
Explorative Characterization of GI Complaints, General Physical and Mental Wellbeing, and Gut Microbiota in Trained Recreative and Competitive Athletes with or without Self-Reported Gastrointestinal Symptoms

 ,
,  , , , , , and
, , , , , and
Abstract
1. Introduction
2. Materials and Methods
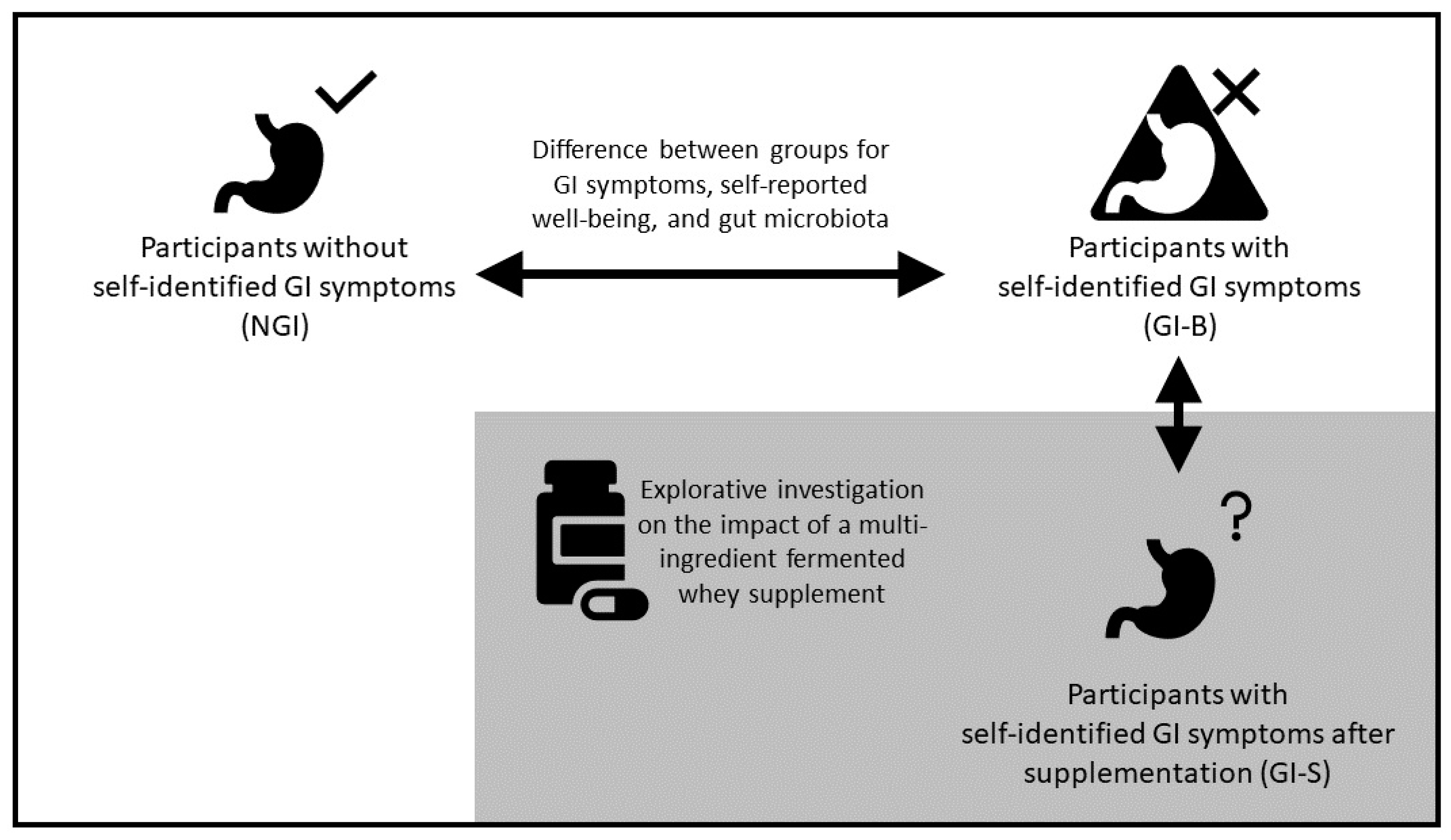
2.1. Study Design
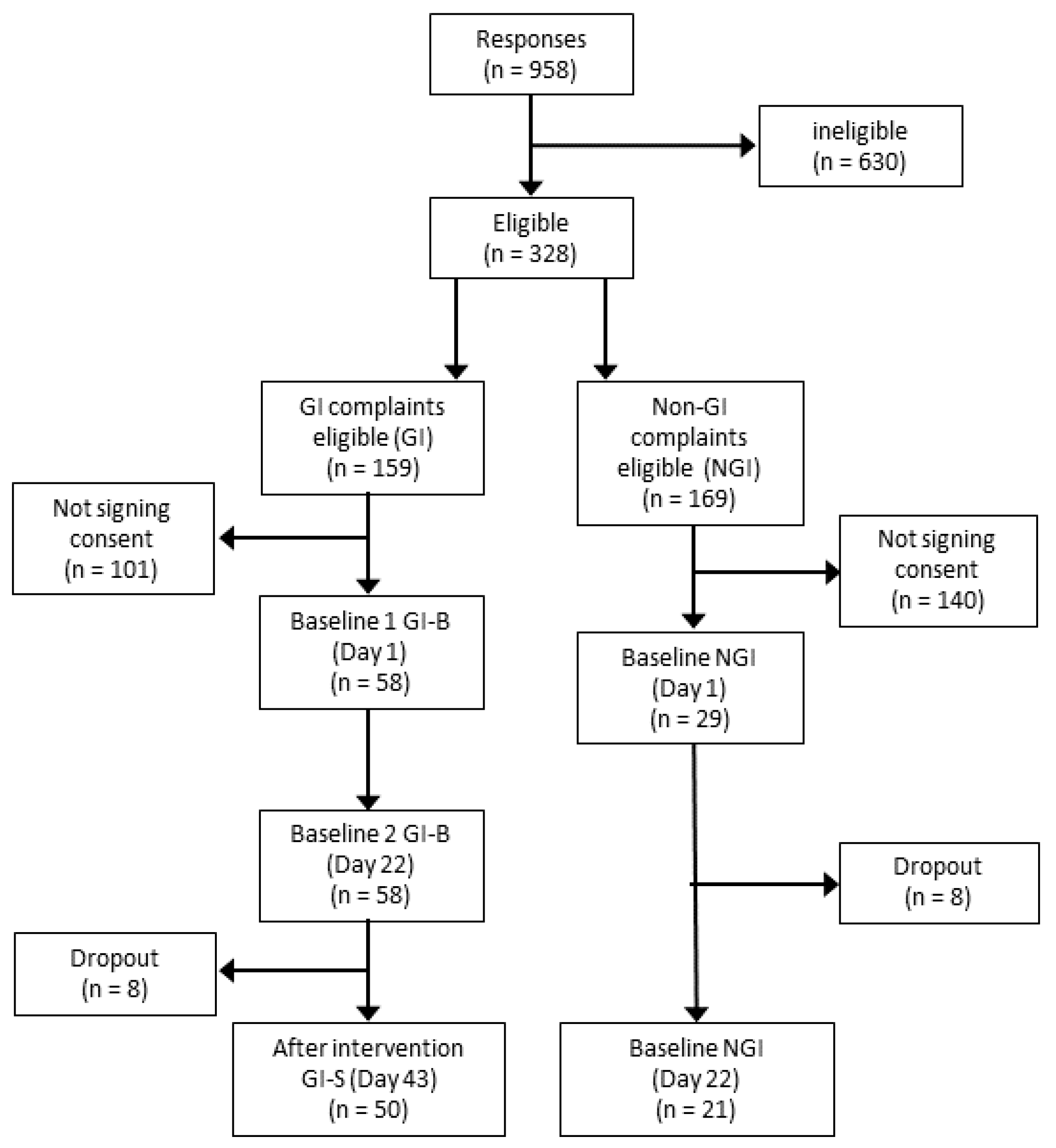
2.2. Study Participants
2.3. Dietary Intervention: Multi-Ingredient Supplement
2.4. Assessment of Body Composition
2.5. Measurement of Digestive Symptoms
2.6. Analysis of Gut Microbiota
2.6.1. Fecal Sample Collection and Storage
2.6.2. DNA Extraction and Analysis Methods
2.6.3. Microbiota Composition Outcomes
2.7. Measurements of Physical and Mental Wellbeing, Sleep Quality, and Total Mood Disturbance
2.7.1. Physical Wellbeing
2.7.2. Mental Wellbeing
2.7.3. Sleep Quality
2.7.4. Total Mood Disturbance
2.8. Assessments of Dietary Intake and Food Quality
2.9. Statistics
3. Results
3.1. Demographics
3.2. GI Complaints and Wellbeing
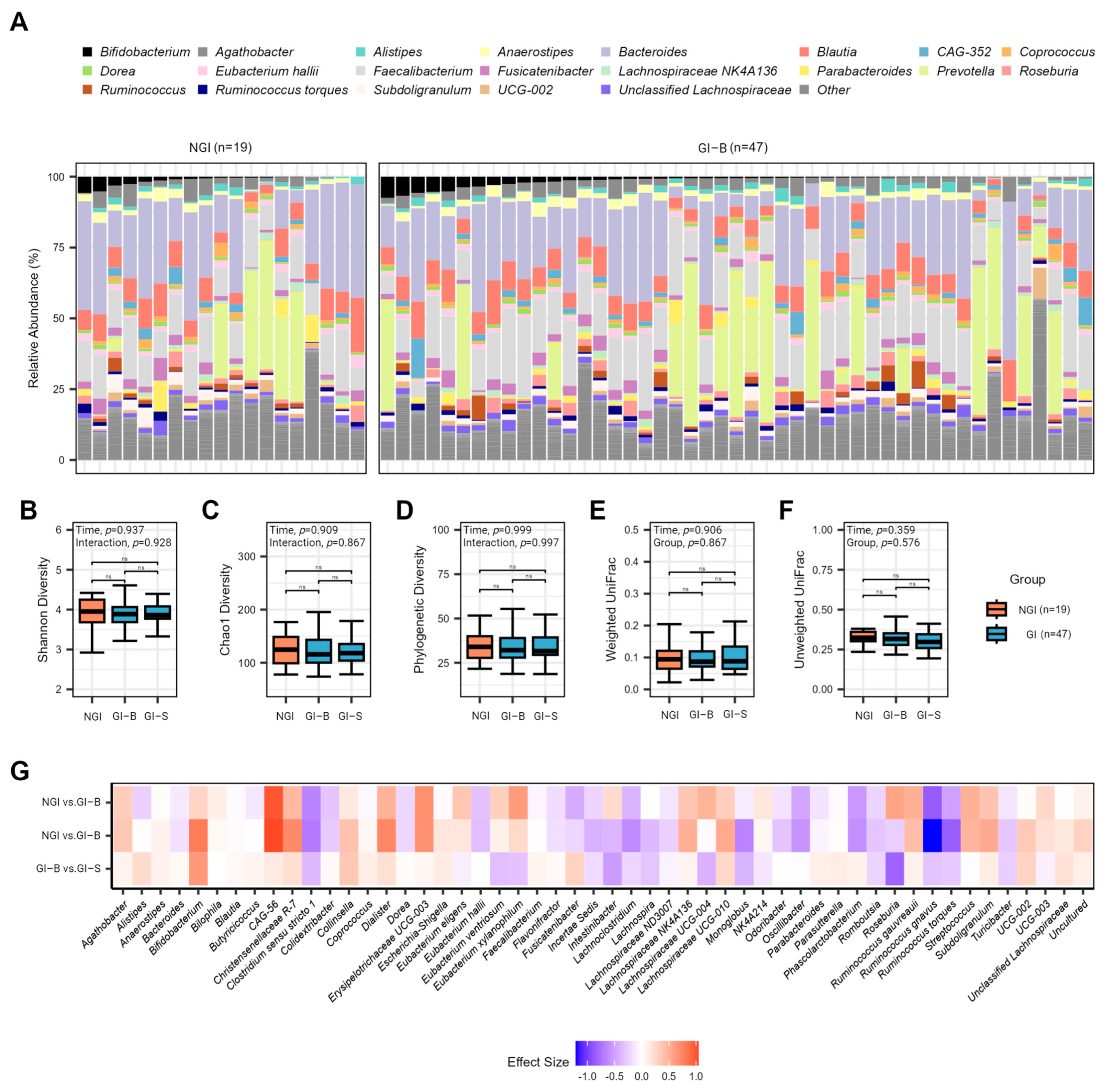
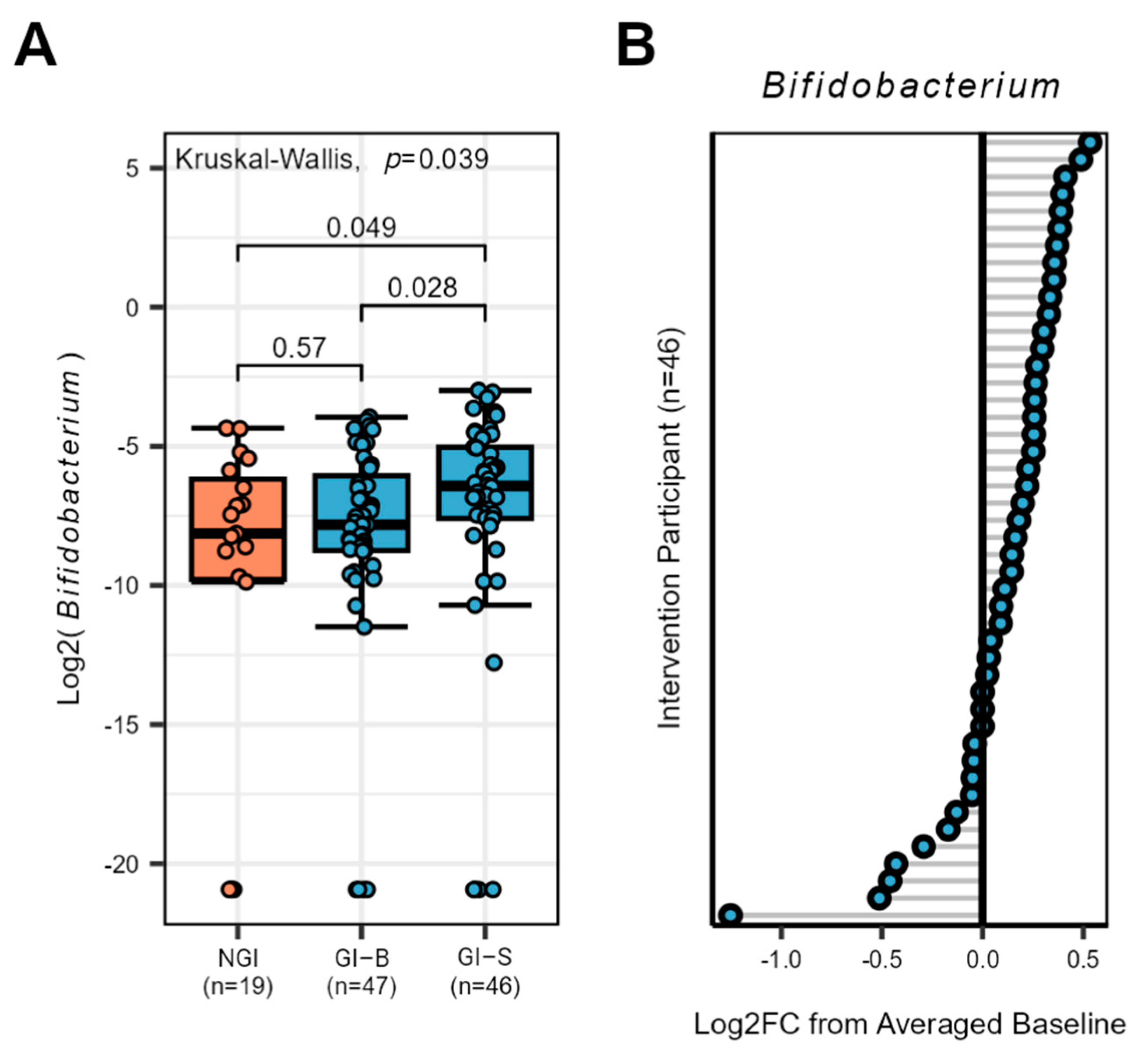
3.3. Gut Microbiota Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- De Oliveira, E.P.; Burini, R.C.; Jeukendrup, A. Gastrointestinal Complaints during Exercise: Prevalence, Etiology, and Nutritional Recommendations. Sports Med. 2014, 44, 79–85. [Google Scholar] [CrossRef]
- Pugh, J.N.; Fearn, R.; Morton, J.P.; Close, G.L. Gastrointestinal Symptoms in Elite Athletes: Time to Recognise the Problem? Br. J. Sports Med. 2018, 52, 487–488. [Google Scholar] [CrossRef]
- Chantler, S.; Wood-Martin, R.; Holliday, A.; Davison, G.; Crabtree, D.R.; Readhead, C.; Jones, B. The Frequency and Severity of Gastrointestinal Symptoms in Rugby Players. Int. J. Sports Med. 2024, 45, 323–331. [Google Scholar] [CrossRef]
- Wardenaar, F.C.; Schott, K.D.; Mohr, A.E.; Ortega-Santos, C.P.; Connolly, J.E. An Exploratory Study Investigating the Prevalence of Gastrointestinal Symptoms in Collegiate Division I American Football Athletes. Int. J. Environ. Res. Public Health 2023, 20, 6453. [Google Scholar] [CrossRef]
- Shaw, A.D.; Davies, G.J. Lactose Intolerance: Problems in Diagnosis and Treatment. J. Clin. Gastroenterol. 1999, 28, 208–216. [Google Scholar] [CrossRef] [PubMed]
- Swagerty, D.; Walling, A.; Klein, R. Lactose Intolerance. Am. Fam Physician 2002, 65, 1845–1851. [Google Scholar] [PubMed]
- Gaskell, S.K.; Taylor, B.; Muir, J.; Costa, R.J.S. Impact of 24-h High and Low Fermentable Oligo-, Di-, Monosaccharide, and Polyol Diets on Markers of Exercise-Induced Gastrointestinal Syndrome in Response to Exertional Heat Stress. Appl. Physiol. Nutr. Metab. 2020, 45, 569–580. [Google Scholar] [CrossRef]
- Snipe, R.M.J.; Khoo, A.; Kitic, C.M.; Gibson, P.R.; Costa, R.J.S. The Impact of Exertional-Heat Stress on Gastrointestinal Integrity, Gastrointestinal Symptoms, Systemic Endotoxin and Cytokine Profile. Eur. J. Appl. Physiol. 2018, 118, 389–400. [Google Scholar] [CrossRef]
- Kårlund, A.; Gómez-Gallego, C.; Turpeinen, A.M.; Palo-Oja, O.M.; El-Nezami, H.; Kolehmainen, M. Protein Supplements and Their Relation with Nutrition, Microbiota Composition and Health: Is More Protein Always Better for Sportspeople? Nutrients 2019, 11, 829. [Google Scholar] [CrossRef] [PubMed]
- Vento, K.A.; Wardenaar, F.C. Third-Party Testing Nutritional Supplement Knowledge, Attitudes, and Use among an NCAA I Collegiate Student-Athlete Population. Front Sports Act. Living 2020, 2, 115. [Google Scholar] [CrossRef]
