
Appropriateness of Ketoanalogues of Amino Acids, Calcium Citrate, and Inulin Supplementation for CKD Management: A RAND/UCLA Consensus

 , ,
, ,  , , ,
, , ,  ,
,  ,
,  and add
Show full author list
and add
Show full author list
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
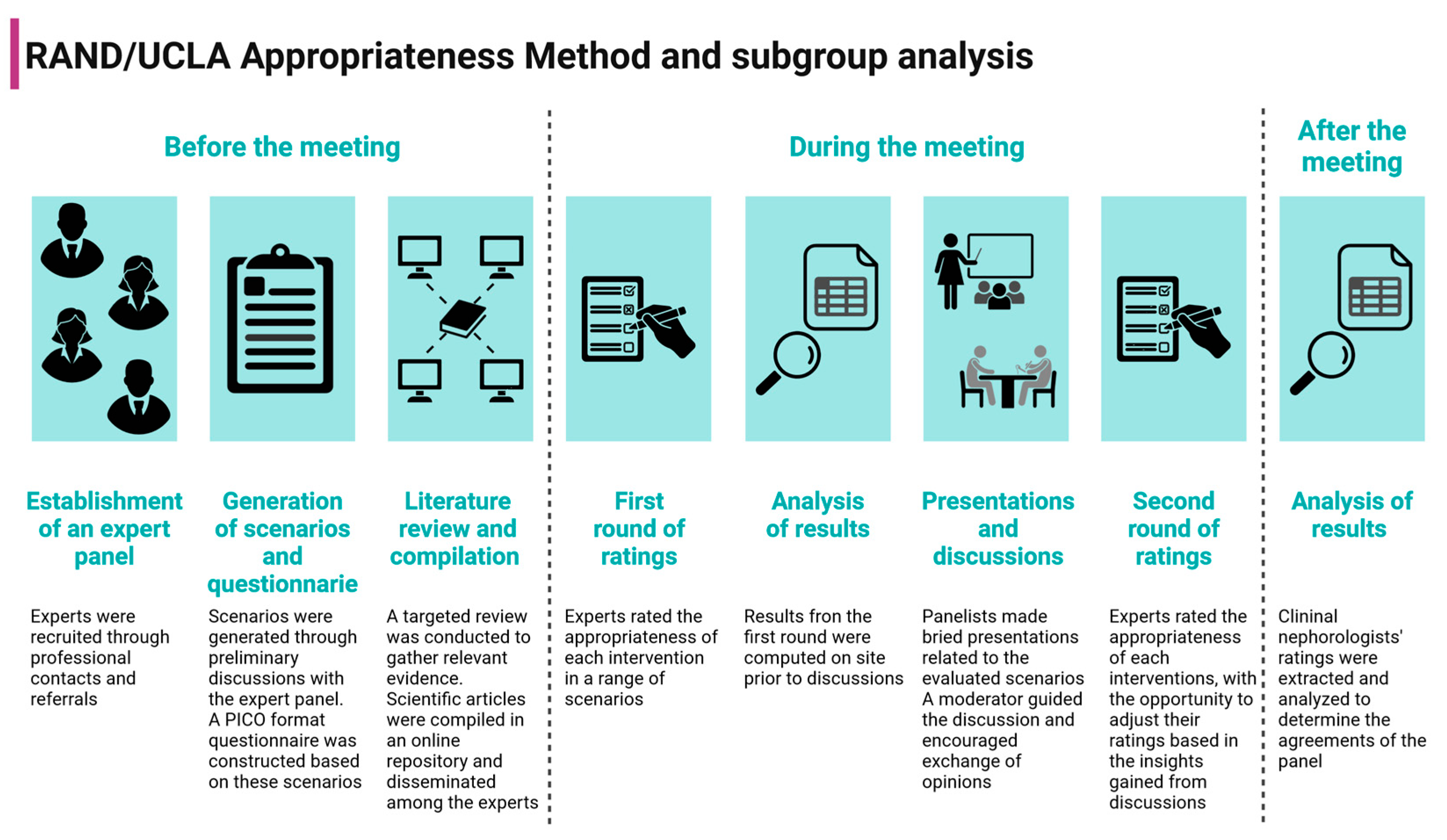
2.1. RAND/UCLA Appropriateness Method
2.2. Establishment of an Expert Panel
2.3. Generation of Scenarios and Literature Review
2.4. Two-Round Consensus
2.5. Statistical Analysis
2.6. Ethical Compliance
3. Results
3.1. Summary of Participants and Answers
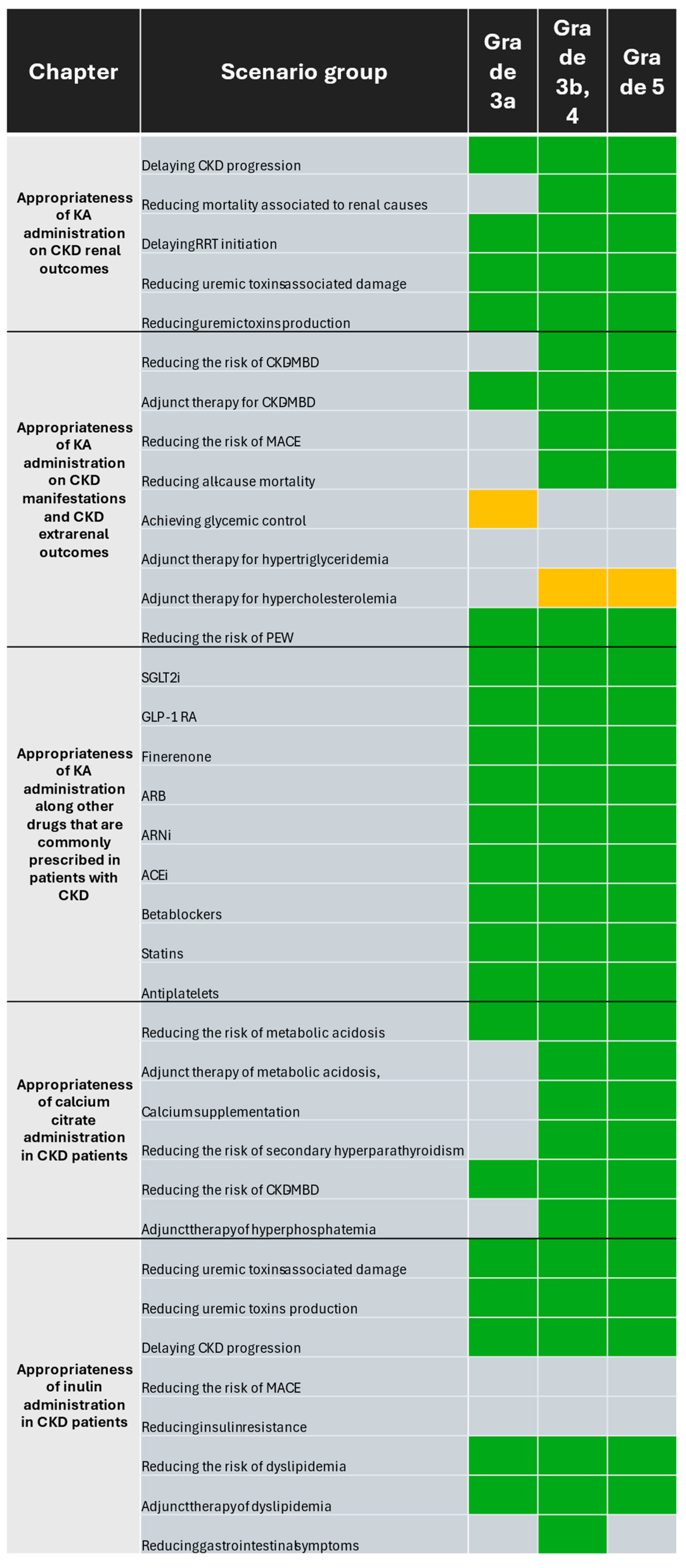
3.2. Appropriateness of Ketoanalogues of Amino Acid Supplementation on Chronic Kidney Disease Renal Outcomes
3.3. Appropriateness of Ketoanalogues of Amino Acid Supplementation on Chronic Kidney Disease Manifestations and Extrarenal Outcomes
3.4. Appropriateness of Ketoanalogues of Amino Acid Supplementation along with Other Drugs That Are Commonly Prescribed in Patients with Chronic Kidney Disease
3.5. Appropriateness of Calcium Citrate Supplementation in Chronic Kidney Disease Patients
3.6. Appropriateness of Inulin Supplementation in Chronic Kidney Disease Patients
4. Discussion
4.1. Supplementation of Low-Protein Diets and Very Low-Protein Diets with Ketoanalogues of Amino Acids Is Considered Appropriate to Reduce Manifestations and Delay Outcomes in Chronic Kidney Disease Patients
4.2. Supplementation with Calcium Citrate Is Considered Appropriate to Reduce Manifestations of Chronic Kidney Disease
4.3. Supplementation with Inulin Is Considered Appropriate to Delay Chronic Kidney Disease Outcomes and Manage Comorbidities
4.4. Future Perspectives
4.5. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kovesdy, C.P. Epidemiology of Chronic Kidney Disease: An Update 2022. Kidney Int. Suppl. 2022, 12, 7–11. [Google Scholar] [CrossRef]
- Liyanage, T.; Ninomiya, T.; Jha, V.; Neal, B.; Patrice, H.M.; Okpechi, I.; Zhao, M.H.; Lv, J.; Garg, A.X.; Knight, J.; et al. Worldwide Access to Treatment for End-Stage Kidney Disease: A Systematic Review. Lancet 2015, 385, 1975–1982. [Google Scholar] [CrossRef]
