
Food Resource Management and Healthy Eating Focus Associates with Diet Quality and Health Behaviors in Low-Income Adults

 , ,
, , 
 and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Overview
2.2. Assessment of Sociodemographic, Health, and Lifestyle Characteristics
2.3. Diet Quality Assessment
2.4. Assessment of Food Management Skills
2.5. Assessment of Healthy Eating Focus
2.6. Assessment of the Impact of COVID-19 Pandemic on Changes in Health-Related Behaviors
2.7. Statistical Analysis
3. Results
3.1. Sociodemographic and Health Characteristics
3.2. The Association of FRM and Healthy Eating Focus with Diet Quality
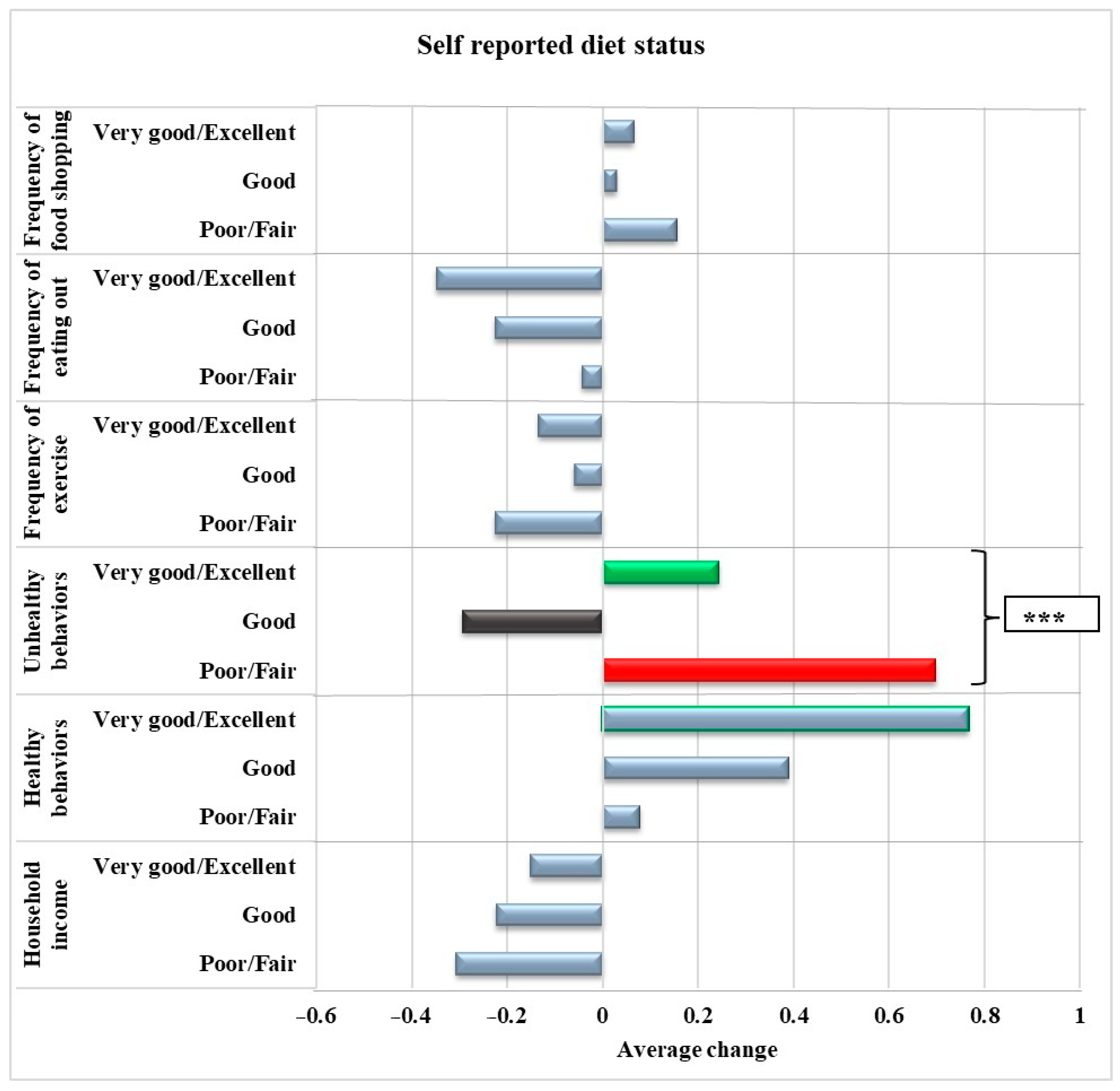
3.3. Association of FRM and Healthy Eating Focus with Self-Reported Changes in Health-Related Behaviors
3.4. Diet Quality and Risk of Overweight and Obesity, Hypertension, and Diabetes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Fanelli, S.M.; Jonnalagadda, S.S.; Pisegna, J.L.; Kelly, O.J.; Krok-Schoen, J.L.; Taylor, C.A. Poorer diet quality observed among US adults with a greater number of clinical chronic disease risk factors. J. Prim. Care Community Health 2020, 11, 2150132720945898. [Google Scholar] [CrossRef] [PubMed]
- Bartfeld, J.; Gundersen, C.; Smeeding, T.; Ziliak, J.P. SNAP Matters: How Food Stamps Affect Health and Well-Being; Stanford University Press: Palo Alto, CA, USA, 2015. [Google Scholar]
- Ratcliffe, C.; McKernan, S.-M.; Zhang, S. How much does the Supplemental Nutrition Assistance Program reduce food insecurity? Am. J. Agric. Econ. 2011, 93, 1082–1098. [Google Scholar] [CrossRef] [PubMed]
