
Predicting Recurrent Deficiency and Suboptimal Monitoring of Thiamin Deficiency in Patients with Metabolic and Bariatric Surgery

 , ,
, , Highlights
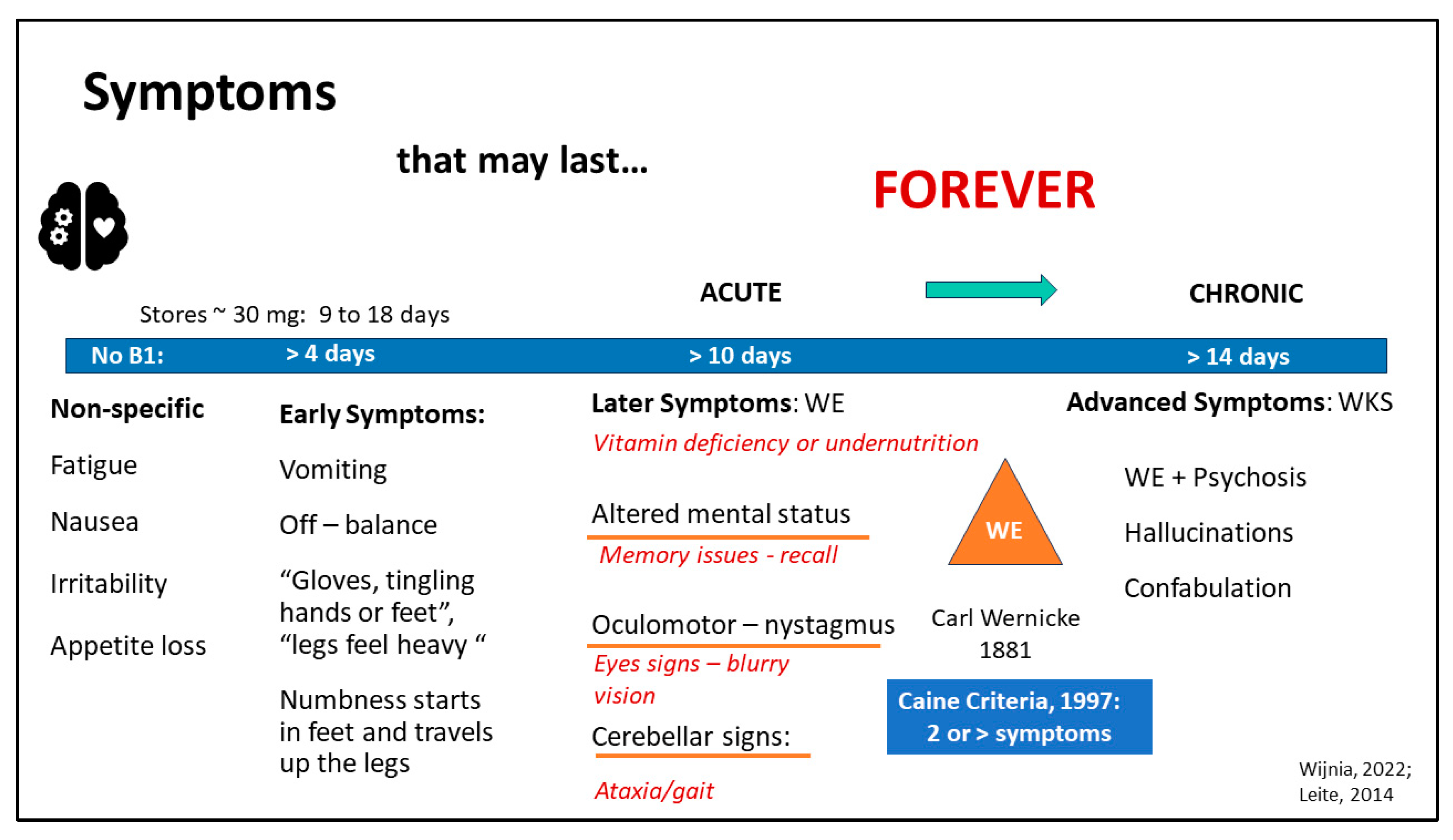
- B1 (thiamine) deficiency appears recurrent, which can become chronic based on lab results and demographics, requiring careful monitoring in patients with symptoms or lab indicators.
