1. Introduction
Adolescence is a crucial stage characterized by rapid physical, cognitive, and socio-emotional development occurring between the ages of 10 and 19 [
1]. During this phase, individuals establish habits and behaviors that can have a profound impact on their long-term health outcomes [
2]. One such behavior of paramount importance is healthy eating.
Healthy eating is crucial for optimal growth, development, and the prevention of chronic diseases in adolescents [
3]. It involves consuming a well-balanced diet that provides essential nutrients while limiting the intake of unhealthy foods. However, the global prevalence of unhealthy dietary behaviors among adolescents, including excessive consumption of processed foods, sugary beverages, and snacks, as well as inadequate intake of nutritious foods such as fruits and vegetables, remains a substantial public health concern [
4,
5]. Studies have indicated that the eating behaviors of the majority of adolescents fall short of healthy dietary recommendations [
6,
7]. This can potentially account for the increasing prevalence of adolescent obesity [
8,
9], which in turn elevates the risk of non-communicable diseases (NCDs) in adulthood [
10,
11]. Therefore, adolescence plays a crucial role in the formation of dietary habits, underscoring the significance of health education [
12].
The Knowledge, Attitude, Belief, and Practices (KABP/KAP) theory is an extensively utilized and well-developed cognitive theory in the field of health education research [
13]. It posits that the process of individual health behavior encompasses the acquisition of knowledge, the development of attitudes, and the formation of behaviors. Individuals will engage in healthy behaviors only when they possess a thorough understanding of health-related knowledge and cultivate positive and accurate beliefs and attitudes [
14]. Based on this theory, adolescents’ knowledge of nutrition can influence their attitudes and behaviors regarding healthy eating [
15]. Identifying gaps in adolescents’ KAP is essential for implementing effective policies promoting healthy eating behavior.
The eating behavior of individuals is influenced by a multitude of personal, familial, and social factors, which also exhibit distinct regional characteristics [
16]. Chongqing, as one of the largest cities in China, stands apart from other cities due to its diverse adolescent population, representing various socioeconomic backgrounds, cultural norms, and dietary habits. The residents of the Chongqing region are recognized for their specific cooking methods, such as stir-frying, frying, and grilling. They have a predilection for spicy and sour flavors, thus often incorporating generous amounts of oil, salt, and chili into their cuisine. Compared to Chongqing, regions such as Jiangsu and Zhejiang, which are also in the south, have lighter tastes [
17]. Research indicates that various digestive system disorders, including chronic atrophic gastritis, gastric ulcers, and Helicobacter pylori infection, are associated with unhealthy dietary habits such as heavy oil and salt intake [
18]. Among China’s population of 1.4 billion, approximately 120 million individuals suffer from gastrointestinal diseases. Among them, the incidence of gastric ulcers is 10%, and the incidence of chronic gastritis is 30% [
19]. Simultaneously, according to the digestive health monitoring data in China, the digestive health score in Chongqing is only 52.22 points (total score of 100) [
20]. This indicates that the prognosis for the prevalence of digestive system diseases in the Chongqing region is also not optimistic. Additionally, in the Chongqing area, there is a phenomenon where communal and lively dining is more popular than individual or solitary dining experiences [
21]. This unique cultural context of Chongqing further underscores the importance of studying the KAP of healthy eating among adolescents in this region. It aids in identifying culturally sensitive strategies that can effectively promote healthy eating behaviors among Chongqing’s adolescent population.
