
The Prevention of Childhood Obesity Is a Priority: The Preliminary Results of the “EpPOI: Education to Prevent Childhood Obesity” Project

 ,
,  ,
,  , ,
, ,  and
and 
Abstract

1. Introduction
2. Materials and Methods
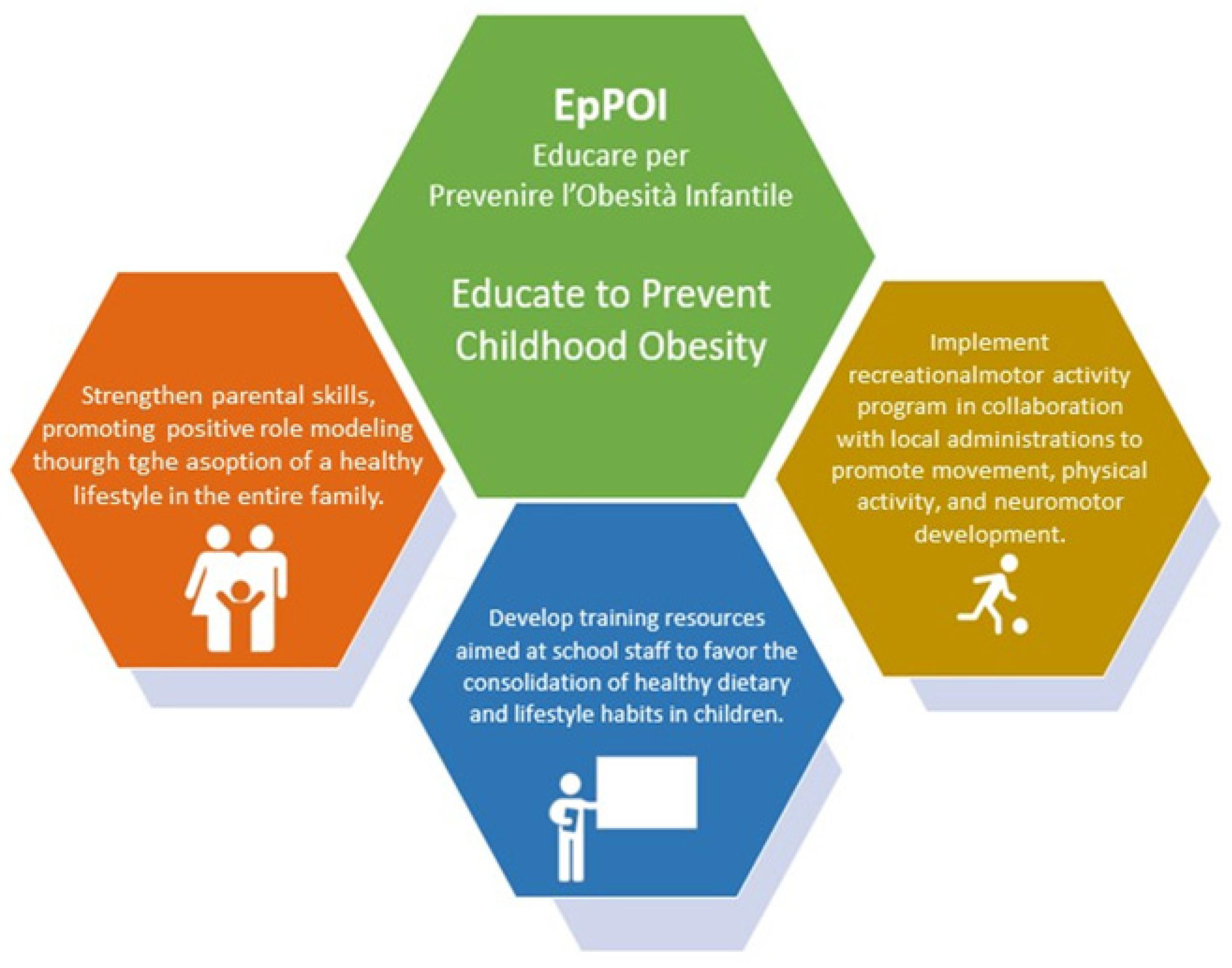
2.1. Objectives
- -
- Insufficient parental perception of body weight and habits of the child;
- -
- An excess of sedentary lifestyle during childhood;
- -
- Unhealthy eating habits during childhood;
- -
- Structural aspects and the promotion of correct lifestyles at school;
- -
- Scarce usability and traceability of information, the failure to involve all of the figures present in the life of children, and the sectorality and fragmentation of the interventions aimed at CO prevention.
