
Assessment of Heavy Metals and Trace Elements in the Human Milk of Women Living in Latvia and an Evaluation of Influencing Factors †


Abstract
1. Introduction
2. Materials and Methods
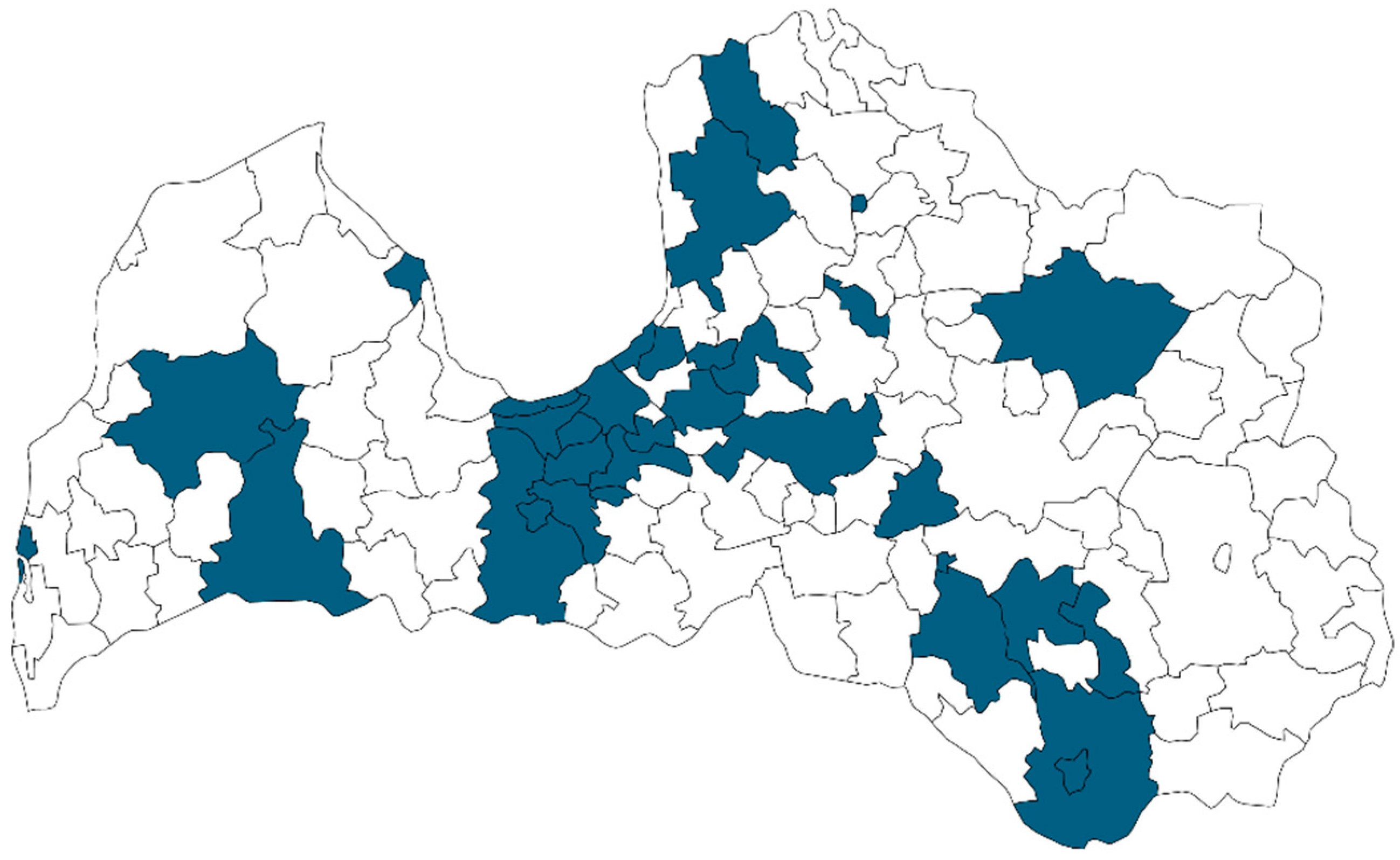
2.1. Selection of Participants and Collection of Human Milk Samples
- Reside in Latvia;
- Singleton pregnancy;
- At least 28 days postpartum;
- Exclusively or partially breastfeeding;
- Mother and child are both healthy (without metabolic disorders, no acute illnesses, etc.).