- Bikbov, B.; Purcell, C.A.; Levey, A.S.; Smith, M.; Abdoli, A.; Abebe, M.; Adebayo, O.M.; Afarideh, M.; Agarwal, S.K.; Agudelo-Botero, M.; et al. Global, Regional, and National Burden of Chronic Kidney Disease, 1990–2017: A Systematic Analysis for the Global Burden of Disease Study 2017. Lancet 2020, 395, 709–733. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes CKD Work Group. KDIGO 2024 Clinical Practice Guideline for the Evaluation and Management of Chronic Kidney Disease. Kidney Int. 2024, 105, s117–s314. [Google Scholar] [CrossRef]
- Noce, A.; Marchetti, M.; Marrone, G.; Di Renzo, L.; Di Lauro, M.; Di Daniele, F.; Albanese, M.; Di Daniele, N.; De Lorenzo, A. Link between Gut Microbiota Dysbiosis and Chronic Kidney Disease. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 2057–2074. [Google Scholar]
- Ikizler, T.A.; Burrowes, J.D.; Byham-Gray, L.D.; Campbell, K.L.; Carrero, J.J.; Chan, W.; Fouque, D.; Friedman, A.N.; Ghaddar, S.; Goldstein-Fuchs, D.J.; et al. KDOQI Clinical Practice Guideline for Nutrition in CKD: 2020 Update. Am. J. Kidney Dis. 2020, 76, S1–S107. [Google Scholar] [CrossRef]
- Saavedra Fuentes, N.E.; Carmona Montesinos, E.; Castañeda Hernández, G.; Campos, I.; Castillo Salinas, J.C.; Castillo Tapia, J.A.; Del Castillo Loreto, K.G.; Falcon Martínez, J.C.; Fuentes García, R.; García de Leon Guerrero, M.Á.; et al. Consenso Mexicano Del Uso De Alfacetoanálogos Sobre Diferentes Desenlaces En El Paciente Con Enfermedad Renal Crónica. Nefrol. Mex. 2024, 45 (Suppl. S1). [Google Scholar]
- Fitch, K.; Bernstein, S.J.; Aguilar, M.D.; Burnand, B.; LaCalle, J.R.; Lazaro, P.; van het Loo, M.; McDonnell, J.; Vader, J.; Kahan, J.P. The Rand/UCLA Appropriateness Method User’s Manual; Rand: Santa Monica, CA, USA, 2001; ISBN 0833029185. [Google Scholar]
- Masuda, E.; Ozsvath, K.; Vossler, J.; Woo, K.; Kistner, R.; Lurie, F.; Monahan, D.; Brown, W.; Labropoulos, N.; Dalsing, M.; et al. The 2020 Appropriate Use Criteria for Chronic Lower Extremity Venous Disease of the American Venous Forum, the Society for Vascular Surgery, the American Vein and Lymphatic Society, and the Society of Interventional Radiology. J. Vasc. Surg. Venous Lymphat. Disord. 2020, 8, 505–525.e4. [Google Scholar] [CrossRef]
- Woo, K.; Ulloa, J.; Allon, M.; Carsten, C.G.; Chemla, E.S.; Henry, M.L.; Huber, T.S.; Lawson, J.H.; Lok, C.E.; Peden, E.K.; et al. Establishing Patient-Specific Criteria for Selecting the Optimal Upper Extremity Vascular Access Procedure. J. Vasc. Surg. 2017, 65, 1089–1103.e1. [Google Scholar] [CrossRef]
