018, 391, 70–81. [Google Scholar] [CrossRef]
- Maglio, M.; Troncone, R. Intestinal Anti-Tissue Transglutaminase2 Autoantibodies: Pathogenic and Clinical Implications for Celiac Disease. Front. Nutr. 2020, 7, 73. [Google Scholar] [CrossRef]
- Husby, S.; Koletzko, S.; Korponay-Szabó, I.R.; Mearin, M.L.; Phillips, A.; Shamir, R.; Troncone, R.; Giersiepen, K.; Branski, D.; Catassi, C.; et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition Guidelines for the Diagnosis of Coeliac Disease. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 136–160. [Google Scholar] [CrossRef]
- Husby, S.; Koletzko, S.; Korponay-Szabó, I.; Kurppa, K.; Mearin, M.L.; Ribes-Koninckx, C.; Shamir, R.; Troncone, R.; Auricchio, R.; Castillejo, G.; et al. European Society Paediatric Gastroenterology, Hepatology and Nutrition Guidelines for Diagnosing Coeliac Disease 2020. J. Pediatr. Gastroenterol. Nutr. 2020, 70, 141–156. [Google Scholar] [CrossRef]
- Trovato, C.M.; Montuori, M.; Anania, C.; Barbato, M.; Vestri, A.R.; Guida, S.; Oliva, S.; Mainiero, F.; Cucchiara, S.; Valitutti, F. Are ESPGHAN “Biopsy-Sparing” Guidelines for Celiac Disease Also Suitable for Asymptomatic Patients? Am. J. Gastroenterol. 2015, 110, 1485–1489. [Google Scholar] [CrossRef]
- Werkstetter, K.J.; Korponay-Szabó, I.R.; Popp, A.; Villanacci, V.; Salemme, M.; Heilig, G.; Lillevang, S.T.; Mearin, M.L.; Ribes-Koninckx, C.; Thomas, A.; et al. Accuracy in Diagnosis of Celiac Disease Without Biopsies in Clinical Practice. Gastroenterology 2017, 153, 924–935. [Google Scholar] [CrossRef]
- Wolf, J.; Petroff, D.; Richter, T.; Auth, M.K.H.; Uhlig, H.H.; Laass, M.W.; Lauenstein, P.; Krahl, A.; Händel, N.; de Laffolie, J.; et al. Validation of Antibody-Based Strategies for Diagnosis of Pediatric Celiac Disease Without Biopsy. Gastroenterology 2017, 153, 410–419.e17. [Google Scholar] [CrossRef]
- Mubarak, A. Tissue Transglutaminase Levels above 100 U/mL and Celiac Disease: A Prospective Study. World J. Gastroenterol. 2012, 18, 4399. [Google Scholar] [CrossRef] [PubMed]
- Ciacci, C.; Bai, J.C.; Holmes, G.; Al-Toma, A.; Biagi, F.; Carroccio, A.; Ciccocioppo, R.; Di Sabatino, A.; Gingold-Belfer, R.; Jinga, M.; et al. Serum Anti-Tissue Transglutaminase IgA and Prediction of Duodenal Villous Atrophy in Adults with Suspected Coeliac Disease without IgA Deficiency (Bi.A.CeD): A Multicentre, Prospective Cohort Study. Lancet Gastroenterol. Hepatol. 2023, 8, 1005–1014. [Google Scholar] [CrossRef]
- Mott, T. A “No-Biopsy” Approach to Diagnosing Celiac Disease. J. Fam. Pr. 2022, 71, 359–361. [Google Scholar] [CrossRef] [PubMed]
- De Leo, L.; Bramuzzo, M.; Ziberna, F.; Villanacci, V.; Martelossi, S.; Leo, G.D.; Zanchi, C.; Giudici, F.; Pandullo, M.; Riznik, P.; et al. Diagnostic Accuracy and Applicability of Intestinal Auto-Antibodies in the Wide Clinical Spectrum of Coeliac Disease. EBioMedicine 2020, 51, 102567. [Google Scholar] [CrossRef]
- Bai, J.C.; Fried, M.; Corazza, G.R.; Schuppan, D.; Farthing, M.; Catassi, C.; Greco, L.; Cohen, H.; Ciacci, C.; Eliakim, R.; et al. World Gastroenterology Organisation Global Guidelines on Celiac Disease. J. Clin. Gastroenterol. 2013, 47, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Popp, A.; Mäki, M. Gluten-Induced Extra-Intestinal Manifestations in Potential Celiac Disease—Celiac Trait. Nutrients 2019, 11, 320. [Google Scholar] [CrossRef] [PubMed]
- Not, T.; Ziberna, F.; Vatta, S.; Quaglia, S.; Martelossi, S.; Villanacci, V.; Marzari, R.; Florian, F.; Vecchiet, M.; Sulic, A.-M.; et al. Cryptic Genetic Gluten Intolerance Revealed by Intestinal Antitransglutaminase Antibodies and Response to Gluten-Free Diet. Gut 2011, 60, 1487–1493. [Google Scholar] [CrossRef]
- Pallav, K.; Xu, H.; Leffler, D.A.; Kabbani, T.; Kelly, C.P. Immunoglobulin A Deficiency in Celiac Disease in the United States. J. Gastroenterol. Hepatol. 2016, 31, 133–137. [Google Scholar] [CrossRef]
