
Efficacy of a Food Supplement Containing Lactobacillus acidophilus LA14, Peptides, and a Multivitamin Complex in Improving Gastroesophageal Reflux Disease-Related Outcomes and Quality of Life of Subjects Showing Mild-to-Moderate Gastroesophageal Reflux Disease

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
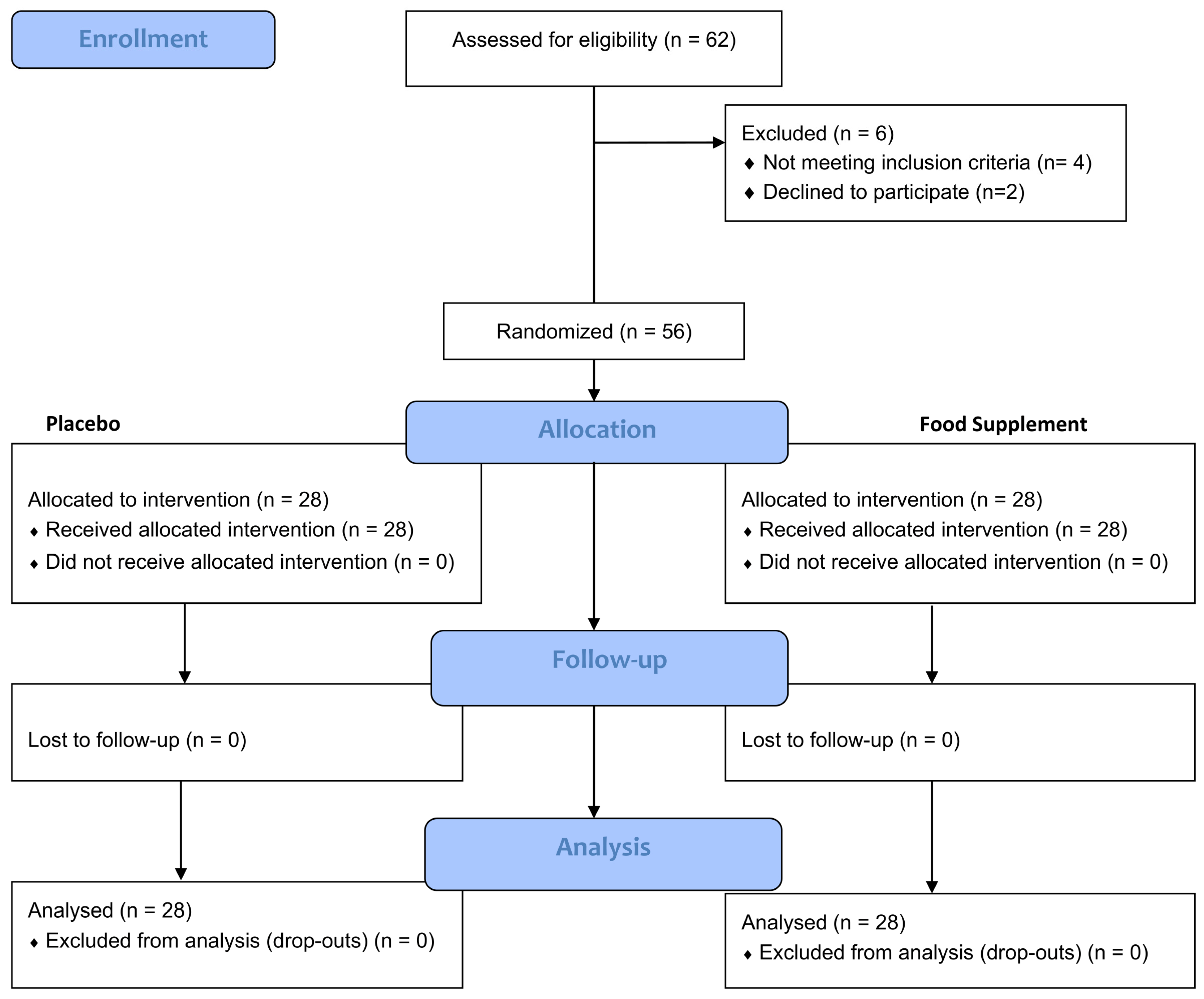
2.1. Study Participants
2.2. Study Design
2.3. Primary and Secondary Outcomes of the Study
2.3.1. Quality of Life Questionnaire (GERD-QoL)
2.3.2. Self-Assessment Questionnaire
2.4. Products
2.5. Statistical Analysis
3. Results
3.1. Heartburn Frequency and Severity
3.2. GERD-QoL Questionnaire
3.3. Self-Assessment Questionnaire
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Katz, P.O.; Dunbar, K.B.; Schnoll-Sussman, F.H.; Greer, K.B.; Yadlapati, R.; Spechler, S.J. ACG Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease. Am. J. Gastroenterol. 2022, 117, 27–56. [Google Scholar] [CrossRef] [PubMed]
- Eusebi, L.H.; Ratnakumaran, R.; Yuan, Y.; Solaymani-Dodaran, M.; Bazzoli, F.; Ford, A.C. Global Prevalence of, and Risk Factors for, Gastro-Oesophageal Reflux Symptoms: A Meta-Analysis. Gut 2018, 67, 430–440. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B.; Sweet, S.; Winchester, C.C.; Dent, J. Update on the Epidemiology of Gastro-Oesophageal Reflux Disease: A Systematic Review. Gut 2014, 63, 871–880. [Google Scholar] [CrossRef] [PubMed]
- Fass, R.; Frazier, R. The Role of Dexlansoprazole Modified-Release in the Management of Gastroesophageal Reflux Disease. Ther. Adv. Gastroenterol. 2017, 10, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Hom, C.; Vaezi, M.F. Extraesophageal Manifestations of Gastroesophageal Reflux Disease. Gastroenterol. Clin. N. Am. 2013, 42, 71–91. [Google Scholar] [CrossRef] [PubMed]
- Antunes, C.; Aleem, A.; Curtis, S.A. Gastroesophageal Reflux Disease. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Nirwan, J.S.; Hasan, S.S.; Babar, Z.-U.-D.; Conway, B.R.; Ghori, M.U. Global Prevalence and Risk Factors of Gastro-Oesophageal Reflux Disease (GORD): Systematic Review with Meta-Analysis. Sci. Rep. 2020, 10, 5814. [Google Scholar] [CrossRef] [PubMed]
- Savarino, V.; Marabotto, E.; Zentilin, P.; Demarzo, M.G.; de Bortoli, N.; Savarino, E. Pharmacological Management of Gastro-Esophageal Reflux Disease: An Update of the State-of-the-Art. Drug Des. Dev. Ther. 2021, 15, 1609–1621. [Google Scholar] [CrossRef] [PubMed]
- Patrick, L. Gastroesophageal Reflux Disease (GERD): A Review of Conventional and Alternative Treatments. Altern. Med. Rev. 2011, 16, 116–133. [Google Scholar] [PubMed]
- Zacny, J.; Zamakhshary, M.; Sketris, I.; van Zanten, S. Systematic review: The efficacy of intermittent and on-demand therapy with histamine. Aliment. Pharmacol. Ther. 2005, 21, 1299–1312. [Google Scholar] [CrossRef]
