Abstract
The COVID-19 pandemic lockdowns affected the lifestyles of children and adolescents, leading to an increase in childhood obesity. Paediatric patients with familial hypercholesterolemia (FH) may be more susceptible to lockdown effects due to their increased cardiovascular risk. However, data are lacking. We investigated the effect of lockdowns on the metabolic profile of paediatric patients with FH. Blood lipids and anthropometry measured in September 2021–April 2022 were retrospectively compared with pre-pandemic values. Thirty participants were included (1–16 years; 57% female). From baseline to post-pandemic, median [P25, P75] blood LDL-C concentration was 125 [112, 150] mg/dL vs. 125 [100, 147] mg/dL (p = 0.894); HDL-C was 58 [52, 65] mg/dL vs. 56 [51, 61] mg/dL (p = 0.107); triglycerides were 64 [44, 86] mg/dL vs. 59 [42, 86] mg/dL (p = 0.178). The BMI z-score did not change significantly (0.19 [−0.58, 0.89] vs. 0.30 [−0.48, 1.10], p = 0.524). The lack of deterioration in metabolic profiles during lockdowns is positive, as some deterioration was expected. We speculate that patients and caregivers were successfully educated about healthy lifestyle and dietary habits. Our results should be interpreted with caution since the study sample was small and heterogeneous. Multicentre research is needed to better understand the impact of lockdowns on this population.
1. Introduction
Familial hypercholesterolemia (FH) is an autosomal dominant genetic disorder that affects the metabolism of low-density lipoproteins (LDL), resulting in elevated concentrations of LDL cholesterol (LDL-C) in the blood from birth [1]. Unlike homozygous FH, which is extremely rare, heterozygous FH (or simply FH) affects about one in 300 people [2,3] and is associated with a milder phenotype [4].
It is estimated that 40% of patients with FH have a known genetic cause for this disorder [5], 90% of these due to mutations in the LDL receptor (LDLR) gene [6]. The LDLR is responsible for the uptake of circulating LDL into the liver [7]. Thus, any mutation that impairs the function of this receptor results in deficient LDL-C uptake and its accumulation in the bloodstream [8]. It is estimated that 88% of patients clinically diagnosed with FH without a known genetic cause may have polygenic hypercholesterolemia [9]. This occurs due to the presence of an above average number of alleles that raise LDL-C. [10].
Lifelong cumulative exposure to elevated LDL-C levels severely increases the risk of premature atherosclerosis and cardiovascular disease (CVD) [4,11,12]. Children with FH often show early signs of atherosclerosis [4], and at 25–39 years old, their risk of incident coronary heart disease is 11 and 17 times higher (for men and women, respectively) than the general population [13]. Treatment for FH should therefore be initiated as early as possible to maximize its benefits—preferably during childhood [14]. Lifestyle interventions are the first line of treatment, with the goal of optimizing lipid profiles. Adopting a healthy lifestyle early in life is also key to preventing additional CVD risk factors, such as tobacco use, poor diet, physical inactivity and several chronic illnesses [15,16,17,18]. Many cases require additional treatment with lipid-lowering drugs, such as statins and ezetimibe [4], which can effectively lower blood LDL-C [19] and, ultimately, reduce CVD risk and mortality in adulthood [20,21]. Ideally, treatment should be conducted at a specialized centre [19] by a multidisciplinary team [17], and blood LDL-C should be monitored every 3 to 6 months [22].
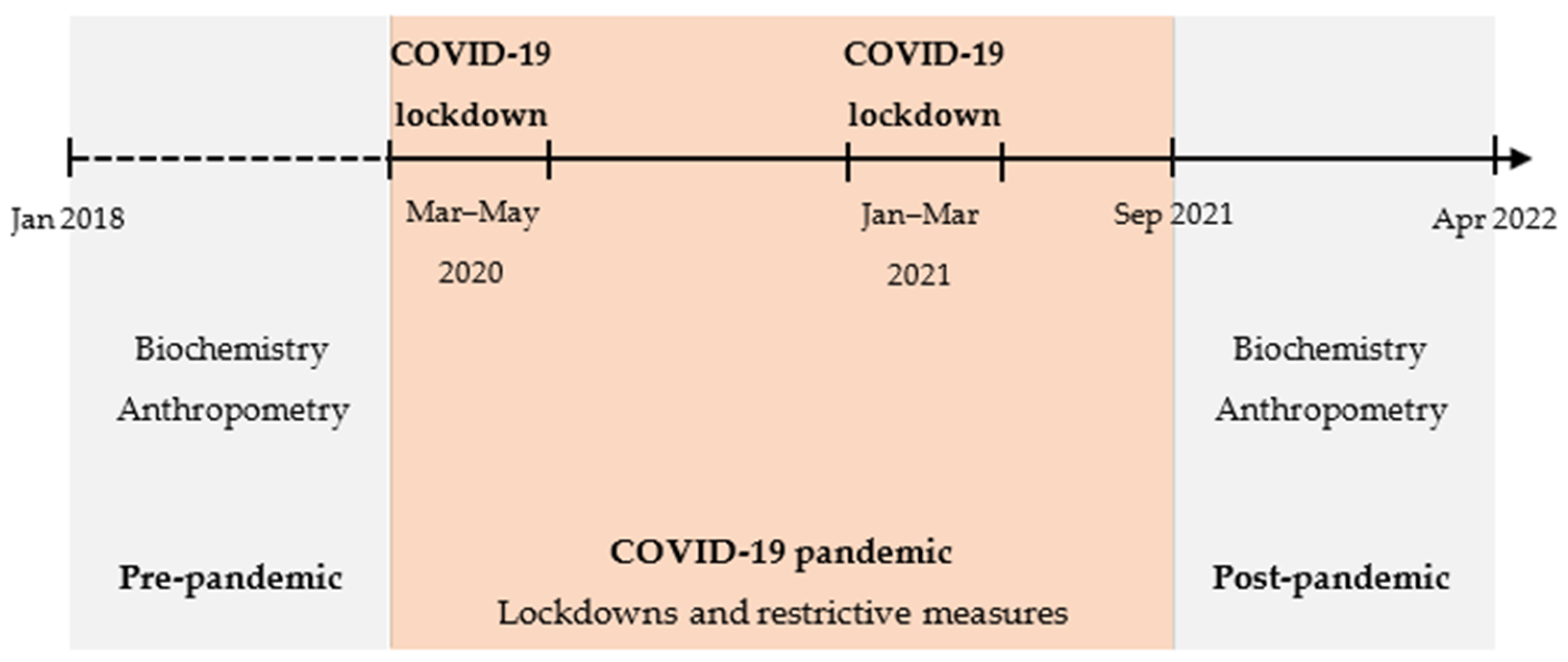
Coronavirus disease 2019 (COVID-19) is a highly transmissible respiratory syndrome. It was declared a pandemic in early 2020 due to its rapid global spread [23,24]. As health services came under severe pressure, many countries implemented restrictive measures to contain the spread of COVID-19 [25,26]. In Portugal, the government imposed two national lockdowns (March–May 2020 and January–March 2021), with mandatory home confinement, closure of schools and businesses, and the obligation to work from home. Health services were also affected, with many appointments, surgeries and interventions being delayed or cancelled. Once the lockdowns were lifted, other restrictive measures were gradually withdrawn over the course of several months [27].
These measures were particularly disruptive for children and adolescents, who had to adapt to online classes, isolation from peers and changes in daily routines [28]. Many—especially those with chronic illnesses—experienced worsening of their mental health, with higher levels of stress, anxiety, depression and even suicidal ideation [29,30,31,32,33].
The eating behaviours and physical activity habits of young people were also impacted. Despite conflicting evidence from isolated studies [34,35], one systematic review [36] demonstrated an overall tendency towards healthier eating habits during lockdown. Adolescents and those from lower socioeconomic groups, however, were more likely to adopt worse eating patterns during this time. The Childhood Obesity Surveillance Initiative (COSI) study [37] showed that, despite an increase in the intake of savoury snacks and sweets, eating home-cooked meals as a family became more frequent among primary school age children. Time spent being physically active among children and adolescents also decreased by 20% during the COVID-19 pandemic [38]. Ultimately, the pandemic landscape has led to increases in childhood obesity rates around the world [39,40]. In Portugal, childhood overweight and obesity increased from 2019 to 2022 for the first time in over a decade, which contradicted the decreasing tendency in previous years [41].
To the best of our knowledge, the effects of COVID-19 lockdowns have been studied in adult patients with FH [42,43] but not in paediatric populations. In adults with FH, negative impacts of the COVID-19 lockdowns on dietary habits, physical activity and lipid profile were reported [42,43,44]. Based on these data, we hypothesized that the lipid and anthropometric profiles of paediatric patients with FH deteriorated during the lockdowns caused by the COVID-19 pandemic.