- Saust, L.T.; Siersma, V.D.; Bjerrum, L.; Hansen, M.P. Development of Quality Indicators for the Diagnosis and Treatment of Urinary Tract Infections in General Practice: A RAND Appropriateness Method. BMJ Open Qual. 2023, 12, e002156. [Google Scholar] [CrossRef]
- Broder, M.S.; Adams, D.M.; Canaud, G.; Collins, C.; Davis, K.; Frieden, I.J.; Gibbs, S.N.; Hammill, A.M.; Kep-pler-Noreuil, K.M.; Nakano, T.A.; et al. RAND/UCLA Modified Delphi Panel on the Severity, Testing, and Medical Management of PIK3CA-Related Spectrum Disorders (PROS). J. Vasc. Anom. 2023, 4, e067. [Google Scholar] [CrossRef]
- Carson-Stevens, A.; Campbell, S.; Bell, B.G.; Cooper, A.; Armstrong, S.; Ashcroft, D.; Boyd, M.; Prosser Evans, H.; Mehta, R.; Sheehan, C.; et al. Identifying ‘Avoidable Harm’ in Family Practice: A RAND/UCLA Appropriateness Method Consensus Study. BMC Fam. Pract. 2019, 20, 134. [Google Scholar] [CrossRef] [PubMed]
- Broder, M.S.; Gibbs, S.N.; Yermilov, I. An Adaptation of the RAND/UCLA Modified Delphi Panel Method in the Time of COVID-19. J. Healthc. Leadersh. 2022, 14, 63–70. [Google Scholar] [CrossRef]
- Kalantar-Zadeh, K.; Jafar, T.H.; Nitsch, D.; Neuen, B.L.; Perkovic, V. Chronic Kidney Disease. Lancet 2021, 398, 786–802. [Google Scholar] [CrossRef]
- Lim, Y.J.; Sidor, N.A.; Tonial, N.C.; Che, A.; Urquhart, B.L. Uremic Toxins in the Progression of Chronic Kidney Disease and Cardiovascular Disease: Mechanisms and Therapeutic Targets. Toxins 2021, 13, 142. [Google Scholar] [CrossRef] [PubMed]
- Li, A.; Lee, H.Y.; Lin, Y.C. The Effect of Ketoanalogues on Chronic Kidney Disease Deterioration: A Meta-Analysis. Nutrients 2019, 11, 957. [Google Scholar] [CrossRef]
- Jiang, Z.; Zhang, X.; Yang, L.; Li, Z.; Qin, W. Effect of Restricted Protein Diet Supplemented with Keto Analogues in Chronic Kidney Disease: A Systematic Review and Meta-Analysis. Int. Urol. Nephrol. 2016, 48, 409–418. [Google Scholar] [CrossRef]
- Yen, C.L.; Fan, P.C.; Lee, C.C.; Kuo, G.; Tu, K.H.; Chen, J.J.; Lee, T.H.; Hsu, H.H.; Tian, Y.C.; Chang, C.H. Advanced Chronic Kidney Disease with Low and Very Low GFR: Can a Low-Protein Diet Supplemented with Ketoanalogues Delay Dialysis? Nutrients 2020, 12, 3358. [Google Scholar] [CrossRef]
- Chen, H.Y.; Sun, C.Y.; Lee, C.C.; Wu, I.W.; Chen, Y.C.; Lin, Y.H.; Fang, W.C.; Pan, H.C. Ketoanalogue Supplements Reduce Mortality in Patients with Pre-Dialysis Advanced Diabetic Kidney Disease: A Nationwide Population-Based Study. Clin. Nutr. 2021, 40, 4149–4160. [Google Scholar] [CrossRef]