- Salisbury, B.H.; Terrell, J.M. Antacids. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Lakananurak, N.; Pitisuttithum, P.; Susantitaphong, P.; Patcharatrakul, T.; Gonlachanvit, S. The Efficacy of Dietary Interventions in Patients with Gastroesophageal Reflux Disease: A Systematic Review and Meta-Analysis of Intervention Studies. Nutrients 2024, 16, 464. [Google Scholar] [CrossRef]
- Martin, Z.; Spry, G.; Hoult, J.; Maimone, I.R.; Tang, X.; Crichton, M.; Marshall, S. What Is the Efficacy of Dietary, Nutraceutical, and Probiotic Interventions for the Management of Gastroesophageal Reflux Disease Symptoms? A Systematic Literature Review and Meta-Analysis. Clin. Nutr. ESPEN 2022, 52, 340–352. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.; Singh, R.; Ro, S.; Ghoshal, U.C. Gut microbiota dysbiosis in functional gastrointestinal disorders: Underpinning the symptoms and pathophysiology. JGH Open. 2021, 5, 976–987. [Google Scholar] [CrossRef] [PubMed]
- Mandarino, F.V.; Sinagra, E.; Raimondo, D.; Danese, S. The Role of Microbiota in Upper and Lower Gastrointestinal Functional Disorders. Microorganisms 2023, 11, 980. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, S.M.; Cundra, L.B.; Yoo, B.S.; Parekh, P.J.; Johnson, D.A. Microbiome and Gastroesophageal Disease: Pathogenesis and Implications for Therapy. Ann. Clin. Gastroenterol. Hepatol. 2020, 4, 020–033. [Google Scholar] [CrossRef]
- Blackett, K.L.; Siddhi, S.S.; Cleary, S.; Steed, H.; Miller, M.H.; Macfarlane, S.; Macfarlane, G.T.; Dillon, J.F. Oesophageal bacterial biofilm changes in gastro-oesophageal reflux disease, barrett’s and oesophageal carcinoma: Association or causality? Aliment. Pharmacol. Ther. 2013, 37, 1084–1092. [Google Scholar] [CrossRef]
- Corning, B.; Copland, A.P.; Frye, J.W. The Esophageal Microbiome in Health and Disease. Curr. Gastroenterol. Rep. 2018, 20, 39. [Google Scholar] [CrossRef]
- Cheng, J.; Ouwehand, A.C. Gastroesophageal Reflux Disease and Probiotics: A Systematic Review. Nutrients 2020, 12, 132. [Google Scholar] [CrossRef] [PubMed]
- Igarashi, M.; Nagano, J.; Tsuda, A.; Suzuki, T.; Koike, J.; Uchida, T.; Matsushima, M.; Mine, T.; Koga, Y. Correlation between the Serum Pepsinogen I Level and the Symptom Degree in Proton Pump Inhibitor-Users Administered with a Probiotic. Pharmaceuticals 2014, 7, 754–764. [Google Scholar] [CrossRef]
- Keita, Å.V.; Söderholm, J.D. Mucosal Permeability and Mast Cells as Targets for Functional Gastrointestinal Disorders. Curr. Opin. Pharmacol. 2018, 43, 66–71. [Google Scholar] [CrossRef]
- Nakae, H.; Tsuda, A.; Matsuoka, T.; Mine, T.; Koga, Y. Gastric Microbiota in the Functional Dyspepsia Patients Treated with Probiotic Yogurt. BMJ Open Gastroenterol. 2016, 3, e000109. [Google Scholar] [CrossRef]
- Chatterjee, C.; Gleddie, S.; Xiao, C.-W. Soybean Bioactive Peptides and Their Functional Properties. Nutrients 2018, 10, 1211. [Google Scholar] [CrossRef] [PubMed]
- Hirata, Y.; Uchida, A. Clinical effects of Gastro AD in gastritis patients. Japn J. Med. Pharm. Sci. 2003, 49, 597–601. [Google Scholar]