- Nord, M.; Golla, A.M. Does SNAP Decrease Food Insecurity? Untangling the Self-Selection Effect. Economic Research Report No. 85; U.S. Department of Agriculture, Economic Research Service, October 2009. [Google Scholar]
- Andreyeva, T.; Tripp, A.S.; Schwartz, M.B. Dietary quality of Americans by Supplemental Nutrition Assistance Program participation status: A systematic review. Am. J. Prev. Med. 2015, 49, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Edwards, C. SNAP: High Costs, Low Nutrition; Cato Institute: Washington, DC, USA, 2023. [Google Scholar]
- Spronk, I.; Kullen, C.; Burdon, C.; O‘Connor, H. Relationship between nutrition knowledge and dietary intake. Br. J. Nutr. 2014, 111, 1713–1726. [Google Scholar] [CrossRef] [PubMed]
- Yahia, N.; Brown, C.A.; Rapley, M.; Chung, M. Level of nutrition knowledge and its association with fat consumption among college students. BMC Public Health 2016, 16, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Glanz, K.; Brug, J.; Van Assema, P. Are awareness of dietary fat intake and actual fat consumption associated?—A Dutch--American Comparison. Eur. J. Clin. Nutr. 1997, 51, 542–547. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, V.K.; Johnston, E.A.; Firestone, M.J.; Stella, S.Y.; Beasley, J.M. Self-rated diet quality and cardiometabolic health among US adults, 2011–2018. Am. J. Prev. Med. 2021, 61, 563–575. [Google Scholar] [CrossRef]
- Wardlaw, M.K.; Hanula, G. EFNEP Behavior Checklist Review; US Department of Agriculture, National Institute of Food and Agriculture: Washington, DC, USA, 2012. Available online: https://nifa.usda.gov/sites/default/files/resource/Behavior%20Checklist%20Review.pdf (accessed on 21 June 2024).