- Unsigned written informed consent;
- Non-compliance with the inclusion criteria.
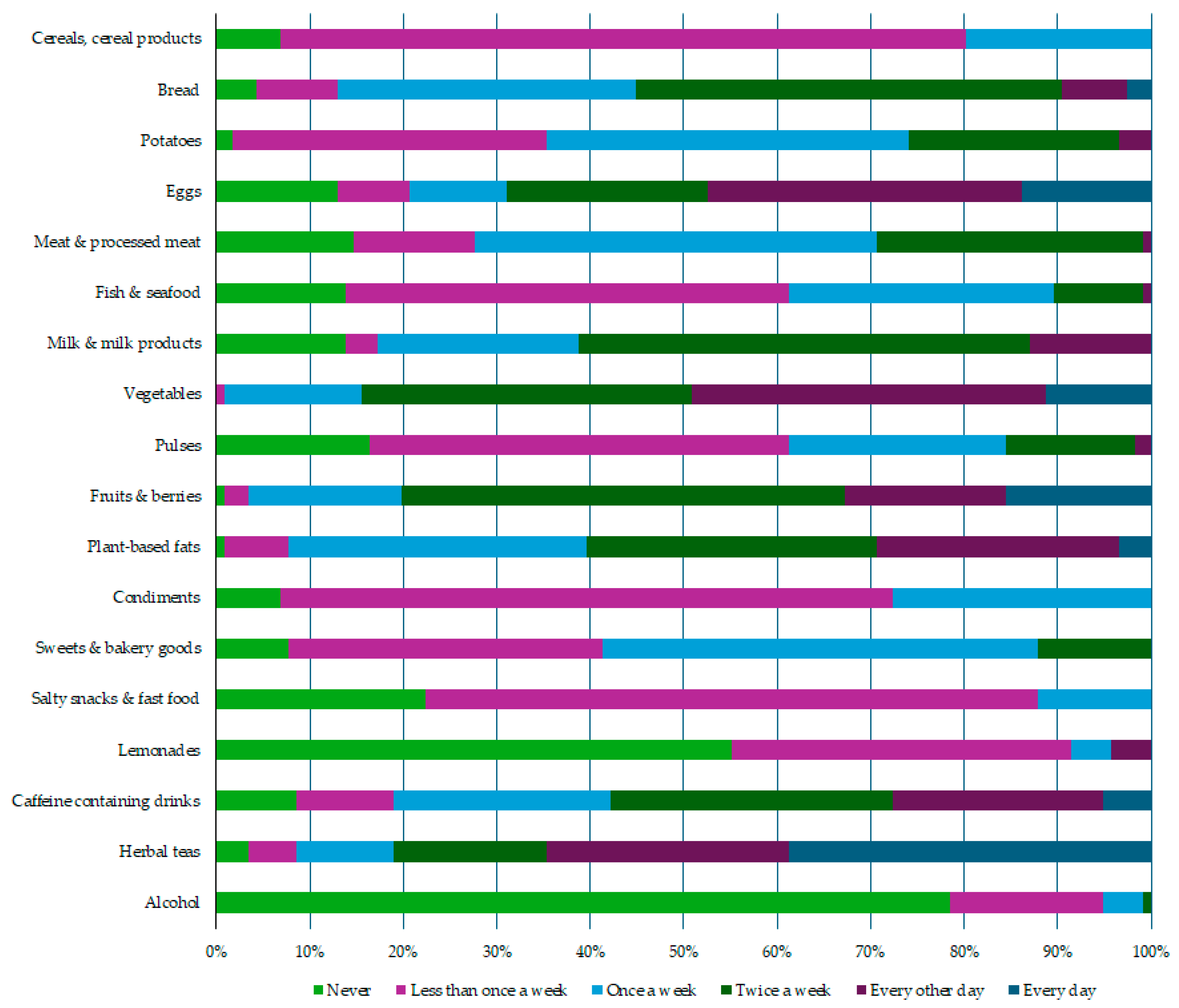
- Never;
- Less than once a week;
- Once a week;
- Two times a week;
- Every other day;
- Every day.
