The methodological framework for this chapter was designed to dissect the socio-demographic and nutritional contours of Chile’s most vulnerable households, based on the work done by [
5] focused on the determinants of household food security and dietary diversity during the COVID-19 pandemic in Bangladesh. Segregated into four strategic objectives, this chapter evaluates household composition, dietary intake patterns, the HDDS, and the development of a Spatial Warning System, each section providing a critical lens on different facets of food security. For the purposes of this research, the HDDS methodology was chosen due to its generality over other, more specific methods of measuring dietary diversity in households, such as methodologies focused on women suggested by [
1,
2], or on children [
1]. For the spatial visualization of food security, Ref. [
13] was used as a reference; however, spatial clustering analysis was not conducted due to concerns about low representativeness and high sensitivity to small data variations, which could hinder the identification of significant spatial patterns.
Until 2013, the FSPFS was focused on increasing family savings and security through self-production of food. Following an evaluation of the program, it was concluded that the saving capacity was difficult to measure and that it should shift focus to peoples’ “right to food”, paralleling a broader change of prioritization among those working for food security. Thus, from 2013 onwards, the program focused on safeguarding the consumption and diversity of food in the most vulnerable families in the country through the improvement of the availability of healthy foods and food education.
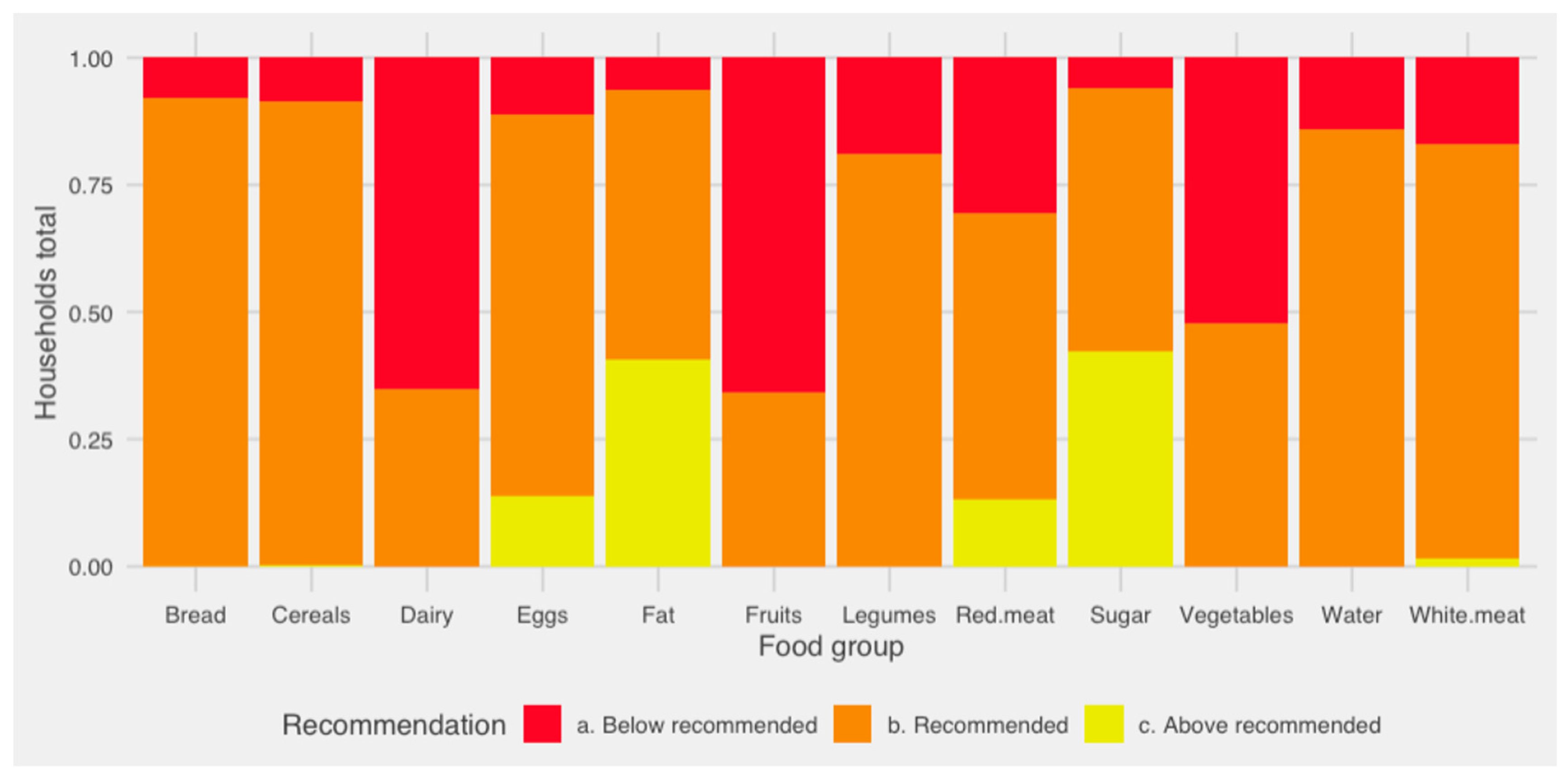
Each family responds to a specific diagnosis regarding their frequency of consumption for 12 food groups, which then lead to three types of recommendations: “below-recommended”, “recommended”, and “above-recommended”. Although the dietary recommendations for the Chilean population for the year 2009/2010 were taken as a reference, most are the result of the program’s own creation. For each of the 12 food groups, a frequency of consumption was defined in order to approximate, over a period of 1 month, dietary intake, and thus determine whether to work on a production technology if the consumption is below what is recommended, or focus on dietary education if consumption is above recommendations. The three categories mentioned above were created based on international standards and the previously mentioned dietary guidelines for the Chilean population and seek to make it easier for the executor, who is the figure that works directly with the families, to perform the job of uploading the information to the centralized system. However, the program recognizes that this type of question never provides information that is 100% accurate, since food guidelines should also be based on the territory, realities, and integrating cultural aspects. A total standardization can, among other things, end up suggesting a culturally or otherwise inappropriate way of asking about culinary or consumption patterns. Finally, one of the most recent modifications of the diagnostic instrument involved adding information on the consumption of the different food groups in terms of “quantity”, improving the accuracy provided by the information associated with the frequency of consumption.