2.2. Selection Criteria
2.3. Setting and Intervention
2.4. Outcome Measures
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, G.A.; Kim, K.K.; Wilding, J.P.H.; World Obesity Federation. Obesity: A chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes. Rev. 2017, 18, 715–723. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [PubMed]
- Lange, S.J.; Kompaniyets, L.; Freedman, D.S.; Kraus, E.M.; Porter, R.; Goodman, A.B. Longitudinal Trends in Body Mass Index Before and During the COVID-19 Pandemic Among Persons Aged 2-19 Years-United States, 2018–2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1278–1283. [Google Scholar] [CrossRef] [PubMed]
- United Nations Children’s Fund [UNICEF]; World Health Organization [WHO]; the International Bank for Reconstruction and Development/The World Bank. Levels and Trends in Child Malnutrition: UNICEF/WHO/the World Bank Group Joint Child Malnutrition Estimates: Key Findings of the 2021 Edition; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Johnson, L.G.; Cho, H.; Lawrence, S.M.; Keenan, G.M. Early childhood (1–5 years) obesity prevention: A systematic review of family-based multicomponent behavioral interventions. Prev. Med. 2024, 181, 107918. [Google Scholar] [CrossRef] [PubMed]
- Garrido-Miguel, M.; Cavero-Redondo, I.; Álvarez-Bueno, C.; Rodríguez-Artalejo, F.; Moreno, L.A.; Ruiz, J.R.; Ahrens, W.; Martínez-Vizcaíno, V. Prevalence and trends of overweight and obesity in European children from 1999 to 2016: A systematic review and Meta-analysis. JAMA Pediatr. 2019, 173, e192430. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Spotlight on Adolescent Health and Well-Being. Findings from the 2017/2018 Health Behaviour in School-Aged Children (HBSC) Survey in Europe and Canada. International Report. Volume 1. Key Findings. Available online: https://research-portal.st-andrews.ac.uk/en/publications/spotlight-on-adolescent-health-and-wellbeing-findings-from-the-20 (accessed on 28 February 2022).
- Gallus, S.; Odone, A.; Lugo, A.; Bosetti, C.; Colombo, P.; Zuccaro, P.; La Vecchia, C. Overweight and obesity prevalence and determinants in Italy: An update to 2010. Eur. J. Nutr. 2013, 52, 677–685. [Google Scholar] [CrossRef] [PubMed]
- Hu, P.; Samuels, S.; Maciejewski, K.R.; Li, F.; Aloe, C.; Van Name, M.; Savoye, M.; Sharifi, M. Changes in Weight-Related Health Behaviors and Social Determinants of Health among Youth with Overweight/Obesity during the COVID-19 Pandemic. Child. Obes. 2022, 18, 369–382. [Google Scholar] [CrossRef] [PubMed]