- Several commonly ordered labs can act as red flags for recurrent or chronic vitamin B1 deficiency, including a Comprehensive Metabolic Panel (CMP) with electrolytes, liver and kidney function enzymes, Complete Blood Count with differential, and Iron Panel (ferritin and transferrin saturation (TSAT)).
- Abnormal nutrient-related labs such as B vitamins (B6, B9 (folate), B12), vitamin D, and vitamin C can also signal a potential vitamin B1 deficiency.
- Certain demographics in the United States, such as African Americans and patients without private insurance, are at a higher risk for vitamin B1 deficiency. Vitamin B1 deficiency is not limited to specific types of surgeries; thus, it is important to screen for it in all surgeries, not just hypo/malabsorptive ones.
Abstract
1. Introduction
2. Methodology
2.1. Sample
2.2. Measures
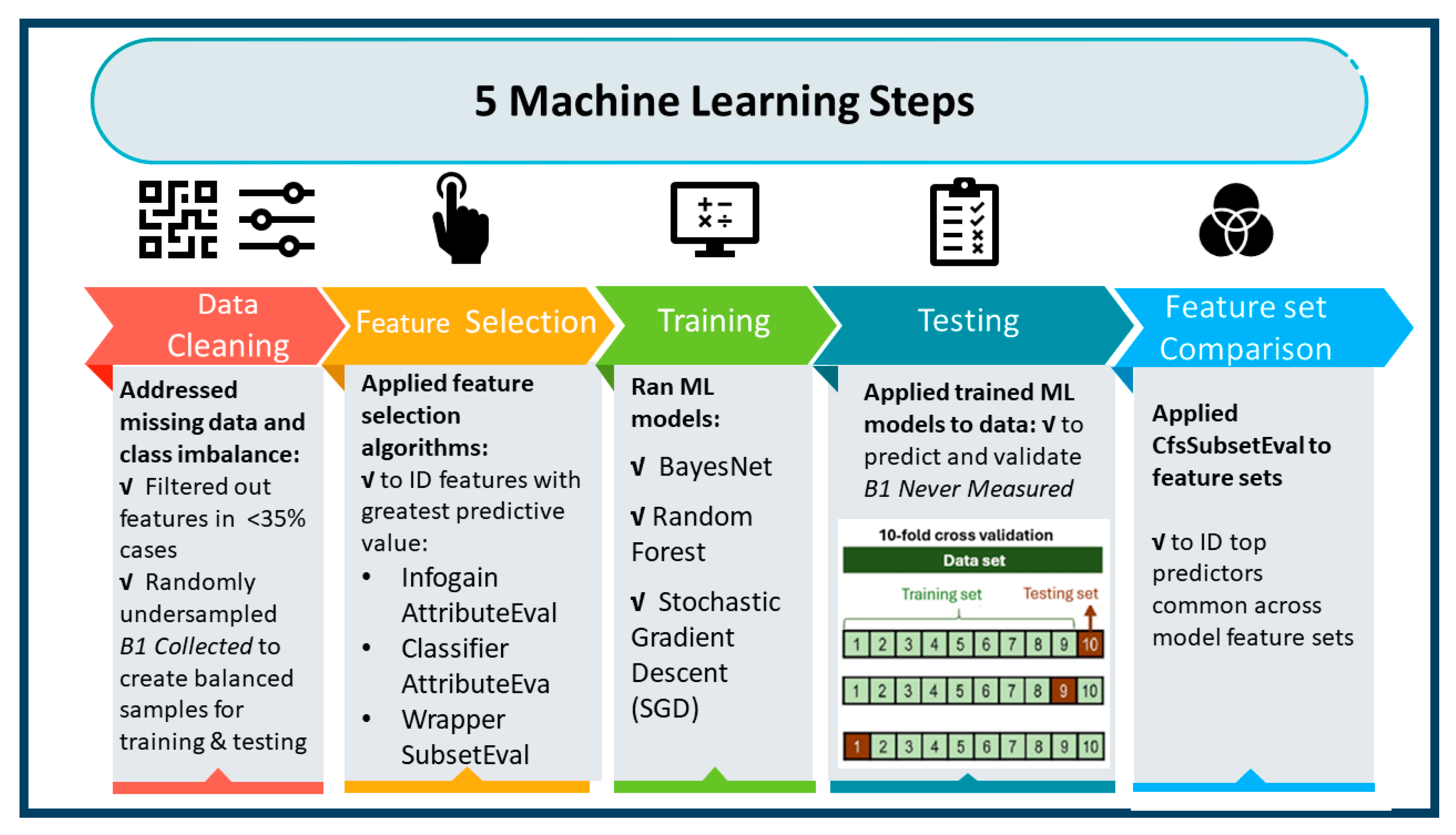
2.3. Data Preparation
2.4. Statistical Analyses
3. Results
3.1. Predictors of Recurrent Thiamin Deficiency
3.2. Failure to Collect Vitamin B1 Labs
4. Discussion
4.1. “Red Flag” Features
- Neurotropic vitamins: Vitamin B1, vitamin B6, and folate act synergistically to maintain a healthy nervous system [35], meaning a deficiency in one may signal a deficiency in the others.
- Fluctuating electrolytes: Electrolytes (calcium, sodium, potassium) vary based on the level of dehydration and repletion, as seen in the present study, which had a high IRR of 1.91–2.87. Thus, patients with fluctuating electrolyte levels, in combination with other micronutrient abnormalities, may be at a greater risk of TD.