- Lega, S.; De Leo, L.; Ziberna, F.; Grigoletto, V.; Gaita, B.; Giangreco, M.; Villanacci, V.; Bramuzzo, M.; Di Leo, G.; Not, T. Rapid Immunochromatography on Fresh Intestinal Biopsy Is Highly Accurate in Detecting Intestinal Antitransglutaminase Antibodies. Am. J. Gastroenterol. 2023, 118, 738–743. [Google Scholar] [CrossRef]
- Roca, M.; Donat, E.; Marco-Maestud, N.; Masip, E.; Hervás-Marín, D.; Ramos, D.; Polo, B.; Ribes-Koninckx, C. Efficacy Study of Anti-Endomysium Antibodies for Celiac Disease Diagnosis: A Retrospective Study in a Spanish Pediatric Population. J. Clin. Med. 2019, 8, 2179. [Google Scholar] [CrossRef] [PubMed]
- Auricchio, R.; Mandile, R.; Del Vecchio, M.R.; Scapaticci, S.; Galatola, M.; Maglio, M.; Discepolo, V.; Miele, E.; Cielo, D.; Troncone, R.; et al. Progression of Celiac Disease in Children with Antibodies Against Tissue Transglutaminase and Normal Duodenal Architecture. Gastroenterology 2019, 157, 413–420.e3. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Classical CD n = 25 | Potential CD n = 8 | Seronegative CD n = 1 | Not-Confirmed CD n = 6 | Controls n= 105 | |
|---|---|---|---|---|---|
| Female, n (%) | 12 (48%) | 8 (100%) | 1 (100%) | 6 (100%) | 69 (66%) |
| Age yr, median (range) | 29.5 (20–48) | 45 (18–71) | 69 | 44 (36–56) | 55 (19–85) |
| Symptoms, n (%) | 25 (100%) | 8 (100%) | 1 (100%) | 5 (83%) | 105 (100%) |
| intestinal | 22 | 8 | 1 | 4 | 104 |
| extraintestinal | 4 | 2 | – | 1 | 6 |
| Family history of CD, n (%) | – | – | – | – | 5 (5%) |
| Autoimmunity, n (%) | 3 (12%) | – | – | 1 (17%) | 6 (6%) |
| diabetes type 1 | 1 | – | – | – | – |
| gastritis | – | – | – | 1 | 6 |
| thyroiditis | 2 | – | – | 1 | 3 |
| IgA deficiency, n (%) | – | – | – | 1 (17%) | 1 (1%) |
| Classical CD n = 62 | Potential CD n = 13 | Seronegative CD n = 2 | Not-Confirmed CD n = 12 | Controls n= 57 | |
|---|---|---|---|---|---|
| Female, n (%) | 37 (60%) | 10 (77%) | 2 (100%) | 4 (33%) | 25 (44%) |
| Age yr, median (range) | 9 (2–18) | 10 (13–18) | 16 (14–18) | 12 (5–18) | 14 (2–18) |
| Symptoms, n (%) | 51 (82%) | 11 (85%) | 2 (100%) | 7 (58%) | 53 (93%) |
| intestinal | 33 | 9 | 1 | 5 | 47 |
| extraintestinal | 31 | 7 | 1 | 5 | 17 |
| Family history of CD, n (%) | 14 (22%) | 2 (15%) | – | 7 (58%) | 1 (2%) |
| Autoimmunity, n (%) | 4 (6%) | 1 (8%) | 2 (100%) | 2 (17%) | 3 (5%) |
| diabetes type 1 | 1 | 1 | – | – | 2 |
| thyroiditis | 3 | – | 2 | 2 | 1 |
| IgA deficiency, n (%) | – | 1 (8%) | – | – | – |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zanchi, C.; Ziberna, F.; Padoin, A.; Visintin, A.; Monica, F.; Simeth, C.; Cannizzaro, R.; Pelizzo, P.; Baragiotta, A.M.; Brosolo, P.; et al. Intestinal Anti-Endomysium Antibodies Are a Useful Tool for Diagnosing Celiac Disease in Pediatric and Adult Patients. Nutrients 2024, 16, 2979. https://doi.org/10.3390/nu16172979
Zanchi C, Ziberna F, Padoin A, Visintin A, Monica F, Simeth C, Cannizzaro R, Pelizzo P, Baragiotta AM, Brosolo P, et al. Intestinal Anti-Endomysium Antibodies Are a Useful Tool for Diagnosing Celiac Disease in Pediatric and Adult Patients. Nutrients. 2024; 16(17):2979. https://doi.org/10.3390/nu16172979
Chicago/Turabian StyleZanchi, Chiara, Fabiana Ziberna, Alessia Padoin, Alessia Visintin, Fabio Monica, Catrin Simeth, Renato Cannizzaro, Paola Pelizzo, Anna Maria Baragiotta, Piero Brosolo, and et al. 2024. "Intestinal Anti-Endomysium Antibodies Are a Useful Tool for Diagnosing Celiac Disease in Pediatric and Adult Patients" Nutrients 16, no. 17: 2979. https://doi.org/10.3390/nu16172979
APA StyleZanchi, C., Ziberna, F., Padoin, A., Visintin, A., Monica, F., Simeth, C., Cannizzaro, R., Pelizzo, P., Baragiotta, A. M., Brosolo, P., Zamora, J. P., Zilli, M., Fontana, G., Di Leo, G., Lega, S., Bramuzzo, M., Ronfani, L., De Leo, L., & Not, T. (2024). Intestinal Anti-Endomysium Antibodies Are a Useful Tool for Diagnosing Celiac Disease in Pediatric and Adult Patients. Nutrients, 16(17), 2979. https://doi.org/10.3390/nu16172979