While some studies have explored the status of KAP related to diet among adolescents in certain regions of China [
22,
23,
24], there remains a dearth of evidence specifically from Chongqing. Moreover, structural equation modeling (SEM) is an analytical technique utilized to untangle intricate relationships and causal pathways while quantitatively assessing the direct and indirect effects of variables, particularly when latent constructs are involved [
25,
26]. According to the KAP theory, there is a causal relationship between knowledge, attitude, and practices [
27,
28]. Prior studies have effectively utilized SEM as a valuable tool to explore and understand the current state of KAP in various domains, including nutrition labeling [
29], influenza vaccination [
30], antibiotic prescribing [
31], and dental caries prevention [
32]. But studies employing structural equation modeling to investigate the intricate relationships between healthy dietary KAP are exceptionally scarce in this context. Hence, our study aimed to develop a comprehensive structural equation model to analyze the relationships between knowledge, attitudes, and practices regarding healthy eating among adolescents in Chongqing. Furthermore, research has indicated that the educational environment plays a significant role in shaping the nutritional knowledge and attitudes of adolescents [
33,
34], so we sought to investigate the impact of the educational environment on the KAP of adolescents.
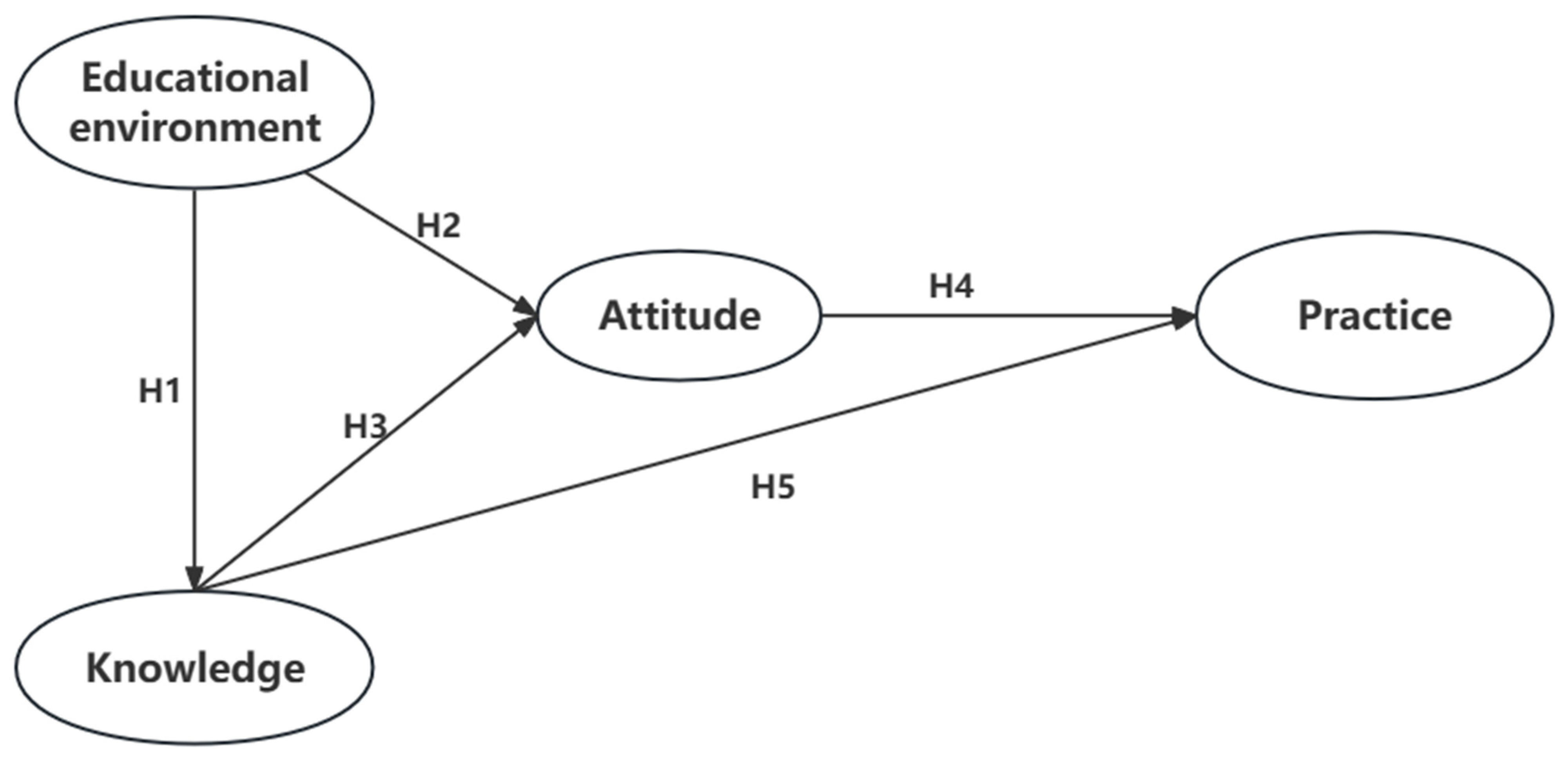
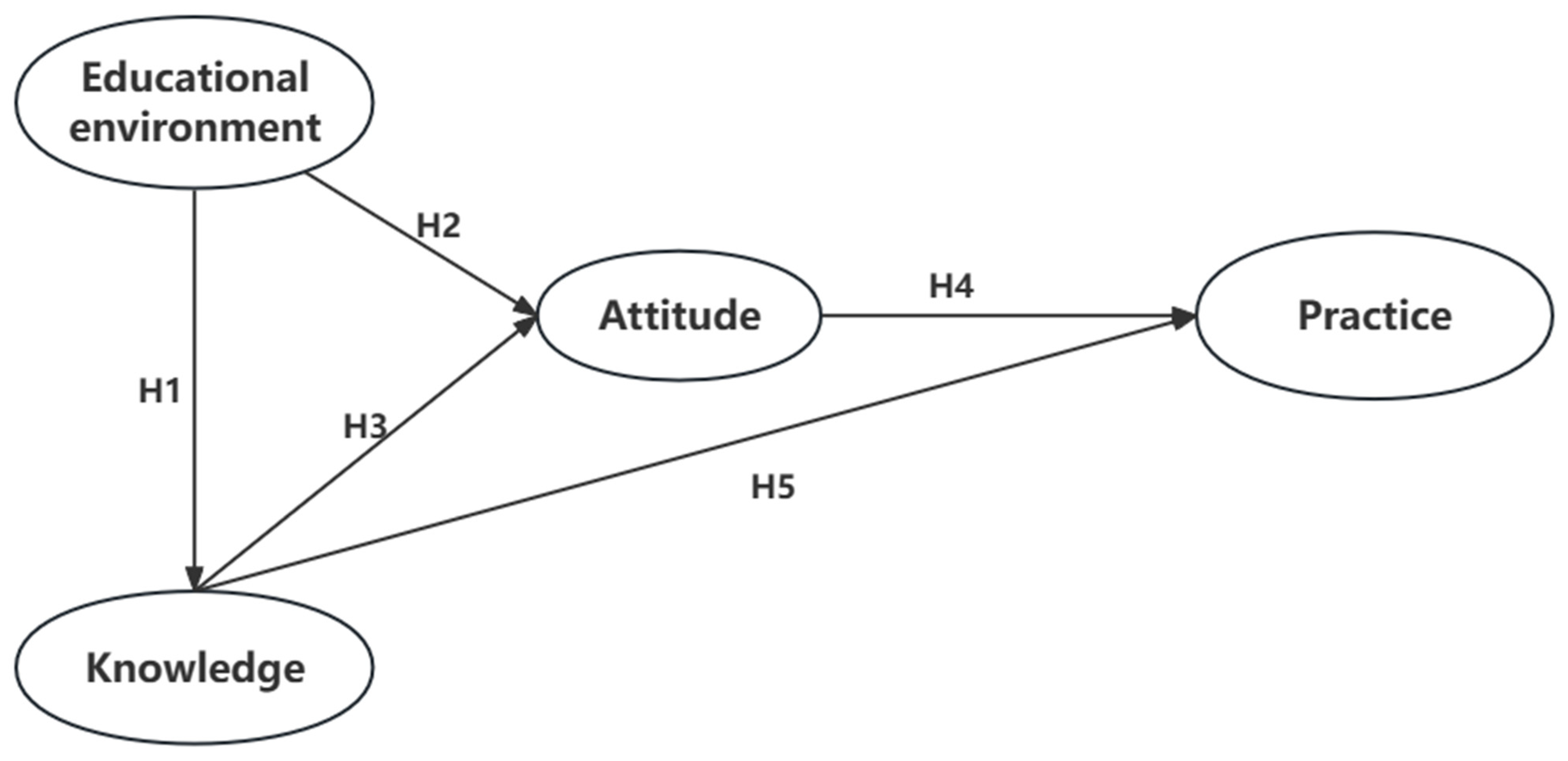
Based on the above research and theoretical foundations, we propose the following five hypotheses (
Figure 1):
Hypothesis 1 (H1): Adolescents who have a better educational environment are more likely to achieve higher scores in healthy eating knowledge.