- Malnutrition indices: a combination of labs from CMP can indicate malnutrition (creatinine, AST/ALT, Total Protein High and Low, Albumin Low, and Glucose Low) and subsequent TD.
- Racial disparities: Including race as a variable in research is critical to further explore why there is a disproportionate number of African Americans with TD and other micronutrient deficiencies. Only two out of ten research studies were included in the systematic review by Jawar et. al., 2024 that explored race as a predictor of TD, specifically African Americans as an independent risk factor for TD as reported in sleeve gastrectomy (OR = 3.9, 95% CI 1.25–12.21, p = 0.019) [36] and gastric bypass (OR = 6.1, 95% CI 3.0–12.4, P < 0.0001) with race as the only predictor of TD (OR 13.4, 95% CI 5.2–34.5) [37].
4.2. Criteria for Diagnosis
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morton, J.M.; Khoury, H.; Brethauer, S.A.; Baker, J.W.; Sweet, W.A.; Mattar, S.; Ponce, J.; Nguyen, N.T.; Rosenthal, R.J.; DeMaria, E.J. First report from the American Society of Metabolic and Bariatric Surgery closed-claims registry: Prevalence, causes, and lessons learned from bariatric surgery medical malpractice claims. Surg. Obes. Relat. Dis. 2022, 18, 943–947. [Google Scholar] [CrossRef] [PubMed]
- Arnold Mackles, M. Gastric Bypass Malpractice Yields $14.1 Million Verdict. HealthCare Risk Mangement. 2022. Available online: https://www.reliasmedia.com/articles/gastric-bypass-malpractice-yields-14-1-million-verdict (accessed on 10 May 2024).
