
Healthy Eating in the Spanish University Community: A Case Study


Abstract
1. Introduction
2. Materials and Methods
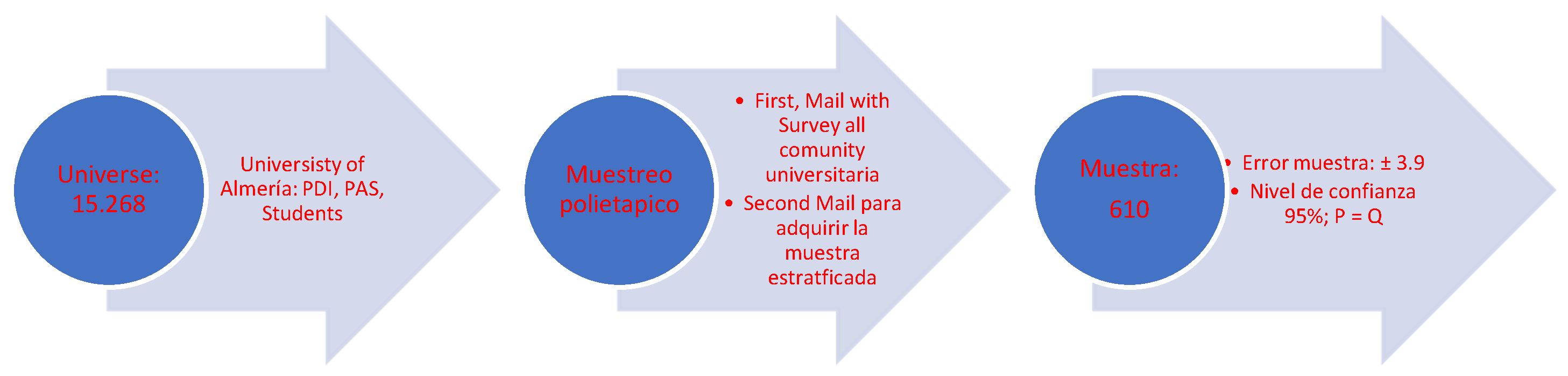
2.1. Participants
2.2. Instrument
- -
- The ratio of monounsaturated fatty acids to saturated fatty acids (MUFA/SFA according to the Spanish Food Composition Database (BEDCA) [28].
- -
- High consumption of vegetables, legumes, fruit and nuts, cereals, and fish.
- -
- Moderate consumption of alcohol, milk, and dairy products.
- -
- Low consumption of meat and derivatives.
2.3. Procedure
3. Results and Discussion
4. Conclusions
Intervention Plan
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Ethical Considerations
References
- Organización Mundial de la Salud. Enfermedades No Transmisibles. 2018. Available online: https://www.who.int/es/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 23 March 2023).
- Jimeno-Martínez, A.; Maneschy, I.; Rupérez, A.I.; Moreno, L.A. Factores determinantes del comportamiento alimentario y su impacto sobre la ingesta y la obesidad en niños. J. Behav. Feed. 2021, 1, 60–71. [Google Scholar]
- Dressl, N.L.; Balzaretti, M.L.; Barrosela, V.B.; Deluchi, D.; Rioja, M.; Torresani, E. Factores influyentes en la alimentación emocional y el riesgo de trastornos de la conducta alimentaria en mujeres adultas. Rev. Nutr. Investig. 2019, 102–147. [Google Scholar]
- Sozoranga, D.; León, D.; Mediavilla, C.; Palchisaca, Z. Comportamiento alimentario, actividad física e intención de práctica en estudiantes de bachillerato durante la pandemia. Polo Conoc. Rev. Cient. Prof. 2020, 5, 147–162. [Google Scholar]
- Agencia Española de Seguridad Alimentaria. Informe del Comité Científico de la Agencia Española de Seguridad Alimentaria y Nutrición Sobre Recomendaciones Dietéticas Saludables y Sostenibles Complementadas con Recomendaciones de Actividad Física Para la Población Española.; Ministerio de Consumo: Madrid, Spain, 2022.
- Keys, A. Coronary heart disease, serum cholesterol, and the diet. Acta Med. Scand. 1980, 207, 153–160. [Google Scholar] [CrossRef]
- Serra, L.; Ribas, L.; García, R.; Pérez, C.; Peña, L.; Aranceta, J. Hábitos alimentarios y consumo de alimentos en la población infantil y juvenil española (1998–2000): Variables socioeconómicas y geográficas. Med. Clín. 2002, 121, 126–131. [Google Scholar]
- Sánchez, M.; García, A.; Hidalgo, J.; García, M.Á.; Tarín, J.; Cano, A. Dieta mediterránea y salud: Una revisión sistemática de estudios epidemiológicos y ensayos de intervención. Maturitas 2020, 136, 25–37. [Google Scholar]
- Romagnolo, D.; Selmin, O. Mediterranean diet and prevention of chronic diseases. Nutr. Today 2017, 52, 208. [Google Scholar] [CrossRef]
- Sotos, M.; Mattei, J. Mediterranean diet and cardiometabolic diseases in racial/ethnic minority populations in the United States. Nutrients 2018, 10, 352. [Google Scholar] [CrossRef]
- Agencia Española de Seguridad Alimentaria. Informe del Comité Científico de la Agencia Española de Seguridad Alimentaria y Nutrición Sobre Recomendaciones Dietéticas Sostenibles y Recomendaciones de Actividad Física Para la Población; Ministerio de Consumo: Madrid, Spain, 2022.
