

Selenium Intake and Postnatal Depression—A Short Review

 ,
,  , , and
, , and
Abstract
1. Introduction
2. Methods
3. Selenium Intake and Its Effects on Maternal Mental Health Outcomes Postpartum

| Study Design | Country | Sample Size | Study Population | Se Dose/Intake | Depression Assessment Method | Selenium-Related Outcome | Ref. |
|---|---|---|---|---|---|---|---|
| Randomised, double-blind, placebo-controlled study | Iran | n = 85 Selenium group n = 44 Placebo group n = 41 | Women aged 16–35 years, primigravid, with gestational age up to 12 weeks. Mean age (±SD)— Selenium group: 21.64 (±2.45) Placebo group: 21.59 (±3.40) | 100 μg/day (administered as selenium yeast tablets from the first trimester until birth) | EPDS Collected within 8 weeks of delivery. | Selenium supplementation was associated with a significant increase in mean serum selenium concentration at term (p < 0.001). Serum selenium concentration remained statistically unchanged by the end of the trial in the control group (p > 0.05). The mean EPDS score in the selenium group was significantly lower than that in the control (placebo) group—8.8 ± 5.1 vs. 10.7 ± 4.4, respectively (p < 0.05). | [61] |
| Cohort study | Canada | n = 475 | Pregnant women aged 16 years and older, with gestational age ≤27 weeks. Mean age (95% CI) — Women with postpartum EPDS score < 10 (n = 416): 31.2 (30.8–31.6) Women with postpartum EPDS score ≥ 10 (n = 59): 31.6 (30.3–32.8) | Mean maternal selenium intake from supplementation (±SD) — Women with postpartum EPDS score < 10 (n = 416): 25 (±17) μg/day Women with postpartum EPDS score ≥ 10 (n = 59): 19 (±13) μg/day | EPDS Collected at each trimester and 12 weeks postpartum. | The mean supplementary intake of selenium was significantly higher in women with EPDS < 10 than in those with EPDS ≥ 10; (p = 0.0015). Selenium intake from supplements was negatively associated with postpartum depressive symptoms. | [62] |
| Case–control study | Iran | n = 163 Case group: n = 81 (women diagnosed with postpartum depression, PPD) Control group: n = 82 (non-PPD) | Women aged 18 to 45 years in postpartum period. Mean age (±SD)— Case group: 28.4 (± 6.7) Control group: 27.2 (± 5.6) | Median dietary maternal selenium intake assessed using semi-quantitative food frequency questionnaire; adjusted for total energy intake. Case group: 6.5 μg/day Control group: 23.7 μg/day | EPDS Case group included women with EPDS scores > 12 during period from 1 month to 6 months postpartum. | Dietary intake of selenium was significantly lower in the PPD group than in the non-PPD control (p < 0.001). Higher intake of selenium was associated with reduced odds of post-partum depression. | [63] |
| Cohort study | New Zealand | n = 87 | Breastfeeding women aged 16 years and older at 3 months postpartum. Mean age (±SD)— 31.5 ± 4.2 | Median maternal selenium intake estimated from weighed four-day diet diary (including supplements)—62 μg/day. Note: 5 out of 87 women were supplemented with selenium, ranging from 25 to 65 μg/day. | EPDS Collected at 3, 6, and 12 months postpartum. | No significant association between plasma selenium values and EPDS scores was observed. | [64] |