- DeMaria, E.; Trigilio-Black, C. Alarming Increase in Malpractice Claims Related to Wernicke’s Encephalopathy Post Bariatric Surgery: An Alert to Monitor for Thiamine Deficiency. Bariatr. Times 2018, 15, 8–9. [Google Scholar]
- Tzoumas, L.; Samara, E.; Tzoumas, K.; Tzimas, P.; Vlachos, K.; Papadopoulos, G. Medico-Legal Analysis of General Surgery Cases in Greece: A 48 Year Study. Cureus 2021, 13, e16205. [Google Scholar] [CrossRef] [PubMed]
- Timsit, G.; Johanet, H. Medico-legal claims in bariatric surgery in France between 2010 and 2015. J. Visc. Surg. 2019, 156 (Suppl. 1), S51–S55. [Google Scholar] [CrossRef] [PubMed]
- Ratnasingham, K.; Knight, J.; Liu, M.; Karatsai, E.; Humadi, S.; Irukulla, S. NHS litigation in bariatric surgery over a ten year period. Int. J. Surg. 2017, 40, 14–16. [Google Scholar] [CrossRef]
- Donnino, M.W.; Vega, J.; Miller, J.; Walsh, M. Myths and misconceptions of Wernicke’s encephalopathy: What every emergency physician should know. Ann. Emerg. Med. 2007, 50, 715–721. [Google Scholar] [CrossRef] [PubMed]
- Frank, L.L. Thiamin in Clinical Practice. JPEN J. Parenter. Enter. Nutr. 2015, 39, 503–520. [Google Scholar] [CrossRef] [PubMed]
- Oudman, E.; Wijnia, J.W.; van Dam, M.; Biter, L.U.; Postma, A. Preventing Wernicke Encephalopathy After Bariatric Surgery. Obes. Surg. 2018, 28, 2060–2068. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.J.; Johnson, C.R.; Koshy, R.; Hess, S.Y.; Qureshi, U.A.; Mynak, M.L.; Fischer, P.R. Thiamine deficiency disorders: A clinical perspective. Ann. N. Y. Acad. Sci. 2021, 1498, 9–28. [Google Scholar] [CrossRef]
- Leite, H.P.; de Lima, L.F.P. Thiamine (Vitamin B1) Deficiency in Intensive Care: Physiology, Risk Factors, Diagnosis, and Treatment. In Diet and Nutrition in Critical Care; Springer: Berlin/Heidelberg, Germany, 2014; pp. 1–16. [Google Scholar]
- Wijnia, J.W. A Clinician’s View of Wernicke-Korsakoff Syndrome. J. Clin. Med. 2022, 11, 6755. [Google Scholar] [CrossRef]
- Sechi, G.; Serra, A. Wernicke’s encephalopathy: New clinical settings and recent advances in diagnosis and management. Lancet Neurol. 2007, 6, 442–455. [Google Scholar] [CrossRef] [PubMed]
- Parrott, J.; Frank, L.; Rabena, R.; Craggs-Dino, L.; Isom, K.A.; Greiman, L. American Society for Metabolic and Bariatric Surgery Integrated Health Nutritional Guidelines for the Surgical Weight Loss Patient 2016 Update: Micronutrients. Surg. Obes. Relat. Dis. 2017, 13, 727–741. [Google Scholar] [CrossRef] [PubMed]
- Mechanick, J.I.; Apovian, C.; Brethauer, S.; Timothy Garvey, W.; Joffe, A.M.; Kim, J.; Kushner, R.F.; Lindquist, R.; Pessah-Pollack, R.; Seger, J.; et al. Clinical Practice Guidelines for the Perioperative Nutrition, Metabolic, and Nonsurgical Support of Patients Undergoing Bariatric Procedures—2019 Update: Cosponsored by American Association of Clinical Endocrinologists/American College of Endocrinology, The Obesity Society, American Society for Metabolic and Bariatric Surgery, Obesity Medicine Association, and American Society of Anesthesiologists. Obesity 2020, 28, O1–O58. [Google Scholar] [PubMed]
