
What Is the Nutritional Quality of Pre-Packed Foods Marketed to Children in Food Stores? A Survey in Switzerland

 , and
, and {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Selection of Food Products
2.2. Definition of Nutritional Quality
2.3. Data Entry
2.4. Data Quality Check
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Sample
3.2. Marketing Techniques
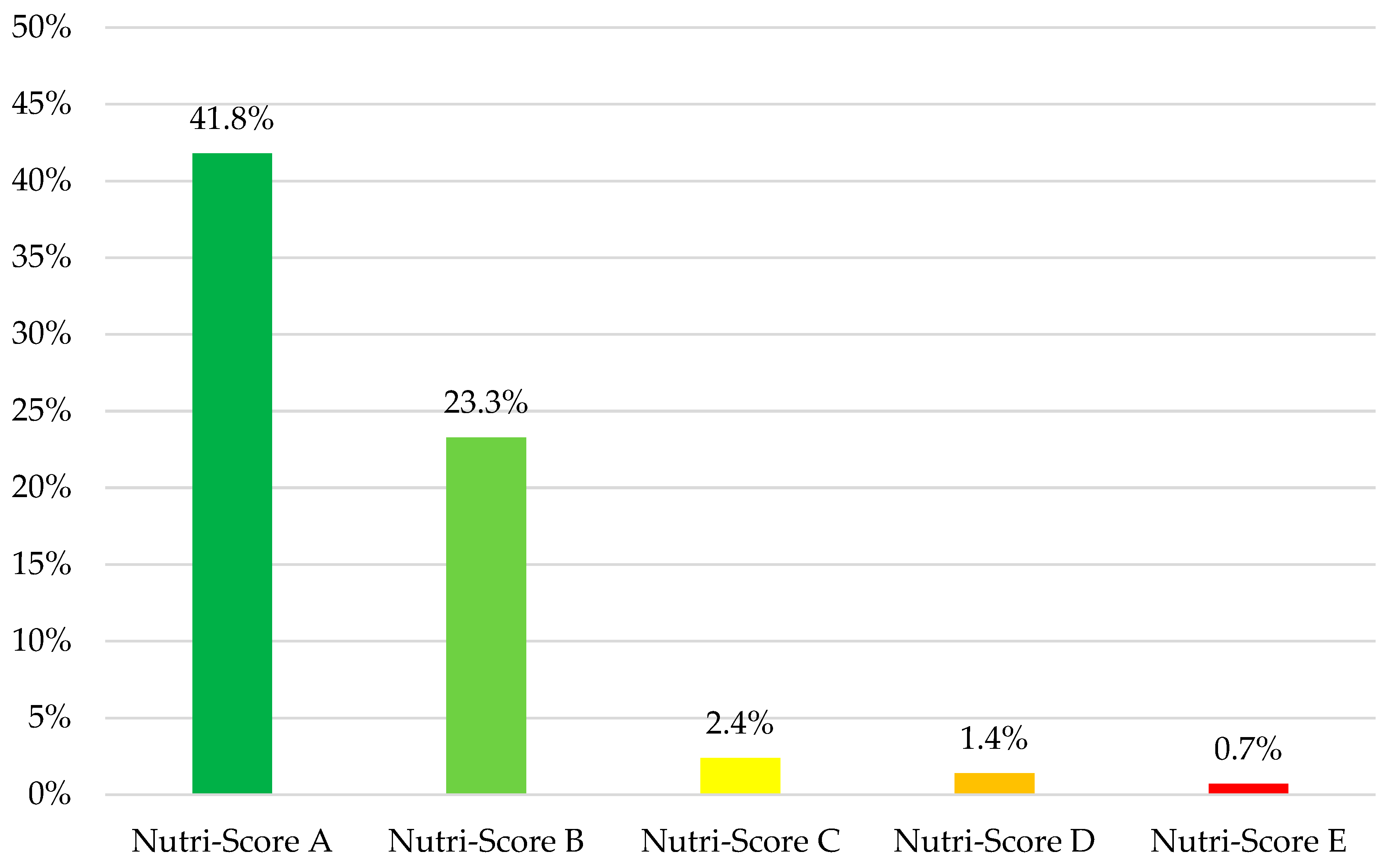
3.3. Nutri-Score
3.4. NOVA Classification
3.5. Compliance with the WHO Nutrient Profile Model
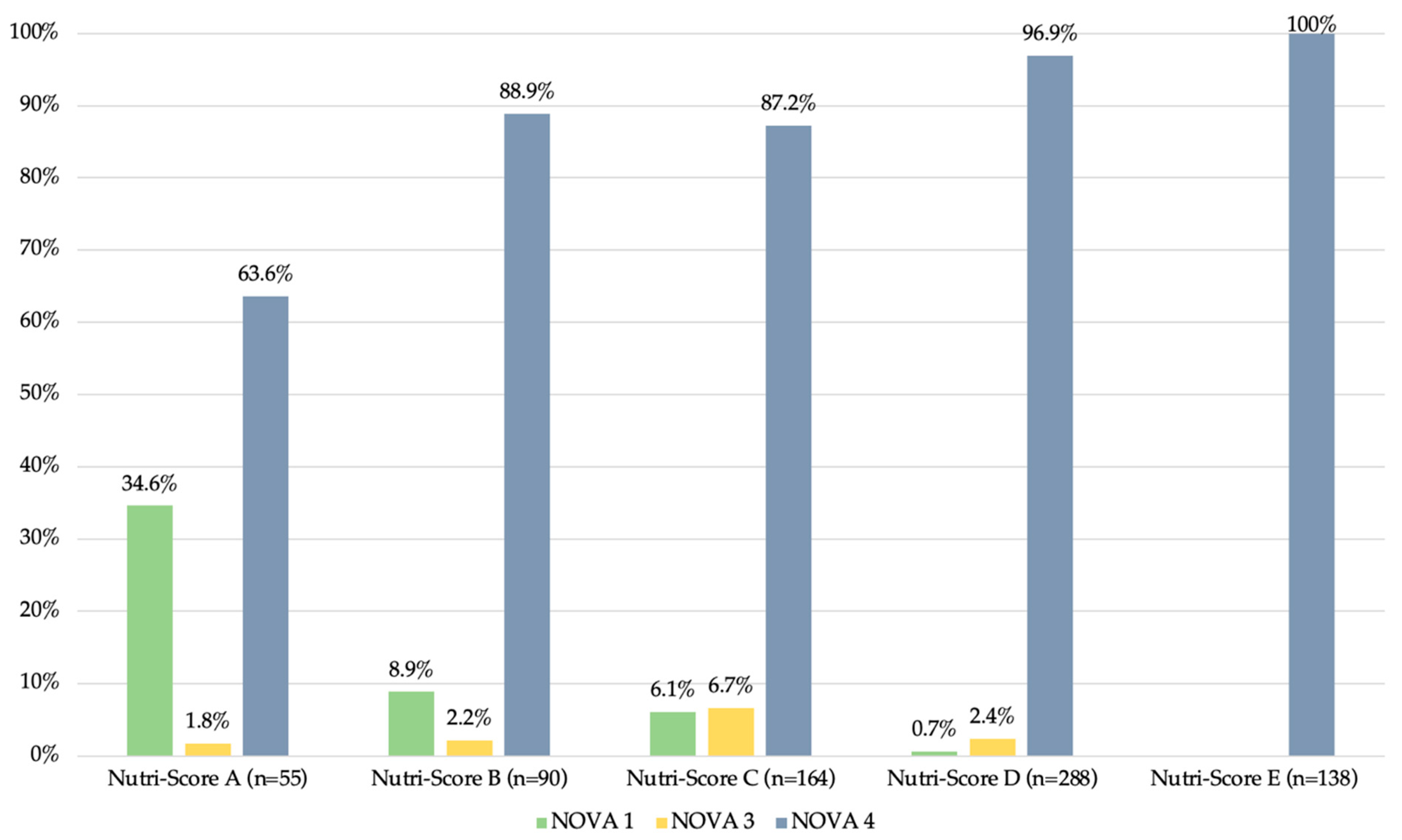
3.6. Nutri-Score and NOVA Classification
3.7. Nutri-Score and WHO NPM
3.8. WHO NPM and NOVA Classification
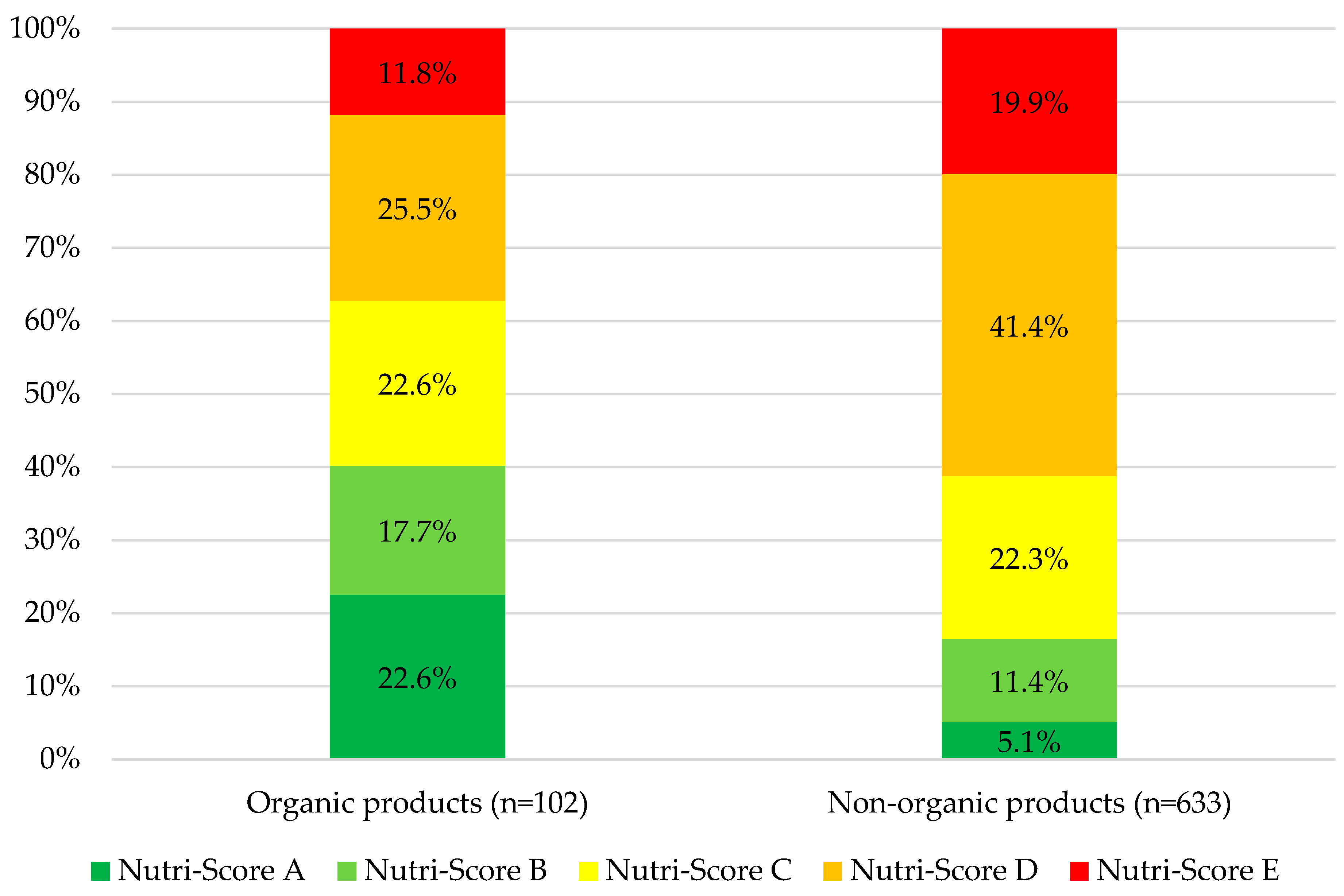
3.9. Organic Products
3.10. Nutritional Claims
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- UNICEF. Protecting Children’s Right to a Healthy Food Environment. Available online: https://www.unicef.nl/files/Advocacy-brief-healthy-food-enviro-final.pdf (accessed on 8 November 2022).
- Organisation Mondiale de la Santé (OMS). Obésité et Surpoids. Available online: https://www.who.int/fr/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 12 November 2022).