- Wardenaar, F.C.; Ceelen, I.J.M.; Van Dijk, J.W.; Hangelbroek, R.W.J.; Van Roy, L.; Van Der Pouw, B.; De Vries, J.H.M.; Mensink, M.; Witkamp, R.F. Nutritional Supplement Use by Dutch Elite and Sub-Elite Athletes: Does Receiving Dietary Counselling Make a Difference? Int. J. Sport Nutr. Exerc. Metab. 2017, 27, 32–42. [Google Scholar] [CrossRef]
- King, A.J.; Etxebarria, N.; Ross, M.L.; Garvican-Lewis, L.; Heikura, I.A.; McKay, A.K.A.; Tee, N.; Forbes, S.F.; Beard, N.A.; Saunders, P.U.; et al. Short-Term Very High Carbohydrate Diet and Gut-Training Have Minor Effects on Gastrointestinal Status and Performance in Highly Trained Endurance Athletes. Nutrients 2022, 14, 1929. [Google Scholar] [CrossRef]
- Oliphant, K.; Allen-Vercoe, E. Macronutrient Metabolism by the Human Gut Microbiome: Major Fermentation by-Products and Their Impact on Host Health. Microbiome 2019, 7, 91. [Google Scholar] [CrossRef]
- Sekirov, I.; Russell, S.L.; Caetano M Antunes, L.; Finlay, B.B. Gut Microbiota in Health and Disease. Physiol. Rev. 2010, 90, 859–904. [Google Scholar] [CrossRef]
- Adak, A.; Khan, M.R. An Insight into Gut Microbiota and Its Functionalities. Cell. Mol. Life Sci. 2019, 76, 473–493. [Google Scholar] [CrossRef] [PubMed]
- Smith, K.A.; Pugh, J.N.; Duca, F.A.; Close, G.L.; Ormsbee, M.J. Gastrointestinal Pathophysiology during Endurance Exercise: Endocrine, Microbiome, and Nutritional Influences. Eur. J. Appl. Physiol. 2021, 121, 2657–2674. [Google Scholar] [CrossRef]
- Pugh, J.N.; Impey, S.G.; Doran, D.A.; Fleming, S.C.; Morton, J.P.; Close, G.L. Acute High-Intensity Interval Running Increases Markers of Gastrointestinal Damage and Permeability but Not Gastrointestinal Symptoms. Appl. Physiol. Nutr. Metab. 2017, 42, 941–947. [Google Scholar] [CrossRef] [PubMed]
- Zuhl, M.; Schneider, S.; Lanphere, K.; Conn, C.; Dokladny, K.; Moseley, P. Exercise Regulation of Intestinal Tight Junction Proteins. Br. J. Sports Med. 2014, 48, 980–986. [Google Scholar] [CrossRef] [PubMed]
- Jeukendrup, A.E.; Vet-Joop, K.; Sturk, A.; Stegen, J.H.J.C.; Senden, J.; Saris, W.H.M.; Wagenmakers, A.J.M. Relationship between Gastro-Intestinal Complaints and Endotoxaemia, Cytokine Release and the Acute-Phase Reaction during and after a Long-Distance Triathlon in Highly Trained Men. Clin. Sci. 2000, 98, 47–55. [Google Scholar] [CrossRef]
- Lamprecht, M.; Frauwallner, A. Exercise, Intestinal Barrier Dysfunction and Probiotic Supplementation. Med. Sport Sci. 2012, 59, 47–56. [Google Scholar] [CrossRef]
- Crowson, M.M.; McClave, S.A. Does the Intestinal Microbiome Impact Athletic Performance? Curr. Gastroenterol. Rep. 2020, 22, 53. [Google Scholar] [CrossRef]
- Engel, S.; Mortensen, B.; Wellejus, A.; Vera-Jimenez, N.; Struve, C.; Brummer, R.J.; Damholt, A.; Woods, T.; Shanahan, F. Safety of Bifidobacterium Breve, Bif195, Employing a Human Exercise-Induced Intestinal Permeability Model: A Randomised, Double-Blinded, Placebo-Controlled, Parallel Group Trial. Benef. Microbes 2022, 13, 243–252. [Google Scholar] [CrossRef]
- Łagowska, K.; Bajerska, J.; Kamiński, S.; Del Bo’, C. Effects of Probiotics Supplementation on Gastrointestinal Symptoms in Athletes: A Systematic Review of Randomized Controlled Trials. Nutrients 2022, 14, 2645. [Google Scholar] [CrossRef] [PubMed]
- Smarkusz-Zarzecka, J.; Ostrowska, L.; Leszczyńska, J.; Cwalina, U. Effect of a Multi-Strain Probiotic Supplement on Gastrointestinal Symptoms and Serum Biochemical Parameters of Long-Distance Runners: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2022, 19, 9363. [Google Scholar] [CrossRef] [PubMed]
- Rauch, C.E.; Mika, A.S.; McCubbin, A.J.; Huschtscha, Z.; Costa, R.J.S. Effect of Prebiotics, Probiotics, and Synbiotics on Gastrointestinal Outcomes in Healthy Adults and Active Adults at Rest and in Response to Exercise—A Systematic Literature Review. Front. Nutr. 2022, 9, 2981. [Google Scholar] [CrossRef] [PubMed]