- Jawara, D.; Ufearo, D.M.; Murtha, J.A.; Fayanju, O.M.; Gannon, B.M.; Ravelli, M.N.; Funk, L.M. Racial disparities in selected micronutrient deficiencies after bariatric surgery: A systematic review. Surg. Obes. Relat. Dis. 2024, 20, 283–290. [Google Scholar] [CrossRef] [PubMed]
- Parrott, J.M.; Parrott, A.J.; Rouhi, A.D.; Parrott, J.S.; Dumon, K.R. What We Are Missing: Using Machine Learning Models to Predict Vitamin C Deficiency in Patients with Metabolic and Bariatric Surgery. Obes. Surg. 2023, 33, 1710–1719. [Google Scholar] [CrossRef] [PubMed]
- Camaschella, C.; Girelli, D. The changing landscape of iron deficiency. Mol. Asp. Med. 2020, 75, 100861. [Google Scholar] [CrossRef]
- Cappellini, M.D.; Comin-Colet, J.; de Francisco, A.; Dignass, A.; Doehner, W.; Lam, C.S.; Macdougall, I.C.; Rogler, G.; Camaschella, C.; Kadir, R. Iron deficiency across chronic inflammatory conditions: International expert opinion on definition, diagnosis, and management. Am. J. Hematol. 2017, 92, 1068–1078. [Google Scholar] [CrossRef] [PubMed]
- Cappellini, M.D.; Musallam, K.M.; Taher, A.T. Iron deficiency anaemia revisited. J. Intern. Med. 2020, 287, 153–170. [Google Scholar] [CrossRef] [PubMed]
- Benotti, P.N.; Wood, G.C.; Dove, J.T.; Kaberi-Otarod, J.; Still, C.D.; Gerhard, G.S.; Bistrian, B.R. Iron deficiency is highly prevalent among candidates for metabolic surgery and may affect perioperative outcomes. Surg. Obes. Relat. Dis. 2021, 17, 1692–1699. [Google Scholar] [CrossRef]
- Green, G.H.; Diggle, P.J. On the operational characteristics of the Benjamini and Hochberg False Discovery Rate procedure. Stat. Appl. Genet. Mol. Biol. 2007, 6, 27. [Google Scholar] [CrossRef]
- Galar, M.; Fernandez, A.; Barrenechea, E.; Bustince, H.; Herrera, F. A review on ensembles for the class imbalance problem: Bagging-, boosting-, and hybrid-based approaches. IEEE Trans. Syst. Man Cybern. Part C (Appl. Rev.) 2011, 42, 463–484. [Google Scholar] [CrossRef]
- Cooper, G.F.; Herskovits, E. A Bayesian method for the induction of probabilistic networks from data. Mach. Learn. 1992, 9, 309–347. [Google Scholar] [CrossRef]
- Breiman, L. Random forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef]
- Rodriguez, J.D.; Perez, A.; Lozano, J.A. Sensitivity analysis of k-fold cross validation in prediction error estimation. IEEE Trans. Pattern Anal. Mach. Intell. 2009, 32, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Witten, I.H.; Frank, E. Data mining: Practical machine learning tools and techniques with Java implementations. ACM Sigmod Rec. 2002, 31, 76–77. [Google Scholar] [CrossRef]
- Caine, D.; Halliday, G.; Kril, J.; Harper, C. Operational criteria for the classification of chronic alcoholics: Identification of Wernicke’s encephalopathy. J. Neurol. Neurosurg. Psychiatry 1997, 62, 51–60. [Google Scholar] [CrossRef]
