
Vitamin D, the Sunshine Molecule That Makes Us Strong: What Does Its Current Global Deficiency Imply?


Abstract
1. Introduction
2. Vitamin D
2.1. Vitamin D, the Sunshine Molecule That Makes Us Strong
2.2. The Vitamin D Receptor (VDR)
2.3. The Characters in This Story
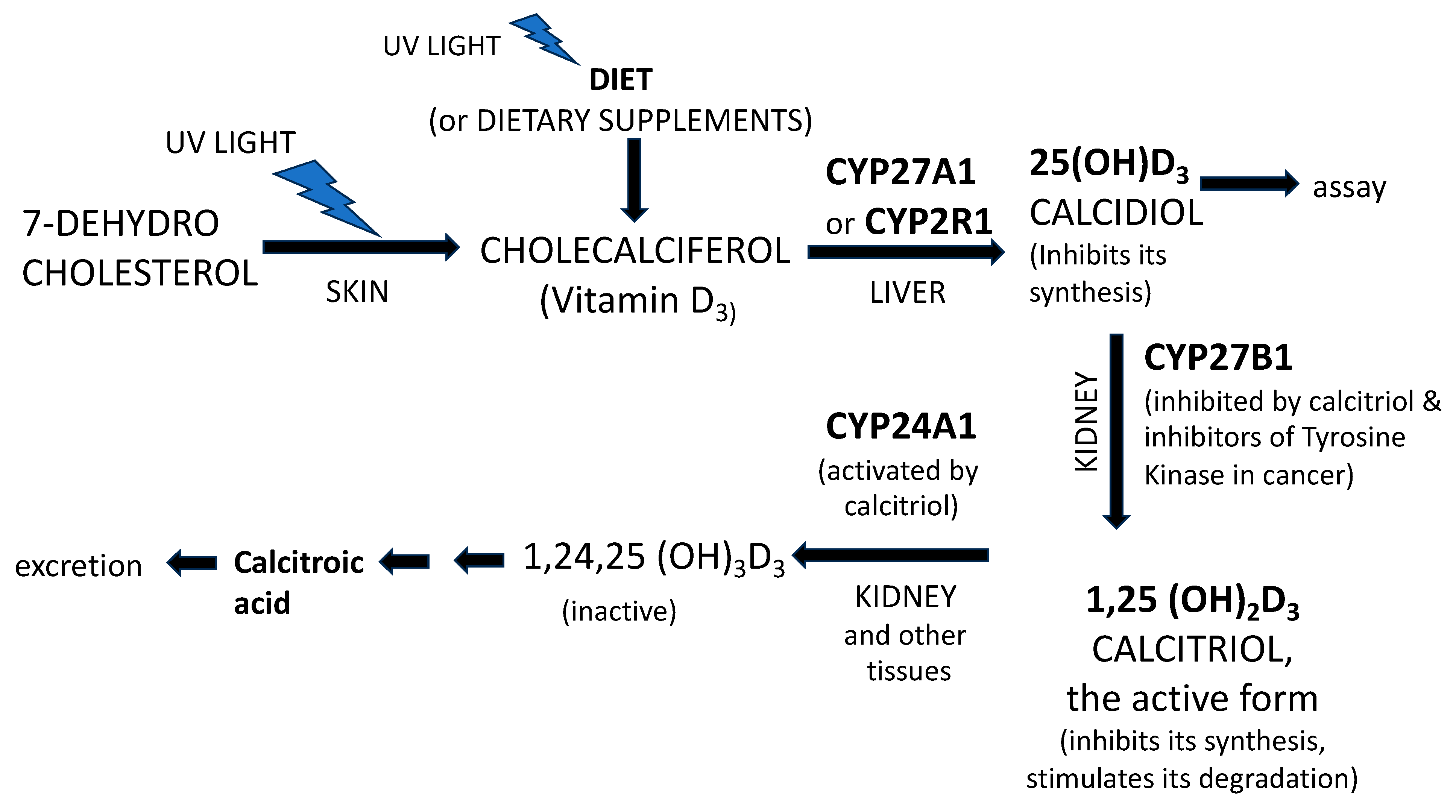
2.4. Vitamin D3 Metabolism [5]
2.5. Vitamin D—Why It Is Present in Plants and Invertebrates
2.6. Assessment of Vitamin D and Reference Ranges
2.7. Administration of Vitamin D
2.8. Vitamin D in Pregnancy
2.9. Low Levels of Vitamin D Could Be a Marker of Potential Predisposition to Multifactorial Chronic Inflammatory Diseases
2.10. What to Do in the Future to Counteract the Prevalence of Vitamin D Deficiency and Insufficiency: Some Suggestions
3. Discussion
Doubts and Contradictions Regarding Vitamin D
4. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Cui, A.; Zhang, T.; Xiao, P.; Fan, Z.; Wang, H.; Zhuang, Y. Global and regional prevalence of vitamin D deficiency in population-based studies from 2000 to 2022: A pooled analysis of 7.9 million participants. Front. Nutr. 2023, 10, 1070808. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. The vitamin D deficiency pandemic: Approaches for diagnosis, treatment and prevention. Rev. Endocr. Metab. Disord. 2017, 18, 153–165. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. The One-Hundred-Year Anniversary of the Discovery of the Sunshine Vitamin D3: Historical, Personal Experience and Evidence-Based Perspectives. Nutrients 2023, 15, 593. [Google Scholar] [CrossRef] [PubMed]
- Deluca, H.F. History of the discovery of vitamin D and its active metabolites. BoneKEy Rep. 2014, 3, 479. [Google Scholar] [CrossRef] [PubMed]
- Christakos, S.; Dhawan, P.; Verstuyf, A.; Verlinden, L.; Carmeliet, G. Vitamin D: Metabolism, Molecular Mechanism of Action, and Pleiotropic Effects. Physiol. Rev. 2016, 96, 365–408. [Google Scholar] [CrossRef] [PubMed]
- Bouillon, R.; Marcocci, C.; Carmeliet, G.; Bikle, D.; White, J.H.; Dawson-Hughes, B.; Lips, P.; Munns, C.F.; Lazaretti-Castro, M.; Giustina, A.; et al. Skeletal and Extraskeletal Actions of Vitamin D: Current Evidence and Outstanding Questions. Endocr. Rev. 2019, 40, 1109–1151. [Google Scholar] [CrossRef]
- Carlberg, C. A Pleiotropic Nuclear Hormone Labelled Hundred Years Ago Vitamin D. Nutrients 2022, 15, 171. [Google Scholar] [CrossRef]