- Cereals, cereal products;
- Bread;
- Potatoes;
- Eggs;
- Meat and processed meat;
- Milk and milk products;
- Fish and seafood;
- Vegetables;
- Pulses;
- Fruits and berries;
- Plant-based fats;
- Condiments;
- Sweets and bakery goods;
- Salty snacks and fast food;
- Lemonades;
- Caffeine-containing drinks;
- Herbal teas;
- Alcohol.
- Non-response to the researcher after agreeing to participate in the study (n = 8 in the first study period, n = 7 in the second study period);
- Not being able to collect the necessary amount of human milk for the analysis of the elements (n = 1 in the first study period, n = 4 in the second study period);
- The child or the mother developed health problems, and thus they no longer met the inclusion criteria of the study (n = 4 in the first study period).
2.2. ICP-MS Analysis
- Plasma mode—normal, robust;
- RF forward power (W)—1300;
- Sampling depth (mm)—8.0;
- Carrier gas flow (L min−1)—0.6;
- Dilution gas flow (L min−1)—0.4;
- Spray chamber temperature (°C)—2;
- Extraction lens 1 (V)—0;
- Kinetic energy discrimination (V)—3.
2.3. Statistical Analysis
3. Results
3.1. Characteristics of the Participants
3.2. Dietary Habits among Participants
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Breastfeeding. Available online: https://www.who.int/health-topics/breastfeeding#tab=tab_2 (accessed on 8 May 2024).
- Rebelo, F.M.; Caldas, E.D. Arsenic, lead, mercury and cadmium: Toxicity, levels in breast milk and the risks for breastfed infants. Environ. Res. 2016, 151, 671–688. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Contaminants in the Food Chain (CONTAM); Schrenk, D.; Bignami, M.; Bodin, L.; Chipman, J.K.; del Mazo, J.; Grasl-Kraupp, B.; Hogstrand, C.; Hoogenboom, L.; Leblanc, J.C.; et al. Update of the Risk Assessment of Inorganic Arsenic in Food. EFSA J. 2024, 22, e8488. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority. Cadmium Dietary Exposure in the European Population. EFSA J. 2012, 10, 2551. [Google Scholar] [CrossRef]
- European Food Safety Authority. Opinion of the Scientific Panel on Dietetic Products, Nutrition and Allergies on a Request from the Commission Related to the Tolerable Upper Intake Level of Tin. EFSA J. 2005, 3, 254. [Google Scholar] [CrossRef]
- European Food Safety Authority. Scientific Opinion on Lead in Food. EFSA J. 2010, 8, 1570. [Google Scholar] [CrossRef]
- European Food Safety Authority. Safety of Aluminium from Dietary Intake. EFSA J. 2008, 6, 754. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority. Update of the Risk Assessment of Nickel in Food and Drinking Water. EFSA J. 2020, 18, 6268. [Google Scholar] [CrossRef]
- Carignan, C.C.; Cottingham, K.L.; Jackson, B.P.; Farzan, S.F.; Gandolfi, A.J. Estimated Exposure to Arsenic in Breastfed and Formula-Fed Infants in a United States Cohort. Environ. Health Perspect. 2015, 123, 500–506. [Google Scholar] [CrossRef]
- Winiarska-Mieczan, A. Cadmium, lead, copper and zinc in breast milk in Poland. Biol. Trace Elem. Res. 2014, 157, 36–44. [Google Scholar] [CrossRef]
- Yurdakök, K. Lead, mercury, and cadmium in breast milk. J. Pediatric Neonatal Individ. Med. 2015, 4, e040223. [Google Scholar] [CrossRef]
- Björklund, K.L.; Vahter, M.; Palm, B.; Grandér, M.; Lignell, S.; Berglund, M. Metals and trace element concentrations in breast milk of first time healthy mothers: A biological monitoring study. Environ. Health 2012, 11, 92. [Google Scholar] [CrossRef] [PubMed]