- Hosmer, D.W., Jr.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression; Wiley Series in Probability and Statistics; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2013. [Google Scholar]
- Taylor, R.A.; Gilson, A.; Chi, L.; Haimovich, A.D.; Crawford, A.; Brandt, C.; Magidson, P.; Lai, J.M.; Levin, S.; Mecca, A.P.; et al. Dementia risk analysis using temporal event modeling on a large real-world dataset. Sci. Rep. 2023, 13, 22618. [Google Scholar] [CrossRef]
- Johnson, L.P.; Asigbee, F.M.; Crowell, R.; Negrini, A. Pre-surgical, surgical and post-surgical experiences of weight loss surgery patients: A closer look at social determinants of health. Clin. Obes. 2018, 8, 265–274. [Google Scholar] [CrossRef]
- Khalid, S.I.; Maasarani, S.; Shanker, R.M.; Becerra, A.Z.; Omotosho, P.; Torquati, A. Social determinants of health and their impact on rates of postoperative complications among patients undergoing vertical sleeve gastrectomy. Surgery 2022, 171, 447–452. [Google Scholar] [CrossRef]
- Schiavo, L.; Scalera, G.; Pilone, V.; De Sena, G.; Capuozzo, V.; Barbarisi, A. Micronutrient defi ciencies in patients candidate for bariatric surgery: A prospective, preoperative trial of screening, diagnosis, and treatment. Int. J. Vitam. Nutr. Res. 2015, 85, 340–347. [Google Scholar] [CrossRef]
- Berger, M.M.; Shenkin, A.; Schweinlin, A.; Amrein, K.; Augsburger, M.; Biesalski, H.K.; Bischoff, S.C.; Casaer, M.P.; Gundogan, K.; Lepp, H.L.; et al. ESPEN micronutrient guideline. Clin. Nutr. 2022, 41, 1357–1424. [Google Scholar] [CrossRef] [PubMed]
- Calderón-Ospina, C.A.; Nava-Mesa, M.O. B Vitamins in the nervous system: Current knowledge of the biochemical modes of action and synergies of thiamine, pyridoxine, and cobalamin. CNS Neurosci. Ther. 2020, 26, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Alsulaim, H.A.; Canner, J.K.; Prokopowicz, G.P.; Steele, K.E. Prevalence and predictors of postoperative thiamine deficiency after vertical sleeve gastrectomy. Surg. Obes. Relat. Dis. 2018, 14, 943–950. [Google Scholar] [CrossRef]
- Clements, R.H.; Katasani, V.G.; Palepu, R.; Leeth, R.R.; Leath, T.D.; Roy, B.P.; Vickers, S.M. Incidence of vitamin deficiency after laparoscopic Roux-en-Y gastric bypass in a university hospital setting. Am. Surg. 2006, 72, 1196–1202, discussion 1203–1194. [Google Scholar] [CrossRef] [PubMed]
- Bushyhead, D.; Quigley, E.M.M. Small Intestinal Bacterial Overgrowth-Pathophysiology and Its Implications for Definition and Management. Gastroenterology 2022, 163, 593–607. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| B1 Deficient (n = 108) | B1 Sufficient (n = 418) | B1 Never Measured (n = 352) | Total (n = 878) | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|
| n or Mean | % or (SD) | n or Mean | % or (SD) | n or Mean | % or (SD) | n or Mean | % or (SD) | ||
| Sex (n, %) | |||||||||
| Female | 102 | 94.4 | 336 | 80.4 | 266 | 75.6 | 704 | 80.18 | <0.001 |