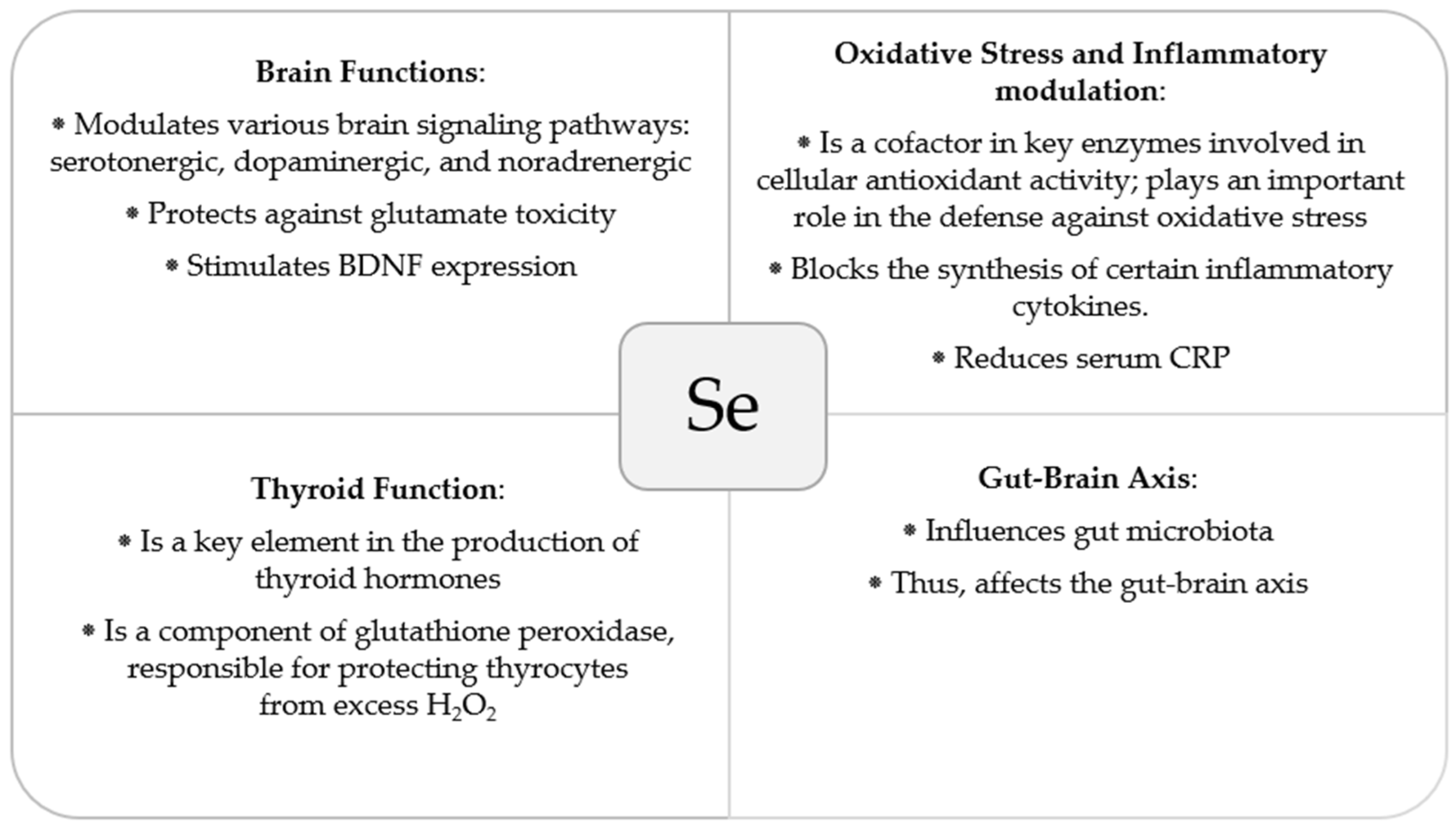
4. Biological Mechanisms That Might Underlie Selenium’s Effects in Postanal Depression
5. Limitations
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Woody, C.A.; Ferrari, A.J.; Siskind, D.J.; Whiteford, H.A.; Harris, M.G. A systematic review and meta-regression of the prevalence and incidence of perinatal depression. J. Affect. Disord. 2017, 219, 86–92. [Google Scholar] [CrossRef]
- Wang, Z.; Liu, J.; Shuai, H.; Cai, Z.; Fu, X.; Liu, Y.; Xiao, X.; Zhang, W.; Krabbendam, E.; Liu, S.; et al. Mapping global prevalence of depression among postpartum women. Transl. Psychiatry 2021, 11, 543. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; Text Revision; American Psychiatric Association: Arlington, VA, USA, 2022; Available online: https://psychiatryonline.org/doi/book/10.1176/appi.books.9780890425787 (accessed on 5 June 2024).
- World Health Organization. International Statistical Classification of Diseases and Related Health Problems, 11th ed.; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Gaynes, B.N.; Gavin, N.; Meltzer-Brody, S.; Lohr, K.N.; Swinson, T.; Gartlehner, G.; Brody, S.; Miller, W.C. 119 Perinatal Depression: Prevalence, Screening Accuracy, and Screening Outcomes: Summary. In AHRQ Evidence Report Summaries; Agency for Healthcare Research and Quality (US): Rockville, MD, USA, 2005; pp. 1–8. [Google Scholar]
- Gelaye, B.; Rondon, M.B.; Araya, R.; Williams, M.A. Epidemiology of Maternal Depression, Risk Factors, and Child Outcomes in Low-Income and Middle-Income Countries. Lancet Psychiatry 2016, 3, 973–982. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.T.S.; Chung, T.K.H. Postnatal Depression: An Update. Best Pract. Res. Clin. Obstet. Gynaecol. 2007, 21, 183–191. [Google Scholar] [CrossRef] [PubMed]
- Craig, M.; Howard, L. Postnatal depression. BMJ Clin. Evid. 2009, 2009, 1407. [Google Scholar] [PubMed]
- Stein, A.; Lehtonen, A.; Harvey, A.G.; Nicol-Harper, R.; Craske, M. The Influence of Postnatal Psychiatric Disorder on Child Development. Is Maternal Preoccupation One of the Key Underlying Processes? Psychopathology 2009, 42, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.J.; La Porte, L.M.; Saleh, M.P.; Allweiss, S.; Adams, M.G.; Zhou, Y.; Silver, R.K. Suicide risk among perinatal women who report thoughts of self-harm on depression screens. Obstet. Gynecol. 2015, 125, 885–893. [Google Scholar] [CrossRef] [PubMed]
- Payne, J.L.; Maguire, J. Pathophysiological mechanisms implicated in postpartum depression. Front. Neuroendocrinol. 2019, 52, 165–180. [Google Scholar] [CrossRef]
- Alamolhoda, S.H.; Kariman, N.; Mirabi, P. Relationship Between Oxidative Stress Concentration and Postpartum Depression: A Cohort Study. Iran. J. Psychiatry Behav. Sci. 2020, 14, e84188. [Google Scholar] [CrossRef]
- EFSA NDA Panel (EFSA Panel on Nutrition, Novel Foods and Food Allergens); Turck, D.; Bohn, T.; Castenmiller, J.; de Henauw, S.; Hirsch-Ernst, K.I.; Knutsen, H.K.; Maciuk, A.; Mangelsdorf, I.; McArdle, H.J.; et al. Scientific Opinion on the Tolerable Upper Intake Level for Selenium. EFSA J. 2023, 21, 7704. [Google Scholar] [CrossRef]