- Wu, C.H.; Yang, Y.W.; Hung, S.C.; Kuo, K.L.; Wu, K.D.; Wu, V.C.; Hsieh, T.C. Ketoanalogues Supplementation Decreases Dialysis and Mortality Risk in Patients with Anemic Advanced Chronic Kidney Disease. PLoS ONE 2017, 12, e0176847. [Google Scholar] [CrossRef]
- Cecchi, S.; Di Stante, S.; Belcastro, S.; Bertuzzi, V.; Cardillo, A.; Diotallevi, L.; Grabocka, X.; Kulurianu, H.; Martello, M.; Nastasi, V.; et al. Supplemented Very Low Protein Diet (SVLPD) in Patients with Advanced Chronic Renal Failure: Clinical and Economic Benefits. Nutrients 2023, 15, 3568. [Google Scholar] [CrossRef]
- Shah, A.P.; Kalantar-Zadeh, K.; Kopple, J.D. Is There a Role for Ketoacid Supplements in the Management of CKD? Am. J. Kidney Dis. 2015, 65, 659–673. [Google Scholar] [CrossRef]
- Marzocco, S.; Dal Piaz, F.; Di Micco, L.; Torraca, S.; Sirico, M.L.; Tartaglia, D.; Autore, G.; Di Iorio, B. Very Low Protein Diet Reduces Indoxyl Sulfate Levels in Chronic Kidney Disease. Blood Purif. 2013, 35, 196–201. [Google Scholar] [CrossRef]
- Koppe, L.; De Oliveira, M.C.; Fouque, D. Ketoacid Analogues Supplementation in Chronic Kidney Disease and Future Perspectives. Nutrients 2019, 11, 2071. [Google Scholar] [CrossRef]
- Huynh, T.N.P.; Nguyen, T.M.; Povero, M.; Pradelli, L. Economic Analysis of a Ketoanalogue-Supplemented Very Low-Protein Diet in Patients With Chronic Kidney Disease in Vietnam. Clin. Ther. 2023, 45, 649–654. [Google Scholar] [CrossRef]
- Ndumele, C.E.; Neeland, I.J.; Tuttle, K.R.; Chow, S.L.; Mathew, R.O.; Khan, S.S.; Coresh, J.; Baker-Smith, C.M.; Carnethon, M.R.; Després, J.P.; et al. A Synopsis of the Evidence for the Science and Clinical Management of Cardiovascular-Kidney-Metabolic (CKM) Syndrome: A Scientific Statement from the American Heart Association. Circulation 2023, 148, 1636–1664. [Google Scholar] [CrossRef]
- Cupisti, A.; Giannese, D.; Moriconi, D.; D’Alessandro, C.; Torreggiani, M.; Piccoli, G.B. Nephroprotection by SGLT2i in CKD Patients: May It Be Modulated by Low-Protein Plant-Based Diets? Front. Med. 2020, 7, 622593. [Google Scholar] [CrossRef]
- Palermo, A.; Naciu, A.M.; Tabacco, G.; Manfrini, S.; Trimboli, P.; Vescini, F.; Falchetti, A. Calcium Citrate: From Biochemistry and Physiology to Clinical Applications. Rev. Endocr. Metab. Disord. 2019, 20, 353–364. [Google Scholar] [CrossRef]