| Male | 6 | 5.6 | 82 | 19.6 | 86 | 24.4 | 174 | 19.8 | |
| Age (mean, SD) | 44.8 | 11 | 48.5 | 12 | 47.3 | 13.6 | 878 | 12.6 | 0.021 |
| Ethnicity (n, %) | 0.019 | ||||||||
| Not Hispanic/Latino | 104 | 96.3 | 384 | 91.9 | 339 | 96.3 | 827 | 94.2 | |
| Hispanic/Latino | 4 | 3.7 | 34 | 8.1 | 13 | 3.7 | 51 | 5.8 | |
| Race (n, %) | <0.001 | ||||||||
| Black | 82 | 78.9 | 141 | 36.2 | 195 | 57.4 | 418 | 50.1 | |
| White or Other | 22 | 21.1 | 249 | 63.9 | 145 | 42.7 | 416 | 49.9 | |
| Domestic Partner (n, %) | 0.016 | ||||||||
| Lives with Partner | 31 | 32.6 | 182 | 48.3 | 112 | 42 | 325 | 44 | |
| Lives Alone | 64 | 67.4 | 195 | 51.7 | 155 | 58.1 | 414 | 56 | |
| Payor (n, %) | |||||||||
| Private Insurance or Self | 47 | 43.93 | 300 | 72.12 | 186 | 54.23 | 533 | 61.55 | |
| No Private Insurance | 60 | 56.07 | 116 | 27.88 | 157 | 45.77 | 333 | 38.45 | |
| BMI * (mean, SD) | 46.7 | 9.4 | 44.1 | 7.5 | 46.1 | 9.6 | 845 | 45.1 | 0.001 |
| Primary Procedure (n, %) | <0.001 | ||||||||
| LSG * | 88 | 82.24 | 341 | 81.97 | 251 | 71.31 | 680 | 77.71 | |
| RYGB * | 13 | 12.15 | 56 | 13.46 | 71 | 20.17 | 140 | 16 | |
| Revision | 5 | 4.67 | 12 | 2.88 | 5 | 1.42 | 22 | 2.51 | |
| Other | 1 | 0.93 | 7 | 1.68 | 25 | 7.1 | 33 | 3.77 | |
| Number of Surgeries (n, %) | 0.422 | ||||||||
| One | 105 | 97.22 | 400 | 95.69 | 345 | 98.01 | 850 | 96.81 | |
| Two | 2 | 1.85 | 15 | 3.59 | 6 | 1.7 | 23 | 2.62 | |
| Three or More | 1 | 0.93 | 3 | 0.72 | 1 | 0.28 | 5 | 0.57 | |
| IRR * | LCI * | UCI * | p-Value | |
|---|---|---|---|---|
| African American | 5.94 | 3.44 | 10.23 | <0.001 |
| No Domestic Partner | 2.03 | 1.26 | 3.27 | 0.004 |
| No Private Health Insurance | 2.91 | 1.91 | 4.45 | <0.001 |
| Unadjusted Models | Adjusted Models | |||||||
|---|---|---|---|---|---|---|---|---|
| IRR | LCI | UCI | p-Value | IRR | LCI | UCI | p-Value | |
| Vitamins and Minerals | ||||||||
| Folate Low | 4.62 | 2.22 | 9.60 | <0.001 | 3.95 | 1.70 | 9.19 | 0.001 |
| Vit B6 Low | 4.62 | 2.96 | 7.20 | <0.001 | 4.68 | 3.00 | 7.30 | <0.001 |
| Vit B12 High | 2.65 | 1.73 | 4.04 | <0.001 | 1.67 | 1.07 | 2.58 | 0.022 |
| Vit C Low | 2.65 | 1.49 | 4.70 | 0.001 | 2.50 | 1.36 | 4.59 | 0.003 |
| Vit D Low | 2.82 | 1.79 | 4.44 | <0.001 | 2.73 | 1.71 | 4.34 | <0.001 |
| Calcium Low | 2.87 | 1.89 | 4.35 | <0.001 | 3.08 | 1.99 | 4.76 | <0.001 |
| Calcium High | 2.24 | 1.04 | 4.82 | 0.040 | 1.80 | 0.89 | 3.66 | 0.103 |
| Sodium Low | 1.91 | 1.16 | 3.14 | 0.011 | 2.32 | 1.45 | 3.73 | <0.001 |
| Potassium Low | 2.33 | 1.47 | 3.70 | <0.001 | 2.07 | 1.30 | 3.29 | 0.002 |
| Potassium High | 2.63 | 1.37 | 5.04 | 0.004 | 2.58 | 1.40 | 4.77 | 0.002 |
| Blood Indices | ||||||||
| Ferritin High | 4.54 | 2.75 | 7.48 | <0.001 | 3.35 | 2.09 | 5.36 | <0.001 |
| Transferrin Low | 1.88 | 1.04 | 3.41 | 0.038 | 1.62 | 0.88 | 2.98 | 0.118 |
| TSAT Low | 2.31 | 1.18 | 4.53 | 0.015 | 2.55 | 1.31 | 4.96 | 0.006 |
| HCT Low | 4.59 | 2.92 | 7.19 | <0.001 | 5.58 | 3.41 | 9.11 | <0.001 |