- Davis, L.M.G.; Martínez, I.; Walter, J.; Hutkins, R. A Dose Dependent Impact of Prebiotic Galactooligosaccharides on the Intestinal Microbiota of Healthy Adults. Int. J. Food Microbiol. 2010, 144, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Mysonhimer, A.R.; Cannavale, C.N.; Bailey, M.A.; Khan, N.A.; Holscher, H.D. Prebiotic Consumption Alters Microbiota but Not Biological Markers of Stress and Inflammation or Mental Health Symptoms in Healthy Adults: A Randomized, Controlled, Crossover Trial. J. Nutr. 2023, 153, 1283–1296. [Google Scholar] [CrossRef] [PubMed]
- Khan, R.; Shah, M.D.; Shah, L.; Lee, P.C.; Khan, I. Bacterial Polysaccharides—A Big Source for Prebiotics and Therapeutics. Front. Nutr. 2022, 9, 2631. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Pérez, D.; Bressa, C.; Bailén, M.; Hamed-Bousdar, S.; Naclerio, F.; Carmona, M.; Pérez, M.; González-Soltero, R.; Montalvo-Lominchar, M.G.; Carabaña, C.; et al. Effect of a Protein Supplement on the Gut Microbiota of Endurance Athletes: A Randomized, Controlled, Double-Blind Pilot Study. Nutrients 2018, 10, 337. [Google Scholar] [CrossRef]
- Horstman, A.M.H.; Ganzevles, R.A.; Kudla, U.; Kardinaal, A.F.M.; van den Borne, J.J.G.C.; Huppertz, T. Postprandial Blood Amino Acid Concentrations in Older Adults after Consumption of Dairy Products: The Role of the Dairy Matrix. Int. Dairy J. 2021, 113, 104890. [Google Scholar] [CrossRef]
- Smith, N.M.; Maloney, N.G.; Shaw, S.; Horgan, G.W.; Fyfe, C.; Martin, J.C.; Suter, A.; Scott, K.P.; Johnstone, A.M. Daily Fermented Whey Consumption Alters the Fecal Short-Chain Fatty Acid Profile in Healthy Adults. Front. Nutr. 2020, 7, 165. [Google Scholar] [CrossRef]
- Zeng, J.; Jiang, J.; Zhu, W.; Chu, Y. Heat-Killed Yogurt-Containing Lactic Acid Bacteria Prevent Cytokine-Induced Barrier Disruption in Human Intestinal Caco-2 Cells. Ann. Microbiol. 2016, 66, 171–178. [Google Scholar] [CrossRef]
- Gao, J.; Li, Y.; Wan, Y.; Hu, T.; Liu, L.; Yang, S.; Gong, Z.; Zeng, Q.; Wei, Y.; Yang, W.; et al. A Novel Postbiotic from Lactobacillus Rhamnosus GG with a Beneficial Effect on Intestinal Barrier Function. Front. Microbiol. 2019, 10, 477. [Google Scholar] [CrossRef] [PubMed]
- Rul, F.; Béra-Maillet, C.; Champomier-Vergès, M.C.; El-Mecherfi, K.E.; Foligné, B.; Michalski, M.C.; Milenkovic, D.; Savary-Auzeloux, I. Underlying Evidence for the Health Benefits of Fermented Foods in Humans. Food Funct. 2022, 13, 4804–4824. [Google Scholar] [CrossRef]
- Ağagündüz, D.; Yılmaz, B.; Şahin, T.Ö.; Güneşliol, B.E.; Ayten, Ş.; Russo, P.; Spano, G.; Rocha, J.M.; Bartkiene, E.; Özogul, F. Dairy Lactic Acid Bacteria and Their Potential Function in Dietetics: The Food-Gut-Health Axis. Foods 2021, 10, 3099. [Google Scholar] [CrossRef] [PubMed]
- Harnett, J.E.; Pyne, D.B.; McKune, A.J.; Penm, J.; Pumpa, K.L. Probiotic Supplementation Elicits Favourable Changes in Muscle Soreness and Sleep Quality in Rugby Players. J. Sci. Med. Sport 2021, 24, 195–199. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, F.; Yamaguchi, T.; Hu, A.; Kobayashi, A.; Kobayashi, H. Effects of Fiber Supplementation for Four Weeks on Athletic Performance in Japanese College Athletes: A Case Study—Measurement of the Athletic Performance, Salivary Biomarkers of Stress, and Mood, Affect Balance. Health 2017, 09, 556–567. [Google Scholar] [CrossRef]
- Zhu, J.; Zhu, Y.; Song, G. Effect of Probiotic Yogurt Supplementation (Bifidobacterium Animalis Ssp. Lactis BB-12) on Gut Microbiota of Female Taekwondo Athletes and Its Relationship with Exercise-Related Psychological Fatigue. Microorganisms 2023, 11, 1403. [Google Scholar] [CrossRef] [PubMed]