- Di Cesare, M.; Sorić, M.; Bovet, P.; Miranda, J.J.; Bhutta, Z.; Stevens, G.A.; Laxmaiah, A.; Kengne, A.-P.; Bentham, J. The Epidemiological Burden of Obesity in Childhood: A Worldwide Epidemic Requiring Urgent Action. BMC Med. 2019, 17, 212. [Google Scholar] [CrossRef] [PubMed]
- Promotion Santé Suisse (PSS). Monitoring Des Données Pondérales Effectué Par Les Services de Santé Scolaires Des Villes de Bâle, Berne et Zurich. Évolution Du Surpoids et de l’obésité Chez Les Enfants et Les Adolescent-e-s Au Cours de L’année Scolaire 2021/22 Avec Accent Sur Le Thème «Origine Nationale et Sociale». Available online: https://promotionsante.ch/sites/default/files/2023-05/Feuille_d_information_084_PSCH_2023-05_-_Monitoring_IMC_2021-2022.pdf (accessed on 5 September 2023).
- UNICEF. Prevention of Overweight and Obesity in Children and Adolescents. Available online: https://www.unicef.org/media/92336/file/Programming-Guidance-Overweight-Prevention.pdf (accessed on 9 November 2022).
- Murray, C.; Aravkin, A.; Zheng, P.; Abbafati, C.; Abbas, K.; Foad, A.; Abdelalim, A.; Abdollahi, M.; Abdollahpour, I.; Abegaz, K.H.; et al. Global Burden of 87 Risk Factors in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1223–1249. [Google Scholar] [CrossRef] [PubMed]