- Fatani, A.; Vaher, K.; Rivero-Mendoza, D.; Alabasi, K.; Dahl, W.J. Fermented Soy Supplementation Improves Indicators of Quality of Life: A Randomized, Placebo-Controlled, Double-Blind Trial in Adults Experiencing Heartburn. BMC Res. Notes 2020, 13, 364. [Google Scholar] [CrossRef] [PubMed]
- Fraser, A.; Delaney, B.C.; Ford, A.C.; Qume, M.; Moayyedi, P. The Short-Form Leeds Dyspepsia Questionnaire validation study. Aliment. Pharmacol. Ther. 2007, 25, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.; Junghard, O.; Dent, J.; Vakil, N.; Halling, K.; Wernersson, B.; Lind, T. Development of the GerdQ, a tool for the diagnosis and management of gastro-oesophageal reflux disease in primary care. Aliment. Pharmacol. Ther. 2009, 30, 1030–1038. [Google Scholar] [CrossRef] [PubMed]
- Gatta, L.; Moayyedi, P.; Tosetti, C.; Vakil, N.; Ubaldi, E.; Barsanti, P.; Fiorini, G.; Castelli, V.; Gargiulo, C.; Lucarini, P.; et al. A validation study of the Italian Short-Form Leeds Dyspepsia Questionnaire. Intern. Emerg. Med. 2010, 5, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Peters, J.H. Surgical treatment of gastroesophageal reflux disease. Gastroenterol. Hepatol. 2014, 10, 247–248. [Google Scholar] [PubMed] [PubMed Central]
- Newberry, C.; Lynch, K. The Role of Diet in the Development and Management of Gastroesophageal Reflux Disease: Why We Feel the Burn. J. Thorac. Dis. 2019, 11 (Suppl. 12), S1594–S1601. [Google Scholar] [CrossRef]
- Belobrajdic, D.P.; James-Martin, G.; Jones, D.; Tran, C.D. Soy and Gastrointestinal Health: A Review. Nutrients 2023, 15, 1959. [Google Scholar] [CrossRef]
- Skoufou, M.; Tsigalou, C.; Vradelis, S.; Bezirtzoglou, E. The Networked Interaction between Probiotics and Intestine in Health and Disease: A Promising Success Story. Microorganisms 2024, 12, 194. [Google Scholar] [CrossRef]
- Hungin, A.P.S.; Mitchell, C.R.; Whorwell, P.; Mulligan, C.; Cole, O.; Agréus, L.; Fracasso, P.; Lionis, C.; Mendive, J.; Philippart de Foy, J.-M.; et al. Systematic Review: Probiotics in the Management of Lower Gastrointestinal Symptoms—An Updated Evidence-Based International Consensus. Aliment. Pharmacol. Ther. 2018, 47, 1054–1070. [Google Scholar] [CrossRef] [PubMed]
- Niu, H.-L.; Xiao, J.-Y. The efficacy and safety of probiotics in patients with irritable bowel syndrome: Evidence based on 35 randomized controlled trials. Int. J. Surg. 2020, 75, 116–127. [Google Scholar] [CrossRef] [PubMed]
- Mekonnen, S.A.; Daniel Merenstein, D.; Fraser, C.M.; Marco, M.L. Molecular mechanisms of probiotic prevention of antibiotic-associated diarrhea. Curr. Opin. Biotechnol. 2020, 61, 226–234. [Google Scholar] [CrossRef] [PubMed]
- Homan, M.; Orel, R. Are Probiotics Useful in Helicobacter Pylori Eradication? World J. Gastroenterol. 2015, 21, 10644–10653. [Google Scholar] [CrossRef]