- Stival, C.; Lugo, A.; Barone, L.; Fattore, G.; Odone, A.; Salvatore, S.; Santoro, E.; Scaglioni, S.; van den Brandt, P.A.; Gallus, S.; et al. OKKio Alla Salute Lombardy Committee. Prevalence and Correlates of Overweight, Obesity and Physical Activity in Italian Children and Adolescents from Lombardy, Italy. Nutrients 2022, 14, 2258. [Google Scholar] [CrossRef] [PubMed]
- Wasniewska, M.; Pepe, G.; Aversa, T.; Bellone, S.; de Sanctis, L.; Di Bonito, P.; Faienza, M.F.; Improda, N.; Licenziati, M.R.; Maffeis, C.; et al. Skeptical Look at the Clinical Implication of Metabolic Syndrome in Childhood Obesity. Children 2023, 10, 735. [Google Scholar] [CrossRef]
- Marcus, C.; Danielsson, P.; Hagman, E. Pediatric obesity-Long-term consequences and effect of weight loss. J. Intern. Med. 2022, 292, 870–891. [Google Scholar] [CrossRef]
- Baker, J.L.; Olsen, L.W.; Sørensen, T.I. Childhood body-mass index and the risk of coronary heart disease in adulthood. N. Engl. J. Med. 2007, 357, 2329–2337. [Google Scholar] [CrossRef] [PubMed]
- Corica, D.; Oreto, L.; Pepe, G.; Calabrò, M.P.; Longobardo, L.; Morabito, L.; Pajno, G.B.; Alibrandi, A.; Aversa, T.; Wasniewska, M. Precocious Preclinical Cardiovascular Sonographic Markers in Metabolically Healthy and Unhealthy Childhood Obesity. Front. Endocrinol. 2020, 11, 56. [Google Scholar] [CrossRef] [PubMed]
- Simmonds, M.; Llewellyn, A.; Owen, C.G.; Woolacott, N. Predicting adult obesity from childhood obesity: A systematic review and meta-analysis. Obes. Rev. 2016, 17, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Twig, G.; Yaniv, G.; Levine, H.; Leiba, A.; Goldberger, N.; Derazne, E.; Shor, D.B.-A.; Tzur, D.; Afek, A.; Shamiss, A.; et al. Body- mass index in 2.3 million adolescents and cardiovascular death in adulthood. N. Engl. J. Med. 2016, 374, 2430–2440. [Google Scholar] [CrossRef] [PubMed]
- Luppino, G.; Wasniewska, M.; Casto, C.; Ferraloro, C.; Li Pomi, A.; Pepe, G.; Morabito, L.A.; Alibrandi, A.; Corica, D.; Aversa, T. Treating Children and Adolescents with Obesity: Predictors of Early Dropout in Pediatric Weight-Management Programs. Children 2024, 11, 205. [Google Scholar] [CrossRef] [PubMed]
- Ho, M.; Garnett, S.P.; Baur, L.; Burrows, T.; Stewart, L.; Neve, M.; Collins, C. Effectiveness of lifestyle interventions in child obesity: Systematic review with meta-analysis. Pediatrics 2012, 130, e1647-71. [Google Scholar] [CrossRef] [PubMed]
- Bleich, S.N.; Vercammen, K.A.; Zatz, L.Y.; Frelier, J.M.; Ebbeling, C.B.; Peeters, A. Interventions to prevent global childhood overweight and obesity: A systematic review. Lancet Diabetes Endocrinol. 2018, 6, 332–346. [Google Scholar] [CrossRef] [PubMed]