- Clark, H.; Coll-Seck, A.M.; Banerjee, A.; Peterson, S.; Dalglish, S.L.; Ameratunga, S.; Balabanova, D.; Bhan, M.K.; Bhutta, Z.A.; Borrazzo, J.; et al. A Future for the World’s Children? A WHO-UNICEF-Lancet Commission. Lancet 2020, 395, 605–658. [Google Scholar] [CrossRef] [PubMed]
- Lane, M.M.; Davis, J.A.; Beattie, S.; Gómez-Donoso, C.; Loughman, A.; O’Neil, A.; Jacka, F.; Berk, M.; Page, R.; Marx, W.; et al. Ultraprocessed Food and Chronic Noncommunicable Diseases: A Systematic Review and Meta-Analysis of 43 Observational Studies. Obes. Rev. 2021, 22, e13146. [Google Scholar] [CrossRef] [PubMed]
- Elizabeth, L.; Machado, P.; Zinöcker, M.; Baker, P.; Lawrence, M. Ultra-Processed Foods and Health Outcomes: A Narrative Review. Nutrients 2020, 12, 1955. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Food Marketing Exposure and Power and Their Associations with Food-Related Attitudes, Beliefs and Behaviours: A Narrative Review. Available online: https://www.who.int/publications-detail-redirect/9789240041783 (accessed on 5 November 2022).