- Bouillon, R.; Carmeliet, G.; Verlinden, L.; van Etten, E.; Verstuyf, A.; Luderer, H.F.; Lieben, L.; Mathieu, C.; Demay, M. Vitamin D and human health: Lessons from vitamin D receptor null mice. Endocr. Rev. 2008, 29, 726–776. [Google Scholar] [CrossRef]
- Medeiros, J.F.P.; de Oliveira Borges, M.V.; Soares, A.A.; Dos Santos, J.C.; de Oliveira, A.B.B.; da Costa, C.H.B.; Cruz, M.S.; Bortolin, R.H.; de Freitas, R.C.C.; Dantas, P.M.S.; et al. The impact of vitamin D supplementation on VDR gene expression and body composition in monozygotic twins: Randomized controlled trial. Sci. Rep. 2020, 10, 11943. [Google Scholar] [CrossRef] [PubMed]
- Vieth, R. Vitamin D supplementation: Cholecalciferol, calcifediol, and calcitriol. Eur. J. Clin. Nutr. 2020, 74, 1493–1497. [Google Scholar] [CrossRef]
- Li, Y.; Yang, C.; Ahmad, H.; Maher, M.; Fang, C.; Luo, J. Benefiting others and self: Production of vitamins in plants. J. Integr. Plant Biol. 2021, 63, 210–227. [Google Scholar] [CrossRef] [PubMed]
- Black, L.J.; Lucas, R.M.; Sherriff, J.L.; Björn, L.O.; Bornman, J.F. In Pursuit of Vitamin D in Plants. Nutrients 2017, 9, 136. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jäpelt, R.B.; Jakobsen, J. Vitamin D in plants: A review of occurrence, analysis, and biosynthesis. Front. Plant Sci. 2013, 4, 136. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dodd, A.N.; Kudla, J.; Sanders, D. The language of calcium signaling. Ann. Rev. Plant Biol. 2010, 6, 593–620. [Google Scholar] [CrossRef] [PubMed]
- Oonincx DG, A.B.; Van Keulen, P.; Finke, M.D.; Baines, F.M.; Vermeulen, M.; Bosch, G. Vermeulen & G. Bosch Evidence of vitamin D synthesis in insects exposed to UVb light. Sci. Rep. 2018, 8, 10807. [Google Scholar] [CrossRef] [PubMed]
- Cantorna, M.T.; Mahon, B.D. Mounting evidence for vitamin D as an environmental factor affecting autoimmune disease prevalence. Exp. Biol. Med. 2004, 229, 1136–1142. [Google Scholar] [CrossRef]
- Kimball, S.M.; Holick, M.F. Official recommendations for Vitamin D through the life stages in developed countries. Eur. J. Clin. Nutr. 2020, 74, 1514–1518. [Google Scholar] [CrossRef] [PubMed]
- Khazai, N.; Judd, S.E.; Tangpricha, V. Calcium and vitamin D: Skeletal and extraskeletal health. Curr. Rheumatol. Rep. 2008, 10, 110–117. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Amon, U.; Yaguboglu, R.; Ennis, M.; Holick, M.F.; Amon, J. Safety Data in Patients with Autoimmune Diseases during Treatment with High Doses of Vitamin D3 According to the “Coimbra Protocol”. Nutrients 2022, 14, 1575. [Google Scholar] [CrossRef] [PubMed]