Methods Employed by Objective
Objective 1—Socio-Demographic Analysis of Vulnerable Households: The first step involved a comprehensive analysis of the FSPFS survey, focusing on households identified in 2019 and expanded to include additional data from 2020. The investigation centered around socio-demographic characteristics, such as household headship, gender of the family head, and number of underaged family members. The analysis was further deepened into food security determinants, including food availability issues, food access issues and water access, and territorial determinants, including all macro-zones.
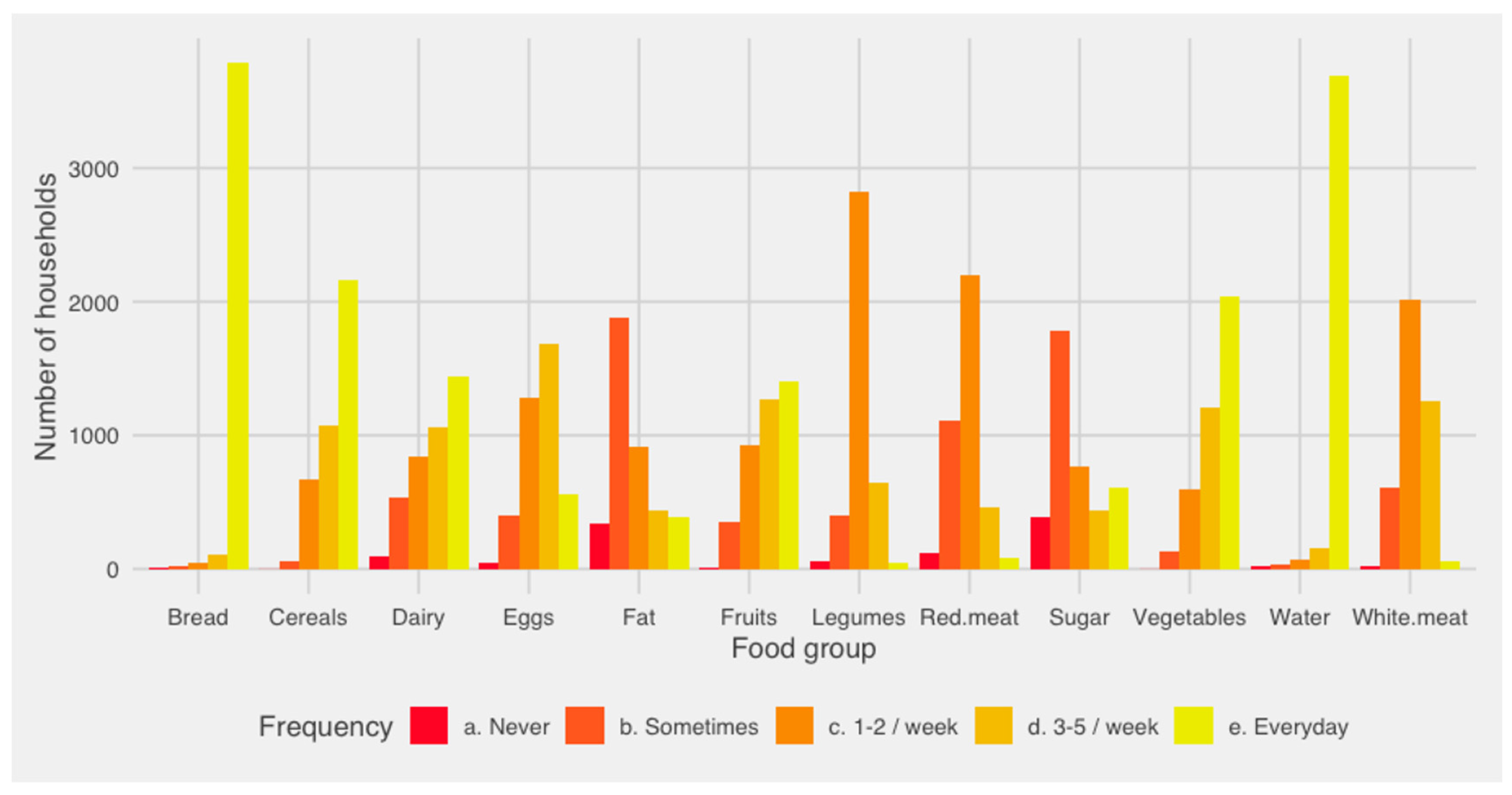
Objective 2—Dietary Intake Frequency Assessment: For the evaluation of dietary habits, a quantitative approach was adopted, which was based on categorizing the intake frequency of n = 12 food groups, listed below, according to national dietary guidelines and intake recommendations.