- García, A.L.; Morillo-Santander, G.; Parrett, A.; Mutoro, A.N. Misrepresentation of Health and Nutrition Claims in Food Marketing to Children Could Adversely Affect Food Choice and Increase Risk of Obesity. Arch. Dis. Child. 2019, 104, 541–546. [Google Scholar] [CrossRef] [PubMed]
- Gilbert-Moreau, J.; Pomerleau, S.; Perron, J.; Gagnon, P.; Labonté, M.-È.; Provencher, V. Nutritional Value of Child-Targeted Food Products: Results from the Food Quality Observatory. Public Health Nutr. 2021, 24, 5329–5337. [Google Scholar] [CrossRef] [PubMed]
- Lavriša, Ž.; Pravst, I. Marketing of Foods to Children through Food Packaging Is Almost Exclusively Linked to Unhealthy Foods. Nutrients 2019, 11, 1128. [Google Scholar] [CrossRef] [PubMed]
- Kelly, B.; Vandevijvere, S.; Ng, S.; Adams, J.; Allemandi, L.; Bahena-Espina, L.; Barquera, S.; Boyland, E.; Calleja, P.; Carmona-Garcés, I.C.; et al. Global Benchmarking of Children’s Exposure to Television Advertising of Unhealthy Foods and Beverages across 22 Countries. Obes. Rev. 2019, 20 (Suppl. 2), 116–128. [Google Scholar] [CrossRef] [PubMed]
- European Commission. Study on the Exposure of Children to Linear, Non-Linear and Online Marketing of Foods High in Fat, Salt or Sugar: Final Report. Available online: https://data.europa.eu/doi/10.2875/928620 (accessed on 8 November 2022).
- Office Fédéral de la Sécurité Alimentaire et des Affaires Vétérinaires (OSAV). Monitoring du Marketing Numérique Destiné aux Enfants avec la Méthode CLICK Développée par l’OMS/Europe. Available online: https://www.blv.admin.ch/blv/fr/home/lebensmittel-und-ernaehrung/ernaehrung/werbung-und-marketing.html (accessed on 29 July 2023).
- Coleman, P.C.; Hanson, P.; van Rens, T.; Oyebode, O. A Rapid Review of the Evidence for Children’s TV and Online Advertisement Restrictions to Fight Obesity. Prev. Med. Rep. 2022, 26, 101717. [Google Scholar] [CrossRef]
- Elías Zambrano, R.; Jiménez-Marín, G.; Galiano-Coronil, A.; Ravina-Ripoll, R. Children, Media and Food. A New Paradigm in Food Advertising, Social Marketing and Happiness Management. Int. J. Environ. Res. Public Health 2021, 18, 3588. [Google Scholar] [CrossRef] [PubMed]
- Enax, L.; Weber, B.; Ahlers, M.; Kaiser, U.; Diethelm, K.; Holtkamp, D.; Faupel, U.; Holzmüller, H.H.; Kersting, M. Food Packaging Cues Influence Taste Perception and Increase Effort Provision for a Recommended Snack Product in Children. Front. Psychol. 2015, 6, 882. [Google Scholar] [CrossRef]
- Sadeghirad, B.; Duhaney, T.; Motaghipisheh, S.; Campbell, N.R.C.; Johnston, B.C. Influence of Unhealthy Food and Beverage Marketing on Children’s Dietary Intake and Preference: A Systematic Review and Meta-Analysis of Randomized Trials. Obes. Rev. 2016, 17, 945–959. [Google Scholar] [CrossRef] [PubMed]
- Boyland, E.J.; Nolan, S.; Kelly, B.; Tudur-Smith, C.; Jones, A.; Halford, J.C.; Robinson, E. Advertising as a Cue to Consume: A Systematic Review and Meta-Analysis of the Effects of Acute Exposure to Unhealthy Food and Nonalcoholic Beverage Advertising on Intake in Children and Adults. Am. J. Clin. Nutr. 2016, 103, 519–533. [Google Scholar] [CrossRef] [PubMed]
- Smith, R.; Kelly, B.; Yeatman, H.; Boyland, E. Food Marketing Influences Children’s Attitudes, Preferences and Consumption: A Systematic Critical Review. Nutrients 2019, 11, 875. [Google Scholar] [CrossRef] [PubMed]
- Lythgoe, A.; Roberts, C.; Madden, A.M.; Rennie, K.L. Marketing Foods to Children: A Comparison of Nutrient Content between Children’s and Non-Children’s Products. Public Health Nutr. 2013, 16, 2221–2230. [Google Scholar] [CrossRef]
- Richonnet, C.; Mosser, F.; Favre, E.; Robert, M.; Martin, F.; Thiebaut, I. Nutritional Quality and Degree of Processing of Children’s Foods Assessment on the French Market. Nutrients 2022, 14, 171. [Google Scholar] [CrossRef] [PubMed]
- Swiss Pledge. Initiative Volontaire Swiss Pledge: Pour des Pratiques Publicitaires Responsables vis-à-vis des Enfants. Available online: https://swiss-pledge.ch/apropos-de-nous/ (accessed on 10 November 2022).