Hypothesis 2 (H2): Adolescents who have a better educational environment are more likely to exhibit a more positive attitude towards healthy eating.
Hypothesis 3 (H3): Adolescents with higher scores in healthy eating knowledge are more likely to demonstrate a more positive attitude towards healthy eating.
Hypothesis 4 (H4): Adolescents who possess a more positive attitude towards healthy eating are more likely to engage in healthy eating practices.
Hypothesis 5 (H5): Adolescents with higher scores in healthy eating knowledge are more likely to engage in healthy eating practices.
Through the identification of specific domains where adolescents may lack adequate knowledge, possess negative attitudes, or engage in unhealthy dietary practices, our findings can inform the development of targeted interventions that effectively address these issues.
4. Discussion
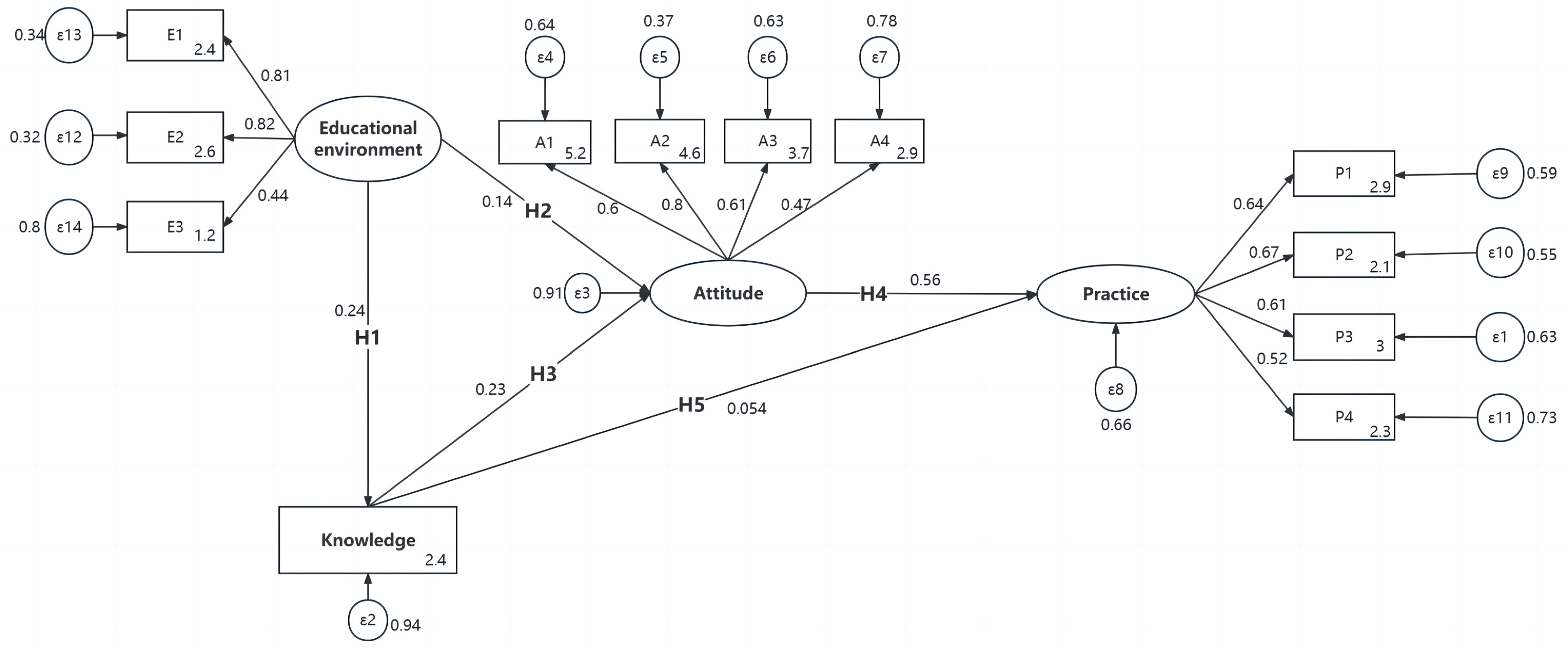
In this study, we developed a comprehensive SEM to analyze the relationship between knowledge, attitudes, and practices regarding healthy eating among adolescents in Chongqing. The study revealed a significant positive relationship between healthy eating-related knowledge and attitudes, attitudes and practices, and knowledge and practices. Our findings align with the fundamental assumption of the KAP theory, which posits a positive relationship among the variables of knowledge, attitude, and practices [
44]. Moreover, similar findings have been reported in community trial research conducted in the United States targeting children [
45] and cross-sectional studies focused on international students in Ireland [
15], as well as cross-sectional studies involving adolescent schoolgirls in Bangladesh [
46]. Furthermore, it is noteworthy that although the path coefficient for the direct effect of knowledge on practices is statistically significant, it is relatively small (only 0.054). In contrast, the coefficient for the indirect effect of knowledge on practices with attitude as the mediating variable is 0.127. The magnitude of the indirect effect is significantly greater than that of the direct effect, indicating the crucial role of attitude in the causal chain of knowledge, attitude, and practices [