- Mandiá, N.; Bermejo-Barrera, P.; Herbello, P.; López-Suárez, O.; Fraga, J.M.; Fernández-Pérez, C.; Couce, M.L. Human Milk Concentrations of Minerals, Essential and Toxic Trace Elements and Association with Selective Medical, Social, Demographic and Environmental Factors. Nutrients 2021, 13, 1885. [Google Scholar] [CrossRef] [PubMed]
- Salmani, M.H.; Mozaffari-Khosravi, H.; Rezaei, Z. The Nickel Concentration in Breast Milk during the First Month of Lactation in Yazd, Center of Iran. Biol. Trace Elem. Res. 2016, 174, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Paiders, J. Saimniecības ģeogrāfija un Latvijas vieta pasaulē. In Latvija: Zeme, Daba, Tauta, Valsts; Nikodemus, O., Kļaviņš, M., Krišjāne, Z., Zelčs, V., Eds.; Latvijas Universitātes Akadēmiskais apgāds: Riga, Latvia, 2018; pp. 521–567. [Google Scholar]
- Tabors, G.; Brūmelis, G.; Nikodemus, O.; Dobkeviča, L.; Viligurs, K. Decreased atmospheric deposition of heavy metals in Latvia shown by long-term monitoring using the moss Pleurozium schreberi. Environ. Sci. Pollut. Res. Int. 2023, 30, 94361–94370. [Google Scholar] [CrossRef] [PubMed]
- SLLC “Latvian Environment, Geology and Meteorology Centre”. 2022 Latvia’s Informative Inventory Report Submitted under the Convention on Long-Range Transboundary Air Pollution. Available online: https://videscentrs.lvgmc.lv/files/Gaiss/Gaisa_piesarnojums/2022_kops.pdf (accessed on 8 May 2024).
- EN 15763:2010; Foodstuffs—Determination of Trace Elements—Determination of Arsenic, Cadmium, Mercury and Lead in Foodstuffs by Inductively Coupled Plasma Mass Spectrometry (ICP-MS) after Pressure Digestion. European Committee for Standardization: Brussels, Belgium, 2010.
- ISO 17294-1:2004; Water Quality—Application of Inductively Coupled Plasma Mass Spectrometry (ICP-MS)—Part 1: General Guidelines. ISO: Geneva, Switzerland, 2004.
- ISO 17294-2:2016; Water Quality—Application of Inductively Coupled Plasma Mass Spectrometry (ICP-MS)—Part 2: Determination of Selected Elements Including Uranium Isotopes. ISO: Geneva, Switzerland, 2006.
- Institute of Medicine (US) Committee on Nutritional Status during Pregnancy and Lactation. Milk Volume. In Nutrition During Lactation; National Academies Press: Washington, DC, USA, 1991; pp. 80–105. [Google Scholar]
- Nahm, F.S. Nonparametric statistical tests for the continuous data: The basic concept and the practical use. Korean J. Anesthesiol. 2016, 69, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Levi, M.; Hjelm, C.; Harari, F.; Vahter, M. ICP-MS measurement of toxic and essential elements in human breast milk. A comparison of alkali dilution and acid digestion sample preparation methods. Clinic. Biochem. 2018, 53, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Noushabadi, Z.S.; Shekaftik, S.O.; Hosseini, A.F.; Ashtarinezhad, A. Blood Level of Workers in a Printing Industry. Arch. Environ. Occup. Health 2019, 3, 360–365. [Google Scholar] [CrossRef]
- European Commission. Commission Regulation (EC) No 2023/915 of 25 April 2023 on Maximum Levels for Certain Contaminants in Food and Repealing Regulation (EC) No 1881/2006. 2023. Available online: https://eur-lex.europa.eu/legal-content/EN/TXT/PDF/?uri=CELEX:32023R0915 (accessed on 8 May 2024).