- Costa, R.J.S.; Snipe, R.M.J.; Kitic, C.M.; Gibson, P.R. Systematic Review: Exercise-Induced Gastrointestinal Syndrome—Implications for Health and Intestinal Disease. Aliment. Pharmacol. Ther. 2017, 46, 246–265. [Google Scholar] [CrossRef]
- Pugh, J.N.; Sparks, A.S.; Doran, D.A.; Fleming, S.C.; Langan-Evans, C.; Kirk, B.; Fearn, R.; Morton, J.P.; Close, G.L. Four Weeks of Probiotic Supplementation Reduces GI Symptoms during a Marathon Race. Eur. J. Appl. Phys. 2019, 119, 1491–1501. [Google Scholar] [CrossRef]
- Hozo, S.P.; Djulbegovic, B.; Hozo, I. Estimating the Mean and Variance from the Median, Range, and the Size of a Sample. BMC Med. Res. Methodol. 2005, 5, 13. [Google Scholar] [CrossRef]
- Dimenäs, E.; Glise, H.; Hallerbäck, B.; Hernqvist, H.; Svedlund, J.; Wiklund, I. Well-Being and Gastrointestinal Symptoms among Patients Referred to Endoscopy Owing to Suspected Duodenal Ulcer. Scand. J. Gastroenterol. 1995, 30, 1046–1052. [Google Scholar] [CrossRef] [PubMed]
- Wiklund, I.K.; Junghard, O.; Grace, E.; Talley, N.J.; Kamm, M.; Van Zanten, S.V.; Paré, P.; Chiba, N.; Leddin, D.S.; Bigard, M.A.; et al. Quality of Life in Reflux and Dyspepsia Patients. Psychometric Documentation of a New Disease-Specific Questionnaire (QOLRAD). Eur. J. Surg. Suppl. 1998, 164, 41–49. [Google Scholar] [CrossRef]
- Svedlund, J.; Sjödin, I.; Dotevall, G. GSRS—A Clinical Rating Scale for Gastrointestinal Symptoms in Patients with Irritable Bowel Syndrome and Peptic Ulcer Disease. Dig. Dis. Sci. 1988, 33, 129–134. [Google Scholar] [CrossRef]
- Klindworth, A.; Pruesse, E.; Schweer, T.; Peplies, J.; Quast, C.; Horn, M.; Glöckner, F.O. Evaluation of General 16S Ribosomal RNA Gene PCR Primers for Classical and Next-Generation Sequencing-Based Diversity Studies. Nucleic Acids Res. 2013, 41, e1. [Google Scholar] [CrossRef] [PubMed]
- Edgar, R.C. Search and Clustering Orders of Magnitude Faster than BLAST. Bioinformatics 2010, 26, 2460–2461. [Google Scholar] [CrossRef] [PubMed]
- Zaharia, M.; Bolosky, W.J.; Curtis, K.; Fox, A.; Patterson, D.; Shenker, S.; Stoica, I.; Karp, R.M.; Sittler, T. Faster and More Accurate Sequence Alignment with SNAP. arXiv 2011, arXiv:1111.5572. [Google Scholar] [CrossRef]
- Cole, J.R.; Wang, Q.; Fish, J.A.; Chai, B.; McGarrell, D.M.; Sun, Y.; Brown, C.T.; Porras-Alfaro, A.; Kuske, C.R.; Tiedje, J.M. Ribosomal Database Project: Data and Tools for High Throughput RRNA Analysis. Nucleic Acids Res. 2014, 42, D633–D642. [Google Scholar] [CrossRef] [PubMed]
- Kaehler, B.D.; Bokulich, N.A.; McDonald, D.; Knight, R.; Caporaso, J.G.; Huttley, G.A. Species Abundance Information Improves Sequence Taxonomy Classification Accuracy. Nat. Commun. 2019, 10, 4643. [Google Scholar] [CrossRef]
- Quast, C.; Pruesse, E.; Yilmaz, P.; Gerken, J.; Schweer, T.; Yarza, P.; Peplies, J.; Glöckner, F.O. The SILVA Ribosomal RNA Gene Database Project: Improved Data Processing and Web-Based Tools. Nucleic Acids Res. 2013, 41, D590–D596. [Google Scholar] [CrossRef]
- McKnight, D.T.; Huerlimann, R.; Bower, D.S.; Schwarzkopf, L.; Alford, R.A.; Zenger, K.R. Methods for Normalizing Microbiome Data: An Ecological Perspective. Methods Ecol. Evol. 2019, 10, 389–400. [Google Scholar] [CrossRef]
- Schat, A.C.H.; Kelloway, E.K.; Desmarais, S. The Physical Health Questionnaire (PHQ): Construct Validation of a Self-Report Scale of Somatic Symptoms. J. Occup. Health Psychol. 2005, 10, 363–381. [Google Scholar] [CrossRef] [PubMed]