- Kaiser, L.; Chaidez, V.; Algert, S.; Horowitz, M.; Martin, A.; Mendoza, C.; Neelon, M.; Ginsburg, D.C. Food resource management education with SNAP participation improves food security. J. Nutr. Educ. Behav. 2015, 47, 374–378.e371. [Google Scholar] [CrossRef] [PubMed]
- González-Monroy, C.; Gómez-Gómez, I.; Olarte-Sánchez, C.M.; Motrico, E. Eating behaviour changes during the COVID-19 pandemic: A systematic review of longitudinal studies. Int. J. Environ. Res. Public Health 2021, 18, 11130. [Google Scholar] [CrossRef]
- Picchioni, F.; Goulao, L.F.; Roberfroid, D. The impact of COVID-19 on diet quality, food security and nutrition in low and middle income countries: A systematic review of the evidence. Clin. Nutr. 2022, 41, 2955–2964. [Google Scholar] [CrossRef]
- Coleman-Jensen, A.; Rabbitt, M.P.; Gregory, C.A.; Singh, A. Household Food Security in the United States in 2019, ERR-275; U.S. Department of Agriculture, Economic Research Service: Washington, DC, USA, 2020.
- Fitzpatrick, K.M.; Harris, C.; Drawve, G.; Willis, D.E. Assessing Food Insecurity among US Adults during the COVID-19 Pandemic. J. Hunger. Environ. Nutr. 2020, 16, 1–16. [Google Scholar] [CrossRef]
- U.S. Census Bureau QuickFacts: Windham County, Connecticut. Available online: https://www.census.gov/quickfacts/fact/table/windhamcountyconnecticut/IPE120218 (accessed on 21 June 2024).
- U.S. Census Bureau QuickFacts: Willimantic CDP, Connecticut. Available online: https://www.census.gov/quickfacts/willimanticcdpconnecticut (accessed on 21 June 2024).
- Marmash, D.; Ha, K.; Sakaki, J.R.; Gorski, I.; Rule, B.; Foster, J.; Puglisi, M.; Chun, O.K. Diet quality, nutritional adequacy, and sociodemographic characteristics of mobile food pantry users in Northeastern connecticut. Nutrients 2021, 13, 1099. [Google Scholar] [CrossRef] [PubMed]
- Marmash, D.; Ha, K.; Sakaki, J.R.; Gorski, I.; Rule, B.; Puglisi, M.; Chun, O.K. The association between diet quality and health status in mobile food pantry users in Northeastern connecticut. Nutrients 2022, 14, 1302. [Google Scholar] [CrossRef] [PubMed]
- Economic Research Service, United States Department of Agriculture Food Access Research Atlas. Available online: https://www.ers.usda.gov/data-products/food-access-research-atlas/ (accessed on 21 June 2024).
- Avelino, D.C.; Duffy, V.B.; Puglisi, M.; Ray, S.; Lituma-Solis, B.; Nosal, B.M.; Madore, M.; Chun, O.K. Can Ordering Groceries Online Support Diet Quality in Adults Who Live in Low Food Access and Low-Income Environments? Nutrients 2023, 15, 862. [Google Scholar] [CrossRef] [PubMed]
- Stunkard, A.J.; Sørensen, T.; Schulsinger, F. Use of the Danish Adoption Register for the study of obesity and thinness. Res. Publ. Assoc. Res. Nerv. Ment Dis. 1983, 60, 115–120. [Google Scholar]
- Branstetter, S.A.; Muscat, J.E.; Mercincavage, M. Time to first cigarette: A potential clinical screening tool for nicotine dependence. J. Addict. Med. 2020, 14, 409. [Google Scholar] [CrossRef] [PubMed]
- King, A.C.; Powell, K.E.; Members of Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report; Office of the Assist ant Secretary for Health: Washington, DC, USA, 2018.