- EU Pledge. The EU Pledge at a Glance. Available online: https://eu-pledge.eu/the-eu-pledge-at-a-glance/ (accessed on 10 November 2022).
- Santé Publique France. Nutri-Score. Available online: https://www.santepubliquefrance.fr/determinants-de-sante/nutrition-et-activite-physique/articles/nutri-score (accessed on 13 November 2022).
- Monteiro, C.A.; Cannon, G.; Levy, R.B.; Moubarac, J.-C.; Louzada, M.L.; Rauber, F.; Khandpur, N.; Cediel, G.; Neri, D.; Martinez-Steele, E.; et al. Ultra-Processed Foods: What They Are and How to Identify Them. Public Health Nutr. 2019, 22, 936–941. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for Europe WHO Regional Office for Europe Nutrient Profile Model: Second Edition. Available online: https://www.who.int/europe/publications/i/item/WHO-EURO-2023-6894-46660-68492 (accessed on 13 April 2023).
- Confédération Suisse. Commerce de Détail. Available online: https://www.eda.admin.ch/aboutswitzerland/fr/home/wirtschaft/taetigkeitsgebiete/detailhandel.html (accessed on 24 March 2024).
- Statista. Organic Food Market: Leading Countries Based on Consumption per Capita. Available online: https://www.statista.com/statistics/263077/per-capita-revenue-of-organic-foods-worldwide-since-2007/ (accessed on 24 March 2024).
- Torres-Schiaffino, D.; Saavedra-Garcia, L. Relationship between Marketing to Children on Food Labeling and Critical Nutrient Content in Processed and Ultra-Processed Products Sold in Supermarkets in Lima, Peru. Nutrients 2020, 12, 3666. [Google Scholar] [CrossRef]
- Meloncelli, N.J.L.; Pelly, F.E.; Cooper, S.L. Nutritional Quality of a Selection of Children’s Packaged Food Available in Australia: The Nutritional Quality of Children’s Food. Nutr. Diet. 2016, 73, 88–94. [Google Scholar] [CrossRef]
- Elliott, C. Assessing “Fun Foods”: Nutritional Content and Analysis of Supermarket Foods Targeted at Children. Obes. Rev. 2008, 9, 368–377. [Google Scholar] [CrossRef] [PubMed]
- Jenkin, G.; Madhvani, N.; Signal, L.; Bowers, S. A Systematic Review of Persuasive Marketing Techniques to Promote Food to Children on Television. Obes. Rev. 2014, 15, 281–293. [Google Scholar] [CrossRef] [PubMed]
- Boyland, E.J.; Harrold, J.A.; Kirkham, T.C.; Halford, J.C.G. Persuasive Techniques Used in Television Advertisements to Market Foods to UK Children. Appetite 2012, 58, 658–664. [Google Scholar] [CrossRef] [PubMed]
- Elliott, C. Marketing Fun Foods: A Profile and Analysis of Supermarket Food Messages Targeted at Children. Can. Public Policy 2008, 34, 259–273. [Google Scholar] [CrossRef]
- Scientific Committee of the Nutri-Score. Update of the Nutri-Score Algorithm. Update Report from the Scientific Committee of the Nutri-Score 2022. Available online: https://nutriscore.blog/2022/08/01/rapport-du-comite-scientifique-europeen-en-charge-de-la-mise-a-jour-du-nutri-score-modifications-apportees-a-lalgorithme-pour-les-aliments-solides/ (accessed on 31 December 2022).
- Office Fédéral de la Sécurité Alimentaire et des Affaires Vétérinaires (OSAV). La Base De Données Suisse Des Valeurs Nutritives. Available online: https://valeursnutritives.ch/fr/ (accessed on 14 July 2023).
- Anses Ciqual. Table de Composition Nutritionnelle Des Aliments. Available online: https://ciqual.anses.fr/ (accessed on 14 July 2023).
- World Health Organization (WHO). WHO Regional Office for Europe. Nutrient Profile Model. Available online: https://www.euro.who.int/__data/assets/pdf_file/0005/270716/Nutrient-children_web-new.pdf (accessed on 2 November 2022).
- Agroscope. Acides Gras Trans: Aucun Risque Pour la Santé en Suisse. Available online: https://www.agroscope.admin.ch/agroscope/fr/home/themen/lebensmittel/ernaehrung-gesundheit/fleischprodukte/fleischfett/trans-fettsaeuren.html (accessed on 26 March 2024).
- Organisation Mondiale de la Santé (OMS). Apport En Sucres Chez L’adulte et L’enfant. Available online: https://apps.who.int/iris/bitstream/handle/10665/155735/WHO_NMH_NHD_15.2_fre.pdf (accessed on 14 December 2022).