Vegetables
Fruits
Dairy
White meat
Red meat
Eggs
Legumes
Water
Bread
Cereals
Fat
Sugar
The assessment stratified households based on “below recommended”, “recommended” and “above recommended” intake levels, further dissecting consumption patterns into weekly intake frequencies (never [0 times/week]; sometimes [0.5 times/week]; [1–2 times/week]; [3–5 times/week]; every day [7 times/week]) to provide a detailed portrayal of the dietary landscape among Chile’s vulnerable populations.
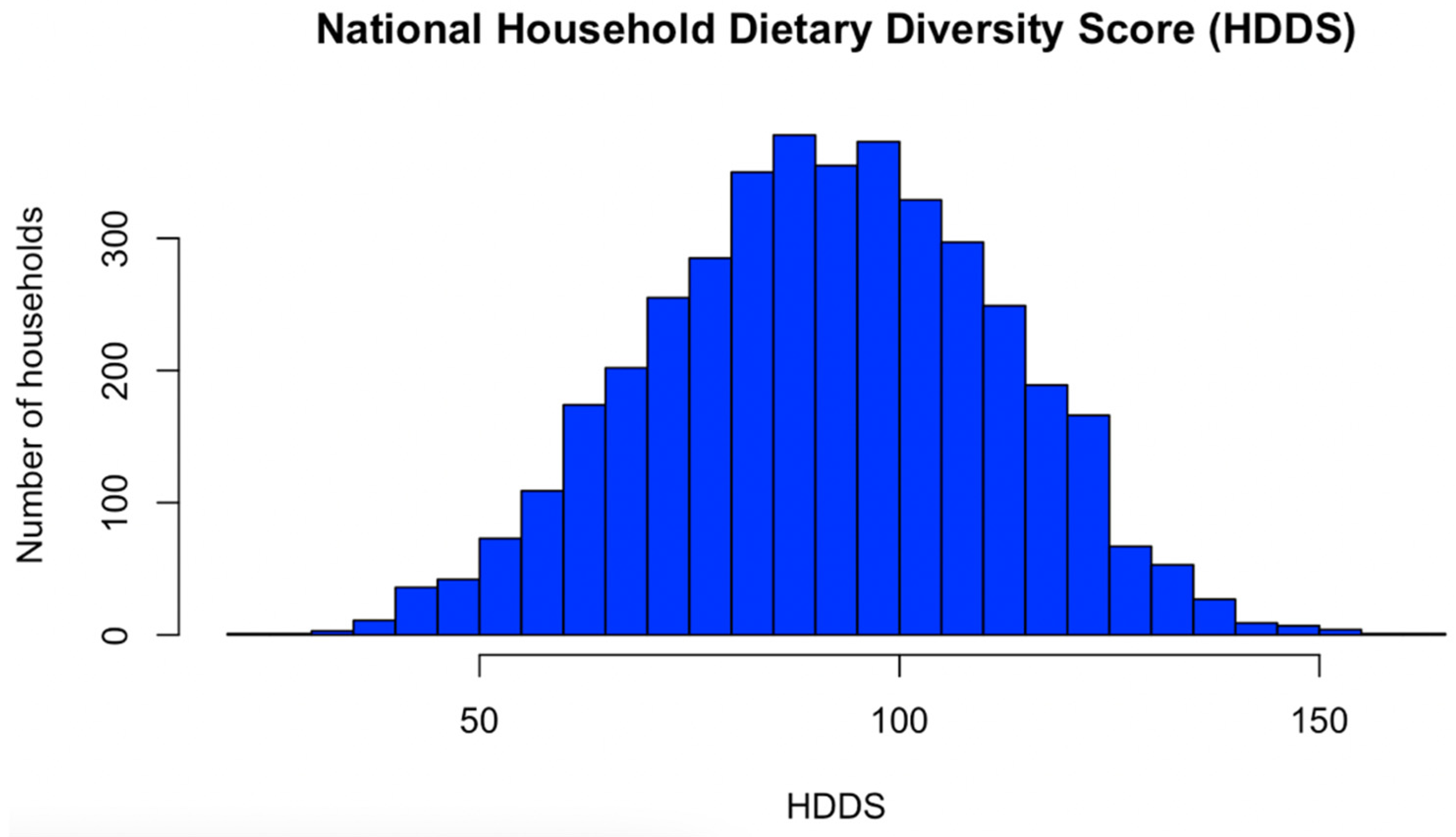
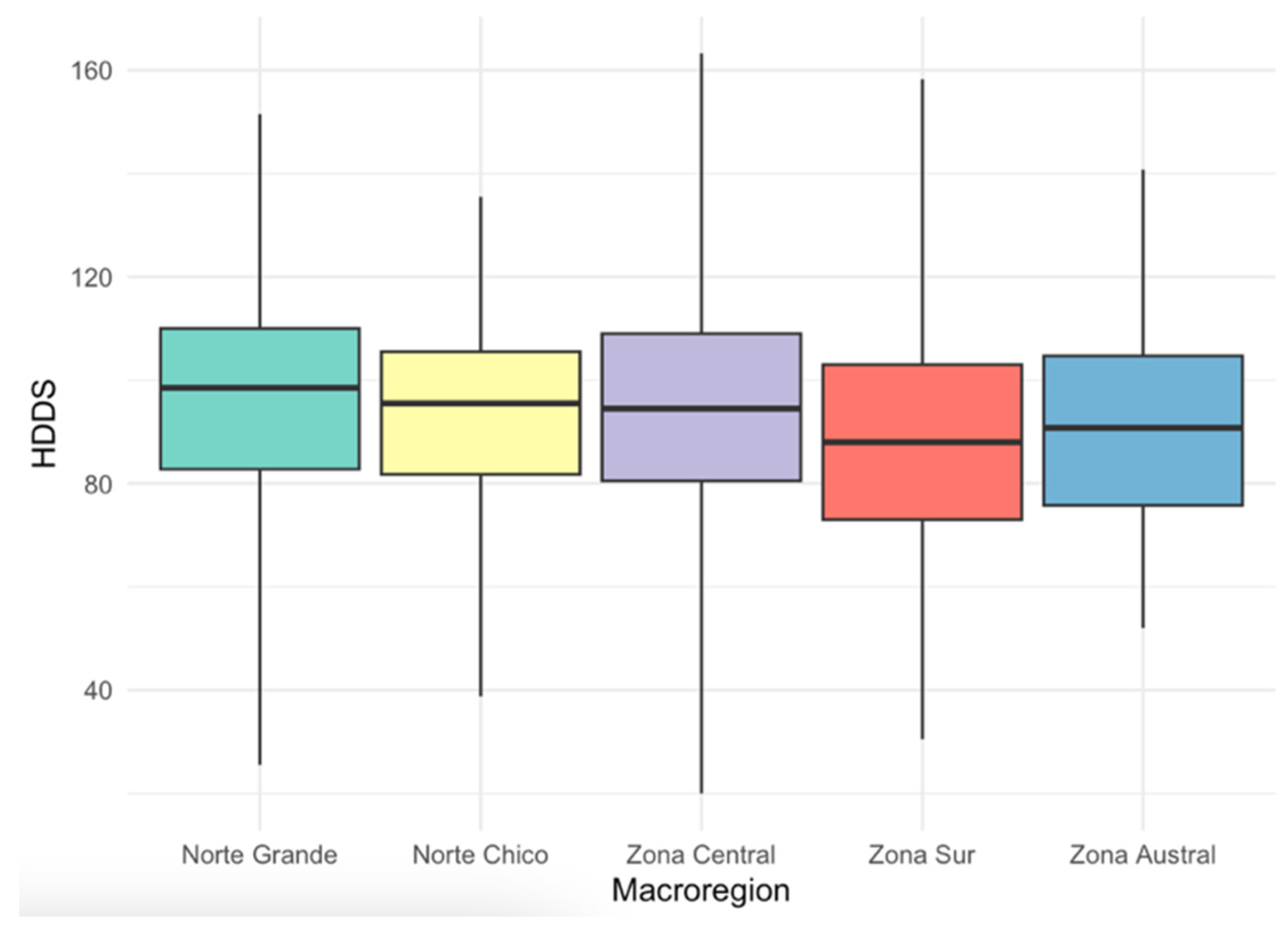
Objective 3—Dietary Diversity Score Calculation and Analysis: The HDDS served as a pivotal metric in this phase, calculated for a sizable cohort to explore correlations with socio-demographic variables, food security determinants, and regional disparities. This objective employed descriptive statistics for a national-level dietary diversity overview, while regional scores were scrutinized to pinpoint macro-zone dietary patterns. Multivariate regression techniques were applied to assess the impact of various socio-demographic and food security factors, alongside geographical considerations, on the HDDS.
The calculation of the HDDS for each household was conducted in several steps utilizing the data on weekly intake frequencies of n = 12 food groups from the FSPFS diagnosis. The methodology employed is outlined as follows:
- a.