- Colby, S.; Zhou, W.; Allison, C.; Mathews, A.E.; Olfert, M.D.; Morrell, J.S.; Byrd-Bredbenner, C.; Greene, G.; Brown, O.; Kattelmann, K. Development and validation of the short healthy eating index survey with a college population to assess dietary quality and intake. Nutrients 2020, 12, 2611. [Google Scholar] [CrossRef]
- Sharafi, M.; Faghri, P.; Huedo-Medina, T.B.; Duffy, V.B. A simple liking survey captures behaviors associated with weight loss in a worksite program among women at risk of type 2 diabetes. Nutrients 2021, 13, 1338. [Google Scholar] [CrossRef] [PubMed]
- Sharafi, M.; Rawal, S.; Fernandez, M.L.; Huedo-Medina, T.B.; Duffy, V.B. Taste phenotype associates with cardiovascular disease risk factors via diet quality in multivariate modeling. Physiol. Behav. 2018, 194, 103–112. [Google Scholar] [CrossRef]
- Xu, R.; Blanchard, B.E.; McCaffrey, J.M.; Woolley, S.; Corso, L.M.; Duffy, V.B. Food liking-based diet quality indexes (dqi) generated by conceptual and machine learning explained variability in cardiometabolic risk factors in young adults. Nutrients 2020, 12, 882. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services and Department of Agriculture Dietary Guidelines for Americans, 2020–2025. 2022. Available online: https://www.dietaryguidelines.gov (accessed on 21 June 2024).
- Hubert, P.; Fiorenti, H.; Duffy, V. Development & Feasibility of an Online Tailored Messages Program to Motivate Healthier Diet & Physical Activity Behaviors in College Students. J. Acad. Nutr. Diet. 2021, 121, A124. [Google Scholar]
- Adjoian, T.K.; Firestone, M.J.; Eisenhower, D.; Stella, S.Y. Validation of self-rated overall diet quality by Healthy Eating Index-2010 score among New York City adults, 2013. Prev. Med. Pep. 2016, 3, 127–131. [Google Scholar] [CrossRef] [PubMed]
- Dubowitz, T.; Cohen, D.A.; Huang, C.Y.; Beckman, R.A.; Collins, R.L. Using a grocery list is associated with a healthier diet and lower BMI among very high-risk adults. J. Nutr. Educ. Behav. 2015, 47, 259–264.e251. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-Y.; Nayga, R.M., Jr.; Capps, O., Jr. The effect of food label use on nutrient intakes: An endogenous switching regression analysis. J. Agric. Resour. Econ. 2000, 25, 215–231. [Google Scholar]
- Ducrot, P.; Méjean, C.; Aroumougame, V.; Ibanez, G.; Allès, B.; Kesse-Guyot, E.; Hercberg, S.; Péneau, S. Meal planning is associated with food variety, diet quality and body weight status in a large sample of French adults. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 12. [Google Scholar] [CrossRef] [PubMed]
- Ozturk, E.E.; Ozgen, L. Association between nutrition label reading status and the healthy diet indicator-2015. J. Food Nutr. Res. 2021, 60, 263–270. [Google Scholar]
- Aggarwal, A.; Monsivais, P.; Cook, A.J.; Drewnowski, A. Positive attitude toward healthy eating predicts higher diet quality at all cost levels of supermarkets. J. Acad. Nutr. Diet. 2014, 114, 266–272. [Google Scholar] [CrossRef] [PubMed]
- Thompson, F.E.; Subar, A.F. Dietary assessment methodology. In Nutrition in the Prevention and Treatment of Disease; Academic Press: Cambridge, MA, USA, 2017; pp. 5–48. [Google Scholar]
- Pallister, T.; Sharafi, M.; Lachance, G.; Pirastu, N.; Mohney, R.P.; MacGregor, A.; Feskens, E.J.; Duffy, V.; Spector, T.D.; Menni, C. Food preference patterns in a UK twin cohort. Twin Res. Hum. Genet. 2015, 18, 793–805. [Google Scholar] [CrossRef]
- Zeigler, Z. COVID-19 self-quarantine and weight gain risk factors in adults. Curr. Obes. Rep. 2021, 10, 423–433. [Google Scholar] [CrossRef] [PubMed]
- Jalloun, R.A.; Youssef, M.H. Nutrition label use in relation to obesity among female college students at Taibah University. Majmaah J. Health Sci. 2020, 8, 77. [Google Scholar] [CrossRef]
- Loftfield, E.; Yi, S.; Immerwahr, S.; Eisenhower, D. Construct validity of a single-item, self-rated question of diet quality. J. Nutr. Educ. Behav. 2015, 47, 181–187. [Google Scholar] [CrossRef]
- Veríssimo, A.C.; Barbosa, M.C.A.; Almeida, N.A.V.; Queiroz, A.C.C.; Kelmann, R.G.; Silva, C.L.A. Association between the habit of reading food labels and health-related factors in elderly individuals of the community. Rev. Nutr. 2019, 32, e180207. [Google Scholar] [CrossRef]
- Gregory, C.; Smith, T.; Wendt, M. How Americans Rate Their Diet Quality: An Increasingly Realistic Perspective. Available online: http://www.ers.usda.gov/publications/pub-details/?pubid=44593 (accessed on 21 June 2024).