30]. This result means our health knowledge education is effective and suggests that when adolescents receive nutrition education, they are more likely to develop positive beliefs and eventually change their behaviors related to nutrition [
47].
Furthermore, our study revealed a significant association between a favorable educational environment and improved knowledge of healthy eating as well as more positive attitudes toward healthy eating among adolescents. These findings align with previous studies [
48,
49,
50]. This suggests that both parental education and the urban environment can play important roles in shaping individuals’ understanding and attitudes regarding healthy eating. In China, most highly educated people live in urban areas [
51]. This urban setting provides a favorable environment for the implementation of school-based nutrition education initiatives and targeted public health campaigns aimed at promoting healthy eating habits among adolescents [
52]. These interventions focus on delivering information about the importance of balanced nutrition, the benefits of specific food groups, and practical strategies for making healthier choices [
53]. Furthermore, parents with higher levels of education in urban areas are often more aware of the significance of healthy eating and actively seek out and utilize available resources and information. They play a crucial role in imparting their knowledge to their adolescent children through conversations, acting as role models, and creating an environment that supports healthy eating habits [
54]. Parental education is frequently associated with higher socioeconomic status, which can further influence adolescents’ access to resources and opportunities for healthy eating [
55,
56]. The advantages of the educational environment in urban areas, as mentioned above, contribute to improved knowledge and positive attitudes toward healthy eating among adolescents. It is imperative to acknowledge that these findings should not undermine the significance of promoting healthy eating behaviors in rural or socioeconomically disadvantaged areas. Access to resources, educational programs, and support for healthy eating should be made accessible and equitable across all communities.