- Kurokawa, S.; Berry, M.J. Selenium. Role of the essential metalloid in health. Met. Ions Life Sci. 2013, 13, 499–534. [Google Scholar] [CrossRef]
- Kang, D.; Lee, J.; Wu, C.; Guo, X.; Lee, B.J.; Chun, J.S.; Kim, J.H. The role of selenium metabolism and selenoproteins in cartilage homeostasis and arthropathies. Exp. Mol. Med. 2020, 52, 1198–1208. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Roman, M.; Jitaru, P.; Barbante, C. Selenium biochemistry and its role for human health. Metallomics 2014, 6, 25–54. [Google Scholar] [CrossRef]
- Nakayama, A.; Hill, K.E.; Austin, L.M.; Motley, A.K.; Burk, R.F. All regions of mouse brain are dependent on selenoprotein P for maintenance of selenium. J. Nutr. 2007, 137, 690–693. [Google Scholar] [CrossRef]
- Ferreira, R.L.U.; Sena-Evangelista, K.C.M.; de Azevedo, E.P.; Pinheiro, F.I.; Cobucci, R.N.; Pedrosa, L.F.C. Selenium in Human Health and Gut Microflora: Bioavailability of Selenocompounds and Relationship with Diseases. Front. Nutr. 2021, 8, 685317. [Google Scholar] [CrossRef]
- Minich, W.B. Selenium Metabolism and Biosynthesis of Selenoproteins in the Human Body. Biochemistry 2022, 87 (Suppl. S1), S168–S177. [Google Scholar] [CrossRef]
- Labunskyy, V.M.; Hatfield, D.L.; Gladyshev, V.N. Selenoproteins: Molecular pathways and physiological roles. Physiol. Rev. 2014, 94, 739–777. [Google Scholar] [CrossRef]
- Rehman, A.; John, P.; Bhatti, A. Biogenic Selenium Nanoparticles: Potential Solution to Oxidative Stress Mediated Inflammation in Rheumatoid Arthritis and Associated Complications. Nanomaterials 2021, 11, 2005. [Google Scholar] [CrossRef]
- Bera, S.; De Rosa, V.; Rachidi, W.; Diamond, A.M. Does a role for selenium in DNA damage repair explain apparent controversies in its use in chemoprevention? Mutagenesis 2013, 28, 127–134. [Google Scholar] [CrossRef]
- Zeng, H. Selenium as an essential micronutrient: Roles in cell cycle and apoptosis. Molecules 2009, 14, 1263–1278. [Google Scholar] [CrossRef]
- Zeng, H. Selenium and the Regulation of Cell Cycle and Apoptosis. In Encyclopedia of Metalloproteins; Kretsinger, R.H., Uversky, V.N., Permyakov, E.A., Eds.; Springer: New York, NY, USA, 2013. [Google Scholar] [CrossRef]
- Rayman, M.P. The importance of selenium to human health. Lancet 2000, 356, 233–241. [Google Scholar] [CrossRef]
- Shimada, B.K.; Alfulaij, N.; Seale, L.A. The Impact of Selenium Deficiency on Cardiovascular Function. Int. J. Mol. Sci. 2021, 22, 10713. [Google Scholar] [CrossRef]
- Benstoem, C.; Goetzenich, A.; Kraemer, S.; Borosch, S.; Manzanares, W.; Hardy, G.; Stoppe, C. Selenium and its supplementation in cardiovascular disease—What do we know? Nutrients 2015, 7, 3094–3118. [Google Scholar] [CrossRef]
- Pereira, M.E.; Souza, J.V.; Galiciolli, M.E.A.; Sare, F.; Vieira, G.S.; Kruk, I.L.; Oliveira, C.S. Effects of Selenium Supplementation in Patients with Mild Cognitive Impairment or Alzheimer’s Disease: A Systematic Review and Meta-Analysis. Nutrients 2022, 14, 3205. [Google Scholar] [CrossRef]