- Zeljkovic, A.; Vekic, J.; Stefanovic, A. Obesity and dyslipidemia in early life: Impact on cardiometabolic risk. Metab. Clin. Exp. 2024, 156, 155919. [Google Scholar] [CrossRef] [PubMed]
- Wimmelmann, C.L.; Sejling, C.; Clarke, R.B.; Elsenburg, L.K.; Sørensen, T.I.; Rod, N.H. Childhood adversity trajectories and weight status in young adult men: A register-based study including 359,783 Danish men. Int. J. Obes. 2024, 48, 1157–1163. [Google Scholar] [CrossRef]
- Bhutta, Z.A.; Norris, S.A.; Roberts, M.; Singhal, A. The global challenge of childhood obesity and its consequences: What can be done? Lancet Glob. Health 2023, 11, e1172–e1173. [Google Scholar] [CrossRef]
- Skinner, A.C.; Perrin, E.M.; Moss, L.A.; Skelton, J.A. Cardiometabolic risks and severity of obesity in children and young adults. N. Engl. J. Med. 2015, 373, 1307–1317. [Google Scholar] [CrossRef] [PubMed]
- Gato-Moreno, M.; Martos-Lirio, M.F.; Leiva-Gea, I.; Bernal-López, M.R.; Vegas-Toro, F.; Fernández-Tenreiro, M.C.; López-Siguero, J.P. Early Nutritional Education in the Prevention of Childhood Obesity. Int. J. Environ. Res. Public Health 2021, 18, 6569. [Google Scholar] [CrossRef] [PubMed]
- Apperley, L.J.; Blackburn, J.; Erlandson-Parry, K.; Gait, L.; Laing, P.; Senniappan, S. Childhood obesity: A review of current and future management options. Clin. Endocrinol. 2022, 96, 288–301. [Google Scholar] [CrossRef] [PubMed]
- Yuksel, H.S.; Şahin, F.N.; Maksimovic, N.; Drid, P.; Bianco, A. School-Based Intervention Programs for Preventing Obesity and Promoting Physical Activity and Fitness: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 347. [Google Scholar] [CrossRef]
- Gregori, D.; Hochdorn, A.; Azzolina, D.; Berchialla, P.; Lorenzoni, G.; OBEY-AD Study Consortium. Does Love Really Make Mothers Blind? A Large Transcontinental Study on Mothers’ Awareness About Their Children’s Weight. Obesity 2018, 26, 1211–1224. [Google Scholar] [CrossRef] [PubMed]
- McDonald, S.W.; Ginez, H.K.; Vinturache, A.E.; Tough, S.C. Maternal perceptions of underweight and overweight for 6–8 years olds from a Canadian cohort: Reporting weights, concerns and conversations with healthcare providers. BMJ Open 2016, 6, e012094. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, J.; Hulman, A.; Narayan, K.M.V.; Cunningham, S.A. Body Mass Index Trajectories From Childhood to Adulthood and Age at Onset of Overweight and Obesity: The Influence of Parents’ Weight Status. Am. J. Epidemiol. 2022, 191, 1877–1885. [Google Scholar] [CrossRef]