- Gadola, L.; Noboa, O.; Marquez, M.N.; Rodriguez, M.J.; Nin, N.; Boggia, J.; Ferreiro, A.; Garcia, S.; Ortega, V.; Musto, M.L.; et al. Calcium Citrate Ameliorates the Progression of Chronic Renal Injury. Kidney Int. 2004, 65, 1224–1230. [Google Scholar] [CrossRef]
- Cabalgante, M.J.R.; Gadola, L.; Luzardo, L.; Márquez, M.; Boggia, J.; Boim, M.A. Calcium Citrate Improves the Epithelial-to-Mesenchymal Transition Induced by Acidosis in Proximal Tubular Cells. J. Bras. Nefrol. 2012, 34, 343–348. [Google Scholar] [CrossRef]
- Quiñones, H.; Hamdi, T.; Sakhaee, K.; Pasch, A.; Moe, O.W.; Pak, C.Y.C. Control of Metabolic Predisposition to Cardiovascular Complications of Chronic Kidney Disease by Effervescent Calcium Magnesium Citrate: A Feasibility Study. J. Nephrol. 2019, 32, 93–100. [Google Scholar] [CrossRef] [PubMed]
- Cushner, H.M.; Copley, J.B.; Lindberg, J.S.; Foulks, C.J. Calcium Citrate, a Nonaluminum-Containing Phosphate-Binding Agent for Treatment of CRF. Kidney Int. 1988, 33, 95–99. [Google Scholar] [CrossRef] [PubMed]
- Saupe, J.; Belmega, G.; Krause, R.; Bennhold, I. Management of Hyperphosphatemia with Calcium Citrate in Hemodialysis Patients. Nephron 1989, 52, 93–94. [Google Scholar] [CrossRef]
- Saha, H.; Pietilä, K.; Mustonen, J.; Pasternacka, A.; Mörsky, P.; Seppälä, E.; Reinikainenc, P. Acute Effects of Calcium Carbonate and Citrate on Secondary Hyperparathyroidism in Chronic Renal Failure. Am. J. Nephrol. 1991, 11, 465–469. [Google Scholar] [CrossRef]
- Nguyen, T.T.U.; Kim, H.W.; Kim, W. Effects of Probiotics, Prebiotics, and Synbiotics on Uremic Toxins, Inflammation, and Oxidative Stress in Hemodialysis Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2021, 10, 4456. [Google Scholar] [CrossRef] [PubMed]
- Chang, L.; Tian, R.; Guo, Z.; He, L.; Li, Y.; Xu, Y.; Zhang, H. Low-Protein Diet Supplemented with Inulin Lowers Protein-Bound Toxin Levels in Patients with Stage 3b-5 Chronic Kidney Disease: A Randomized Controlled Study. Nutr. Hosp. 2023, 40, 819–828. [Google Scholar] [CrossRef]
- Lai, S.; Mazzaferro, S.; Muscaritoli, M.; Mastroluca, D.; Testorio, M.; Perrotta, A.; Esposito, Y.; Carta, M.; Campagna, L.; Di Grado, M.; et al. Prebiotic Therapy with Inulin Associated with Low Protein Diet in Chronic Kidney Disease Patients: Evaluation of Nutritional, Cardiovascular and Psychocognitive Parameters. Toxins 2020, 12, 381. [Google Scholar] [CrossRef]