The aim of this study was to determine whether the COVID-19 pandemic lockdowns affected the lipid and anthropometric profiles of paediatric patients with FH in an exploratory analysis.
2. Materials and Methods
2.1. Study Design
This was a retrospective, longitudinal single-centre study conducted at the Reference Centre of Inherited Metabolic Diseases in Hospital Dona Estefânia, Unidade Local de Saúde São José (ULSSJ).
The participants went through a routine clinical and nutritional assessment between September 2021 and April 2022 (post-pandemic) that included biochemical and anthropometric measurements, which were retrospectively compared with pre-pandemic (baseline) results. We considered the last biochemical analysis performed before the first national lockdown was declared (March 2020).
The primary outcomes were changes in LDL-C concentrations and BMI z-scores between both assessments. Changes in the remaining biochemical and anthropometric parameters were secondary outcomes. The study design is illustrated in Figure 1.
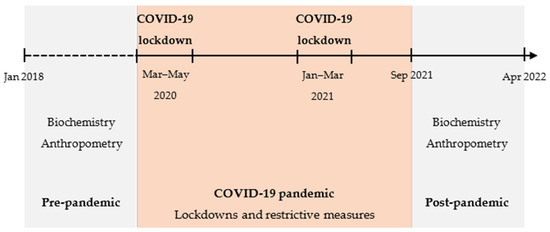
Figure 1.
Study design. COVID-19, coronavirus disease 2019.
2.2. Participants
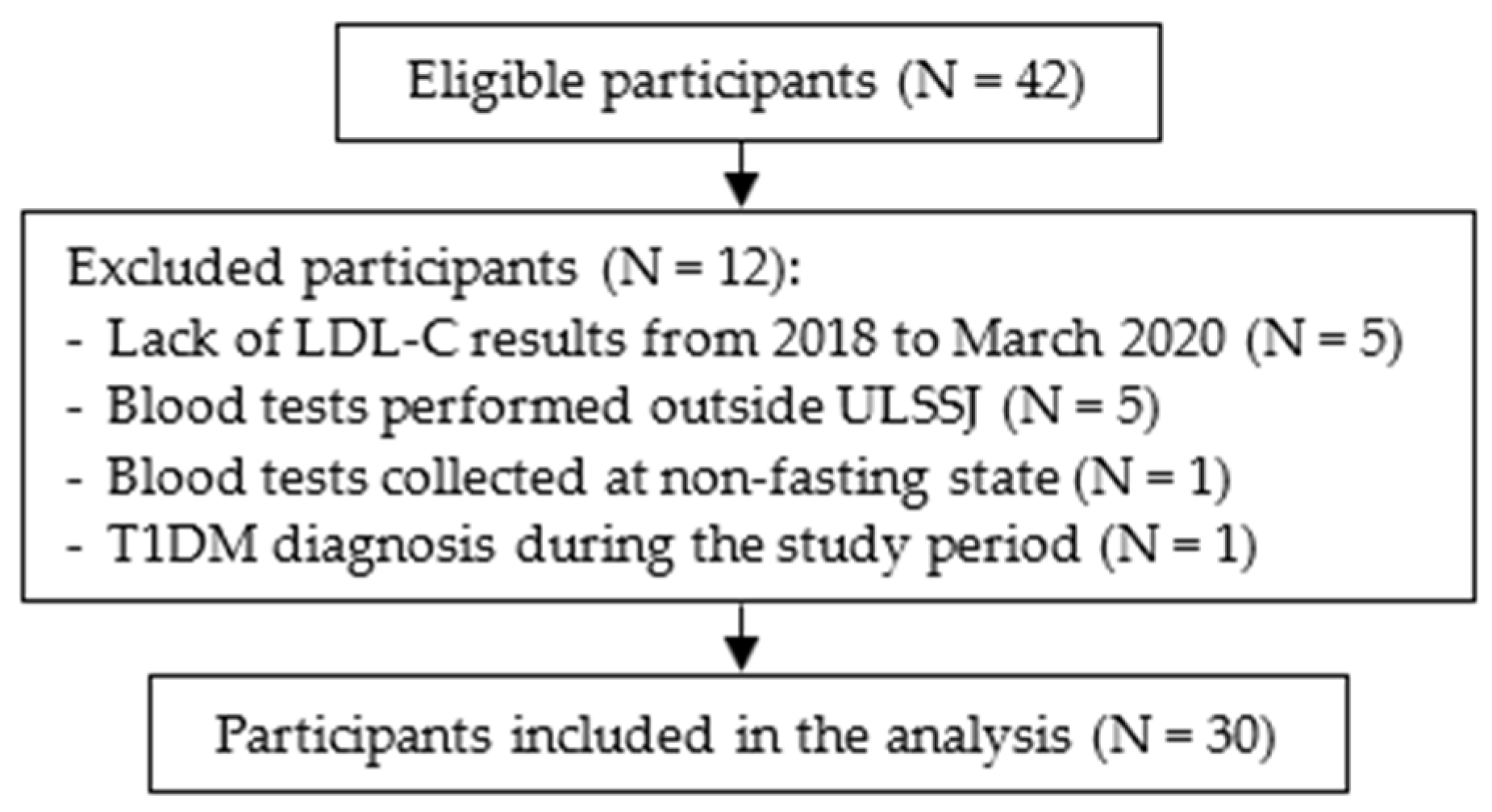
Patients who attended a nutrition appointment between September 2021 and April 2022 were eligible to participate if they were 18 years old or younger, had a confirmed diagnosis of FH and were in follow-up at ULSSJ in 2019. The Simon Broome diagnostic criteria [45] were used to confirm an FH diagnosis. We identified 42 eligible individuals. Exclusion criteria were lack of LDL-C results from 2018 to March 2020 (N = 5); blood tests performed outside of ULSSJ (N = 5); blood samples collected at a non-fasting state (N = 1); and diagnosis of type 1 diabetes mellitus (T1DM) during the study period (N = 1) (Figure 2).
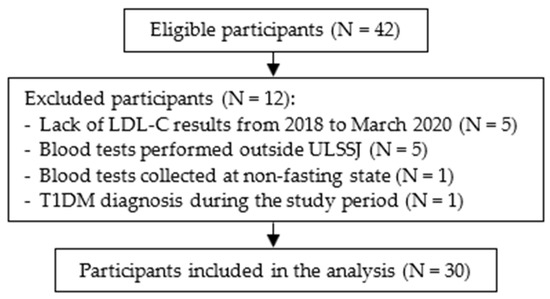
Figure 2.
Participant flowchart. ULSSJ, Unidade Local de Saúde São José; LDL-C, low-density lipoprotein cholesterol; T1DM, type 1 diabetes mellitus.
Patients were invited to participate by the clinical team at routine follow-up hospital visits. A convenience sampling method was used. To reduce the risk of bias and obtain a more representative sample, consecutive cases meeting the inclusion criteria were recruited.
2.3. Data Collection
Data collection was conducted between February and May of 2022 by retrieving data from hospital clinical records. Gender, date of birth, age at follow-up initiation at the Reference Centre, pharmacological treatment with cholesterol-lowering drugs at baseline, length of follow-up at baseline, pre-treatment LDL-C concentration, genetic testing results, family history in terms of hypercholesterolemia, presence of FH mutations, premature CHD and sudden death were documented. Premature CHD was considered when it occurred before the age of 55 years in men and 60 years in women [46].
2.3.1. Lipid Profile and Other Biochemical Parameters
The following parameters of lipid profile were collected at baseline and post-pandemic: LDL-C, HDL-C, triglycerides (TG), total cholesterol (TC), lipoprotein a (Lp(a)), apolipoprotein A (apoA) and apolipoprotein B (apoB). Additional biochemical parameters included glucose, alanine aminotransferase (ALT) and aspartate aminotransferase (AST). Measurements were performed on blood samples collected after an overnight fast at the laboratory in ULSSJ from the Reference Centre of Local Health Unit São José.
Blood lipid concentrations were classified as acceptable, borderline or abnormal according to the cut-offs established in the 2018 Blood Cholesterol guideline, published by the American College of Cardiology and the American Heart Association [47]. LDL-C blood levels were classified as acceptable (<110 mg/dL), borderline (110–129 mg/dL) or abnormal (≥130 mg/dL). For HDL-C, ranges were >45 mg/dL.