- Prochaska, J.J.; Sung, H.Y.; Max, W.; Shi, Y.; Ong, M. Validity Study of the K6 Scale as a Measure of Moderate Mental Distress Based on Mental Health Treatment Need and Utilization. Int. J. Methods Psychiatr. Res. 2012, 21, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. The Diagnostic Validity of the Athens Insomnia Scale. J. Psychosom. Res. 2003, 55, 263–267. [Google Scholar] [CrossRef]
- Heuchert, J.; McNair, D. Profile of Mood States, 2nd ed.; APA PsycNet: Washington, DC, USA, 2023. [Google Scholar]
- Subar, A.F.; Kirkpatrick, S.I.; Mittl, B.; Zimmerman, T.P.; Thompson, F.E.; Bingley, C.; Willis, G.; Islam, N.G.; Baranowski, T.; McNutt, S.; et al. The Automated Self-Administered 24-Hour Dietary Recall (ASA24): A Resource for Researchers, Clinicians, and Educators from the National Cancer Institute. J. Acad. Nutr. Diet. 2012, 112, 1134–1137. [Google Scholar] [CrossRef] [PubMed]
- Vento, K.A.; Delgado, F.; Skinner, J.; Wardenaar, F. Funding and College-Provided Nutritional Resources on Diet Quality among Female Athletes. J. Am. Coll. Health 2021, 71, 1732–1739. [Google Scholar] [CrossRef]
- Richardson, J.T.E. Eta squared and partial eta squared as measures of effect size in educational research. Educ. Res. Rev. 2011, 6, 135–147. [Google Scholar] [CrossRef]
- Mohr, A.E.; Jasbi, P.; Bowes, D.A.; Dirks, B.; Whisner, C.M.; Arciero, K.M.; Poe, M.; Gu, H.; Gumpricht, E.; Sweazea, K.L.; et al. Exploratory Analysis of One versus Two-Day Intermittent Fasting Protocols on the Gut Microbiome and Plasma Metabolome in Adults with Overweight/Obesity. Front. Nutr. 2022, 9, 2546. [Google Scholar] [CrossRef]
- Lin, H.; Peddada, S. Das Analysis of Compositions of Microbiomes with Bias Correction. Nat. Commun. 2020, 11, 3514. [Google Scholar] [CrossRef]
- Wilson, P.B.; Fearn, R.; Pugh, J. Occurrence and Impacts of Gastrointestinal Symptoms in Team-Sport Athletes: A Preliminary Survey. Clin. J. Sport Med. 2023, 33, 239–245. [Google Scholar] [CrossRef]
- Schoemaker, M.H.; Hageman, J.H.J.; Ten Haaf, D.; Hartog, A.; Scholtens, P.A.M.J.; Boekhorst, J.; Nauta, A.; Bos, R. Prebiotic Galacto-Oligosaccharides Impact Stool Frequency and Fecal Microbiota in Self-Reported Constipated Adults: A Randomized Clinical Trial. Nutrients 2022, 14, 309. [Google Scholar] [CrossRef] [PubMed]
- Costa, R.J.S.; Miall, A.; Khoo, A.; Rauch, C.; Snipe, R.; Camões-Costa, V.; Gibson, P. Gut-Training: The Impact of Two Weeks Repetitive Gut-Challenge during Exercise on Gastrointestinal Status, Glucose Availability, Fuel Kinetics, and Running Performance. Appl. Physiol. Nutr. Metab. 2017, 42, 547–557. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, M.I.; Mikhail, A.; Lan, L.; Di Carlo, A.; Hamilton, B.; Barnard, K.; Hettinga, B.P.; Hatcher, E.; Tarnopolsky, M.G.; Nederveen, J.P.; et al. A Five-Ingredient Nutritional Supplement and Home-Based Resistance Exercise Improve Lean Mass and Strength in Free-Living Elderly. Nutrients 2020, 12, 2391. [Google Scholar] [CrossRef] [PubMed]
- Nagpal, R.; Mainali, R.; Ahmadi, S.; Wang, S.; Singh, R.; Kavanagh, K.; Kitzman, D.W.; Kushugulova, A.; Marotta, F.; Yadav, H. Gut Microbiome and Aging: Physiological and Mechanistic Insights. Nutr. Health Aging 2018, 4, 267–285. [Google Scholar] [CrossRef] [PubMed]
- Suda, K.; Matsuda, K. How Microbes Affect Depression: Underlying Mechanisms via the Gut–Brain Axis and the Modulating Role of Probiotics. Int. J. Mol. Sci. 2022, 23, 1172. [Google Scholar] [CrossRef] [PubMed]
- Guo, C.; Huo, Y.-J.; Li, Y.; Han, Y.; Zhou, D. Gut-Brain Axis: Focus on Gut Metabolites Short-Chain Fatty Acids. World J. Clin. Cases 2022, 10, 1754–1763. [Google Scholar] [CrossRef] [PubMed]