Although the results of this study showed that adolescents’ knowledge, attitudes, and practices of healthy eating were unsatisfactory. However, there are still some results worth noting. Specifically, the correct rate related to nutrition labels was the highest, followed by the awareness rate of diseases caused by long-term consumption of sugary drinks. It may be because teenagers are in a critical period of growth and development, and sugary drinks are popular during their growth. Studies have shown that adolescents are an important target group for nutrition intervention, and the prevalence of obesity and other phenomena has stimulated people’s interest in improving adolescent nutrition education [
57]. Therefore, schools and parents have greater publicity and education in this regard, and parents have greater supervision of children’s related eating behaviors. Parents in many countries are encouraging their children to buy prepackaged foods by identifying and understanding nutritional labels [
51]. Six countries—Australia, Canada, Chile, Mexico, the United Kingdom, and the United States—have generally higher awareness of nutrition labels among children and adolescents [
58]. Compared to other countries, China also needs to strengthen nutrition education on “how to interpret nutrition labels”. For the awareness rate of diseases caused by the consumption of sugary drinks, the prevalence of knowledge about the health status of drinking sugary drinks was similar in different studies. For example, relevant studies in the United States and Australia were similar to the results of this study [
59]. However, the discussion on the correlation between knowledge of sugary drinks and the intake behavior related to sugary drinks among adolescents was not carried out in this study. However, this study was not conducted to explore the correlation between knowledge about sugary drinks and the consumption behavior related to sugary drinks among adolescents. The results of this study show that nearly half of middle school students are willing to use knowledge to guide their daily behavior. Future research could further track healthy eating behaviors, such as how often children and adolescents pay attention to nutrition labels when purchasing pre-packaged foods and limiting consumption of sugar-sweetened beverages.
According to the results of this study, more people hold a neutral attitude toward the food safety risks of roadside stalls. In addition to conducting food safety-related education activities for middle school students, the relevant departments should also strengthen the food hygiene and safety awareness of food operators around schools. The owners of “roadside stalls” should be reminded of food safety risks, and food safety knowledge such as fast inspection of edible agricultural products and toxic and harmful products should be propagandized to improve the food safety awareness of “roadside stall” food operators.
The advantages of this study are as follows: firstly, it employs an SEM approach to rigorously examine the theoretical framework rooted in the well-established KAP model. Remarkably, this study stands as the pioneering endeavor utilizing SEM to delve into the intricate interplay between knowledge, attitudes, and practices concerning healthy eating within the adolescent population of Chongqing. Secondly, a notable strength lies in the substantial sample size, ensuring the representativeness and reliability of our research results. However, there are still a few limitations in the present study. Firstly, this study is conducted as a cross-sectional study, which means that it captures data at a single point in time. However, it is important to recognize that dietary behavior change is a complex process that may occur over a long period. Therefore, longitudinal studies are necessary to examine the causal relationship between knowledge, attitudes, and behaviors related to diet. Secondly, it is important to acknowledge that the survey in this study primarily relied on online platforms. However, it is worth considering that relying solely on online platforms may introduce biases and potential inaccuracies in the data collected. Not all individuals have equal access to the internet, and the online sample may not be fully representative of the target population. In addition, this study was about adolescents whose data in terms of height and weight were self-reported, which may lead to the presence of bias due to subjective factors or other reasons. Lastly, it is important to acknowledge that the dimensions of healthy eating KAP are abstract constructs, lacking a widely accepted consensus on precise measurement variables. Consequently, the measurement variables employed in this study may not capture the entirety of knowledge, attitudes, and behaviors regarding a healthy diet. Therefore, further research endeavors should aim to explore and establish a more comprehensive understanding and definition of individuals’ healthy eating knowledge, attitudes, and behaviors.





 ,
, 


{kind=link}
{kind=link}