The following blood lipid results were considered acceptable, borderline and abnormal, respectively: for LDL-C, <110 mg/dL, 110–129 mg/dL and ≥130 mg/dL; for HDL-C, >45 mg/dL, 40–45 mg/dL and <40 mg/dL; for TG (0–9 years of age), <75 mg/dL, 75–99 mg/dL and ≥100 mg/dL; for TG (10–19 years), <90 mg/dL, 90–129 mg/dL and ≥130 mg/dL; and for TC, <170 mg/dL, 170–199 mg/dL and ≥200 mg/dL.
2.3.2. Anthropometry
Weight and height were measured in light clothing at baseline and post-pandemic. Body weight was measured used a SECA® electronic scale (GmbH & Co. KG, Birmingham, UK) having a precision of 0.1 kg, and height was measured using a stadiometer to the nearest 1 mm. At baseline, single measurements were performed, while in the post-pandemic timepoint, the average of three measurements was calculated. Body mass index (BMI) was calculated as weight (kg)/height (m)2. Weight, height and BMI z-scores were calculated and classified according to the World Health Organization age-specific criteria [48,49,50], using the software WHO Anthro® (WHO, Version 3.2.2) and WHO AnthroPlus® (WHO, Version 1.0.4).
2.4. Statistical Analysis
Statistical analysis was performed using the software IBM® SPSS® Statistics 26 for Windows. Statistical significance was considered when p < 0.05.
The normality of continuous variable distributions was assessed using the Shapiro–Wilk test, complemented by histogram analysis. Normally distributed continuous variables were presented as mean ± standard deviation (SD), while non-normally distributed variables were reported as the median and interquartile range [P25, P75]. For comparisons within the same group (baseline versus post-pandemic), parametric tests (paired samples Student’s t-test) and nonparametric tests (Wilcoxon signed-rank test) were used where appropriate, considering normality assumptions. Hypotheses for categorical variables were tested using a chi-squared test or Fisher’s exact test, as appropriate.
A secondary analysis was conducted to explore potential associations between changes in LDL-C concentrations or BMI z-score and various variables, including biochemical and anthropometric measures, gender, age, genotype and pharmacotherapy. To establish associations with quantitative variables, each variable was categorized into two to three clinically relevant groups, aiming for relatively equal case distribution. Changes in LDL-C concentrations or BMI z-score within each category were assessed using the paired samples Student’s t-test or the Wilcoxon signed-rank test, depending on the normality of the variable’s distribution. Furthermore, differences in changes in LDL-C concentrations and BMI z-score between categories of each variable were analysed. For variables with two categories (e.g., gender), differences were determined using the independent samples t-test for normally distributed variables or the Mann–Whitney test for non-normally distributed variables. For variables with three categories, One-Way ANOVA and Kruskal–Wallis statistical tests were used for normally and non-normally distributed variables, respectively.
2.5. Ethical Statement
This research project respected ethical principles and was approved by the Ethical Committees of NOVA Medical School, Universidade NOVA de Lisboa (No. 128/2021/CEFCM) and Unidade Local de Saúde São José (Process No. 1113/2021). Each participant’s parent was asked to give written informed consent.
Data were collected and used in conformity with the General Data Protection Regulation of the European Union (Regulation (EU) 2016/679) to ensure subject confidentiality. Each participant was given a unique identification number to be used in the project database. Participant names and contact information were stored in a separate file. Both documents were protected by a password and were accessible only to clinical and research team members.
3. Results
3.1. Sample Characteristics
Table 1 shows the characteristics of the study sample (N = 30) at baseline, i.e., in the pre-pandemic period. The study sample included 13 boys and 17 girls aged 1 to 16 years, with a median of 11 years. Participants had been followed up at the Reference Centre for Inherited Metabolic Diseases since the median age of 8 years. In March of 2020, participants had been followed for 3 [1, 5] years (median [P25, P75]).

Table 1.
Baseline sample characteristics.
The median [P25, P75] pre-treatment LDL-C concentration was 158 [136, 197] mg/dL. In most cases, the FH diagnosis was based solely on clinical criteria. Twelve (40%) participants also underwent genetic testing, and three had a confirmed FH causing mutation in the LDLR gene. Three other participants had mutations of likely pathogenicity in the same gene. Five participants had at least one family member with the same mutation. About 27% of participants had a known family history of premature CHD or sudden death, while 90% had family history of hypercholesterolemia.
Changes in LDL-C concentrations or BMI z-score were not associated with any of the previously mentioned variables.
3.2. Lipid Profile and Other Biochemical Parameters
For each variable, the results shown in Table 2 refer to participants who had both pre- and post-pandemic data available. Other participants were excluded from this analysis for better comparability.
Table 2.
Comparison between baseline and post-pandemic regarding age, biochemical parameters and anthropometry.
The median LDL-C concentrations were unchanged between the baseline (125 [112, 150] mg/dL) and post-pandemic period (125 [100, 147] mg/dL); p = 0.894. The median concentrations of HDL-C, TG and TC did not change significantly between baseline and the post-pandemic period, as seen in Table 2. However, TC results were available for only a third of participants.
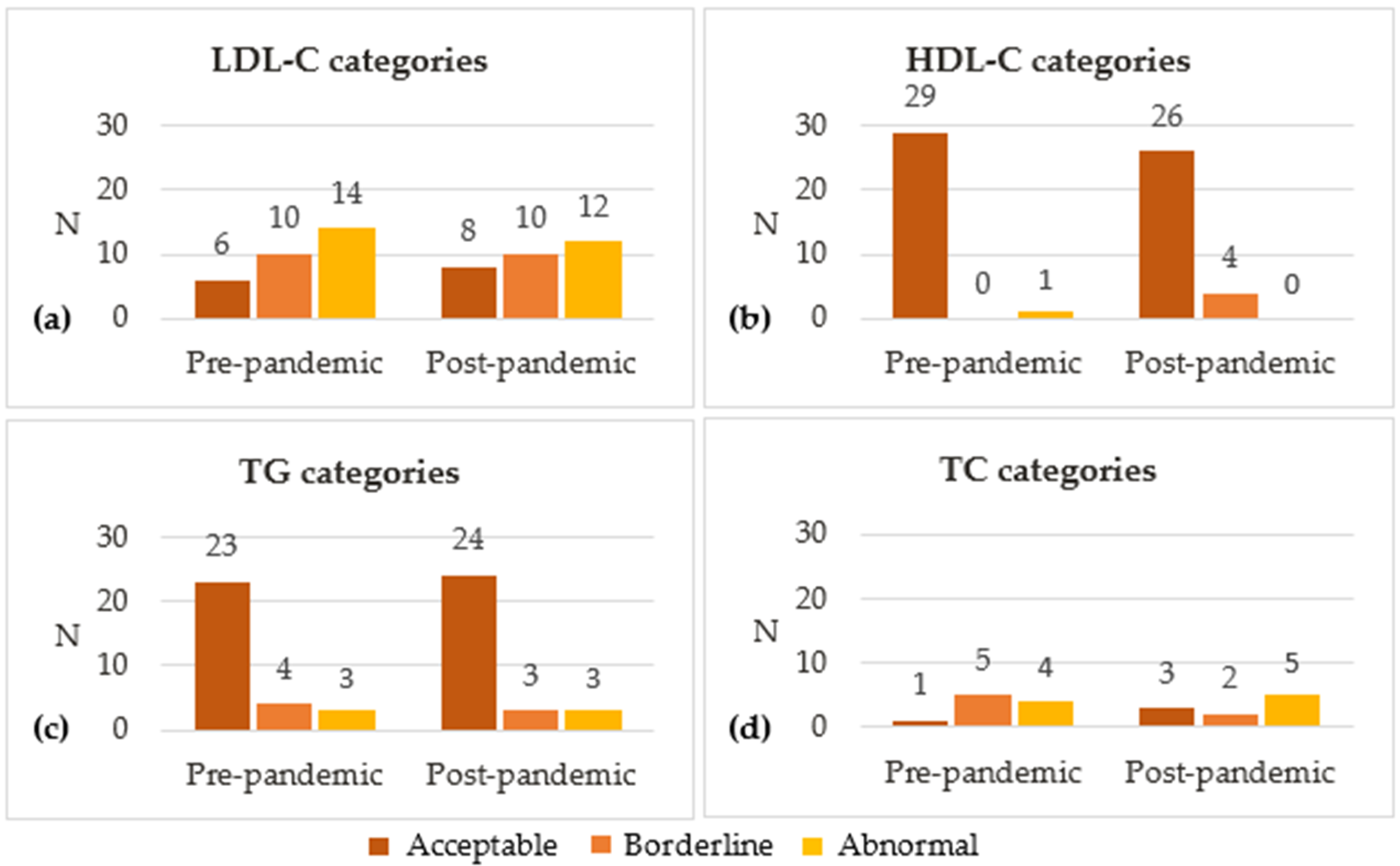
Figure 3 shows the classification of blood lipid concentrations as acceptable, borderline and abnormal. Between baseline and post-pandemic, the percentage of participants with acceptable LDL-C blood levels (<110 mg/dL) increased from 20% to 27%, while those with abnormal LDL-C levels (≥130 mg/dL) decreased from 47% to 40%. Most participants had acceptable levels of HDL-C (>45 mg/dL; 97% vs. 87%) and TG (<75 mg/dL or <90 mg/dL, respectively, for those aged <10 and ≥10 years; 77% vs. 80%) on both period assessments. A minority of the subsample whose TC levels were measured had acceptable TC levels (<170 mg/dL; 10% vs. 30%), with 40% to 50% having abnormal concentrations (≥200 mg/dL) at each moment.