- Order of the Cabinet of Ministers No. 359 of the Republic of Latvia. Adopted 26 May 2022. Public Health Guidelines for the year 2021–2027. Available online: https://likumi.lv/ta/id/332751-sabiedribas-veselibas-pamatnostadnes-2021-2027-gadam (accessed on 8 May 2024).
- Centre for Disease Prevention and Control of Latvia. Health Statistics Database. Data on Breastfeeding. Available online: https://statistika.spkc.gov.lv/pxweb/lv/Health/Health__Mates_berna_veseliba/MCH100_kruts_barosana.px/ (accessed on 8 May 2024).
- Theurich, M.A.; Davanzo, R.; Busck-Rasmussen, M.; Díaz-Gómez, N.M.; Brennan, C.; Kylberg, E.; Bærug, A.; McHugh, L.; Weikert, C.; Abraham, K.; et al. Breastfeeding Rates and Programs in Europe. A Survey of 11 National Breastfeeding Committees and Representatives. J. Pediatr. Gastroenterol. Nutr. 2019, 68, 400–407. [Google Scholar] [CrossRef]
- Rollins, N.; Piwoz, E.; Baker, P.; Kingston, G.; Mabaso, K.M.; McCoy, D.; Ribeiro Neves, P.A.; Pérez-Escamilla, R.; Richter, L.; Russ, K.; et al. Marketing of commercial milk formula: A system to capture parents, communities, science, and policy. Lancet 2023, 401, 486–502. [Google Scholar] [CrossRef]
- Consumer Rights Protection Centre. Consumer Rights Protection Centre Calls on Influencers, Manufacturers, and Distributors of Products to Comply with the Ban on Advertising Infant Formulae. Available online: https://www.ptac.gov.lv/lv/jaunums/ptac-aicina-influencerus-razotajus-un-produktu-izplatitajus-ieverot-maksligo-maisijumu-zidainiem-reklamu-aizliegumu (accessed on 8 May 2024).
- Cabinet Regulation No. 370 of the Republic of Latvia. Adopted 26 May 2008. Regulations Regarding Infant Formulae and Follow-on Formulae for Infants. Available online: https://likumi.lv/ta/en/en/id/175983-regulations-regarding-infant-formulae-and-follow-on-formulae-for-infants (accessed on 8 May 2024).
- The Ministry of Health of the Republic of Latvia. Healthy Nutrition Recommendations for Women during Lactation Period, 2022. Available online: https://www.vm.gov.lv/lv/media/11193/download?attachment (accessed on 8 May 2024).
- Vollset, M.; Iszatt, N.; Enger, Ø.; Gjengedal, E.L.; Eggesbø, M. Concentration of mercury, cadmium, and lead in breast milk from Norwegian mothers: Association with dietary habits, amalgam and other factors. Sci. Total Environ. 2019, 677, 466–473. [Google Scholar] [CrossRef] [PubMed]
- Tratnik, J.S.; Falnoga, I.; Mazej, D.; Kocman, D.; Fajon, V.; Jagodic, M.; Stajnko, A.; Trdin, A.; Šlejkovec, Z.; Jeran, Z.; et al. Results of the first national human biomonitoring in Slovenia: Trace elements in men and lactating women, predictors of exposure and reference values. Int. J. Hyg. Environ. Health 2019, 222, 563–582. [Google Scholar] [CrossRef] [PubMed]
- Vincēviča-Gaile, Z.; Varakājs, D. Concentration of potentially toxic elements in various berries grown in allotment gardens of Rīga city, Latvia. Proc. Latv. Acad. Sect. B 2017, 6, 496–501. [Google Scholar] [CrossRef]
- Vincevica-Gaile, Z.; Klavins, M.; Rudovica, V.; Viksna, A. Research review trends in food analysis in Latvia: Major and trace element content. Environ. Geochem. Health 2013, 35, 693–703. [Google Scholar] [CrossRef] [PubMed]