- Fullerton, D.J.; Zhang, L.M.; Kleitman, S. An Integrative Process Model of Resilience in an Academic Context: Resilience Resources, Coping Strategies, and Positive Adaptation. PLoS ONE 2021, 16, e0246000. [Google Scholar] [CrossRef]
- Liu, R.T.; Walsh, R.F.L.; Sheehan, A.E. Prebiotics and Probiotics for Depression and Anxiety: A Systematic Review and Meta-Analysis of Controlled Clinical Trials. Neurosci. Biobehav. Rev. 2019, 102, 13–23. [Google Scholar] [CrossRef] [PubMed]
- Freijy, T.M.; Cribb, L.; Oliver, G.; Metri, N.J.; Opie, R.S.; Jacka, F.N.; Hawrelak, J.A.; Rucklidge, J.J.; Ng, C.H.; Sarris, J. Effects of a High-Prebiotic Diet versus Probiotic Supplements versus Synbiotics on Adult Mental Health: The “Gut Feelings” Randomised Controlled Trial. Front. Neurosci. 2023, 16, 1097278. [Google Scholar] [CrossRef] [PubMed]
- Mutoh, N.; Kakiuchi, I.; Hiraku, A.; Iwabuchi, N.; Kiyosawa, K.; Igarashi, K.; Tanaka, M.; Nakamura, M.; Miyasaka, M. Heat-Killed Lactobacillus Helveticus Improves Mood States: A Randomised, Double-Blind, Placebo-Controlled Study. Benef. Microbes 2023, 14, 109–117. [Google Scholar] [CrossRef]
- Axling, U.; Önning, G.; Combs, M.A.; Bogale, A.; Högström, M.; Svensson, M. The Effect of Lactobacillus Plantarum 299v on Iron Status and Physical Performance in Female Iron-Deficient Athletes: A Randomized Controlled Trial. Nutrients 2020, 12, 1279. [Google Scholar] [CrossRef]
- Murata, M.; Kondo, J.; Iwabuchi, N.; Takahashi, S.; Yamauchi, K.; Abe, F.; Miura, K. Effects of Paraprobiotic Lactobacillus Paracasei MCC1849 Supplementation on Symptoms of the Common Cold and Mood States in Healthy Adults. Benef. Microbes 2018, 9, 855–864. [Google Scholar] [CrossRef]
- Vulevic, J.; Tzortzis, G.; Juric, A.; Gibson, G.R. Effect of a Prebiotic Galactooligosaccharide Mixture (B-GOS®) on Gastrointestinal Symptoms in Adults Selected from a General Population Who Suffer with Bloating, Abdominal Pain, or Flatulence. Neurogastroenterol. Motil. 2018, 30, e13440. [Google Scholar] [CrossRef]
- Johnstone, N.; Milesi, C.; Burn, O.; van den Bogert, B.; Nauta, A.; Hart, K.; Sowden, P.; Burnet, P.W.; Kadosh, K.C. Anxiolytic Effects of a Galacto-Oligosaccharides Prebiotic in Healthy Female Volunteers Are Associated with Reduced Negative Bias and the Gut Bacterial Composition. medRxiv 2019, 19011403. [Google Scholar] [CrossRef]
- Ma, C.; Wasti, S.; Huang, S.; Zhang, Z.; Mishra, R.; Jiang, S.; You, Z.; Wu, Y.; Chang, H.; Wang, Y.; et al. The Gut Microbiome Stability Is Altered by Probiotic Ingestion and Improved by the Continuous Supplementation of Galactooligosaccharide. Gut Microbes 2020, 12, 1785252. [Google Scholar] [CrossRef]
- Schaafsma, A.; Mallee, L.; van den Belt, M.; Floris, E.; Kortman, G.; Veldman, J.; van den Ende, D.; Kardinaal, A. The Effect of a Whey-Protein and Galacto-Oligosaccharides Based Product on Parameters of Sleep Quality, Stress, and Gut Microbiota in Apparently Healthy Adults with Moderate Sleep Disturbances: A Randomized Controlled Cross-over Study. Nutrients 2021, 13, 2204. [Google Scholar] [CrossRef] [PubMed]
- Krumbeck, J.A.; Rasmussen, H.E.; Hutkins, R.W.; Clarke, J.; Shawron, K.; Keshavarzian, A.; Walter, J. Probiotic Bifidobacterium Strains and Galactooligosaccharides Improve Intestinal Barrier Function in Obese Adults but Show No Synergism When Used Together as Synbiotics. Microbiome 2018, 6, 121. [Google Scholar] [CrossRef]
- Widyastuti, Y.; Febrisiantosa, A.; Tidona, F. Health-Promoting Properties of Lactobacilli in Fermented Dairy Products. Front. Microbiol. 2021, 12, 673890. [Google Scholar] [CrossRef]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; MacEra, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical Activity and Public Health: Updated Recommendation for Adults from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef] [PubMed]