- Mehta, K.; Phillips, C.; Ward, P.; Coveney, J.; Handsley, E.; Carter, P. Marketing Foods to Children through Product Packaging: Prolific, Unhealthy and Misleading. Public Health Nutr. 2012, 15, 1763–1770. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, V.M.; Rayner, M.; Fernandes, A.C.; de Oliveira, R.C.; Proença, R.P.d.C.; Fiates, G.M.R. Comparison of the Nutritional Content of Products, with and without Nutrient Claims, Targeted at Children in Brazil. Br. J. Nutr. 2016, 115, 2047–2056. [Google Scholar] [CrossRef] [PubMed]
- Boyland, E.; McGale, L.; Maden, M.; Hounsome, J.; Boland, A.; Angus, K.; Jones, A. Association of Food and Nonalcoholic Beverage Marketing with Children and Adolescents’ Eating Behaviors and Health: A Systematic Review and Meta-Analysis. JAMA Pediatr. 2022, 176, e221037. [Google Scholar] [CrossRef] [PubMed]
- Ministère de la Santé et de la Prévention Nutri-Score. Evaluation à 3 Ans Du Logo Nutritionnel Nutri-Score. Available online: https://solidarites-sante.gouv.fr/IMG/pdf/nutriscorebilan3ans.pdf (accessed on 31 December 2022).
- Falquet, M.-N.; Brunner, T.; Lehmann, U.; Augé, C.; Améliorer L’efficacité Du Nutri-Score En Suisse. Rapport Scientifique Pour Répondre Au Postulat 20.3913 « Améliorer L’efficacité Du Nutri-Score ». Available online: https://www.blv.admin.ch/blv/fr/home/dokumentation/nsb-news-list.msg-id-92042.html (accessed on 31 December 2022).
- Julia, C.; Ducrot, P.; Péneau, S.; Deschamps, V.; Méjean, C.; Fézeu, L.; Touvier, M.; Hercberg, S.; Kesse-Guyot, E. Discriminating Nutritional Quality of Foods Using the 5-Color Nutrition Label in the French Food Market: Consistency with Nutritional Recommendations. Nutr. J. 2015, 14, 100. [Google Scholar] [CrossRef]
- Julia, C.; Kesse-Guyot, E.; Touvier, M.; Méjean, C.; Fezeu, L.; Hercberg, S. Application of the British Food Standards Agency Nutrient Profiling System in a French Food Composition Database. Br. J. Nutr. 2014, 112, 1699–1705. [Google Scholar] [CrossRef] [PubMed]
- Julia, C.; Méjean, C.; Touvier, M.; Péneau, S.; Lassale, C.; Ducrot, P.; Hercberg, S.; Kesse-Guyot, E. Validation of the FSA Nutrient Profiling System Dietary Index in French Adults—Findings from SUVIMAX Study. Eur. J. Nutr. 2016, 55, 1901–1910. [Google Scholar] [CrossRef]
- Hercberg, S.; Touvier, M.; Salas-Salvado, J. The Nutri-Score Nutrition Label. Int. J. Vitam. Nutr. Res. 2022, 92, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Deschasaux, M.; Huybrechts, I.; Julia, C.; Hercberg, S.; Egnell, M.; Srour, B.; Kesse-Guyot, E.; Latino-Martel, P.; Biessy, C.; Casagrande, C.; et al. Association between Nutritional Profiles of Foods Underlying Nutri-Score Front-of-Pack Labels and Mortality: EPIC Cohort Study in 10 European Countries. BMJ 2020, 370, m3173. [Google Scholar] [CrossRef] [PubMed]
- Adriouch, S.; Julia, C.; Kesse-Guyot, E.; Méjean, C.; Ducrot, P.; Péneau, S.; Donnenfeld, M.; Deschasaux, M.; Menai, M.; Hercberg, S.; et al. Prospective Association between a Dietary Quality Index Based on a Nutrient Profiling System and Cardiovascular Disease Risk. Eur. J. Prev. Cardiol. 2016, 23, 1669–1676. [Google Scholar] [CrossRef] [PubMed]
- Julia, C.; Fézeu, L.K.; Ducrot, P.; Méjean, C.; Péneau, S.; Touvier, M.; Hercberg, S.; Kesse-Guyot, E. The Nutrient Profile of Foods Consumed Using the British Food Standards Agency Nutrient Profiling System Is Associated with Metabolic Syndrome in the SU.VI.MAX Cohort. J. Nutr. 2015, 145, 2355–2361. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Wang, H.; Zhang, P.; Popkin, B.M.; Coyle, D.H.; Ding, J.; Dong, L.; Zhang, J.; Du, W.; Pettigrew, S. Nutritional Quality of Pre-Packaged Foods in China under Various Nutrient Profile Models. Nutrients 2022, 14, 2700. [Google Scholar] [CrossRef] [PubMed]
- Baldridge, A.S.; Huffman, M.D.; Taylor, F.; Xavier, D.; Bright, B.; Van Horn, L.V.; Neal, B.; Dunford, E. The Healthfulness of the US Packaged Food and Beverage Supply: A Cross-Sectional Study. Nutrients 2019, 11, 1704. [Google Scholar] [CrossRef] [PubMed]