- Cardoso, B.R.; Ong, T.P.; Jacob-Filho, W.; Jaluul, O.; Freitas, M.I.; Cozzolino, S.M. Nutritional status of selenium in Alzheimer’s disease patients. Br. J. Nutr. 2010, 103, 803–806. [Google Scholar] [CrossRef]
- Guillin, O.M.; Vindry, C.; Ohlmann, T.; Chavatte, L. Selenium, Selenoproteins and Viral Infection. Nutrients 2019, 11, 2101. [Google Scholar] [CrossRef]
- Avery, J.C.; Hoffmann, P.R. Selenium, Selenoproteins, and Immunity. Nutrients 2018, 10, 1203. [Google Scholar] [CrossRef]
- Mistry, H.D.; Broughton Pipkin, F.; Redman, C.W.; Poston, L. Selenium in reproductive health. Am. J. Obstet. Gynecol. 2012, 206, 21–30. [Google Scholar] [CrossRef]
- Qazi, I.H.; Angel, C.; Yang, H.; Pan, B.; Zoidis, E.; Zeng, C.J.; Han, H.; Zhou, G.B. Selenium, Selenoproteins, and Female Reproduction: A Review. Molecules 2018, 23, 3053. [Google Scholar] [CrossRef]
- Foresta, C.; Flohé, L.; Garolla, A.; Roveri, A.; Ursini, F.; Maiorino, M. Male fertility is linked to the selenoprotein phospholipid hydroperoxide glutathione peroxidase. Biol. Reprod. 2002, 67, 967–971. [Google Scholar] [CrossRef]
- Pieczyńska, J.; Grajeta, H. The role of selenium in human conception and pregnancy. J. Trace Elem. Med. Biol. 2015, 29, 31–38. [Google Scholar] [CrossRef]
- Rayman, M.P.; Searle, E.; Kelly, L.; Johnsen, S.; Bodman-Smith, K.; Bath, S.C.; Mao, J.; Redman, C.W. Effect of selenium on markers of risk of pre-eclampsia in UK pregnant women: A randomised, controlled pilot trial. Br. J. Nutr. 2014, 112, 99–111. [Google Scholar] [CrossRef]
- Askari, G.; Iraj, B.; Salehi-Abargouei, A.; Fallah, A.A.; Jafari, T. The association between serum selenium and gestational diabetes mellitus: A systematic review and meta-analysis. J. Trace Elem. Med. Biol. 2015, 29, 195–201. [Google Scholar] [CrossRef]
- Hamdan, H.Z.; Hamdan, S.Z.; Adam, I. Association of Selenium Levels with Gestational Diabetes Mellitus: An Updated Systematic Review and Meta-Analysis. Nutrients 2022, 14, 3941. [Google Scholar] [CrossRef]
- Kilonzo, V.W.; Sasuclark, A.R.; Torres, D.J.; Coyle, C.; Pilat, J.M.; Williams, C.S.; Pitts, M.W. Juvenile Selenium Deficiency Impairs Cognition, Sensorimotor Gating, and Energy Homeostasis in Mice. Front. Nutr. 2021, 8, 667587. [Google Scholar] [CrossRef]
- Gashu, D.; Stoecker, B.J. Selenium and Cognition: Mechanism and Evidence. In Handbook of Famine, Starvation, and Nutrient Deprivation; Preedy, V., Patel, V., Eds.; Springer: Cham, Switzerland, 2017. [Google Scholar] [CrossRef]
- Benton, D. Selenium intake, mood and other aspects of psychological functioning. Nutr. Neurosci. 2002, 5, 363–374. [Google Scholar] [CrossRef]
- Sajjadi, S.S.; Foshati, S.; Haddadian-Khouzani, S.; Rouhani, M.H. The role of selenium in depression: A systematic review and meta-analysis of human observational and interventional studies. Sci. Rep. 2022, 12, 1045. [Google Scholar] [CrossRef]
- Institute of Medicine (US) Panel on Dietary Antioxidants and Related Compounds. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids; National Academies Press (US): Washington, DC, USA, 2000. [Google Scholar]
- Committee on Medical Aspects of Food Policy. Dietary Reference Values for Food Energy and Nutrients for the United Kingdom; HMSO: London, UK, 1991.