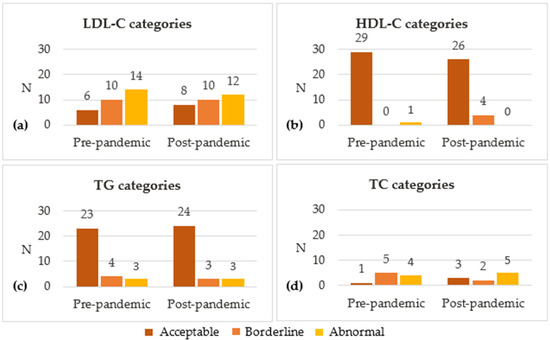
Figure 3.
Distribution of different categories of (a) LDL-C, (b) HDL-C, (c) TG and (d) TC. The following blood lipid results were considered acceptable, borderline and abnormal, respectively: for LDL-C, <110 mg/dL, 110–129 mg/dL and ≥130 mg/dL; for HDL-C, >45 mg/dL, 40–45 mg/dL and <40 mg/dL; for TG (0–9 years of age), <75 mg/dL, 75–99 mg/dL and ≥100 mg/dL; for TG (10–19 years), <90 mg/dL, 90–129 mg/dL and ≥130 mg/dL; and for TC, <170 mg/dL, 170–199 mg/dL and ≥200 mg/dL. HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TC, total cholesterol; TG, triglycerides.
Data were missing for other biochemical parameters, mostly at baseline. The available data allowed comparisons between pre- and post-pandemic results in 10 to 19 participants from the total sample, depending on the variable. Concentrations remained almost unchanged for Lp(a), apoA, apoB, glucose, ALT and AST (as seen in Table 2).
No significant associations were found between any other biochemical variables and changes in LDL-C concentrations or BMI z-score between pre- and post-pandemic periods.
3.3. Anthropometry
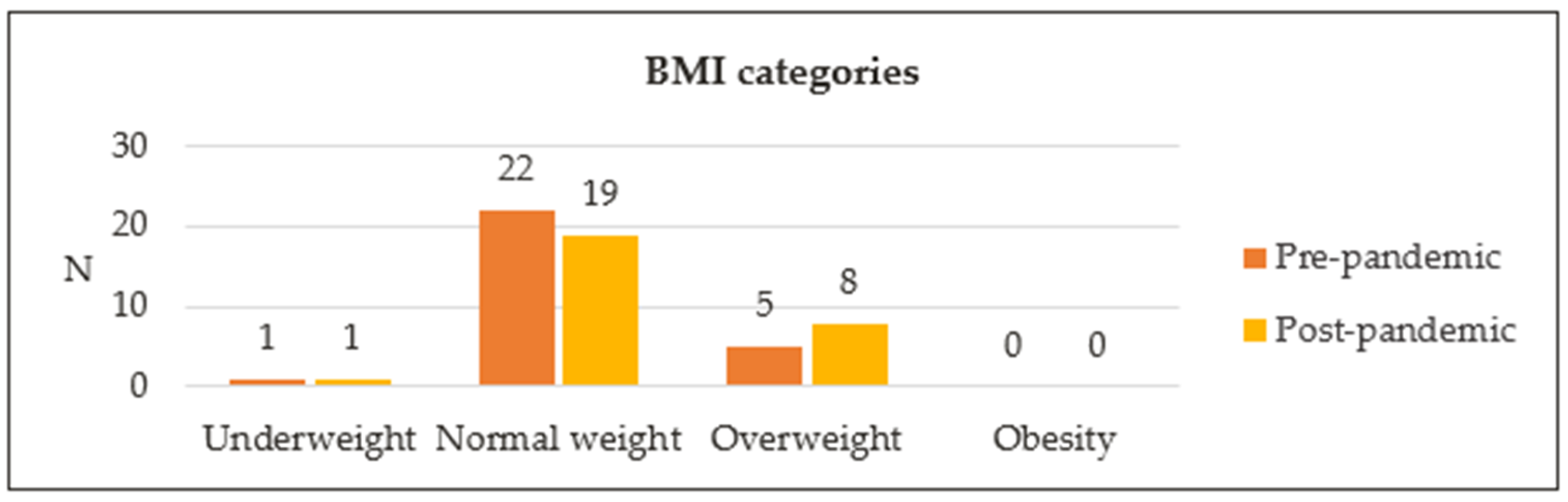
Twenty-eight participants were included in this analysis, as two children had missing anthropometric data at baseline (Table 2). Significant increases (p < 0.001) were seen in median weight, height and BMI between baseline and the post-pandemic period. Changes in height z-score and BMI z-score, however, were not significant. Median height z-score was −0.72 [−1.14, 0.56] at baseline, compared with −0.54 [−1.17, 0.90] post-pandemic (p = 0.097). Median BMI z-score increased from 0.19 [−0.58, 0.89] at baseline to 0.30 [−0.48, 1.10] post-pandemic (p = 0.524). The distribution of BMI categories is represented in Figure 4. Most participants had normal BMI for their age: 79% at baseline vs. 68% post-pandemic. Five participants (18%) were classified as overweight at baseline, vs. eight participants (29%) post-pandemic. One participant who was overweight at baseline reverted to normal weight post-pandemic, while four others of normal weight became overweight in the post-pandemic period.
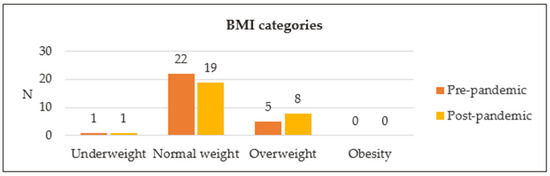
Figure 4.
Distribution of different BMI categories. BMI, body mass index.
No significant associations were found between anthropometric variables and changes in LDL-C concentrations or BMI z-score between the pre- and post-pandemic periods.
4. Discussion
The pandemic caused by COVID-19 led to lockdowns, school closures, self-isolation and social distancing measures across the globe [25]. These restrictive measures have impacted the physical and mental health of children and adolescents [31,51,52,53,54], disrupting their dietary habits [35,36], decreasing physical activity and promoting sedentary behaviours [52,55,56]. In particular, a reduction in physical activity may have an independent negative effect on the lipid profile of children and adolescents [57,58,59]. In this exploratory analysis, we investigated the effects of the COVID-19 pandemic lockdowns on biochemical and anthropometric profiles of children and adolescents with FH in follow-up at our Reference Centre of Inherited Metabolic Diseases. We hypothesized that blood lipids and anthropometric profiles would deteriorate between the pre-pandemic period and September 2021 to April 2022. However, the exploratory findings obtained in a sample of 30 paediatric patients with FH did not confirm our hypothesis. No significant changes were observed between the pre- and post-pandemic periods in median blood concentrations of LDL-C, other parameters of lipid profile or remaining biochemical parameters. The median z-scores for height and BMI remained stable, with very small and non-significant increases.
The changes in median LDL-C concentrations were not significant between the two time point assessments, and the slight increase in TC and decreases in HDL-C and TG were neither statistically nor clinically significant. Taken together with steady Lp(a), apoA and apoB, this suggests an overall stable lipid profile of the participants between the pre-pandemic period and September 2021 to April 2022. The distribution of LDL-C concentrations across the different percentile categories (normal, borderline and abnormal) was also similar in the pre- and post-pandemic periods, which further confirms this notion.
Significant lipid profile deterioration has also been documented in adults with [60] and without [61,62,63] dyslipidaemia. Specifically in adults with FH, the SARS-CoV-2 pandemic severely limited access to lipidologists and cardiologists, resulting in a reduction in lipid profile assessments [43,44]. In these patients, lockdown restrictions also promoted sedentary lifestyles, decreased dietary adherence and increased intake of fatty meals [42,44]. In a retrospective study of 260 adults with FH, significant alterations in the lipid profile were observed 12 months after the implementation of the lockdown measures. These findings included a reduction in the mean HDL-C (53.2 vs. 47.8 mg/dL, p < 0.05) and an increase in the mean non-HDL-C (117.2 vs. 133.1 mg/dL, p < 0.05) [43]. On the other hand, no post-lockdown changes were found in the lipid or glycaemic profiles of children and adolescents with obesity [64,65]—but an increase in the severity of obesity was noted [64].