- Williams, A.S.; Ge, B.; Petroski, G.; Kruse, R.L.; McElroy, J.A.; Koopman, R.J. Socioeconomic Status and Other Factors Associated with Childhood Obesity. J. Am. Board Fam. Med. 2018, 31, 514–521. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Question | Answer |
|---|---|
| 1. Age group | >20 |
| 20–25 | |
| 25–30 | |
| 30–35 | |
| 35–40 | |
| >40 | |
| 2. Education level | primary school diploma |
| middle school diploma | |
| diploma | |
| degree | |
| 3. Where do you get information about nutrition and physical activity? | pediatricians |
| internet | |
| family or friends | |
| specialists | |
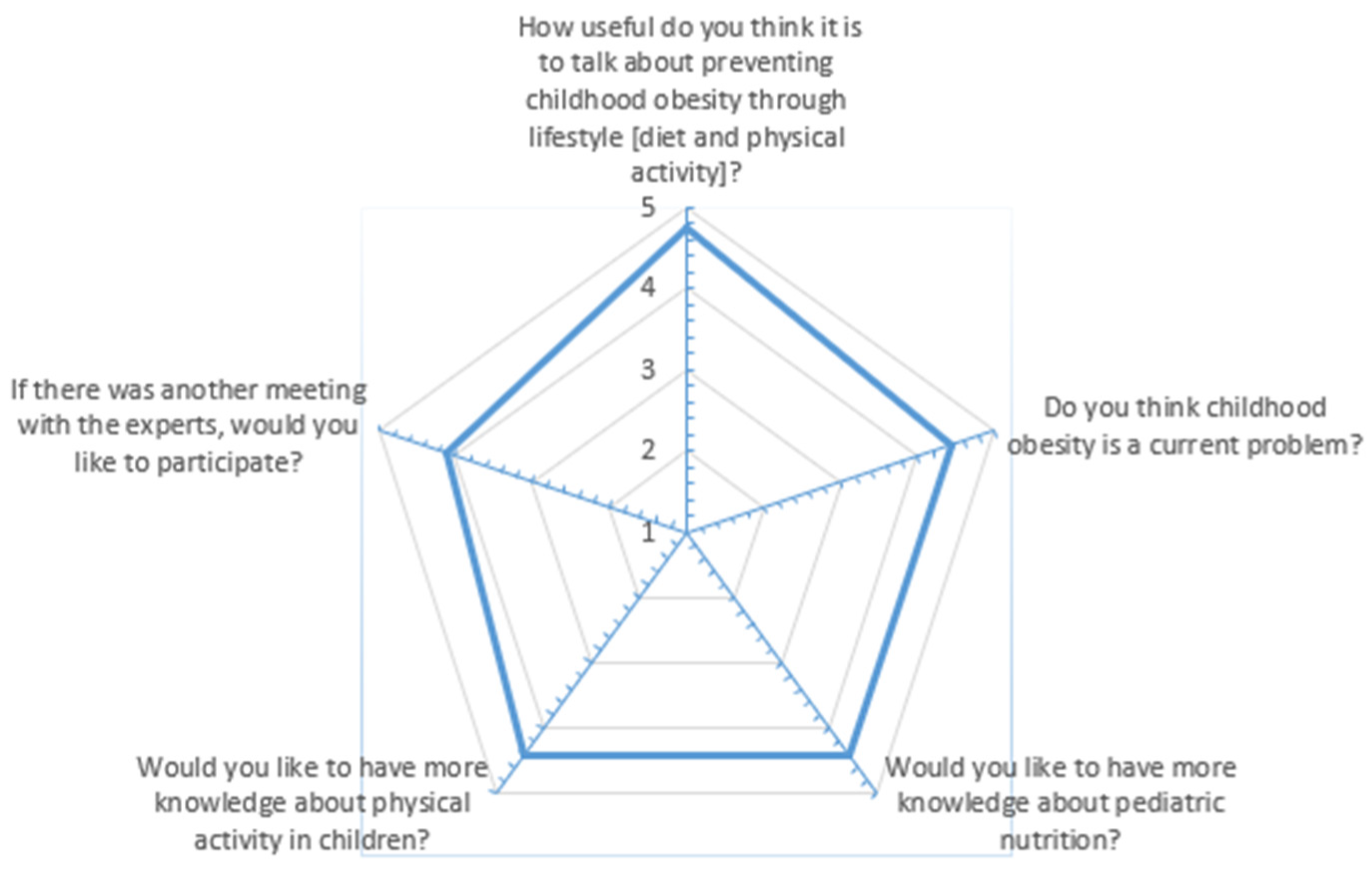
| 4. How useful do you think it is to talk about preventing childhood obesity through lifestyle [diet and physical activity]? | from 1 [a little] to 5 [a lot] |
| 5. Do you think childhood obesity is a current problem? | from 1 [a little] to 5 [a lot] |
| 6. If there was another meeting with the experts, would you like to participate? | from 1 [a little] to 5 [a lot] |
| 7. Would you like to have more knowledge about pediatric nutrition? | from 1 [a little] to 5 [a lot] |
| 8. Would you like to have more knowledge about physical activity in children? | from 1 [a little] to 5 [a lot] |
| 9. Have you made any changes in your teaching activity after the meeting with the specialists? [only for school staff] | from 1 [a little] to 5 [a lot] |
| 9. Have you made any changes to your family lifestyle after meeting with the specialists? [only for parents] | from 1 [a little] to 5 [a lot] |
| 10. What changes did you make? |
| Likert Scale [n] | Frequency [n] | Percentage [%] |
|---|---|---|
| 4. How useful do you think it is to talk about preventing childhood obesity through lifestyle [diet and physical activity]? | ||
| 1 | 0 | 0 |
| 2 | 0 | 0 |
| 3 | 6 | 6.3% |
| 4 | 14 | 76% |
| 5 | 76 | 79.2% |
| 5. Do you think childhood obesity is a current problem? | ||
| 1 | 1 | 1% |
| 2 | 0 | 0 |
| 3 | 16 | 16.7% |
| 4 | 18 | 18.8% |
| 5 | 61 | 63.5% |
| 6. If there was another meeting with the experts, would you like to participate? | ||
| 1 | 7 | 7.3% |
| 2 | 4 | 4.2% |
| 3 | 13 | 13.5% |
| 4 | 19 | 19.8% |
| 5 | 53 | 55.2% |
| 7. Would you like to have more knowledge about pediatric nutrition? | ||
| 1 | 1 | 1% |
| 2 | 4 | 4.2% |
| 3 | 12 | 12.5% |
| 4 | 15 | 15.6% |
| 5 | 64 | 66.7% |
| 8. Would you like to have more knowledge about physical activity in children? | ||
| 2 | 4 | 4.2% |
| 3 | 14 | 14.6% |
| 4 | 18 | 18.8% |
| 5 | 60 | 62.5% |
| 4. How useful do you think it is to talk about preventing childhood obesity through lifestyle [diet and physical activity]? | 5. Do you think childhood obesity is a current problem? | 6. If there was another meeting with the experts, would you like to participate? | 7. Would you like to have more knowledge about pediatric nutrition? | 8. Would you like to have more knowledge about physical activity in children? | ||