- Bleys, J.; Navas-Acien, A.; Guallar, E. Serum selenium levels and all-cause, cancer, and cardiovascular mortality among US adults. Arch. Intern. Med. 2008, 168, 404–410. [Google Scholar] [CrossRef]
- Brodin, O.; Hackler, J.; Misra, S.; Wendt, S.; Sun, Q.; Laaf, E.; Stoppe, C.; Björnstedt, M.; Schomburg, L. Selenoprotein P as Biomarker of Selenium Status in Clinical Trials with Therapeutic Dosages of Selenite. Nutrients. 2020, 12, 1067. [Google Scholar] [CrossRef]
- Zachara, B.A.; Wardak, C.; Didkowski, W.; Maciag, A.; Marchaluk, E. Changes in blood selenium and glutathione concentrations and glutathione peroxidase activity in human pregnancy. Gynecol. Obstet. Investig. 1993, 35, 12–17. [Google Scholar] [CrossRef]
- Ferrer, E.; Alegría, A.; Barberá, R.; Farré, R.; Lagarda, M.J.; Monleon, J. Whole blood selenium content in pregnant women. Sci. Total Environ. 1999, 227, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Mihailović, M.; Cvetković, M.; Ljubić, A.; Kosanović, M.; Nedeljković, S.; Jovanović, I.; Pesut, O. Selenium and malondialdehyde content and glutathione peroxidase activity in maternal and umbilical cord blood and amniotic fluid. Biol. Trace Elem. Res. 2000, 73, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Zachara, B.A.; Dobrzyński, W.; Trafikowska, U.; Szymański, W. Blood selenium and glutathione peroxidases in miscarriage. BJOG 2001, 108, 244–247. [Google Scholar] [CrossRef] [PubMed]
- Duntas, L.H. Selenium and At-Risk Pregnancy: Challenges and Controversies. Thyroid Res. 2020, 13, 16. [Google Scholar] [CrossRef] [PubMed]
- Mariath, A.B.; Bergamaschi, D.P.; Rondo, P.H.; Ana, C.A.T.; de Fragas Hinnig, P.; Abbade, J.F.; Diniz, S.G. The Possible Role of Selenium Status in Adverse Pregnancy Outcomes. Br. J. Nutr. 2011, 105, 1418–1428. [Google Scholar] [CrossRef] [PubMed]
- Varsi, K.; Bolann, B.; Torsvik, I.; Rosvold Eik, T.C.; Høl, P.J.; Bjørke-Monsen, A.-L. Impact of Maternal Selenium Status on Infant Outcome during the First 6 Months of Life. Nutrients 2017, 9, 486. [Google Scholar] [CrossRef] [PubMed]
- Skröder, H.M.; Hamadani, J.D.; Tofail, F.; Persson, L.Å.; Vahter, M.E.; Kippler, M.J. Selenium Status in Pregnancy Influences Children’s Cognitive Function at 1.5 Years of Age. Clin. Nutr. 2015, 34, 923–930. [Google Scholar] [CrossRef] [PubMed]
- Polanska, K.; Krol, A.; Sobala, W.; Gromadzinska, J.; Brodzka, R.; Calamandrei, G.; Chiarotti, F.; Wasowicz, W.; Hanke, W. Selenium Status during Pregnancy and Child Psychomotor Development—Polish Mother and Child Cohort Study. Pediatr. Res. 2016, 79, 863–869. [Google Scholar] [CrossRef] [PubMed]
- Polanska, K.; Hanke, W.; Krol, A.; Gromadzinska, J.; Kuras, R.; Janasik, B.; Wasowicz, W.; Mirabella, F.; Chiarotti, F.; Calamandrei, G. Micronutrients during Pregnancy and Child Psychomotor Development: Opposite Effects of Zinc and Selenium. Environ. Res. 2017, 158, 583–589. [Google Scholar] [CrossRef]
- Lee, A.S.E.; Ji, Y.; Raghavan, R.; Wang, G.; Hong, X.; Pearson, C.; Mirolli, G.; Bind, E.; Steffens, A.; Mukherjee, J.; et al. Maternal Prenatal Selenium Levels and Child Risk of Neurodevelopmental Disorders: A Prospective Birth Cohort Study. Autism Res. 2021, 14, 2533–2543. [Google Scholar] [CrossRef]
- FoodData Central. U.S. Department of Agriculture. Available online: https://fdc.nal.usda.gov/fdc-app.html#/food-search?component=1103 (accessed on 5 June 2024).
- Food Composition Data. EFSA. Available online: https://www.efsa.europa.eu/en/microstrategy/food-composition-data (accessed on 5 June 2024).
- Cox, J.L.; Holden, J.M.; Sagovsky, R. Detection of Postnatal Depression. Development of the 10-Item Edinburgh Postnatal Depression Scale. Br. J. Psychiatry 1987, 150, 782–786. [Google Scholar] [CrossRef] [PubMed]
- Mokhber, N.; Namjoo, M.; Tara, F.; Boskabadi, H.; Rayman, M.P.; Ghayour-Mobarhan, M.; Sahebkar, A.; Majdi, M.R.; Tavallaie, S.; Azimi-Nezhad, M.; et al. Effect of supplementation with selenium on postpartum depression: A randomized double-blind placebo-controlled trial. J. Matern. Fetal Neonatal Med. 2011, 24, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Leung, B.M.; Kaplan, B.J.; Field, C.J.; Tough, S.; Eliasziw, M.; Gomez, M.F.; McCargar, L.J.; Gagnon, L.; APrON Study Team. Prenatal micronutrient supplementation and postpartum depressive symptoms in a pregnancy cohort. BMC Pregnancy Childbirth 2013, 13, 2. [Google Scholar] [CrossRef] [PubMed]