Regardless of the COVID-19 pandemic lockdowns, some blood lipid profile deterioration could be expected given that the median age of the study population was 11 years at baseline and 13 years in the post-pandemic period. A tendency towards increases in TC, LDL-C and TG during early adolescence has been documented in large cross-sectional studies [66,67,68]. This is likely because early adolescence and puberty are characterized by a temporary decrease in insulin sensitivity and an increase in insulin resistance [69], which can affect lipid metabolism and lead to increased blood cholesterol and TG, as well as decreased HDL-C levels [70].
The median BMI z-score increased from 0.19 to 0.30 between the pre- and post-pandemic periods. However, this increase did not reach statistical significance. In contrast, two meta-analyses [39,40] did find small but significant increases in BMI z-scores and in the prevalence of overweight and obesity among children and adolescents. However, heterogeneity was high for most outcomes in both studies, and the certainty of evidence was very low in the meta-analysis by Anderson et al. [39].
Interestingly, the increase in body weight and BMI was not significant in paediatric sub-populations with chronic conditions (T1DM and obesity) in the meta-analysis by Chang et al. [40], similarly to what was observed in our study sample. However, according to other studies, paediatric patients with overweight and obesity gained weight during the lockdowns [64,65,71,72]. Furthermore, the increase in BMI z-score and reduction in physical activity were more pronounced in children with obesity when compared to children with other endocrine diseases, despite no significant changes to dietary habits [73].
Epidemiological data have shown that increasing trajectories in adiposity in childhood [74] and adolescence [75] are associated with worse cardiometabolic profiles in adulthood. For a child with FH, who is already at a higher risk of CVD than their peers [76], overweight and obesity further increases that risk [77,78]. On the other hand, evidence suggests that reversing high BMI may reduce CVD risk [75,79]. This underscores the importance of nutritional management in paediatric FH, especially when overweight or obesity are present. In the present study, four participants who were previously at a normal weight became overweight during the pandemic. Whether or not this was a direct consequence of the COVID-19 lockdowns, it is crucial to provide closer monitoring and personalized nutritional intervention to these participants.
Another meta-analysis showed improvements in glycaemic control of paediatric patients with T1DM during lockdowns [80]. The authors hypothesized that home confinements may have allowed parents to be more engaged in the management of their child’s condition. In turn, family engagement facilitates healthy dietary changes and is associated with better health outcomes of children with chronic illnesses [81,82,83]. We speculate that this may have been an important factor contributing to the lack of deterioration of post-pandemic lipid and anthropometric profiles in our study. This also suggests that patients from our Reference Centre were well educated regarding the importance of a healthy lifestyle in FH, even before the pandemic. Finally, COVID-19-related fear may have prompted these patients and caregivers to adhere to lifestyle recommendations to reduce the risk of becoming severely ill.
Having a genetic diagnosis of FH in our study sample was not associated with higher LDL-C levels at any time point or a worsening in lipid profile post-pandemic. There are many possible explanations for this. The fact that few participants had identifiable FH mutations likely limited our statistical power to detect significant associations. Additionally, most participants had not undergone genetic testing. Lastly, individuals with negative genetic results may have undetected pathogenic variants, variants in genes that were not analysed in the genetic tests or variants in as-yet-undiscovered genes [1]. Otherwise, the FH phenotype observed in these participants could be explained by a polygenic aetiology [19] or high levels of Lp(a) [84].
To the best of our knowledge, this was the first study to investigate the effects of the restrictive measures and lockdowns amid the COVID-19 pandemic on children and adolescents with FH. We believe this constitutes a major strength of this study. Additionally, this study included other biochemical parameters besides lipid profile and all variables were directly measured, which increased the reliability of our findings.
However, our study had several limitations. This study was retrospective and designed after the start of the COVID-19 pandemic. Data at baseline were not properly controlled, which resulted in lower quality data and more missing information compared to the post-pandemic period. It is possible that this may have masked the magnitude of changes in some relevant outcomes. A convenience sampling method was used, although recruitment of consecutive cases could have mitigated the risk of bias and lack of representativity. Furthermore, the study sample was small and significantly heterogenous in terms of age, length of follow-up, genetic profile and use of lipid-lowering drugs, thereby limiting our statistical power. Pubertal development and body composition were also not assessed. Finally, the absence of data on dietary and physical activity habits, adherence to prescribed drugs, and environmental factors in the pre-pandemic period restricts our ability to fully understand the influence of these lifestyle factors on the metabolic profile of paediatric patients with FH during lockdowns.
5. Conclusions
The results of the present exploratory analysis suggest that the lipid and anthropometric profiles of children and adolescents with FH did not deteriorate after successive lockdowns and restrictive measures imposed to contain the spread of COVID-19. These are positive results that contradicted our hypothesis that there would be some deterioration in lipid and anthropometric profiles. However, there was a small increase in the number of participants with overweight in the post-pandemic period, suggesting a possible negative effect of the lockdowns in these participants.
We speculate that the clinical team at the Reference Centre were successful in educating patients and families about FH, the associated cardiovascular risk and the need to maintain a healthy lifestyle and diet. Ultimately, this awareness may have contributed to patients maintaining healthy habits during the COVID-19 lockdown period.
However, due to the small and heterogeneous study sample, the results of this exploratory analysis should be interpreted with caution. Further research using a multicentre approach is essential to gain a better understanding of the impact of lockdowns on this population.
Author Contributions
Conceptualization, L.P.-d.-S., A.C.F. and J.C.R.; methodology, L.P.-d.-S., A.C.F., A.M.-R. and J.C.R.; formal analysis, M.P. and A.M.-R.; investigation, M.P.; writing—original draft preparation, M.P.; writing—review and editing, all authors; supervision, L.P.-d.-S., A.C.F. and J.C.R. All authors have read and agreed to the published version of the manuscript.
Funding
CINTESIS—UIDB/04255/2020 and UIDP/04255/2020, a program financially supported by Fundação para a Ciência e Tecnologia/Ministério da Ciência, Tecnologia e Ensino Superior, through national funds is acknowledged.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committees of NOVA Medical School, Universidade NOVA de Lisboa (No. 128/2021/CEFCM; approved on 24 September 2021) and Unidade Local de Saúde São José (No. 1113/2021; approved on 29 September 2021).
Informed Consent Statement
Informed consent was obtained from the caregivers of all subjects involved in the study.
Data Availability Statement
The data will be made available from the authors upon reasonable request. The data are not publicly available due to privacy and ethical reasons.