Quantification of Intake Frequencies: The weekly intake frequency of each food group was recorded as (Household Weekly Frequency), where i represents each of the 12 food groups. The frequency was quantified on a scale based on the reported intake:
- -
Never [0 times/week] = 0
- -
Twice per month [0.5 times/week] = 0.5
- -
1–2 times/week = 1.5
- -
3–5 times/week = 4
- -
Every day [7 times/week] = 7
- b.
Weighting of Food Groups: Each
was then multiplied by a weight factor
specific to each food group to reflect its importance in the diet, as shown in
Table 3. The weight factors
were derived from [
26] nutritional guidelines that emphasize the relative nutritional contribution of each food group:
- c.
Calculation of HDDS: The HDDS for each household was calculated by summing the weighted frequencies of all 12 food groups:
The final HDDS is a summative score that indicates the dietary diversity of the household, serving as a proxy for nutritional adequacy. Higher HDDS values suggest greater dietary diversity and, potentially, better household nutritional status.
Using the “lm” function in R, a multilinear regression model with HDDS as the dependent variable was constructed. The model included Head of Household Age, Gender, Underaged family members, Food Access Issues, Food Availability Issues, Water Access, and Macro-zone as independent variables. To assess the collinearity among the variables in the dataset, a Variance Inflation Factor (VIF) test was employed by calculating VIF values for each predictor using the “vif” function from the “car” package. A VIF value exceeding 5 was considered indicative of significant collinearity.