| HGB Low | 4.12 | 2.59 | 6.56 | <0.001 | 4.65 | 2.79 | 7.75 | <0.001 |
| RBC Low | 2.17 | 1.40 | 3.38 | 0.001 | 2.12 | 1.36 | 3.31 | 0.001 |
| AID | 2.30 | 1.45 | 3.66 | <0.001 | 1.95 | 1.24 | 3.08 | 0.004 |
| FID30–100 | 3.09 | 1.58 | 6.02 | 0.001 | 2.97 | 1.44 | 6.13 | 0.003 |
| FID > 100 | 4.78 | 3.13 | 7.30 | <0.001 | 3.63 | 2.37 | 5.57 | <0.001 |
| CMP Labs | ||||||||
| Creatinine High | 1.99 | 1.17 | 3.38 | 0.011 | 2.34 | 1.31 | 4.17 | 0.004 |
| AST Low | 3.01 | 1.97 | 4.60 | <0.001 | 3.01 | 1.92 | 4.71 | <0.001 |
| ALT Low | 4.54 | 2.85 | 7.25 | <0.001 | 4.49 | 2.70 | 7.46 | <0.001 |
| Total Protein High | 3.00 | 1.79 | 5.03 | <0.001 | 3.10 | 1.85 | 5.19 | <0.001 |
| Total Protein Low | 1.59 | 1.01 | 2.52 | 0.046 | 1.79 | 1.11 | 2.87 | 0.017 |
| Albumin Low | 2.89 | 1.89 | 4.41 | <0.001 | 2.83 | 1.81 | 4.42 | <0.001 |
| Glucose Low | 2.27 | 1.42 | 3.64 | <0.001 | 2.27 | 1.40 | 3.68 | 0.001 |
| Algorithm | Number of Features | Accuracy a | AUC b | TD True Positives c | TD False Positives d | TD True Negatives | TD False Negatives |
|---|---|---|---|---|---|---|---|
| BayesNet | 85 | 75.12% | 0.82 | 0.67 | 0.17 | 0.83 | 0.33 |
| Random Forest | 54 | 80.90% | 0.86 | 0.75 | 0.13 | 0.87 | 025 |
| SGD Hinge Loss | 95 | 75.75% | 0.76 | 0.73 | 0.22 | 0.79 | 0.27 |
| BayesNet | N Folds | RandomForest | N Folds | SGD Hinge Loss | N Folds |
|---|---|---|---|---|---|
| Folate Ever High * | 10 | Folate Ever High * | 10 | Folate Times High + | 10 |
| Vit B6 Ever High * | 10 | Vit D Times Low + | 10 | Vit B6 Times Low ** | 10 |
| Vit B6 Times Low ** | 10 | HGB Ever Low ** | 10 | Vit C Ever Low * | 10 |
| Vit C Ever Low * | 10 | AST Times High | 10 | MCV Ever High * | 8 |
| Surgery Type ** | 10 | Patient Age | 10 | Surgery Type ** | 7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parrott, J.M.; Parrott, A.J.; Parrott, J.S.; Williams, N.N.; Dumon, K.R. Predicting Recurrent Deficiency and Suboptimal Monitoring of Thiamin Deficiency in Patients with Metabolic and Bariatric Surgery. Nutrients 2024, 16, 2226. https://doi.org/10.3390/nu16142226
Parrott JM, Parrott AJ, Parrott JS, Williams NN, Dumon KR. Predicting Recurrent Deficiency and Suboptimal Monitoring of Thiamin Deficiency in Patients with Metabolic and Bariatric Surgery. Nutrients. 2024; 16(14):2226. https://doi.org/10.3390/nu16142226
Chicago/Turabian StyleParrott, Julie M., Austen J. Parrott, J. Scott Parrott, Noel N. Williams, and Kristoffel R. Dumon. 2024. "Predicting Recurrent Deficiency and Suboptimal Monitoring of Thiamin Deficiency in Patients with Metabolic and Bariatric Surgery" Nutrients 16, no. 14: 2226. https://doi.org/10.3390/nu16142226
APA StyleParrott, J. M., Parrott, A. J., Parrott, J. S., Williams, N. N., & Dumon, K. R. (2024). Predicting Recurrent Deficiency and Suboptimal Monitoring of Thiamin Deficiency in Patients with Metabolic and Bariatric Surgery. Nutrients, 16(14), 2226. https://doi.org/10.3390/nu16142226