- Guenther, P.M.; Kirkpatrick, S.I.; Reedy, J.; Krebs-Smith, S.M.; Buckman, D.W.; Dodd, K.W.; Casavale, K.O.; Carroll, R.J. The Healthy Eating Index-2010 is a valid and reliable measure of diet quality according to the 2010 Dietary Guidelines for Americans. J. Nutr. 2014, 144, 399–407. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Survey Item | Item Range | Scores of Study Sample | |
|---|---|---|---|
| FRM skills | Mean ± SD | ||
| Plan meals | How often does your family eat evening meals together? | 1–6 1 | 4.57 ± 1.64 |
| Importance of reading nutrition labels | When you shop for food, how important is the nutrition label to you? For example, the amount of sodium or sugars. | 1–3 2 | 2.16 ± 0.65 |
| Compare prices | When you shop for food, how important is cost to you? | 1–3 2 | 2.66 ± 0.53 |
| Grocery list | When you shop for groceries, how often do you use a list? | 1–4 3 | 2.81 ± 1.03 |
| Run out of food | Within the past month, did the food you bought last and did you have money to buy more? | 1–3 4 | 2.36 ± 0.77 |
| Healthy eating focus | |||
| Healthy food | How concerned are you about how healthy your food is? | 1–3 5 | 2.07 ± 0.71 |
| Self-evaluated diet | How would you rate your overall diet quality? | 1–3 6 | 1.66 ± 0.70 |
| sHEI Tertile 1 | p-Value 2 | Liking-DQI Tertile 1 | p-Value 2 | |||||
|---|---|---|---|---|---|---|---|---|
| T1 (n = 87) | T2 (n = 88) | T3 (n = 88) | T1 (n = 90) | T2 (n = 90) | T3 (n = 90) | |||
| n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | |||
| Gender | <0.001 | 0.054 | ||||||
| Male | 29 (11) | 30 (11.4) | 7 (2.7) | 22 (8.2) | 30 (11.1) | 16 (5.9) | ||
| Female | 58 (22) | 58 (22.1) | 81 (30.8) | 68 (25.2) | 60 (22.2) | 74 (27.4) | ||
| Age | 0.28 | <0.001 | ||||||
| 19–39 | 61 (23.2) | 70 (26.6) | 58 (22.1) | 76 (28.2) | 66 (24.4) | 52 (19.3) | ||
| 40–49 | 21 (8.0) | 15 (5.7) | 22 (8.4) | 14 (5.2) | 18 (6.7) | 29 (10.7) | ||
| 60+ | 5 (1.9) | 3 (1.1) | 8 (3.0) | 0 (0) | 6 (2.2) | 9 (3.3) | ||
| Race/ ethnicity | 0.59 | 0.69 | ||||||
| White/Caucasian | 48 (18.3) | 45 (17.1) | 46 (17.5) | 48 (17.8) | 49 (18.1) | 45 (16.7) | ||
| Black/African American | 3 (1.1) | 9 (3.4) | 4 (1.5) | 2 (0.7) | 7 (2.6) | 7 (2.6) | ||
| Latino/Hispanic | 31 (11.8) | 31 (11.8) | 33 (12.6) | 35 (13.0) | 30 (11.1) | 34 (12.6) | ||
| Others 3 | 5 (1.9) | 3 (1.1) | 5 (1.9) | 5 (1.8) | 4 (1.5) | 4 (1.5) | ||
| Primary Language | 0.76 | <0.05 | ||||||