| 4. How useful do you think it is to talk about preventing childhood obesity through lifestyle [diet and physical activity]? | Correlation coefficient | 1.000 | 0.310 ** | 0.532 ** | 0.533 ** | 0.349 ** |
| p-value | 0.002 * | 0.000 * | 0.00 * | 0.00 * | ||
| 5. Do you think childhood obesity is a current problem? | Correlation coefficient | 0.310 ** | 1.000 | 0.430 ** | 0.348 | 0.329 |
| p-value | 0.002 * | 0.000 * | 0.001 * | 0.001 * | ||
| 6. If there was another meeting with the experts, would you like to participate? | Correlation coefficient | 0.532 ** | 0.430 ** | 1.000 | 0.770 ** | 0.531 ** |
| p-value | 0.000 * | 0.000 * | 0.000 * | 0.000 * | ||
| 7. Would you like to have more knowledge about pediatric nutrition? | Correlation coefficient | 0.553 ** | 0.348 ** | 0.770 ** | 1.000 | 0.571 ** |
| p-value | 0.000 * | 0.001 * | 0.000 * | 0.000 * | ||
| 8. Would you like to have more knowledge about physical activity in children? | Correlation coefficient | 0.349 ** | 0.329 ** | 0.531 ** | 0.571 ** | 1.000 |
| p-value | 0.000 * | 0.001 * | 0.000 * | 0.000 * | ||
| Education Level | ||
| Education level | Correlation coefficient | 1.000 |
| p-value | ||
| 4. How useful do you think it is to talk about preventing childhood obesity through lifestyle [diet and physical activity]? | Correlation coefficient | 0.13 |
| p-value | 0.902 | |
| 5. Do you think childhood obesity is a current problem? | Correlation coefficient | 0.127 |
| p-value | 0.218 | |
| 6. If there was another meeting with the experts, would you like to participate? | Correlation coefficient | −0.051 |
| p-value | 0.624 | |
| 7. Would you like to have more knowledge about pediatric nutrition? | Correlation coefficient | 0.089 |
| p-value | 0.387 | |
| 8. Would you like to have more knowledge about physical activity in children? | Correlation coefficient | 0.96 |
| p-value | 0.352 | |
| Age | ||
| Age | Correlation coefficient | 1.000 |
| p-value | ||
| 4. How useful do you think it is to talk about preventing childhood obesity through lifestyle (diet and physical activity)? | Correlation coefficient | 0.038 |
| p-value | 0.712 | |
| 5. Do you think childhood obesity is a current problem? | Correlation coefficient | 0.263 ** |
| p-value | 0.010 ** | |
| 6. If there was another meeting with the experts, would you like to participate? | Correlation coefficient | 0.131 |
| p-value | 0.204 | |