- Luiten, C.M.; Steenhuis, I.H.; Eyles, H.; Ni Mhurchu, C.; Waterlander, W.E. Ultra-Processed Foods Have the Worst Nutrient Profile, yet They Are the Most Available Packaged Products in a Sample of New Zealand Supermarkets. Public Health Nutr. 2016, 19, 530–538. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Martínez Steele, E.; Du, M.; Pomeranz, J.L.; O’Connor, L.E.; Herrick, K.A.; Luo, H.; Zhang, X.; Mozaffarian, D.; Zhang, F.F. Trends in Consumption of Ultraprocessed Foods among US Youths Aged 2–19 Years, 1999–2018. JAMA 2021, 326, 519–530. [Google Scholar] [CrossRef] [PubMed]
- Martines, R.M.; Machado, P.P.; Neri, D.A.; Levy, R.B.; Rauber, F. Association between Watching TV Whilst Eating and Children’s Consumption of Ultraprocessed Foods in United Kingdom. Matern. Child. Nutr. 2019, 15, e12819. [Google Scholar] [CrossRef]
- Fardet, A.; Thivel, D.; Gerbaud, L.; Rock, E. A Sustainable and Global Health Perspective of the Dietary Pattern of French Population during the 1998–2015 Period from INCA Surveys. Sustainability 2021, 13, 7433. [Google Scholar] [CrossRef]
- Vandevijvere, S. Uptake of Nutri-Score during the First Year of Implementation in Belgium. Arch. Public Health 2020, 78, 107. [Google Scholar] [CrossRef] [PubMed]
- Juul, F.; Parekh, N.; Martinez-Steele, E.; Monteiro, C.A.; Chang, V.W. Ultra-Processed Food Consumption among US Adults from 2001 to 2018. Am. J. Clin. Nutr. 2022, 115, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Rauber, F.; Louzada, M.L.d.C.; Steele, E.M.; de Rezende, L.F.M.; Millett, C.; Monteiro, C.A.; Levy, R.B. Ultra-Processed Foods and Excessive Free Sugar Intake in the UK: A Nationally Representative Cross-Sectional Study. BMJ Open 2019, 9, e027546. [Google Scholar] [CrossRef] [PubMed]
- Julia, C.; Martinez, L.; Allès, B.; Touvier, M.; Hercberg, S.; Méjean, C.; Kesse-Guyot, E. Contribution of Ultra-Processed Foods in the Diet of Adults from the French NutriNet-Santé Study. Public Health Nutr. 2018, 21, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Vedovato, G.M.; Vilela, S.; Severo, M.; Rodrigues, S.; Lopes, C.; Oliveira, A. Ultra-Processed Food Consumption, Appetitive Traits and BMI in Children: A Prospective Study. Br. J. Nutr. 2021, 125, 1427–1436. [Google Scholar] [CrossRef] [PubMed]
- Pagliai, G.; Dinu, M.; Madarena, M.P.; Bonaccio, M.; Iacoviello, L.; Sofi, F. Consumption of Ultra-Processed Foods and Health Status: A Systematic Review and Meta-Analysis. Br. J. Nutr. 2021, 125, 308–318. [Google Scholar] [CrossRef] [PubMed]
- Leffa, P.S.; Hoffman, D.J.; Rauber, F.; Sangalli, C.N.; Valmórbida, J.L.; Vitolo, M.R. Longitudinal Associations between Ultra-Processed Foods and Blood Lipids in Childhood. Br. J. Nutr. 2020, 124, 341–348. [Google Scholar] [CrossRef]
- Bertoni Maluf, V.A.; Bucher Della Torre, S.; Jotterand Chaparro, C.; Belle, F.N.; Khalatbari-Soltani, S.; Kruseman, M.; Marques-Vidal, P.; Chatelan, A. Description of Ultra-Processed Food Intake in a Swiss Population-Based Sample of Adults Aged 18 to 75 Years. Nutrients 2022, 14, 4486. [Google Scholar] [CrossRef] [PubMed]
- Martínez Steele, E.; Popkin, B.M.; Swinburn, B.; Monteiro, C.A. The Share of Ultra-Processed Foods and the Overall Nutritional Quality of Diets in the US: Evidence from a Nationally Representative Cross-Sectional Study. Popul. Health Metr. 2017, 15, 6. [Google Scholar] [CrossRef]
- Khandpur, N.; Neri, D.A.; Monteiro, C.; Mazur, A.; Frelut, M.-L.; Boyland, E.; Weghuber, D.; Thivel, D. Ultra-Processed Food Consumption among the Paediatric Population: An Overview and Call to Action from the European Childhood Obesity Group. Ann. Nutr. Metab. 2020, 76, 109–113. [Google Scholar] [CrossRef]
- Foodwatch. Les Enfants, Cibles Du Marketing de La Malbouffe: L’heure de L’action Politique. Available online: https://www.foodwatch.org/fileadmin/-FR/Documents/Foodwatch_Publication_rapport_malbouffe_pub-enfants_23_09_12.pdf (accessed on 15 September 2023).
- Galan, P.; Kesse, E.; Touvier, M.; Deschasaux, M.; Srour, B.; Chazelas, E.; Baudry, J.; Fialon, M.; Julia, C.; Hercberg, S. Nutri-Score et Ultra-Transformation: Deux Dimensions Différentes, Complémentaires et Non Contradictoires. Available online: https://nutriscore.blog/2020/12/07/nutri-score-et-ultra-transformation-deux-dimensions-differentes-complementaires-et-non-contradictoires/ (accessed on 8 September 2023).