- Amini, S.; Jafarirad, S.; Amani, R.; Sayyah Bargard, M.; Cheraghian, B.; Hemmati, A.A. The relationship between dietary intakes during pregnancy and incidence of postpartum depression: A case–control study. Nutr. Food Sci. 2019, 50, 751–764. [Google Scholar] [CrossRef]
- Jin, Y.; Coad, J.; Pond, R.; Kim, N.; Brough, L. Selenium intake and status of postpartum women and postnatal depression during the first year after childbirth in New Zealand—Mother and Infant Nutrition Investigation (MINI) study. J. Trace Elem. Med. Biol. 2020, 61, 126503. [Google Scholar] [CrossRef] [PubMed]
- Johnson, C.C.; Fordyce, F.M.; Rayman, M.P. Symposium on ‘Geographical and geological influences on nutrition’: Factors controlling the distribution of selenium in the environment and their impact on health and nutrition. Proc. Nutr. Soc. 2010, 69, 119–132. [Google Scholar] [CrossRef] [PubMed]
- Castaño, A.; Ayala, A.; Rodríguez-Gómez, J.A.; Herrera, A.J.; Cano, J.; Machado, A. Low selenium diet increases the dopamine turnover in prefrontal cortex of the rat. Neurochem. Int. 1997, 30, 549–555. [Google Scholar] [CrossRef]
- Brüning, C.A.; Prigol, M.; Roehrs, J.A.; Nogueira, C.W.; Zeni, G. Involvement of the serotonergic system in the anxiolytic-like effect caused by m-trifluoromethyl-diphenyl diselenide in mice. Behav. Brain Res. 2009, 205, 511–517. [Google Scholar] [CrossRef]
- Solovyev, N.D. Importance of selenium and selenoprotein for brain function: From antioxidant protection to neuronal signalling. J. Inorg. Biochem. 2015, 153, 1–12. [Google Scholar] [CrossRef]
- Kumari, S.; Mehta, S.L.; Li, P.A. Glutamate induces mitochondrial dynamic imbalance and autophagy activation: Preventive effects of selenium. PLoS ONE 2012, 7, e39382. [Google Scholar] [CrossRef]
- Olguín-Albuerne, M.; Morán, J. Redox Signaling Mechanisms in Nervous System Development. Antioxid. Redox Signal. 2018, 28, 1603–1625. [Google Scholar] [CrossRef] [PubMed]
- Steinert, J.R.; Amal, H. The contribution of an imbalanced redox signalling to neurological and neurodegenerative conditions. Free Radic. Biol. Med. 2022, 194, 71–83. [Google Scholar] [CrossRef]
- Zakeri, N.; Asbaghi, O.; Naeini, F.; Afsharfar, M.; Mirzadeh, E.; kasra Naserizadeh, S. Selenium supplementation and oxidative stress: A review. PharmaNutrition 2021, 17, 100263. [Google Scholar] [CrossRef]
- Uotila, J.; Tuimala, R.; Aarnio, T.; Pyykkö, K.; Ahotupa, M. Lipid peroxidation products, selenium-dependent glutathione peroxidase and vitamin E in normal pregnancy. Eur. J. Obstet. Gynecol. Reprod. Biol. 1991, 42, 95–100. [Google Scholar] [CrossRef]
- Biswas, K.; McLay, J.; Campbell, F.M. Selenium Supplementation in Pregnancy-Maternal and Newborn Outcomes. J. Nutr. Metab. 2022, 2022, 4715965. [Google Scholar] [CrossRef] [PubMed]
- Rayman, M.P. Selenium intake, status, and health: A complex relationship. Hormones 2020, 19, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Osimo, E.F.; Pillinger, T.; Rodriguez, I.M.; Khandaker, G.M.; Pariante, C.M.; Howes, O.D. Inflammatory markers in depression: A meta-analysis of mean differences and variability in 5166 patients and 5083 controls. Brain Behav. Immun. 2020, 87, 901–909. [Google Scholar] [CrossRef] [PubMed]
- Thomas, S.; Laury-Kleintop, L.; Prendergast, G.C. Reliable detection of indoleamine 2,3 dioxygenase-1 in murine cells and tissues. Methods Enzymol. 2019, 629, 219–233. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.H.; Haroon, E.; Raison, C.L.; Felger, J.C. Cytokine targets in the brain: Impact on neurotransmitters and neurocircuits. Depress. Anxiety 2013, 30, 297–306. [Google Scholar] [CrossRef]
- Maes, M.; Verkerk, R.; Bonaccorso, S.; Ombelet, W.; Bosmans, E.; Scharpé, S. Depressive and anxiety symptoms in the early puerperium are related to increased degradation of tryptophan into kynurenine, a phenomenon which is related to immune activation. Life Sci. 2002, 71, 1837–1848. [Google Scholar] [CrossRef]
- Tseng, C.K.; Ho, C.T.; Hsu, H.S.; Lin, C.H.; Li, C.I.; Li, T.C.; Liu, C.S.; Lin, C.C.; Lin, W.Y. Selenium is inversely associated with interleukin-6 in the elderly. J. Nutr. Health Aging 2013, 17, 280–284. [Google Scholar] [CrossRef]