- Vincevica-Gaile, Z.; Klavins, M.; Zilgalve, L. Trace and Major Element Concentration in Cottage Cheese from Latvia. In Recent Researches in Sociology, Financing, Environment & Health Sciences; Mastorakis, N., Mladenov, V., Savkovic-Stevanovic, J., Eds.; WSEAS Press: Meloneras, Spain, 2011; pp. 169–173. [Google Scholar]
- Vincevica-Gaile, Z.; Klavins, M. Concentration of Elements in Food: How Can It Reflect Impact of Environmental and Other Influencing Factors? Environ. Clim. Technol. 2014, 12, 15–19. [Google Scholar] [CrossRef]
- Vincevica-Gaile, Z.; Gaga, K.; Klavins, M. Food and Environment: Trace Element Content of Hen Eggs from Different Housing Types. APCBEE Procedia 2013, 5, 221–226. [Google Scholar] [CrossRef]
- Cherkani-Hassani, A.; Slaoui, M.; Ghanname, I.; Mojemmi, B.; Eljaoudi, R.; Belhaj, A.; Kers, B.; Flayou, M.; Mouane, N. Lead concentrations in breast milk of Moroccan nursing mothers and associated factors of exposure: CONTAMILK STUDY. Environ. Toxicol. Pharmacol. 2021, 85, 103629. [Google Scholar] [CrossRef] [PubMed]
- Latvian Environmental Protection Fund, University of Latvia. Assessment of Drinking Water Quality in Wells in Latvia, 2021. Available online: https://lvafa.vraa.gov.lv/faili/materiali/dazadi/2020/55/Akas_Latvija_atskaite_552020.pdf (accessed on 8 May 2024).
- Klavins, M.; Rodinov, V.; Cimdins, P.; Klavina, I.; Purite, M.; Druvietis, I. Well water quality in Latvia. Int. J. Environ. Sci. 1996, 50, 41–50. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Year 2016–2017, n = 66 | Year 2022–2023, n = 50 | |
|---|---|---|
| Characteristics | Mean ± Standard Deviation (Range) | |
| Maternal characteristics | ||
| Age (years) | 31 ± 4 (23–39) | 30 ± 4 (21–40) |
| Maternal body mass index 1 | 22.33 ± 3.22 (17.85–32.18) | 23.14 ± 7.00 (17.82–29.07) |
| Parity | 2 ± 1 (1–4) | 1 ± 1 (1–4) |
| Breastfeeding pattern | 39—exclusive breastfeeding, 27—partial breastfeeding (two participants combining breastfeeding and formula feeding, 25 participants combining breastfeeding with complementary feeding) | 50—exclusive breastfeeding |
| Milk expression manner | 19—by hand 38—using a breast pump 9—combining both methods | 11—by hand 31—using a breast pump 8—combining both methods |
| Child characteristics | ||
| Age (months) | 6 ± 4 (2–21) | 3 ± 1 (1–5) |
| Sex | 31—female, 35—males | 23—females, 27—males |
| Birth weight (kg) | 3.51 ± 0.59 (1.60–5.36) | 3.50 ± 0.44 (2.70–4.60) |
| Birth length (cm) | 53 ± 3 (42–61) | 53 ± 3 (49–60) |
| Element (Symbol) | Detection Limit (mg kg−1) | Year 2016–2017, n = 66 | Year 2022–2023, n = 50 |
|---|---|---|---|
| Mean (mg kg−1) (Range) | |||
| Arsenic (As) | 0.005 | <0.005 (<0.005–0.009) | not analysed |
| Cadmium (Cd) | 0.005 | <0.005 | <0.005 |
| Lead (Pb) | 0.010 | <0.010 (<0.010–0.047) | <0.010 |
| Aluminium (Al) | 5 | <5 | not analysed |
| Tin (Sn) | 0.5 | <0.5 | not analysed |
| Nickel (Ni) | 0.5 | <0.5 | not analysed |