- Bai, X.; Zhu, M.; He, Y.; Wang, T.; Tian, D.; Shu, J. The impacts of probiotics in eradication therapy of Helicobacter pylori. Arch. Microbiol. 2022, 204, 692. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lee, M.; Kim, D.; Kim, H.; Jo, S.; Kim, O.-K.; Lee, J. Gastro-Protective Effect of Fermented Soybean (Glycine max (L.) Merr.) in a Rat Model of Ethanol/HCl-Induced Gastric Injury. Nutrients 2022, 14, 2079. [Google Scholar] [CrossRef]
- Barchi, A.; Massimino, L.; Mandarino, F.V.; Vespa, E.; Sinagra, E.; Almolla, O.; Passaretti, S.; Fasulo, E.; Parigi, T.L.; Cagliani, S.; et al. Microbiota profiling in esophageal diseases: Novel insights into molecular staining and clinical outcomes. Comput. Struct. Biotechnol. J. 2023, 23, 626–637. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]



{kind=link}
{kind=link}
{kind=link}
| Heartburn Frequency | ||||
| Placebo | Food Supplement | |||
| Time | Score | Tx − T0 | Score | Tx − T0 |
| T0 | 1.90 ± 0.1 | 1.77 ± 0.1 | ||
| T14 | 1.78 ± 0.1 | −0.12 ± 0.08 | 1.30 ± 0.1 *** | −0.47 ± 0.09 # |
| T28 | 1.88 ± 0.1 | −0.01 ± 0.09 | 1.24 ± 0.1 *** | −0.53 ± 0.08 ### |
| Heartburn Severity | ||||
| Placebo | Food Supplement | |||
| Time | Score | Tx − T0 | Score | Tx − T0 |
| T0 | 2.17 ± 0.1 | 2.20 ± 0.1 | ||
| T14 | 2.06 ± 0.1 | −0.10 ± 0.08 | 1.83 ± 0.1 ** | −3.7 ± 0.11 |
| T28 | 2.16 ± 0.1 | −0.01 ± 0.09 | 1.60 ± 0.1 *** | −6.1 ± 0.10 ### |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tursi, F.; Benedetto, E.; Spina, A.; De Ponti, I.; Amone, F.; Nobile, V. Efficacy of a Food Supplement Containing Lactobacillus acidophilus LA14, Peptides, and a Multivitamin Complex in Improving Gastroesophageal Reflux Disease-Related Outcomes and Quality of Life of Subjects Showing Mild-to-Moderate Gastroesophageal Reflux Disease. Nutrients 2024, 16, 1759. https://doi.org/10.3390/nu16111759
Tursi F, Benedetto E, Spina A, De Ponti I, Amone F, Nobile V. Efficacy of a Food Supplement Containing Lactobacillus acidophilus LA14, Peptides, and a Multivitamin Complex in Improving Gastroesophageal Reflux Disease-Related Outcomes and Quality of Life of Subjects Showing Mild-to-Moderate Gastroesophageal Reflux Disease. Nutrients. 2024; 16(11):1759. https://doi.org/10.3390/nu16111759
Chicago/Turabian StyleTursi, Francesco, Edoardo Benedetto, Amelia Spina, Ileana De Ponti, Fabio Amone, and Vincenzo Nobile. 2024. "Efficacy of a Food Supplement Containing Lactobacillus acidophilus LA14, Peptides, and a Multivitamin Complex in Improving Gastroesophageal Reflux Disease-Related Outcomes and Quality of Life of Subjects Showing Mild-to-Moderate Gastroesophageal Reflux Disease" Nutrients 16, no. 11: 1759. https://doi.org/10.3390/nu16111759
APA StyleTursi, F., Benedetto, E., Spina, A., De Ponti, I., Amone, F., & Nobile, V. (2024). Efficacy of a Food Supplement Containing Lactobacillus acidophilus LA14, Peptides, and a Multivitamin Complex in Improving Gastroesophageal Reflux Disease-Related Outcomes and Quality of Life of Subjects Showing Mild-to-Moderate Gastroesophageal Reflux Disease. Nutrients, 16(11), 1759. https://doi.org/10.3390/nu16111759