| English | 78 (29.7) | 77 (29.3) | 80 (30.4) | 87 (32.2) | 79 (29.3) | 77 (28.5) | ||
| Non-English | 9 (3.4) | 11 (4.2) | 7 (3) | 3 (1.1) | 11 (4.1) | 13 (4.8) | ||
| Education | 0.06 | 0.22 | ||||||
| ≤8th grade/Some High School | 8 (3.1) | 15 (5.7) | 5 (1.9) | 8 (3.0) | 13 (4.8) | 9 (3.3) | ||
| H.S. graduate/ GED | 28 (10.6) | 22 (8.4) | 20 (7.6) | 32 (11.8) | 21 (7.8) | 18 (6.7) | ||
| Some college or technical | 30 (11.4) | 31 (11.8) | 29 (11) | 25 (9.3) | 33 (12.2) | 34 (12.6) | ||
| Graduate/ professional degree | 21 (8.0) | 20 (7.6) | 34 (12.9) | 25 (9.3) | 23 (8.5) | 29 (10.7) | ||
| Employment | 0.77 | 0.35 | ||||||
| Full-time employment | 44 (16.7) | 42 (16.0) | 39 (14.8) | 42 (15.5) | 49 (18.1) | 39 (14.4) | ||
| Part-time employment | 13 (4.9) | 20 (7.6) | 18 (6.9) | 20 (7.4) | 18(6.7) | 13 (4.8) | ||
| Unemployed, active seeking | 12 (4.6) | 10 (3.8) | 9 (3.4) | 10 (3.7) | 8 (3.0) | 14 (5.2) | ||
| Unemployed, not seeking | 18 (6.8) | 16 (6.1) | 22 (8.4) | 18 (6.7) | 15 (5.6) | 24 (8.9) | ||
| Cigarette smoking | <0.05 | 0.18 | ||||||
| Current (inc. e-cigarettes) | 21 (8) | 29 (11) | 13 (4.9) | 27 (10) | 23 (8.5) | 16 (5.9) | ||
| Former | 10 (3.8) | 16 (6.1) | 16 (6.1) | 11 (4.1) | 12 (4.4) | 20 (7.4) | ||
| Never | 56 (21.3) | 43 (16.4) | 59 (22.4) | 52 (19.3) | 55 (20.4) | 54 (20) | ||
| Physical activity/week | <0.05 | <0.05 | ||||||
| <150 min | 82 (31.2) | 72 (27.4) | 71 (27) | 79 (29.3) | 82 (30.4) | 69 (25.5) | ||
| ≥150 min | 5 (1.9) | 16 (6.1) | 17 (6.4) | 11 (4.1) | 8 (2.9) | 21 (7.8) | ||
| Overweight and obesity | <0.05 | 0.76 | ||||||
| Yes | 69 (26.3) | 64 (24.4) | 53 (20.2) | 60 (22.3) | 65 (24.1) | 64 (23.8) | ||
| No | 17 (6.5) | 24 (9.2) | 35 (13.4) | 29 (10.8) | 25 (9.3) | 26 (9.7) | ||
| Diabetes | 0.28 | 0.07 | ||||||
| Yes | 11 (4.2) | 8 (3) | 5 (1.9) | 5 (1.9) | 13 (4.8) | 6 (2.2) | ||
| No | 76 (28.9) | 80 (30.4) | 83 (31.6) | 85 (31.5) | 77 (28.5) | 84 (31.1) | ||
| Hypertension | 0.19 | 0.22 | ||||||
| Yes | 23 (8.8) | 16 (6.1) | 14 (5.3) | 16 (5.9) | 22 (8.2) | 13 (4.8) | ||
| No | 64 (24.3) | 72 (27.4) | 74 (28.1) | 74 (27.4) | 68 (25.2) | 77 (28.5) | ||
| FRM Skills and Healthy Eating Focus | sHEI (n = 263) | Liking-DQI (n = 270) | ||
|---|---|---|---|---|
| Crude | Adjusted 2 | Crude | Adjusted 2 | |
| Mean ± SD | Mean ± SE | Mean ± SD | Mean ± SE | |
| Plan meals | ||||