- Srour, B.; Fezeu, L.K.; Kesse-Guyot, E.; Allès, B.; Méjean, C.; Andrianasolo, R.M.; Chazelas, E.; Deschasaux, M.; Hercberg, S.; Galan, P.; et al. Ultra-Processed Food Intake and Risk of Cardiovascular Disease: Prospective Cohort Study (NutriNet-Santé). BMJ 2019, 365, l1451. [Google Scholar] [CrossRef] [PubMed]
- Soczynska, I.; da Costa, B.R.; O’Connor, D.L.; Jenkins, D.J.A.; Birken, C.S.; Juando-Prats, C.; Maguire, J.L. Parent and Physician Beliefs, Perceptions and Knowledge of Plant Milks for Children. Nutr. Health 2023, 02601060231171299. [Google Scholar] [CrossRef] [PubMed]
- Fifi, A.C.; Pagan, D.N.; Chakraborty, P.; Mahajan, N.; Axelrod, C.; Bayes, L.Y.; Katz, D.T. Physician and Parent Perceptions on Plant-Based Beverages as Substitutes for Cow’s Milk: A Single City Survey. J. Pediatr. Gastroenterol. Nutr. 2022, 75, e25–e29. [Google Scholar] [CrossRef] [PubMed]
- Kraak, V.I.; Vandevijvere, S.; Sacks, G.; Brinsden, H.; Hawkes, C.; Barquera, S.; Lobstein, T.; Swinburn, B.A. Progress Achieved in Restricting the Marketing of High-Fat, Sugary and Salty Food and Beverage Products to Children. Bull. World Health Organ. 2016, 94, 540–548. [Google Scholar] [CrossRef]
- Chambers, S.A.; Freeman, R.; Anderson, A.S.; MacGillivray, S. Reducing the Volume, Exposure and Negative Impacts of Advertising for Foods High in Fat, Sugar and Salt to Children: A Systematic Review of the Evidence from Statutory and Self-Regulatory Actions and Educational Measures. Prev. Med. 2015, 75, 32–43. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). A Framework for Implementing the Set of Recommendations on the Marketing of Foods and Non-Alcoholic Beverages to Children. Available online: https://www.who.int/publications-detail-redirect/9789241503242 (accessed on 26 March 2024).
- World Health Organization (WHO). Policies to Protect Children from the Harmful Impact of Food Marketing: WHO Guideline. Available online: https://www.who.int/publications-detail-redirect/9789240075412 (accessed on 26 March 2024).
- Safe Food Advocacy Europe. Norway to Ban Unhealthy Food Adverts Aimed at Kids. Available online: https://www.safefoodadvocacy.eu/norway-to-ban-unhealthy-food-adverts-aimed-at-kids/ (accessed on 9 November 2023).
- The European Consumer Organisation (BEUC). Food Marketing to Chlidren Needs Rules. A Snapshot Report about How Self-Regulation Fails to Prevent Unhealthy Foods to Be Marketed to Children. Available online: https://www.beuc.eu/sites/default/files/publications/beuc-x-2021-084_food_marketing_to_children_needs_rules_with_teeth.pdf (accessed on 8 November 2022).
- Best-ReMaP. About Us—Best-ReMaP. Available online: https://bestremap.eu/about-us/ (accessed on 18 May 2024).
- Kanter, R.; Vanderlee, L.; Vandevijvere, S. Front-of-Package Nutrition Labelling Policy: Global Progress and Future Directions. Public Health Nutr. 2018, 21, 1399–1408. [Google Scholar] [CrossRef]
- Roberto, C.A.; Ng, S.W.; Ganderats-Fuentes, M.; Hammond, D.; Barquera, S.; Jauregui, A.; Taillie, L.S. The Influence of Front-of-Package Nutrition Labeling on Consumer Behavior and Product Reformulation. Annu. Rev. Nutr. 2021, 41, 529–550. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pellegrino, F.; Tan, M.; Richonnet, C.; Reinert, R.; Bucher Della Torre, S.; Chatelan, A. What Is the Nutritional Quality of Pre-Packed Foods Marketed to Children in Food Stores? A Survey in Switzerland. Nutrients 2024, 16, 1656. https://doi.org/10.3390/nu16111656
Pellegrino F, Tan M, Richonnet C, Reinert R, Bucher Della Torre S, Chatelan A. What Is the Nutritional Quality of Pre-Packed Foods Marketed to Children in Food Stores? A Survey in Switzerland. Nutrients. 2024; 16(11):1656. https://doi.org/10.3390/nu16111656
Chicago/Turabian StylePellegrino, Fabien, Monique Tan, Celine Richonnet, Raphaël Reinert, Sophie Bucher Della Torre, and Angeline Chatelan. 2024. "What Is the Nutritional Quality of Pre-Packed Foods Marketed to Children in Food Stores? A Survey in Switzerland" Nutrients 16, no. 11: 1656. https://doi.org/10.3390/nu16111656
APA StylePellegrino, F., Tan, M., Richonnet, C., Reinert, R., Bucher Della Torre, S., & Chatelan, A. (2024). What Is the Nutritional Quality of Pre-Packed Foods Marketed to Children in Food Stores? A Survey in Switzerland. Nutrients, 16(11), 1656. https://doi.org/10.3390/nu16111656