Acknowledgments
This work was conducted as part of an MSc thesis in Human Nutrition and Metabolism by one of the authors (MP) at NOVA Medical School, Faculdade de Ciências Médicas, Universidade NOVA de Lisboa, Lisboa, Portugal.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Watts, G.F.; Gidding, S.; Wierzbicki, A.S.; Toth, P.P.; Alonso, R.; Brown, W.V.; Bruckert, E.; Defesche, J.; Lin, K.K.; Livingston, M.; et al. Integrated guidance on the care of familial hypercholesterolaemia from the International FH Foundation. Eur. J. Prev. Cardiol. 2015, 22, 849–854. [Google Scholar] [CrossRef]
- Hu, P.; Dharmayat, K.I.; Stevens, C.A.T.; Sharabiani, M.T.A.; Jones, R.S.; Watts, G.F.; Genest, J.; Ray, K.K.; Vallejo-Vaz, A.J. Prevalence of Familial Hypercholesterolemia Among the General Population and Patients With Atherosclerotic Cardiovascular Disease: A Systematic Review and Meta-Analysis. Circulation 2020, 141, 1742–1759. [Google Scholar] [CrossRef]
- Beheshti, S.O.; Madsen, C.M.; Varbo, A.; Nordestgaard, B.G. Worldwide Prevalence of Familial Hypercholesterolemia: Meta-Analyses of 11 Million Subjects. J. Am. Coll. Cardiol. 2020, 75, 2553–2566. [Google Scholar] [CrossRef] [PubMed]
- Reijman, M.D.; Kusters, D.M.; Wiegman, A. Advances in familial hypercholesterolaemia in children. Lancet Child Adolesc. Health 2021, 5, 652–661. [Google Scholar] [CrossRef]
- Taylor, A.; Wang, D.; Patel, K.; Whittall, R.; Wood, G.; Farrer, M.; Neely, R.D.; Fairgrieve, S.; Nair, D.; Barbir, M.; et al. Mutation detection rate and spectrum in familial hypercholesterolaemia patients in the UK pilot cascade project. Clin. Genet 2010, 77, 572–580. [Google Scholar] [CrossRef] [PubMed]
- Austin, M.A.; Hutter, C.M.; Zimmern, R.L.; Humphries, S.E. Genetic causes of monogenic heterozygous familial hypercholesterolemia: A HuGE prevalence review. Am. J. Epidemiol. 2004, 160, 407–420. [Google Scholar] [CrossRef]
- Jeon, H.; Blacklow, S.C. Structure and physiologic function of the low-density lipoprotein receptor. Annu. Rev. Biochem. 2005, 74, 535–562. [Google Scholar] [CrossRef] [PubMed]
- Defesche, J.C.; Gidding, S.S.; Harada-Shiba, M.; Hegele, R.A.; Santos, R.D.; Wierzbicki, A.S. Familial hypercholesterolaemia. Nat. Rev. Dis. Primers 2017, 3, 17093. [Google Scholar] [CrossRef]
- Futema, M.; Shah, S.; Cooper, J.A.; Li, K.; Whittall, R.A.; Sharifi, M.; Goldberg, O.; Drogari, E.; Mollaki, V.; Wiegman, A.; et al. Refinement of Variant Selection for the LDL Cholesterol Genetic Risk Score in the Diagnosis of the Polygenic Form of Clinical Familial Hypercholesterolemia and Replication in Samples from 6 Countries. Clin. Chem. 2015, 61, 231–238. [Google Scholar] [CrossRef]
- Talmud, P.J.; Shah, S.; Whittall, R.; Futema, M.; Howard, P.; Cooper, J.A.; Harrison, S.C.; Li, K.; Drenos, F.; Karpe, F.; et al. Use of low-density lipoprotein cholesterol gene score to distinguish patients with polygenic and monogenic familial hypercholesterolaemia: A case-control study. Lancet 2013, 381, 1293–1301. [Google Scholar] [CrossRef] [PubMed]
- Viigimaa, M.; Heinsar, S.; Lovic, D.; Katsimardou, A.; Piperidou, A.; Duishvili, D. New Horizons in the Pathogenesis, Pathophysiology and Treatment of Familial Hypercholesterolaemia. Curr. Pharm. Des. 2018, 24, 3599–3604. [Google Scholar] [CrossRef] [PubMed]
- Borén, J.; Chapman, M.J.; Krauss, R.M.; Packard, C.J.; Bentzon, J.F.; Binder, C.J.; Daemen, M.J.; Demer, L.L.; Hegele, R.A.; Nicholls, S.J.; et al. Low-density lipoproteins cause atherosclerotic cardiovascular disease: Pathophysiological, genetic, and therapeutic insights: A consensus statement from the European Atherosclerosis Society Consensus Panel. Eur. Heart J. 2020, 41, 2313–2330. [Google Scholar] [CrossRef] [PubMed]
- Mundal, L.J.; Igland, J.; Veierød, M.B.; Holven, K.B.; Ose, L.; Selmer, R.M.; Wisloff, T.; Kristiansen, I.S.; Tell, G.S.; Leren, T.P.; et al. Impact of age on excess risk of coronary heart disease in patients with familial hypercholesterolaemia. Heart 2018, 104, 1600. [Google Scholar] [CrossRef]
- Banderali, G.; Capra, M.E.; Biasucci, G.; Stracquadaino, R.; Viggiano, C.; Pederiva, C. Detecting Familial hypercholesterolemia in children and adolescents: Potential and challenges. Ital. J. Pediatr. 2022, 48, 115. [Google Scholar] [CrossRef] [PubMed]
- Akioyamen, L.E.; Genest, J.; Chu, A.; Inibhunu, H.; Ko, D.T.; Tu, J.V. Risk factors for cardiovascular disease in heterozygous familial hypercholesterolemia: A systematic review and meta-analysis. J. Clin. Lipidol. 2019, 13, 15–30. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, E.B.; Hedegaard, B.S.; Retterstøl, K. Familial hypercholesterolaemia: History, diagnosis, screening, management and challenges. Heart 2020, 106, 1940–1946. [Google Scholar] [CrossRef] [PubMed]
- Watts, G.F.; Gidding, S.S.; Mata, P.; Pang, J.; Sullivan, D.R.; Yamashita, S.; Raal, F.J.; Santos, R.D.; Ray, K.K. Familial hypercholesterolaemia: Evolving knowledge for designing adaptive models of care. Nat. Rev. Cardiol. 2020, 17, 360–377. [Google Scholar] [CrossRef] [PubMed]
- Yusuf, S.; Joseph, P.; Rangarajan, S.; Islam, S.; Mente, A.; Hystad, P.; Brauer, M.; Kutty, V.R.; Gupta, R.; Wielgosz, A.; et al. Modifiable risk factors, cardiovascular disease, and mortality in 155 722 individuals from 21 high-income, middle-income, and low-income countries (PURE): A prospective cohort study. Lancet 2020, 395, 795–808. [Google Scholar] [CrossRef] [PubMed]
- Mainieri, F.; Tagi, V.M.; Chiarelli, F. Recent Advances on Familial Hypercholesterolemia in Children and Adolescents. Biomedicines 2022, 10, 1043. [Google Scholar] [CrossRef]
- Luirink, I.K.; Wiegman, A.; Kusters, D.M.; Hof, M.H.; Groothoff, J.W.; de Groot, E.; Kastelein, J.J.P.; Hutten, B.A. 20-Year Follow-up of Statins in Children with Familial Hypercholesterolemia. N. Engl. J. Med. 2019, 381, 1547–1556. [Google Scholar] [CrossRef]
- Tada, H.; Kojima, N.; Yamagami, K.; Nomura, A.; Nohara, A.; Usui, S.; Sakata, K.; Takamura, M.; Kawashiri, M.-a. Early diagnosis and treatments in childhood are associated with better prognosis in patients with familial hypercholesterolemia. Am. J. Prev. Cardiol. 2022, 12, 100434. [Google Scholar] [CrossRef] [PubMed]
- Koletzko, B. 3.20 Hypercholesterolemia. In Pediatric Nutrition in Practice, 3rd ed.; Koletzko, B., Bhutta, Z.A., Cai, W., Dhansay, M.A., Duggan, C.P., Makrides, M., Orsi, M., Eds.; World Review of Nutrition and Dietetics; Karger: Basel, Switzerland, 2022; Volume 124, pp. 362–367. [Google Scholar]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19—11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 1 March 2023).
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Onyeaka, H.; Anumudu, C.K.; Al-Sharify, Z.T.; Egele-Godswill, E.; Mbaegbu, P. COVID-19 pandemic: A review of the global lockdown and its far-reaching effects. Sci. Prog. 2021, 104, 00368504211019854. [Google Scholar] [CrossRef]
- Wang, D.; Mao, Z. A comparative study of public health and social measures of COVID-19 advocated in different countries. Health Policy 2021, 125, 957–971. [Google Scholar] [CrossRef] [PubMed]
- Ferreira da Silva, R.; Macedo, M.; Conceição, J. A pandemia de COVID-19 em Portugal: Evolução, Vacinação e Farmacovigilância. RevistaMultidisciplinar 2022, 4, 135–154. [Google Scholar] [CrossRef]
- Capra, M.E.; Stanyevic, B.; Giudice, A.; Monopoli, D.; Decarolis, N.M.; Esposito, S.; Biasucci, G. The Effects of COVID-19 Pandemic and Lockdown on Pediatric Nutritional and Metabolic Diseases: A Narrative Review. Nutrients 2022, 15, 88. [Google Scholar] [CrossRef]
- Sharma, M.; Idele, P.; Manzini, A.; Aladro, C.; Ipince, A.; Olsson, G.; Banati, P.; Anthony, D. Life in Lockdown: Child and Adolescent Mental Health and Well-Being in the Time of COVID-19; UNICEF Office of Research—Innocenti: Florence, Italy, 2021. [Google Scholar]
- Di Fazio, N.; Morena, D.; Delogu, G.; Volonnino, G.; Manetti, F.; Padovano, M.; Scopetti, M.; Frati, P.; Fineschi, V. Mental Health Consequences of COVID-19 Pandemic Period in the European Population: An Institutional Challenge. Int. J. Environ. Res. Public Health 2022, 19, 9347. [Google Scholar] [CrossRef] [PubMed]
- Harrison, L.; Carducci, B.; Klein, J.D.; Bhutta, Z.A. Indirect effects of COVID-19 on child and adolescent mental health: An overview of systematic reviews. BMJ Glob. Health 2022, 7, e010713. [Google Scholar] [CrossRef]
- Samji, H.; Wu, J.; Ladak, A.; Vossen, C.; Stewart, E.; Dove, N.; Long, D.; Snell, G. Review: Mental health impacts of the COVID-19 pandemic on children and youth—A systematic review. Child Adolesc. Ment. Health 2022, 27, 173–189. [Google Scholar] [CrossRef]
- Saulle, R.; De Sario, M.; Bena, A.; Capra, P.; Culasso, M.; Davoli, M.; De Lorenzo, A.; Lattke, L.S.; Marra, M.; Mitrova, Z.; et al. School closures and mental health, wellbeing and health behaviours among children and adolescents during the second COVID-19 wave: A systematic review of the literature. Epidemiol. Prev. 2022, 46, 333–352. [Google Scholar] [CrossRef]
- Medrano, M.; Cadenas-Sanchez, C.; Oses, M.; Arenaza, L.; Amasene, M.; Labayen, I. Changes in lifestyle behaviours during the COVID-19 confinement in Spanish children: A longitudinal analysis from the MUGI project. Pediatr. Obes. 2020, 16, e12731. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Roso, M.B.; de Carvalho Padilha, P.; Mantilla-Escalante, D.C.; Ulloa, N.; Brun, P.; Acevedo-Correa, D.; Arantes Ferreira Peres, W.; Martorell, M.; Aires, M.T.; de Oliveira Cardoso, L.; et al. COVID-19 Confinement and Changes of Adolescent’s Dietary Trends in Italy, Spain, Chile, Colombia and Brazil. Nutrients 2020, 12, 1807. [Google Scholar] [CrossRef]
- Brakspear, L.; Boules, D.; Nicholls, D.; Burmester, V. The Impact of COVID-19-Related Living Restrictions on Eating Behaviours in Children and Adolescents: A Systematic Review. Nutrients 2022, 14, 3657. [Google Scholar] [CrossRef]
- World Health Organization—European Region. Nutrition, Physical Activity, Well-Being and COVID-19—Results from 13 Countries Participating in Round 6 of the Childhood Obesity Surveillance Initiative Study; WHO: Geneva, Switzerland, 2023.