| Never | 39.27 ± 9.52 | 40.91 ± 2.49 | −21.35 ± 31.65 | −16.82 ± 8.09 |
| Occasionally/monthly | 51.13 ± 6.34 | 52.27 ± 2.02 | −1.36 ± 34.42 | 4.94 ± 7.60 |
| Couple of times per month | 47.80 ± 8.90 | 49.08 ± 2.10 | −3.95± 33.01 | 1.65 ± 7.23 |
| Weekly | 49.41 ± 7.65 | 52.16 ± 1.83 | −15.62 ± 32.94 | −5.11 ± 6.53 |
| Couple of times per week | 48.43± 9.83 | 49.68 ± 1.57 | −4.42 ± 34.41 | −1.49 ± 5.67 |
| Usually/always | 52.11 ± 10.05 | 53.50 ± 1.27 | 5.63 ± 32.53 | 10.80 ± 4.54 |
| p-value 1 | <0.001 | <0.001 | <0.01 | <0.01 |
| Importance of reading nutrition labels | ||||
| Not important | 41.72 ± 10.27 | 43.80 ± 1.85 | −21.43 ± 34.90 | −14.21 ± 6.28 |
| Somewhat important | 50.10 ± 8.83 | 51.46 ± 1.13 | −1.62 ± 33.15 | 2.97 ± 4.08 |
| Very important | 52.50 ± 9.52 | 54.34 ± 1.41 | 4.88 ± 32.00 | 11.28 ± 5.01 |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 |
| Compare prices | ||||
| Not important | 51.34 ± 8.65 | 54.83 ± 4.38 | −28.71 ± 22.54 | −13.27 ± 13.20 |
| Somewhat important | 51.12 ± 9.65 | 52.54 ± 1.33 | −4.70± 36.64 | 0.50 ± 4.67 |
| Very important | 49.19 ± 9.82 | 50.57 ± 1.28 | −0.63 ± 32.85 | 5.72 ± 4.42 |
| p-value | 0.33 | 0.22 | 0.08 | 0.20 |
| Grocery List | ||||
| Never | 46.38 ± 11.00 | 48.52 ± 1.90 | −12.60 ± 40.63 | −5.95 ± 6.54 |
| Occasionally | 47.50 ± 8.53 | 49.52 ± 1.38 | −9.64 ± 32.57 | −1.90 ± 4.91 |
| Sometimes | 52.16 ± 9.04 | 54.33 ± 1.48 | −4.40 ± 33.38 | 5.54 ± 5.09 |
| Usually/always | 51.24 ± 10.20 | 52.91 ± 1.47 | 8.18 ± 30.57 | 13.22 ± 5.16 |
| p-value | <0.01 | <0.01 | <0.01 | <0.01 |
| Run out of food | ||||
| Often | 50.11 ± 11.02 | 51.07 ± 2.06 | 0.30 ± 31.53 | 5.80 ± 6.92 |
| Sometimes | 49.91 ± 8.90 | 51.79 ± 1.42 | −3.75 ± 31.70 | 4.00 ± 4.92 |
| Never | 49.81± 9.96 | 51.27 ± 1.24 | −2.59 ± 36.24 | 1.56 ± 4.42 |
| p-value | 0.99 | 0.90 | 0.85 | 0.76 |
| Healthy Food | ||||
| Not at all concerned/not too concerned | 46.19 ± 9.73 | 48.08 ± 1.44 | −14.57 ± 30.49 | −7.95 ± 4.86 |
| Somewhat concerned | 49.31 ± 9.48 | 51.45 ± 1.32 | −6.27 ± 34.93 | 1.34 ± 4.59 |
| Very concerned | 53.17 ± 9.28 | 55.43 ± 1.42 | 13.30 ± 29.13 | 19.63 ± 4.93 |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 |
| Self-evaluated diet | ||||
| Poor/fair | 45.48 ± 9.53 | 45.71 ± 1.31 | −11.81 ± 35.07 | −7.84 ± 4.77 |
| Good | 53.44 ± 8.37 | 53.62 ± 1.15 | 5.54 ± 32.23 | 7.31 ± 4.32 |
| Very good/Excellent | 54.03 ± 8.16 | 54.21 ± 1.67 | 6.40 ± 26.46 | 10.99 ± 6.22 |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 |