- Grant, W.B.; Al Anouti, F.; Moukayed, M. Targeted 25-hydroxyvitamin D concentration measurements and vitamin D3 supplementation can have important patient and public health benefits. Eur. J. Clin. Nutr. 2020, 74, 366–376. [Google Scholar] [CrossRef]
- Yuan, Y.; Tai, W.; Xu, P.; Fu, Z.; Wang, X.; Long, W.; Guo, X.; Ji, C.; Zhang, L.; Zhang, Y. Association of maternal serum 25-hydroxyvitamin D concentrations with risk of preeclampsia: A nested case-control study and meta-analysis. J. Matern. Fetal Neonatal Med. 2021, 34, 1576–1585. [Google Scholar] [CrossRef] [PubMed]
- McDonnell, S.L.; Baggerly, K.A.; Baggerly, C.A.; Aliano, J.L.; French, C.B.; Baggerly, L.L.; Ebeling, M.D.; Rittenberg, C.S.; Goodier, C.G.; Mateus Niño, J.F.; et al. Maternal 25(OH)D concentrations ≥ 40 ng/mL associated with 60% lower preterm birth risk among general obstetrical patients at an urban medical center. PLoS ONE 2017, 12, e0180483. [Google Scholar] [CrossRef] [PubMed]
- García-Serna, A.M.; Morales, E. Neurodevelopmental effects of prenatal vitamin D in humans: Systematic review and meta-analysis. Mol. Psychiatry 2020, 25, 2468–2481. [Google Scholar] [CrossRef]
- GBD 2021 Risk Factors Collaborators. Global burden and strength of evidence for 88 risk factors in 204 countries and 811 subnational locations, 1990–2021: A systematic analysis for the Global Burden of Disease Study 2021. Lancet 2024, 403, 2162–2203. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Riccio, P.; Rossano, R. Diet, Gut Microbiota, and Vitamins D + A in Multiple Sclerosis. Neurotherapeutics 2018, 15, 75–91. [Google Scholar] [CrossRef]
- Ellison, D.L.; Moran, H.R. Vitamin D: Vitamin or Hormone? Nurs. Clin. N. Am. 2021, 56, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Muscogiuri, G. Introduction to Vitamin D: Current evidence and future directions. Eur. J. Clin. Nutr. 2020, 74, 1491–1492. [Google Scholar] [CrossRef]
- Ruggiero, C.; Tafaro, L.; Cianferotti, L.; Tramontana, F.; Macchione, I.G.; Caffarelli, C.; Virdis, A.; Ferracci, M.; Rinonapoli, G.; Mecocci, P.; et al. Targeting the Hallmarks of Aging with Vitamin D: Starting to Decode the Myth. Nutrients 2024, 16, 906. [Google Scholar] [CrossRef]
- Bellan, M.; Andreoli, L.; Mele, C.; Sainaghi, P.P.; Rigamonti, C.; Piantoni, S.; De Benedittis, C.; Aimaretti, G.; Pirisi, M.; Marzullo, P. Pathophysiological Role and Therapeutic Implications of Vitamin D in Autoimmunity: Focus on Chronic Autoimmune Diseases. Nutrients 2020, 12, 789. [Google Scholar] [CrossRef]