| 7. Would you like to have more knowledge about pediatric nutrition? | Correlation coefficient | 0.212 * |
| p-value | 0.038 * | |
| 8. Would you like to have more knowledge about physical activity in children? | Correlation coefficient | 1.66 |
| p-value | 0.106 | |
| Variables | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| Age | 1.68 | 1.078–2.643 | 0.022 * | 1.520 | 0.943–2.451 | 0.086 |
| Education level | 1.499 | 0.705–3.188 | 0.293 | 1.264 | 0.531–3.006 | 0.596 |
| 4. How useful do you think it is to talk about preventing childhood obesity through lifestyle [diet and physical activity]? | 1.584 | 0.702–3.573 | 0.267 | 0.916 | 0.350–2.396 | 0.857 |
| 6. If there was another meeting with the experts, would you like to participate? | 1.568 | 1.066–2.307 | 0.022 * | 1.170 | 0.709–1.929 | 0.539 |
| 7. Would you like to have more knowledge about pediatric nutrition? | 2.315 | 1.373–3.903 | 0.002 * | 2.093 | 1.222–3.584 | 0.007 * |
| 8. Would you like to have more knowledge about physical activity in children? | 2.001 | 1.162–3.445 | 0.012 * | 2.001 | 1.162–3.445 | 0.012 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Porri, D.; Luppino, G.; Morabito, L.A.; La Rosa, E.; Pepe, G.; Corica, D.; Valenzise, M.; Messina, M.F.; Zirilli, G.; Li Pomi, A.; et al. The Prevention of Childhood Obesity Is a Priority: The Preliminary Results of the “EpPOI: Education to Prevent Childhood Obesity” Project. Nutrients 2024, 16, 2538. https://doi.org/10.3390/nu16152538
Porri D, Luppino G, Morabito LA, La Rosa E, Pepe G, Corica D, Valenzise M, Messina MF, Zirilli G, Li Pomi A, et al. The Prevention of Childhood Obesity Is a Priority: The Preliminary Results of the “EpPOI: Education to Prevent Childhood Obesity” Project. Nutrients. 2024; 16(15):2538. https://doi.org/10.3390/nu16152538
Chicago/Turabian StylePorri, Debora, Giovanni Luppino, Letteria Anna Morabito, Elisa La Rosa, Giorgia Pepe, Domenico Corica, Mariella Valenzise, Maria Francesca Messina, Giuseppina Zirilli, Alessandra Li Pomi, and et al. 2024. "The Prevention of Childhood Obesity Is a Priority: The Preliminary Results of the “EpPOI: Education to Prevent Childhood Obesity” Project" Nutrients 16, no. 15: 2538. https://doi.org/10.3390/nu16152538
APA StylePorri, D., Luppino, G., Morabito, L. A., La Rosa, E., Pepe, G., Corica, D., Valenzise, M., Messina, M. F., Zirilli, G., Li Pomi, A., Alibrandi, A., Di Mauro, D., Aversa, T., & Wasniewska, M. G. (2024). The Prevention of Childhood Obesity Is a Priority: The Preliminary Results of the “EpPOI: Education to Prevent Childhood Obesity” Project. Nutrients, 16(15), 2538. https://doi.org/10.3390/nu16152538