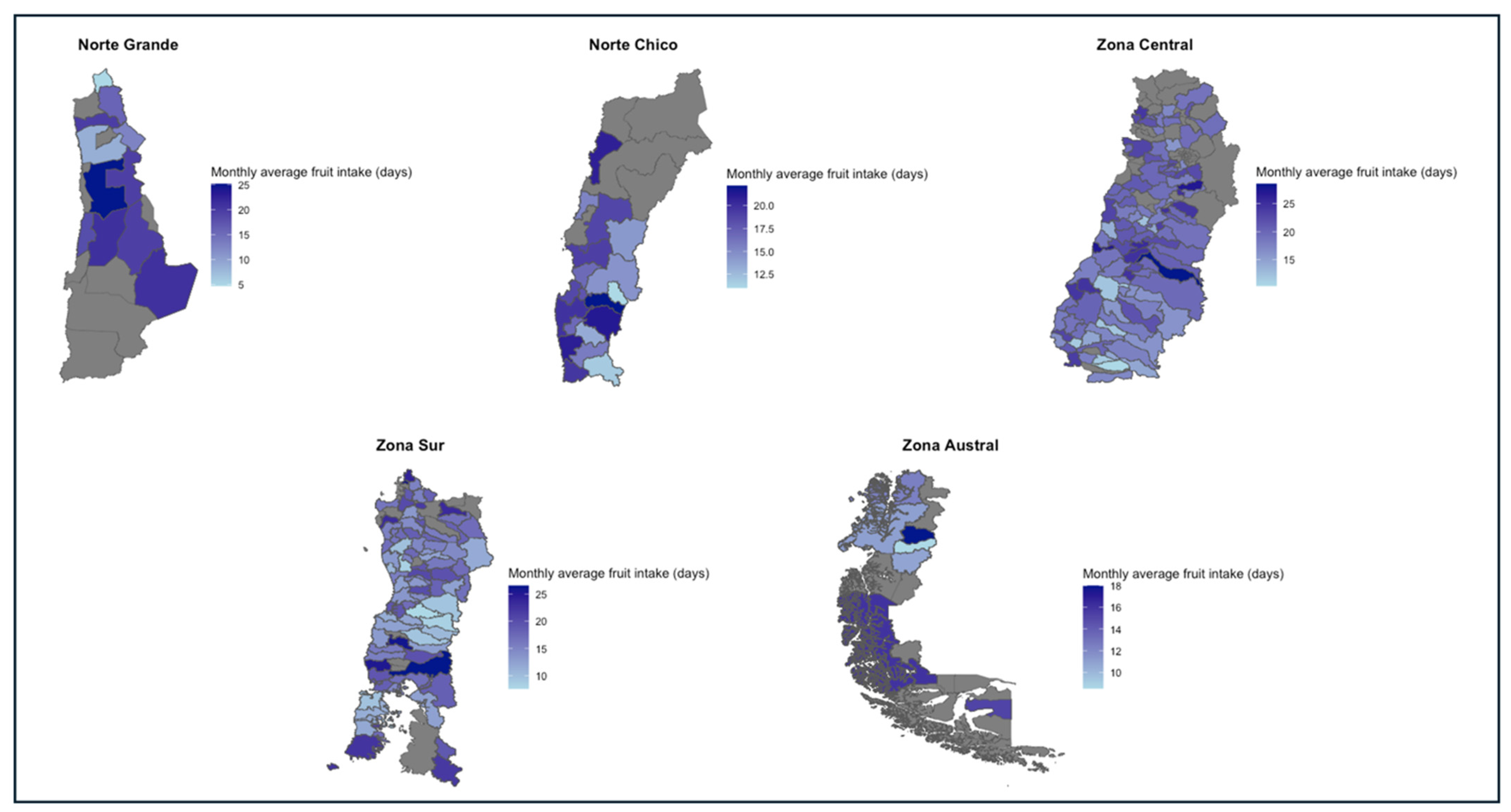
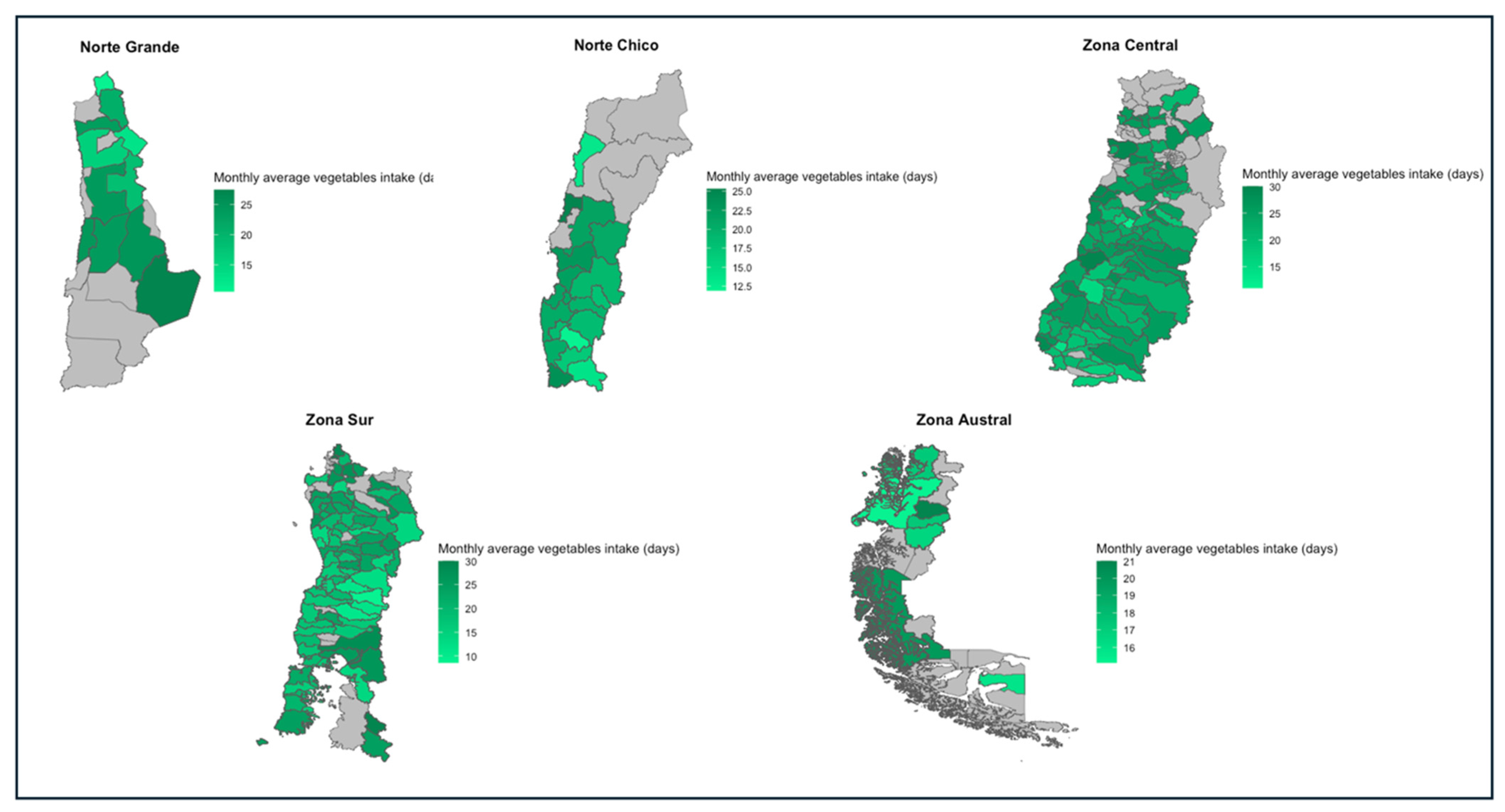
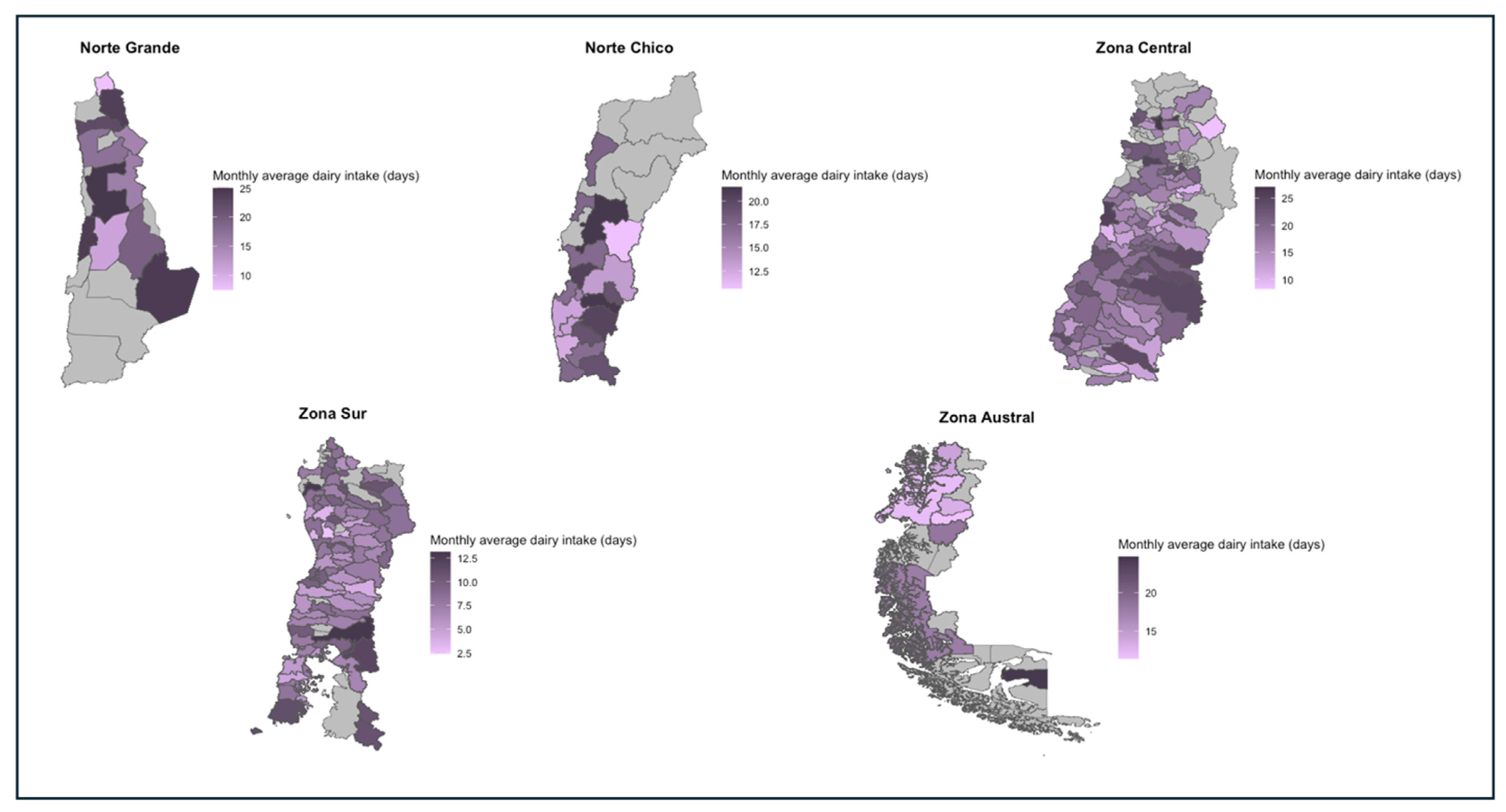
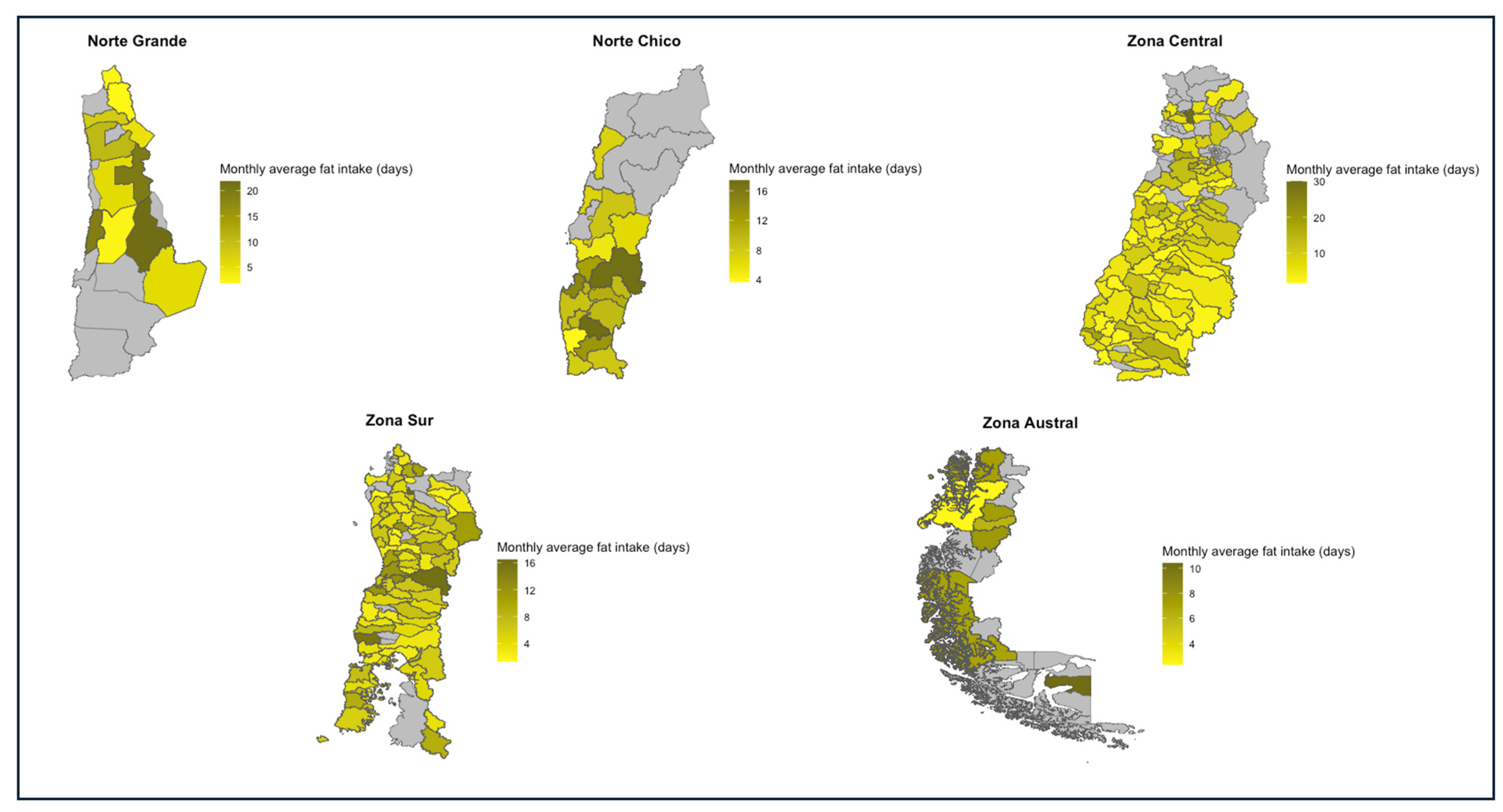
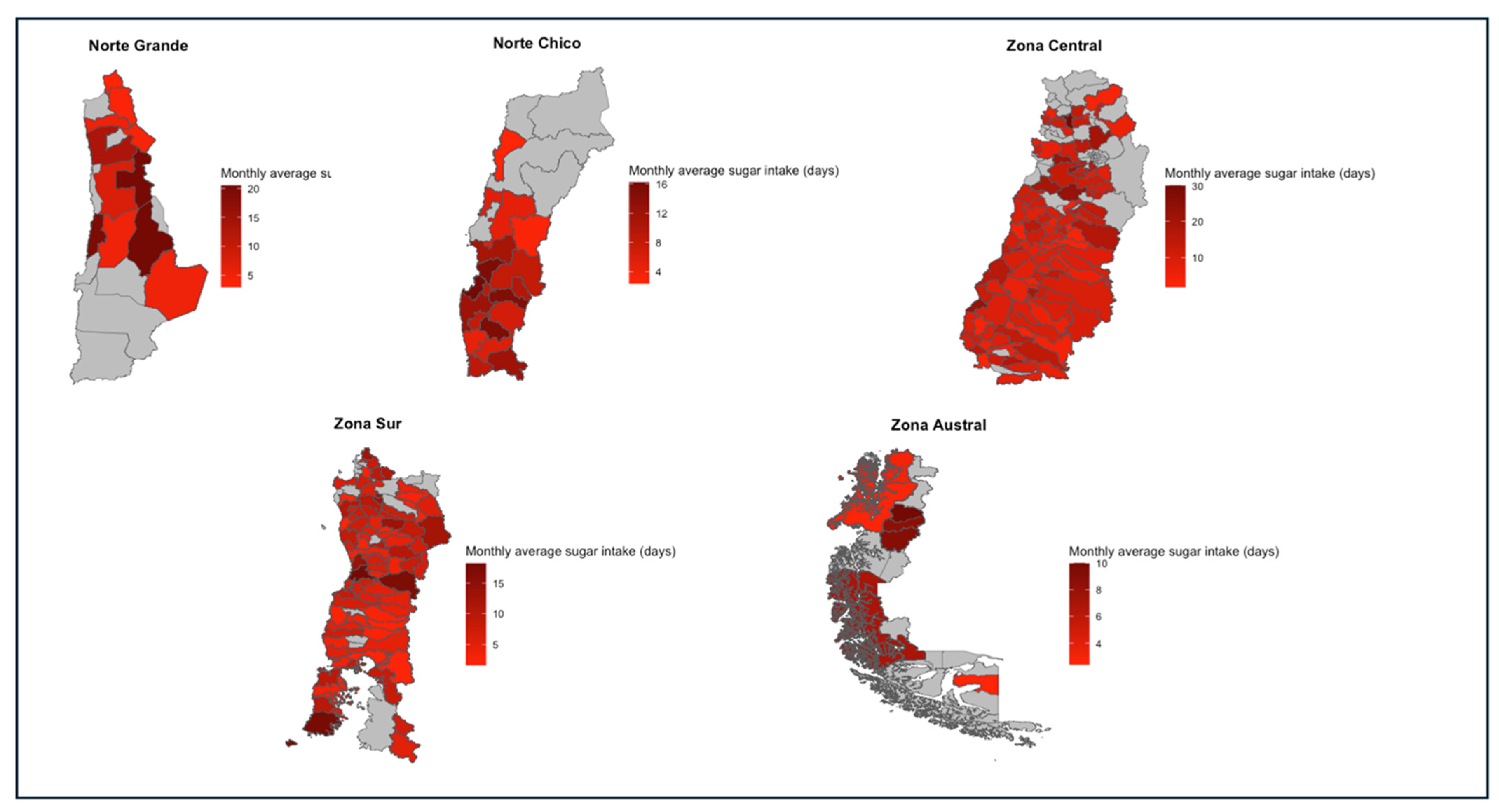
Objective 4—Development of a Spatial Warning System: The data for this objective analysis were extracted from the diagnostic surveys from the FSPFS database. Based on Objective 2 of our preliminary analysis, which identified problematic food group intakes, five critical food groups were selected: fruits, vegetables, dairy products, sugars, and fats. These groups were chosen due to their significant deviation from the recommended intake levels—fruits, vegetables, and dairy intake were typically under the recommended thresholds, while sugars and fats were consumed above the recommended thresholds.
Descriptive statistics were computed for each of the five critical food groups across all macro-zones. For the data analysis, the RStudio environment was utilized with its packages “tidyverse”, “chilemapas”, “sf”, “ggplot2”, and “dplyr”. The monthly intake averages were