- Asbaghi, O.; Saboori, S.; Hekmatdoost, A.; Abdollahpour, F.; Rad, E.Y.; Salehpour, S. Effects of selenium supplementation on serum C reactive protein level: A systematic review and meta-analysis of randomized controlled clinical trials. Obes. Med. 2020, 17, 100182. [Google Scholar] [CrossRef]
- Szpunar, M.J.; Malaktaris, A.; Baca, S.A.; Hauger, R.L.; Lang, A.J. Are alterations in estradiol, cortisol, and inflammatory cytokines associated with depression during pregnancy and postpartum? An exploratory study. Brain Behav. Immun. Health 2021, 16, 100309. [Google Scholar] [CrossRef]
- Xia, H.; Zhu, X.; Zhu, C. Associations between pro-inflammatory cytokines and fatigue in pregnant women. PeerJ 2022, 10, e13965. [Google Scholar] [CrossRef] [PubMed]
- Kraus, T.A.; Sperling, R.S.; Engel, S.M.; Lo, Y.; Kellerman, L.; Singh, T.; Loubeau, M.; Ge, Y.; Garrido, J.L.; Rodriguez-Garcia, M.; et al. Peripheral blood cytokine profiling during pregnancy and post-partum periods. Am. J. Reprod. Immunol. 2010, 64, 411–426. [Google Scholar] [CrossRef] [PubMed]
- Blackmore, E.R.; Moynihan, J.A.; Rubinow, D.R.; Pressman, E.K.; Gilchrist, M.; O’Connor, T.G. Psychiatric symptoms and proinflammatory cytokines in pregnancy. Psychosom. Med. 2011, 73, 656–663. [Google Scholar] [CrossRef] [PubMed]
- Ross, K.M.; Miller, G.; Culhane, J.; Grobman, W.; Simhan, H.N.; Wadhwa, P.D.; Williamson, D.; McDade, T.; Buss, C.; Entringer, S.; et al. Patterns of peripheral cytokine expression during pregnancy in two cohorts and associations with inflammatory markers in cord blood. Am. J. Reprod. Immunol. 2016, 76, 406–414. [Google Scholar] [CrossRef]
- Stokkeland, L.M.T.; Giskeødegård, G.F.; Stridsklev, S.; Ryan, L.; Steinkjer, B.; Tangeras, L.H.; Vanky, E.; Iversen, A.-C. Serum cytokine patterns in first half of pregnancy. Cytokine 2019, 119, 188–196. [Google Scholar] [CrossRef]
- Christian, L.M.; Porter, K. Longitudinal changes in serum proinflammatory markers across pregnancy and postpartum: Effects of maternal body mass index. Cytokine 2014, 70, 134–140. [Google Scholar] [CrossRef]
- Maes, M.; Lin, A.H.; Ombelet, W.; Stevens, K.; Kenis, G.; De Jongh, R.; Cox, J.; Bosmans, E. Immune activation in the early puerperium is related to postpartum anxiety and depressive symptoms. Psychoneuroendocrinology 2000, 25, 121–137. [Google Scholar] [CrossRef]
- Arthur, J.R.; Nicol, F.; Beckett, G.J. The role of selenium in thyroid hormone metabolism and effects of selenium deficiency on thyroid hormone and iodine metabolism. Biol. Trace Elem. Res. 1992, 34, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Minnetti, M.; Sada, V.; Feola, T.; Giannetta, E.; Pozza, C.; Gianfrilli, D.; Isidori, A.M.; Cozzolino, A. Selenium Supplementation in Pregnant Women with Autoimmune Thyroiditis: A Practical Approach. Nutrients 2022, 14, 2234. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, P.M.D.S.; Longoni, A.; Pinheiro, R.T.; Assis, A.M. Postpartum depression in maternal thyroidal changes. Thyroid Res. 2022, 15, 6. [Google Scholar] [CrossRef] [PubMed]
- Dama, M.; Steiner, M.; Lieshout, R.V. Thyroid peroxidase autoantibodies and perinatal depression risk: A systematic review. J. Affect. Disord. 2016, 198, 108–121. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Xu, S.; Zhang, H.; Cao, W.; Wang, K.; Chen, G.; Di, H.; Cao, M.; Liu, C. Selenium supplementation for autoimmune thyroiditis: A systematic review and meta-analysis. Int. J. Endocrinol. 2014, 2014, 904573. [Google Scholar] [CrossRef] [PubMed]
- Köhrle, J. Selenium, Iodine and Iron–Essential Trace Elements for Thyroid Hormone Synthesis and Metabolism. Int. J. Mol. Sci. 2023, 24, 3393. [Google Scholar] [CrossRef] [PubMed]
- Severo, J.S.; Morais, J.B.S.; de Freitas, T.E.C.; Andrade, A.L.P.; Feitosa, M.M.; Fontenelle, L.C.; de Oliveira, A.R.S.; Cruz, K.J.C.; do Nascimento Marreiro, D. The Role of Zinc in Thyroid Hormones Metabolism. Int. J. Vitam. Nutr. Res. 2019, 89, 80–88. [Google Scholar] [CrossRef] [PubMed]
- Castrén, E.; Monteggia, L.M. Brain-Derived Neurotrophic Factor Signaling in Depression and Antidepressant Action. Biol. Psychiatry 2021, 90, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Liu, W.; Ge, T.; Leng, Y.; Pan, Z.; Fan, J.; Yang, W.; Cui, R. The Role of Neural Plasticity in Depression: From Hippocampus to Prefrontal Cortex. Neural Plast. 2017, 2017, 6871089. [Google Scholar] [CrossRef]