- Neville, R.D.; Lakes, K.D.; Hopkins, W.G.; Tarantino, G.; Draper, C.E.; Beck, R.; Madigan, S. Global Changes in Child and Adolescent Physical Activity During the COVID-19 Pandemic: A Systematic Review and Meta-analysis. JAMA Pediatr. 2022, 176, 886–894. [Google Scholar] [CrossRef]
- Anderson, L.N.; Yoshida-Montezuma, Y.; Dewart, N.; Jalil, E.; Khattar, J.; De Rubeis, V.; Carsley, S.; Griffith, L.E.; Mbuagbaw, L. Obesity and weight change during the COVID-19 pandemic in children and adults: A systematic review and meta-analysis. Obes. Rev. 2023, 24, e13550. [Google Scholar] [CrossRef] [PubMed]
- Chang, T.-H.; Chen, Y.-C.; Chen, W.-Y.; Chen, C.-Y.; Hsu, W.-Y.; Chou, Y.; Chang, Y.-H. Weight Gain Associated with COVID-19 Lockdown in Children and Adolescents: A Systematic Review and Meta-Analysis. Nutrients 2021, 13, 3668. [Google Scholar] [CrossRef]
- Departamento de Alimentação e Nutrição. Infográfico—Obesidade Infantil 2022; Instituto Nacional de Saúde Doutor Ricardo Jorge: Lisbon, Portugal, 2023.
- Kayikcioglu, M.; Tokgozoglu, L.; Tuncel, O.K.; Pirildar, S.; Can, L. Negative impact of COVID-19 pandemic on the lifestyle and management of patients with homozygous familial hypercholesterolemia. J. Clin. Lipidol. 2020, 14, 751–755. [Google Scholar] [CrossRef] [PubMed]
- Scicali, R.; Piro, S.; Ferrara, V.; Di Mauro, S.; Filippello, A.; Scamporrino, A.; Romano, M.; Purrello, F.; Di Pino, A. Direct and Indirect Effects of SARS-CoV-2 Pandemic in Subjects with Familial Hypercholesterolemia: A Single Lipid-Center Real-World Evaluation. J. Clin. Med. 2021, 10, 4363. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.; Leung, K.S.K.; Garg, T.; Mazzoleni, A.; Miteu, G.D.; Zakariya, F.; Awuah, W.A.; Yin, E.T.S.; Haroon, F.; Hussain, Z.; et al. Barriers and shortcomings in access to cardiovascular management and prevention for familial hypercholesterolemia during the COVID-19 pandemic. Clin. Cardiol. 2023, 46, 831–844. [Google Scholar] [CrossRef]
- Risk of fatal coronary heart disease in familial hypercholesterolaemia. Scientific Steering Committee on behalf of the Simon Broome Register Group. BMJ 1991, 303, 893–896. [Google Scholar] [CrossRef]
- Wiegman, A.; Gidding, S.S.; Watts, G.F.; Chapman, M.J.; Ginsberg, H.N.; Cuchel, M.; Ose, L.; Averna, M.; Boileau, C.; Borén, J.; et al. Familial hypercholesterolaemia in children and adolescents: Gaining decades of life by optimizing detection and treatment. Eur. Heart J. 2015, 36, 2425–2437. [Google Scholar] [CrossRef] [PubMed]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Blood Cholesterol: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e1082–e1143. [Google Scholar] [CrossRef] [PubMed]
- de Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. BMI-for-Age (0–5 years). Available online: https://www.who.int/childgrowth/standards/bmi_for_age/en/ (accessed on 22 September 2022).
- World Health Organization. BMI-for-Age (5–19 years). Available online: http://www.who.int/growthref/who2007_bmi_for_age/en/ (accessed on 22 September 2022).
- Heidari-Beni, M.; Bemanalizadeh, M.; Heshmat, R.; Qorbani, M.; Kelishadi, R. Changes in Lifestyle Behaviors of Children and Adolescents during the COVID-19 Pandemic and the Impact on the Development of Non-Communicable Diseases: A Narrative Review. Med. J. Islam. Repub. Iran 2022, 36, 165. [Google Scholar] [CrossRef]
- Ilesanmi, O.; Afolabi, A.; Kwaghe, A. A scope review on the global impact of COVID-19 lockdown on adolescents’ health. Afr. Health Sci. 2021, 21, 1518–1526. [Google Scholar] [CrossRef] [PubMed]
- Panchal, U.; Salazar de Pablo, G.; Franco, M.; Moreno, C.; Parellada, M.; Arango, C.; Fusar-Poli, P. The impact of COVID-19 lockdown on child and adolescent mental health: Systematic review. Eur. Child Adolesc. Psychiatry 2021, 32, 1151–1177. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.; Shah, N.; Mbeledogu, C.; Garstang, J. Child wellbeing in the United Kingdom following the COVID-19 lockdowns. Paediatr. Child Health 2021, 31, 445–448. [Google Scholar] [CrossRef] [PubMed]
- Caroppo, E.; Mazza, M.; Sannella, A.; Marano, G.; Avallone, C.; Claro, A.E.; Janiri, D.; Moccia, L.; Janiri, L.; Sani, G. Will Nothing Be the Same Again?: Changes in Lifestyle during COVID-19 Pandemic and Consequences on Mental Health. Int. J. Environ. Res. Public Health 2021, 18, 8433. [Google Scholar] [CrossRef] [PubMed]
- Rahman, A.M.; Chandrasekaran, B. Estimating the Impact of the Pandemic on Children’s Physical Health: A Scoping Review. J. Sch. Health 2021, 91, 936–947. [Google Scholar] [CrossRef]
- Barbosa, A.O.; Silva, J.; Silva, D.J.; Cabral, T.G.; Jesus, F.M.; Mendonça, G.; Prazeres Filho, A.; Moura, I.R.D.; Cristina da Costa Silva, E.; Rocha, S.; et al. Longitudinal association between moderate to vigorous physical activity and lipid profile indicators in adolescents. Eur. J. Sport. Sci. 2023, 23, 1405–1414. [Google Scholar] [CrossRef]
- Gil-Campos, M.; Pérez-Ferreirós, A.; Llorente-Cantarero, F.J.; Anguita-Ruiz, A.; Bedoya-Carpente, J.J.; Kalén, A.; Moreno, L.A.; Bueno, G.; Gil, Á.; Aguilera, C.M.; et al. Association of Diet, Physical Activity Guidelines and Cardiometabolic Risk Markers in Children. Nutrients 2021, 13, 2954. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, A.G.; Janssen, I. Dose-response relationship between physical activity and dyslipidemia in youth. Can. J. Cardiol. 2010, 26, 201–205. [Google Scholar] [CrossRef]
- Perrone, M.A.; Feola, A.; Pieri, M.; Donatucci, B.; Salimei, C.; Lombardo, M.; Perrone, A.; Parisi, A. The Effects of Reduced Physical Activity on the Lipid Profile in Patients with High Cardiovascular Risk during COVID-19 Lockdown. Int. J. Environ. Res. Public Health 2021, 18, 8858. [Google Scholar] [CrossRef] [PubMed]
- Lia, L.; Ricci, E.; Colaprico, C.; Di Legge, E.; Faticoni, A.; Donini, L.M.; La Torre, G. Assessment of the Impact of COVID-19 Lockdown on the Nutritional Status and Lipid Profile of Employees in a Teaching Hospital in Rome: A Retrospective Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 4549. [Google Scholar] [CrossRef] [PubMed]
- Ramírez Manent, J.I.; Altisench Jané, B.; Sanchís Cortés, P.; Busquets-Cortés, C.; Arroyo Bote, S.; Masmiquel Comas, L.; López González, Á.A. Impact of COVID-19 Lockdown on Anthropometric Variables, Blood Pressure, and Glucose and Lipid Profile in Healthy Adults: A before and after Pandemic Lockdown Longitudinal Study. Nutrients 2022, 14, 1237. [Google Scholar] [CrossRef]