- McFarlane, C.; Ramos, C.I.; Johnson, D.W.; Campbell, K.L. Prebiotic, Probiotic, and Synbiotic Supplementation in Chronic Kidney Disease: A Systematic Review and Meta-Analysis. J. Ren. Nutr. 2019, 29, 209–220. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saavedra-Fuentes, N.; Carmona-Montesinos, E.; Castañeda-Hernández, G.; Campos, I.; Castillo-Salinas, J.C.; Castillo-Tapia, J.A.; Del Castillo-Loreto, K.G.; Falcón-Martínez, J.C.; Fuentes-García, R.; García de León Guerrero, M.Á.; et al. Appropriateness of Ketoanalogues of Amino Acids, Calcium Citrate, and Inulin Supplementation for CKD Management: A RAND/UCLA Consensus. Nutrients 2024, 16, 2930. https://doi.org/10.3390/nu16172930
Saavedra-Fuentes N, Carmona-Montesinos E, Castañeda-Hernández G, Campos I, Castillo-Salinas JC, Castillo-Tapia JA, Del Castillo-Loreto KG, Falcón-Martínez JC, Fuentes-García R, García de León Guerrero MÁ, et al. Appropriateness of Ketoanalogues of Amino Acids, Calcium Citrate, and Inulin Supplementation for CKD Management: A RAND/UCLA Consensus. Nutrients. 2024; 16(17):2930. https://doi.org/10.3390/nu16172930
Chicago/Turabian StyleSaavedra-Fuentes, Nadia, Enrique Carmona-Montesinos, Gilberto Castañeda-Hernández, Israel Campos, Juan Carlos Castillo-Salinas, Javier Alberto Castillo-Tapia, Karla Guadalupe Del Castillo-Loreto, Juan Carlos Falcón-Martínez, Raquel Fuentes-García, Miguel Ángel García de León Guerrero, and et al. 2024. "Appropriateness of Ketoanalogues of Amino Acids, Calcium Citrate, and Inulin Supplementation for CKD Management: A RAND/UCLA Consensus" Nutrients 16, no. 17: 2930. https://doi.org/10.3390/nu16172930
APA StyleSaavedra-Fuentes, N., Carmona-Montesinos, E., Castañeda-Hernández, G., Campos, I., Castillo-Salinas, J. C., Castillo-Tapia, J. A., Del Castillo-Loreto, K. G., Falcón-Martínez, J. C., Fuentes-García, R., García de León Guerrero, M. Á., García-García, V., Gómez-García, E. F., González-Toledo, R., Jaime, A., Rely, K., Lerma, C., Morales-Buenrostro, L. E., Quilantan-Rodriguez, M., Rodriguez-Matías, A., ... Ramirez-Ramirez, E. (2024). Appropriateness of Ketoanalogues of Amino Acids, Calcium Citrate, and Inulin Supplementation for CKD Management: A RAND/UCLA Consensus. Nutrients, 16(17), 2930. https://doi.org/10.3390/nu16172930