- Thomas, D.T.; Erdman, K.A.; Burke, L.M. Position of the Academy of Nutrition and Dietetics, Dietitians of Canada, and the American College of Sports Medicine: Nutrition and Athletic Performance. J. Acad. Nutr. Diet. 2016, 116, 501–528. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Individual Variables | NGI (n = 21) | GI-B and GI-S (n = 50) | p-Value |
|---|---|---|---|
| Age | |||
| Years | 25.7 ± 4.7 | 26.6 ± 5.4 | 0.60 |
| Sex | |||
| Male, % (n) | 52 (11) | 66 (33) | 0.24 |
| Female, % (n) | 48 (10) | 32 (16) | |
| Intersex, % (n) | 0 (0) | 2 (1) | |
| Baseline demographics | |||
| Age, years (mean ± SD) | 26.6 ± 5.42 | 25.7 ± 4.66 | 0.60 |
| BMI, kg/m2 (mean ± SD) | 25.1 ± 3.89 | 25.1 ± 3.51 | 0.78 |
| Height, cm (mean ± SD) | 171 ± 7.96 | 174 ± 10.3 | 0.21 |
| Body weight, kg (mean ± SD) | 74.0 ± 15.3 | 76.6 ± 15.3 | 0.65 |
| Waist-to-hip ratio (mean ± SD) | 0.93 ± 0.20 | 0.87 ± 0.13 | 0.25 |
| Ethnicity | |||
| Hispanic/Latino, % (n) | 14 (3) | 18 (9) | 0.70 |
| Non-Hispanic/Latino, % (n) | 86 (18) | 82 (41) | |
| Race * | |||
| White, % (n) | 86 (18) | 78 (39) | 0.46 |
| Black/African American, % (n) | 5 (1) | 4 (2) | 0.88 |
| Asian/Asian American, % (n) | 29 (6) | 10 (5) | 0.05 |
| Native American, % (n) | 5 (1) | 4 (2) | 0.88 |
| Pacific Islander, % (n) | 5 (1) | 2 (1) | 0.52 |
| Indian, % (n) | 0 (0) | 2 (1) | 0.51 |
| Other, % (n) | 0 (0) | 4 (2) | 0.35 |
| Sports * | |||
| Team sports, % (n) | 14 (3) | 42 (21) | 0.02 |
| Weight training, % (n) | 42 (9) | 40 (20) | 0.75 |
| Track and field/Endurance, % (n) | 19 (4) | 12 (6) | 0.41 |
| Others, % (n) | 24 (5) | 6 (3) | 0.01 |
| Baseline (Day 1 and Day 22) | Comparing Baseline between Groups | Day 43 (after Supplementation) | Comparing Baseline vs. Day 43 in GI Group | ||||
|---|---|---|---|---|---|---|---|
| NGI (n = 21) | GI-B (n = 50) | F-Value | p-Value and η2 | GI-S (n = 50) | F-Value | p-Value and η2 | |
| GSRS (total) | 24.1 ± 8.48 21.0 (17.0–29.5) | 30.3 ± 8.82 29.8 (23.8–35.6) | 7.46 | 0.008 η2 = 0.10 | 27.2 ± 8.24 25.5 (21.0–30.3) | 3.22 | 0.076 η2 = 0.03 |
| PHQ | 33.9 ± 10.7 32.5 (25.3–41.0) | 38.5 ± 9.68 38.5 (29.5–45.5) | 3.13 | 0.081 η2 = 0.04 | 33.3 ± 10.7 32.0 (25.0–42.5) | 6.97 | 0.010 η2 = 0.06 |
| K6 | 4.07 ± 3.79 4.00 (1.00–4.75) | 4.67 ± 3.18 4.25 (2.50–6.63) | 0.47 | 0.497 η2 = 0.01 | 3.96 ± 3.60 3.00 (1.00–5.25) | 1.11 | 0.295 η2 = 0.01 |
| AIS-8 | 5.43 ± 4.23 4.00 (3.00–7.50) | 5.24 ± 3.69 4.50 (2.50–7.63) | 0.03 | 0.857 η2 = 0.001 | 4.36 ± 3.68 3.00 (1.75–6.25) | 1.46 | 0.230 η2 = 0.01 |
| POMS (total mood disturbance) | 10.1 ± 16.1 4.00 (−0.75–17.0) | 10.4 ± 12.1 8.50 (2.88–14.3) | 0.01 | 0.942 η2 < 0.001 | 9.00 ± 13.3 3.00 (−1.00–16.3) | 0.28 | 0.595 η2 < 0.01 |
| REAP (food-quality score) | 57.4 ± 4.75 57.0 (54.3–61.5) | 57.7 ± 5.43 57.0 (54.8–62.5) | 0.06 | 0.808 η2 = 0.001 | 58.2 ± 6.62 60.0 (53.8–63.0) | 0.16 | 0.687 η2 < 0.01 |
| Energy (Kcal—ASA24) | 2043 ± 1029 1814 (1268–2309) | 2681 ± 1430 2453 (1837–3115) | 2.57 | 0.114 η2 = 0.07 | 2641 ± 1077 2507 (1860–3557) | 0.04 | 0.838 η2 < 0.001 |
| Protein (g—ASA24) | 101 ± 46.7 84.9 (65.3–129) | 157 ± 98.7 125 (97.2–197) | 5.53 | 0.022 η2 = 0.13 | 138 ± 68.5 128 (91.0–169) | 1.28 | 0.261 η2 = 0.01 |
| Protein (g/kg) | 1.42 ± 0.44 1.26 (1.10–1.77) | 1.96 ± 0.80 1.85 (1.28–2.50) | 5.62 | 0.021 η2 = 0.08 | 1.77 ± 0.79 1.72 (1.27–2.17) | 1.69 | 0.198 η2 = 0.02 |
| Protein (En%) | 21.7 ± 7.31 22.0 (15.0–25.0) | 23.1 ± 5.18 22.0 (20.0–25.0) | 0.82 | 0.368 η2 = 0.01 | 21.2 ± 7.12 21.0 (16.0–25.0) | 1.91 | 0.170 η2 = 0.02 |