- Mosiołek, A.; Mosiołek, J.; Jakima, S.; Pięta, A.; Szulc, A. Effects of Antidepressant Treatment on Neurotrophic Factors (BDNF and IGF-1) in Patients with Major Depressive Disorder (MDD). J. Clin. Med. 2021, 10, 3377. [Google Scholar] [CrossRef]
- Caviedes, A.; Lafourcade, C.; Soto, C.; Wyneken, U. BDNF/NF-κB Signaling in the Neurobiology of Depression. Curr. Pharm. Des. 2017, 23, 3154–3163. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.H.; Nicol, F.; Beckett, G.J.; Arthur, J.R. Selenoprotein expression and brain development in preweanling selenium- and iodine-deficient rats. J. Mol. Endocrinol. 1998, 20, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Szopa, A.; Herbet, M.; Poleszak, E.; Bogatko, K.; Ostrowska-Leśko, M.; Świąder, K.; Szponar, J.; Serefko, A. Effects of Selen on the Antidepressant-like Activity of Agents Affecting the Adenosinergic Neurotransmission. Metabolites 2022, 12, 586. [Google Scholar] [CrossRef] [PubMed]
- Li, L.X.; Chu, J.H.; Chen, X.W.; Gao, P.C.; Wang, Z.Y.; Liu, C.; Fan, R.F. Selenium ameliorates mercuric chloride-induced brain damage through activating BDNF/TrKB/PI3K/AKT and inhibiting NF-κB signaling pathways. J. Inorg. Biochem. 2022, 229, 111716. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Um, P.; Dickerman, B.A.; Liu, J. Zinc, Magnesium, Selenium and Depression: A Review of the Evidence, Potential Mechanisms and Implications. Nutrients 2018, 10, 584. [Google Scholar] [CrossRef] [PubMed]
- Duman, R.S.; Monteggia, L.M. A neurotrophic model for stress-related mood disorders. Biol. Psychiatry 2006, 59, 1116–1127. [Google Scholar] [CrossRef] [PubMed]
- Hing, B.; Sathyaputri, L.; Potash, J.B. A comprehensive review of genetic and epigenetic mechanisms that regulate BDNF expression and function with relevance to major depressive disorder. Am. J. Med. Genet. B Neuropsychiatr. Genet. 2018, 177, 143–167. [Google Scholar] [CrossRef] [PubMed]
- Thompson Ray, M.; Weickert, C.S.; Wyatt, E.; Webster, M.J. Decreased BDNF, trkB-TK+ and GAD67 mRNA expression in the hippocampus of individuals with schizophrenia and mood disorders. J. Psychiatry Neurosci. 2011, 36, 195–203. [Google Scholar] [CrossRef] [PubMed]
- Tripp, A.; Oh, H.; Guilloux, J.P.; Martinowich, K.; Lewis, D.A.; Sibille, E. Brain-derived neurotrophic factor signaling and subgenual anterior cingulate cortex dysfunction in major depressive disorder. Am. J. Psychiatry 2012, 169, 1194–1202. [Google Scholar] [CrossRef]
- Castrén, E.; Antila, H. Neuronal plasticity and neurotrophic factors in drug responses. Mol. Psychiatry 2017, 22, 1085–1095. [Google Scholar] [CrossRef]
- Chen, B.; Dowlatshahi, D.; MacQueen, G.M.; Wang, J.F.; Young, L.T. Increased hippocampal BDNF immunoreactivity in subjects treated with antidepressant medication. Biol. Psychiatry 2001, 50, 260–265. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Kim, K.H.; Lee, B.H.; Kim, Y.K. Plasma level of brain-derived neurotrophic factor (BDNF) in patients with postpartum depression. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 109, 110245. [Google Scholar] [CrossRef] [PubMed]
- Gao, X.; Wang, J.; Yao, H.; Cai, Y.; Cheng, R. Serum BDNF concentration after delivery is associated with development of postpartum depression: A 3-month follow up study. J. Affect. Disord. 2016, 200, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Chen, C.; Yu, H.; Yang, Z. Fecal Microbiota Changes in Patients With Postpartum Depressive Disorder. Front. Cell Infect. Microbiol. 2020, 10, 567268. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karkoszka, N.; Gibula-Tarlowska, E.; Kotlinska, J.; Bielenica, A.; Gawel, K.; Kedzierska, E. Selenium Intake and Postnatal Depression—A Short Review. Nutrients 2024, 16, 1926. https://doi.org/10.3390/nu16121926
Karkoszka N, Gibula-Tarlowska E, Kotlinska J, Bielenica A, Gawel K, Kedzierska E. Selenium Intake and Postnatal Depression—A Short Review. Nutrients. 2024; 16(12):1926. https://doi.org/10.3390/nu16121926
Chicago/Turabian StyleKarkoszka, Natalia, Ewa Gibula-Tarlowska, Jolanta Kotlinska, Anna Bielenica, Kinga Gawel, and Ewa Kedzierska. 2024. "Selenium Intake and Postnatal Depression—A Short Review" Nutrients 16, no. 12: 1926. https://doi.org/10.3390/nu16121926
APA StyleKarkoszka, N., Gibula-Tarlowska, E., Kotlinska, J., Bielenica, A., Gawel, K., & Kedzierska, E. (2024). Selenium Intake and Postnatal Depression—A Short Review. Nutrients, 16(12), 1926. https://doi.org/10.3390/nu16121926