- Riccio, P.; Rossano, R.; Larocca, M.; Trotta, V.; Mennella, I.; Vitaglione, P.; Ettorre, M.; Graverini, A.; De Santis, A.; Di Monte, E.; et al. Anti-inflammatory nutritional intervention in patients with relapsing-remitting and primary-progressive multiple sclerosis: A pilot study. Exp. Biol. Med. 2016, 241, 620–635. [Google Scholar] [CrossRef]
- Amrein, K.; Scherkl, M.; Hoffmann, M.; Neuwersch-Sommeregger, S.; Köstenberger, M.; Tmava Berisha, A.; Martucci, G.; Pilz, S.; Malle, O. Vitamin D deficiency 2.0: An update on the current status worldwide. Eur. J. Clin. Nutr. 2020, 74, 1498–1513. [Google Scholar] [CrossRef] [PubMed]
- Pugach, I.Z.; Pugach, S. Strong correlation between prevalence of severe vitamin D deficiency and population mortality rate from COVID-19 in Europe. Wien. Klin. Wochenschr. 2021, 133, 403–405. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
{kind=link}
| PUBMED Search | Results (No Filters) (A) | Results 1983–2003 (B) | Results 2004–2024 (C) | Fold Increase 2004–2024/ 1983–2003 |
|---|---|---|---|---|
| Section 1 | ||||
| 1.1. Vitamin D deficiency & Rickets | 15,288 | 4006 | 4809 | 1.2 |
| 1.2. Vitamin D deficiency & chronic inflammatory diseases | 462 | 22 | 440 | 20.0 |
| 1.3. Vitamin D deficiency & cardiovascular disease | 3291 | 165 | 2905 | 17.6 |
| 1.4. Vitamin D deficiency & cancer | 4035 | 452 | 3215 | 7.1 |
| Section 2 | ||||
| 2.1. Vitamin D deficiency prevalence rate | 45 | 1072 | 23.8 | |
| 2.2. Rickets prevalence rate | 44 | 122 | 2.8 | |
| 2.3. Chronic Inflammatory Diseases prevalence rate | 288 | 2281 | 7.9 | |
| 2.4. Cardiovascular disease prevalence rate | 27,267 | 94,337 | 3.5 | |
| 2.5. Cancer prevalence rate | 47,470 | 135,244 | 2.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riccio, P. Vitamin D, the Sunshine Molecule That Makes Us Strong: What Does Its Current Global Deficiency Imply? Nutrients 2024, 16, 2015. https://doi.org/10.3390/nu16132015
Riccio P. Vitamin D, the Sunshine Molecule That Makes Us Strong: What Does Its Current Global Deficiency Imply? Nutrients. 2024; 16(13):2015. https://doi.org/10.3390/nu16132015
Chicago/Turabian StyleRiccio, Paolo. 2024. "Vitamin D, the Sunshine Molecule That Makes Us Strong: What Does Its Current Global Deficiency Imply?" Nutrients 16, no. 13: 2015. https://doi.org/10.3390/nu16132015
APA StyleRiccio, P. (2024). Vitamin D, the Sunshine Molecule That Makes Us Strong: What Does Its Current Global Deficiency Imply? Nutrients, 16(13), 2015. https://doi.org/10.3390/nu16132015