| Fiber (g—ASA24) | 16.4 ± 6.60 16.3 (11.0–22.0) | 22.2 ± 10.2 22.1 (14.5–27.6) | 4.57 | 0.036 η2 = 0.10 | 22.8 ± 10.3 22.0 (16.2–27.7) | 0.05 | 0.816 η2 < 0.01 |
| NGI (n = 21) | GI-B (n = 50) | GI-S (n = 50) | |||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
| Upper abdominal pain | 81 | 10 | 5 | 10 | 5 | 0 | 0 | 28 | 30 | 16 | 20 | 4 | 2 | 0 | 46 | 32 | 12 | 10 | 0 | 0 | 0 |
| Heartburn | 90 | 5 | 5 | 5 | 5 | 0 | 0 | 74 | 18 | 2 | 4 | 2 | 0 | 0 | 88 | 6 | 4 | 0 | 2 | 0 | 0 |
| Acid reflux | 76 | 14 | 5 | 5 | 5 | 5 | 0 | 64 | 26 | 6 | 0 | 2 | 2 | 0 | 80 | 10 | 8 | 2 | 0 | 0 | 0 |
| Hunger | 52 | 38 | 10 | 10 | 0 | 0 | 0 | 22 | 36 | 20 | 18 | 4 | 0 | 0 | 50 | 24 | 12 | 8 | 6 | 0 | 0 |
| Nausea | 71 | 24 | 10 | 5 | 0 | 0 | 0 | 42 | 38 | 10 | 8 | 0 | 2 | 0 | 68 | 10 | 14 | 6 | 2 | 0 | 0 |
| Rumbling | 62 | 24 | 14 | 5 | 0 | 0 | 0 | 18 | 38 | 32 | 12 | 0 | 0 | 0 | 38 | 30 | 22 | 6 | 4 | 0 | 0 |
| Bloated | 48 | 24 | 10 | 14 | 10 | 0 | 0 | 12 | 22 | 14 | 30 | 12 | 10 | 0 | 28 | 22 | 22 | 24 | 2 | 2 | 0 |
| Burping | 67 | 14 | 12 | 5 | 5 | 0 | 0 | 38 | 34 | 22 | 4 | 2 | 0 | 0 | 60 | 26 | 8 | 4 | 2 | 0 | 0 |
| Gas/flatus | 48 | 19 | 19 | 14 | 5 | 5 | 0 | 6 | 32 | 20 | 24 | 16 | 2 | 0 | 22 | 24 | 32 | 16 | 2 | 0 | 4 |
| Constipation | 71 | 14 | 14 | 5 | 5 | 0 | 0 | 44 | 24 | 16 | 8 | 6 | 2 | 0 | 54 | 14 | 18 | 8 | 6 | 0 | 0 |
| Diarrhea | 76 | 10 | 14 | 0 | 5 | 5 | 0 | 50 | 20 | 10 | 14 | 6 | 0 | 0 | 58 | 20 | 12 | 6 | 4 | 0 | 0 |
| Loose stools | 71 | 14 | 10 | 10 | 0 | 0 | 0 | 66 | 12 | 12 | 8 | 0 | 2 | 0 | 80 | 10 | 8 | 2 | 0 | 0 | 0 |
| Hard stools | 81 | 10 | 10 | 5 | 0 | 0 | 0 | 54 | 26 | 16 | 2 | 2 | 0 | 0 | 70 | 18 | 6 | 6 | 0 | 0 | 0 |
| Urgent need to defecate | 71 | 19 | 5 | 10 | 0 | 0 | 0 | 52 | 28 | 10 | 8 | 0 | 2 | 0 | 66 | 18 | 8 | 4 | 2 | 0 | 2 |
| Incomplete evacuation | 67 | 19 | 14 | 10 | 0 | 0 | 0 | 22 | 30 | 22 | 20 | 0 | 6 | 0 | 44 | 22 | 24 | 4 | 4 | 2 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wardenaar, F.C.; Mohr, A.E.; Ortega-Santos, C.P.; Nyakayiru, J.; Kersch-Counet, C.; Chan, Y.; Clear, A.-M.; Kurka, J.; Schott, K.D.; Seltzer, R.G.N. Explorative Characterization of GI Complaints, General Physical and Mental Wellbeing, and Gut Microbiota in Trained Recreative and Competitive Athletes with or without Self-Reported Gastrointestinal Symptoms. Nutrients 2024, 16, 1712. https://doi.org/10.3390/nu16111712
Wardenaar FC, Mohr AE, Ortega-Santos CP, Nyakayiru J, Kersch-Counet C, Chan Y, Clear A-M, Kurka J, Schott KD, Seltzer RGN. Explorative Characterization of GI Complaints, General Physical and Mental Wellbeing, and Gut Microbiota in Trained Recreative and Competitive Athletes with or without Self-Reported Gastrointestinal Symptoms. Nutrients. 2024; 16(11):1712. https://doi.org/10.3390/nu16111712
Chicago/Turabian StyleWardenaar, Floris C., Alex E. Mohr, Carmen P. Ortega-Santos, Jean Nyakayiru, Christine Kersch-Counet, Yat Chan, Anna-Marie Clear, Jonathan Kurka, Kinta D. Schott, and Ryan G. N. Seltzer. 2024. "Explorative Characterization of GI Complaints, General Physical and Mental Wellbeing, and Gut Microbiota in Trained Recreative and Competitive Athletes with or without Self-Reported Gastrointestinal Symptoms" Nutrients 16, no. 11: 1712. https://doi.org/10.3390/nu16111712
APA StyleWardenaar, F. C., Mohr, A. E., Ortega-Santos, C. P., Nyakayiru, J., Kersch-Counet, C., Chan, Y., Clear, A.-M., Kurka, J., Schott, K. D., & Seltzer, R. G. N. (2024). Explorative Characterization of GI Complaints, General Physical and Mental Wellbeing, and Gut Microbiota in Trained Recreative and Competitive Athletes with or without Self-Reported Gastrointestinal Symptoms. Nutrients, 16(11), 1712. https://doi.org/10.3390/nu16111712