| sHEI | p-Trend | |||
|---|---|---|---|---|
| T1 (n = 87) | T2 (n = 88) | T3 (n = 88) | ||
| Overweight and obesity | ||||
| Unadjusted | 1.00 | 0.66 (0.32–1.33) | 0.37 (0.19–0.74) | <0.01 |
| Adjusted 3 | 1.00 | 0.71 (0.34–1.49) | 0.37 (0.18–0.76) | <0.01 |
| Hypertension | ||||
| Unadjusted | 1.00 | 0.62 (0.30–1.27) | 0.53 (0.25–1.11) | 0.08 |
| Adjusted | 1.00 | 0.80 (0.36–1.77) | 0.61 (0.26–1.39) | 0.24 |
| Diabetes | ||||
| Unadjusted | 1.00 | 0.69 (0.26–1.81) | 0.42 (0.14–1.25) | 0.11 |
| Adjusted | 1.00 | 1.05 (0.37–3.03) | 0.38 (0.12–1.26) | 0.13 |
| Liking-DQI | p-trend | |||
| T1 (n = 90) | T2 (n = 90) | T3 (n = 90) | ||
| Overweight and obesity | ||||
| Unadjusted | 1.00 | 1.26 (0.66–2.38) | 1.19 (0.63–2.25) | 0.59 |
| Adjusted | 1.00 | 1.04 (0.54–2.03) | 1.12 (0.56–2.24) | 0.74 |
| Hypertension | ||||
| Unadjusted | 1.00 | 1.50 (0.73–3.08) | 0.78 (0.35–1.73) | 0.57 |
| Adjusted | 1.00 | 1.16 (0.53–2.54) | 0.52 (0.21–1.31) | 0.18 |
| Diabetes | ||||
| Unadjusted | 1.00 | 2.87 (0.98–8.42) | 1.21 (0.36–4.13) | 0.79 |
| Adjusted | 1.00 | 2.52 (0.82–7.77) | 0.82 (0.22–3.12) | 0.74 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Darooghegi Mofrad, M.; Nosal, B.M.; Avelino, D.C.; Killion, K.; Puglisi, M.; Duffy, V.B.; Chun, O.K. Food Resource Management and Healthy Eating Focus Associates with Diet Quality and Health Behaviors in Low-Income Adults. Nutrients 2024, 16, 2043. https://doi.org/10.3390/nu16132043
Darooghegi Mofrad M, Nosal BM, Avelino DC, Killion K, Puglisi M, Duffy VB, Chun OK. Food Resource Management and Healthy Eating Focus Associates with Diet Quality and Health Behaviors in Low-Income Adults. Nutrients. 2024; 16(13):2043. https://doi.org/10.3390/nu16132043
Chicago/Turabian StyleDarooghegi Mofrad, Manije, Briana M. Nosal, Daniela C. Avelino, Kate Killion, Michael Puglisi, Valerie B. Duffy, and Ock K. Chun. 2024. "Food Resource Management and Healthy Eating Focus Associates with Diet Quality and Health Behaviors in Low-Income Adults" Nutrients 16, no. 13: 2043. https://doi.org/10.3390/nu16132043
APA StyleDarooghegi Mofrad, M., Nosal, B. M., Avelino, D. C., Killion, K., Puglisi, M., Duffy, V. B., & Chun, O. K. (2024). Food Resource Management and Healthy Eating Focus Associates with Diet Quality and Health Behaviors in Low-Income Adults. Nutrients, 16(13), 2043. https://doi.org/10.3390/nu16132043