- He, Z.; Zhang, Y.; Xu, X.; Mei, Y.; Rahmani, J.; Seraj, S.S.; Qi, X. COVID-19 Pandemic Impact on Cardiometabolic Markers in Adults in Chongqing, China: A Retrospective Cohort Study. Front. Public Health 2022, 10, 859488. [Google Scholar] [CrossRef]
- Samur, B.M.; Samur, T.G.; Gul-Sir, U.; Hatipoglu, N. Vicious cycle between severity of childhood obesity and pandemic: Potential impact of metformin. Obes. Med. 2022, 33, 100433. [Google Scholar] [CrossRef]
- Valenzise, M.; D’Amico, F.; Cucinotta, U.; Lugarà, C.; Zirilli, G.; Zema, A.; Wasniewska, M.; Pajno, G.B. The lockdown effects on a pediatric obese population in the COVID-19 era. Ital. J. Pediatr. 2021, 47, 209. [Google Scholar] [CrossRef] [PubMed]
- Hickman, T.B.; Briefel, R.R.; Carroll, M.D.; Rifkind, B.M.; Cleeman, J.I.; Maurer, K.R.; Johnson, C.L. Distributions and trends of serum lipid levels among United States children and adolescents ages 4-19 years: Data from the Third National Health and Nutrition Examination Survey. Prev. Med. 1998, 27, 879–890. [Google Scholar] [CrossRef] [PubMed]
- Cook, S.; Auinger, P.; Huang, T.T.K. Growth Curves for Cardio-Metabolic Risk Factors in Children and Adolescents. J. Pediatr. 2009, 155, S6.e15–S16.e26. [Google Scholar] [CrossRef]
- Tamir, I.; Heiss, G.; Glueck, C.J.; Christensen, B.; Kwiterovich, P.; Rifkind, B.M. Lipid and lipoprotein distributions in white children ages 6-19 yr. The lipid research clinics program prevalence study. J. Chronic. Dis. 1981, 34, 27–39. [Google Scholar] [CrossRef] [PubMed]
- Tagi, V.M.; Samvelyan, S.; Chiarelli, F. An update of the consensus statement on insulin resistance in children 2010. Front. Endocrinol. 2022, 13, 1061524. [Google Scholar] [CrossRef] [PubMed]
- Ormazabal, V.; Nair, S.; Elfeky, O.; Aguayo, C.; Salomon, C.; Zuñiga, F.A. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc. Diabetol. 2018, 17, 122. [Google Scholar] [CrossRef]
- Arayess, L.; Knockaert, N.; Winkens, B.; Lubrecht, J.W.; Verweij, M.; Vreugdenhil, A.C.E. The Side-Effects of the COVID-19 Pandemic: Increased BMI z-Score in Children with Overweight and Obesity in a Personalised Lifestyle Intervention One Year after the Start of the Pandemic in The Netherlands. Nutrients 2022, 14, 1942. [Google Scholar] [CrossRef] [PubMed]
- Pietrobelli, A.; Fearnbach, N.; Ferruzzi, A.; Vrech, M.; Heo, M.; Faith, M.; Pecoraro, L.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; et al. Effects of COVID-19 lockdown on lifestyle behaviors in children with obesity: Longitudinal study update. Obes. Sci. Pract. 2022, 8, 525–528. [Google Scholar] [CrossRef] [PubMed]
- Zachurzok, A.; Wójcik, M.; Gawlik, A.; Starzyk, J.B.; Mazur, A. An Attempt to Assess the Impact of Pandemic Restrictions on the Lifestyle, Diet, and Body Mass Index of Children with Endocrine Diseases-Preliminary Results. Nutrients 2021, 14, 156. [Google Scholar] [CrossRef] [PubMed]
- Bjerregaard, L.G.; Adelborg, K.; Baker, J.L. Change in body mass index from childhood onwards and risk of adult cardiovascular disease. Trends Cardiovasc. Med. 2020, 30, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Araújo, J.; Barros, H.; Ramos, E.; Li, L. Trajectories of total and central adiposity throughout adolescence and cardiometabolic factors in early adulthood. Int. J. Obes. 2016, 40, 1899–1905. [Google Scholar] [CrossRef]
- Poznyak, A.V.; Litvinova, L.; Poggio, P.; Orekhov, A.N.; Melnichenko, A.A. Familial Hypercholesterolaemia as a Predisposing Factor for Atherosclerosis. Biomedicines 2022, 10, 2639. [Google Scholar] [CrossRef]
- Alonso, R.; Mata, N.; Castillo, S.; Fuentes, F.; Saenz, P.; Muñiz, O.; Galiana, J.; Figueras, R.; Diaz, J.L.; Gomez-Enterría, P.; et al. Cardiovascular disease in familial hypercholesterolaemia: Influence of low-density lipoprotein receptor mutation type and classic risk factors. Atherosclerosis 2008, 200, 315–321. [Google Scholar] [CrossRef]
- Besseling, J.; Kindt, I.; Hof, M.; Kastelein, J.J.; Hutten, B.A.; Hovingh, G.K. Severe heterozygous familial hypercholesterolemia and risk for cardiovascular disease: A study of a cohort of 14,000 mutation carriers. Atherosclerosis 2014, 233, 219–223. [Google Scholar] [CrossRef] [PubMed]
- Buscot, M.J.; Thomson, R.J.; Juonala, M.; Sabin, M.A.; Burgner, D.P.; Lehtimäki, T.; Hutri-Kähönen, N.; Viikari, J.S.A.; Raitakari, O.T.; Magnussen, C.G. Distinct child-to-adult body mass index trajectories are associated with different levels of adult cardiometabolic risk. Eur. Heart J. 2018, 39, 2263–2270. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.; Chen, Y.; Sun, C.; Zhou, Z. The impact of COVID lockdown on glycaemic control in paediatric patients with type 1 diabetes: A systematic review and meta-analysis of 22 observational studies. Front. Endocrinol. 2022, 13, 1069559. [Google Scholar] [CrossRef]
- Pugh, P.; Hemingway, P.; Christian, M.; Higginbottom, G. Children’s, parents’, and other stakeholders’ perspectives on the factors influencing the initiation of early dietary change in the management of childhood chronic disease: A mixed studies systematic review using a narrative synthesis. Patient Educ. Couns. 2021, 104, 844–857. [Google Scholar] [CrossRef]
- Smith, B.M.; Sharma, R.; Das, A.; Aboumatar, H.; Pitts, S.I.; Day, J.; Holzhauer, K.; Bass, E.; Bennett, W.L. Patient and family engagement strategies for children and adolescents with chronic diseases: A review of systematic reviews. Patient Educ. Couns. 2021, 104, 2213–2223. [Google Scholar] [CrossRef]
- Carman, K.L.; Dardess, P.; Maurer, M.; Sofaer, S.; Adams, K.; Bechtel, C.; Sweeney, J. Patient and family engagement: A framework for understanding the elements and developing interventions and policies. Health Aff. 2013, 32, 223–231. [Google Scholar] [CrossRef]
- Ellis, K.L.; Pang, J.; Chan, D.C.; Hooper, A.J.; Bell, D.A.; Burnett, J.R.; Watts, G.F. Familial combined hyperlipidemia and hyperlipoprotein(a) as phenotypic mimics of familial hypercholesterolemia: Frequencies, associations and predictions. J. Clin. Lipidol. 2016, 10, 1329–1337.e1323. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).