| Food Products and Drinks Categories 1 | Year 2016–2017, n = 66 | Year 2022–2023, n = 50 | p-Value |
|---|---|---|---|
| Mean ± Standard Deviation (Range) | |||
| Cereals, cereal products | 1.02 ± 0.44 (0–2) | 1.30 ± 0.43 (0–2) | 0.031 |
| Eggs | 2.62 ± 1.54 (0–5) | 3.42 ± 1.53 (0–5) | 0.003 |
| Sweets and bakery goods | 1.40 ± 0.62 (0–3) | 2.01 ± 0.72 (0–3) | 0.002 |
| Alcohol | 0.48 ± 0.71 (0–3) | 0.00 ± 0.00 (0–0) | 0.000 |
| Element (Symbol) | This Study, Latvia | Björklund et al. (2012), Sweden [12] | Mandiá et al. (2021), Spain [13] |
|---|---|---|---|
| Arsenic (As) | <5 (<5–9.27) | 0.55 ± 0.70 (0.04–4.60) | 1.37 ± 1.82 (0.93–1.82) |
| Cadmium (Cd) | <5 | 0.09 ± 0.05 (0.03–0.27) | 0.15 ± 0.20 (0.10–0.20) |
| Lead (Pb) | <10 (<10–48.41) | 1.50 ± 0.90 (0.74–6.40) | 0.30 ± 0.23 (0.25–0.36) |
| Aluminium (Al) | <5000 | 185.00 ± 584.00 (21.00–4393.00) | 7.29 ± 1.11 (7.02–7.56) |
| Tin (Sn) | <500 | 0.40 ± 0.10 (0.21–0.77) | 0.07 ± 0.00 (0.07–0.07) |
| Nickel (Ni) | <500 | 0.96 ± 6.5 (<0.085–47.00) | 2.35 ± 2.69 (1.69–3.00) |
| Element (Symbol) | Mean (mg kg−1) (Range) | Maximum Level Set in the Commission Regulation (CE) No. 2023/915 (mg kg−1) [25] |
|---|---|---|
| Arsenic (As) | <0.005 (<0.005–0.009) | 0.020 (infant formulae and follow-on formulae marketed as powder) 0.010 (infant formulae and follow-on formulae marketed as liquid) |
| Cadmium (Cd) | <0.005 | 0.010 (infant formulae, follow-on formulae marketed as powder and manufactured from cow’s milk proteins or from cow’s milk protein hydrolysates) 0.005 (infant formulae, follow-on formulae marketed as liquid and manufactured from cow’s milk proteins or from cow’s milk protein hydrolysates) |
| Lead (Pb) | <0.010 (<0.010–0.047) | 0.020 (infant formulae and follow-on formulae marketed as powder) 0.010 (infant formulae and follow-on formulae marketed as liquid) |
| Aluminium (Al) | <5 | Not defined |
| Tin (Sn) | <0.5 | 50 (canned infant formulae and follow-on formulae, including infant milk and follow-on milk, excluding dried and powdered products) |
| Nickel (Ni) | <0.5 | Not defined |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aumeistere, L.; Beluško, A.; Ciproviča, I. Assessment of Heavy Metals and Trace Elements in the Human Milk of Women Living in Latvia and an Evaluation of Influencing Factors. Nutrients 2024, 16, 1568. https://doi.org/10.3390/nu16111568
Aumeistere L, Beluško A, Ciproviča I. Assessment of Heavy Metals and Trace Elements in the Human Milk of Women Living in Latvia and an Evaluation of Influencing Factors. Nutrients. 2024; 16(11):1568. https://doi.org/10.3390/nu16111568
Chicago/Turabian StyleAumeistere, Līva, Alīna Beluško, and Inga Ciproviča. 2024. "Assessment of Heavy Metals and Trace Elements in the Human Milk of Women Living in Latvia and an Evaluation of Influencing Factors" Nutrients 16, no. 11: 1568. https://doi.org/10.3390/nu16111568
APA StyleAumeistere, L., Beluško, A., & Ciproviča, I. (2024). Assessment of Heavy Metals and Trace Elements in the Human Milk of Women Living in Latvia and an Evaluation of Influencing Factors. Nutrients, 16(11), 1568. https://doi.org/10.3390/nu16111568