calculated to determine the mean number of days each food group was consumed. To capture the variability in consumption patterns, we identified the highest and lowest intake frequencies, along with the corresponding number and percentage of households. The mode representing the most common reported intake frequency was also calculated along with its prevalence among the households. To quantify the degree of intake deficiency, we determined the percentage of households consuming at/below/above the recommended levels for each food group.
The spatial visualization analysis of the five critical food groups’ intakes across macro-zones in Chile involved the following steps of data processing and geographical mapping:
- a.
Conversion of Weekly Intake Frequency to Monthly Frequency:
Since the data provided by the FSPFS diagnosis survey considered a weekly intake, the function
was defined to convert weekly frequency intake to monthly frequency intake.
- b.
Calculation of Commune-Level Averages
For each commune, i.e., the smallest administrative division in Chile, the average monthly frequency intake, defined as
was calculated, by aggregating individual household monthly frequency intakes for a given food group
and then dividing by the total number of households in the commune.
where
is the number of households in the commune.
Each commune’s CommuneAverage(i) was georeferenced using its coordinates provided by the “chilemapas” package in RStudio. This process involved associating the calculated average intake values with their respective spatial locations on the Chilean map.
A Choropleth map was applied to represent the average intake values. Communes with higher average intakes of a particular food group are displayed in darker shades, while those with lower average intakes are shown in lighter shades. This gradient visually represents the distribution of intake frequencies across different communes and macro-zones.
We identified and grouped communes within the macro-zones based on the proportion of households with intake levels below the recommended threshold for fruits, vegetables, and dairy, and above the recommended threshold for fats and sugars. The benchmark for categorization was set at 50% or more of households deviating from the recommended intake levels.
For visual representation, we employed a horizontal barplot with a red gradient fill, where the intensity of the red color corresponded to the proportion of households in each commune with above or below the recommended dietary intake. The gradient provided a visual scale of adherence to dietary recommendations, with darker shades indicating a higher percentage of households not meeting the recommended intake. The analysis was designed to yield both visual and quantitative interpretations of dietary patterns, facilitating the development of targeted nutritional interventions. The formula employed for determining the thresholds was
where a proportion equal to or greater than 50% indicated a significant deviation from recommended dietary patterns. The proportion of households not meeting the recommendations per food group in different macro-zones can be found in
Supplementary Material.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}