- Caplliure, J.; Peralta, T.; Carrera, S.; Cuerda, M.; Drehmer, E.; López, M.; De la Rubia Ortí, J.E. Alternativa terapéutica de la dieta mediterránea cetogénica para mejorar la actividad mitocondrial en la Esclerosis Lateral Amiotrófica (ELA): Una Revisión Integral. Cienc. Aliment. Nutr. 2020, 8, 23–35. [Google Scholar]
- Failde, J.M.; Ruiz, L.; Pérez, M.R.; Lameiras, M.; Rodríguez, Y. Evolución de la calidad de vida y comportamientos relacionados con la salud en estudiantes universitarios españoles. Rev. Int. Planif. Gest. Salud 2019, 34, 789–801. [Google Scholar]
- Guzmán, M.; Lobo, M. Beneficios de la reducción del consumo de azúcares y aumento de la actividad física en adultos jóvenes con obesidad y la prevención de la diabetes. Acta Acad. 2020, 67, 185–194. [Google Scholar]
- Trichopoulos, D. Diet and survival of elderly greeks-a link to the past. Am. J. Clin. Nutr. 1995, 61, S1346–S1350. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Bamia, C.; Trichopoulos, D. Anatomy of health effects of Mediterranean diet: Greek EPIC prospective cohort study. Br. Med. J. 2009, 338, b2337. [Google Scholar] [CrossRef] [PubMed]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean diet and survival in a Greek population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef]
- Troncoso, C.; Amaya, J.P. Factores sociales en las conductas alimentarias de estudiantes universitarios. Rev. Chil. Nutr. 2009, 36, 1090–1097. [Google Scholar] [CrossRef]
- Vilarnau, C.; Stracker, D.; Funtikov, A.; da Silva, R.; Estruch, R.; Bach-Faig, A. Worldwide adherence to Mediterranean Diet between 1960 and 2011. Eur. J. Clin. Nutr. 2019, 72 (Suppl. S1), 83–91. [Google Scholar] [CrossRef]
- Serra, L.; Castro, I.; Ruano, C. La Dieta Mediterránea: Claves y Evolución en España; Panorama Social: Madrid, Spain, 2014. [Google Scholar]
- Vall, H.; Andrés, A.; Saldaña, C. El impacto de la pandemia por covid-19 y del confinamiento en las alteraciones alimentarias y el malestar emocional en adolescentes y jóvenes de España. Behav. Psychol. 2021, 29, 345–364. [Google Scholar] [CrossRef]
- Bravo, S.; Castillo, A.; Izquierdo, D.; Rodas, P. Hábitos alimenticios, nocivos y rendimiento académico en estudiantes universitarios en tiempos de COVID-19. Vive Rev. Salud 2021, 4, 225–238. [Google Scholar]
- Rojas, J.A. Alimentación emocional durante tiempos de COVID-19 en adultos jóvenes de 18 a 29 años. Rev. Mex. Med. Forense Cienc. Salud 2020, 5, 66–71. [Google Scholar]
- Esparza, L.; Cruzado, A.; Dávila, M.; Díaz, Y.; La Cruz, D.; Ascoy, B.; Huamán, J. Modificaciones de la conducta alimentaria, actividad física y salud mental por la cuarentena COVID-19 en adultos jóvenes. Rev. Med. Herediana 2022, 33, 15–23. [Google Scholar] [CrossRef]
- Instituto Nacional de Estadística. Encuesta Nacional de Salud. Ministerio de Sanidad-Secretaría General de Salud Digital, Información e Innovación del Sistema Nacional de Salud; INE: Madrid, Spain, 2022.
- López, P.J.T.; Marcos, A.T.; Royo, J.M.P.; Carbayo, J.A.H.; Marcos, M.L.T.; Gil, J.F.L. Physical activity and its association with Mediterranean diet patterns among Spanish university students. Nutr. Hosp. Organo Of. Soc. Esp. Nutr. Parenter. Enter. 2022, 39, 603–609. [Google Scholar]
- Padial, R.; Viciana, M.; Palomares, J. Adherencia a la dieta mediterránea, la actividad física y su relación con el IMC, en estudiantes universitarios del grado de primaria, mención de educación física, de Granada. Educ. Sport Health Phys. Act. 2018, 2, 30–49. [Google Scholar] [CrossRef]
- Ministerio de Sanidad, Servicios Sociales e Igualdad. In Base de Datos Española de Composición de Alimentos. Available online: https://www.bedca.net/ (accessed on 23 March 2023).
- Giménez, N. Estudio Nutricional de Población Mediterránea Situada en el Sureste Español y su Relación con Patologías Asociadas al Estado Nutricional. Ph.D. Thesis, Universidad de Murcia, Murcia, Spain, 2019. [Google Scholar]
- Hodge, A.M.; Bassett, J.K.; Shivappa, N.; Hebert, J.R.; English, D.R.; Giles, G.G.; Severi, G. Dietary inflammatory index, Mediterranean diet score, and lung cancer: A prospective study. Cancer Causes Control 2016, 27, 907–917. [Google Scholar] [CrossRef] [PubMed]
- García-Gabarra, A.; Castellà-Soley, M.; Calleja-Fernández, A. Ingestas de energía y nutrientes recomendadas en la Unión Europea: 2008–2016. Nutr. Hosp. 2017, 34, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Medina, F.X.; Aguilar, A.; Solé, J.M. Aspectos sociales y culturales sobre la obesidad: Reflexiones necesarias desde la salud pública. Nutr. Clín. Diet. Hosp. 2014, 34, 67–71. [Google Scholar]
- Ruiz, E.; Ávila, J.M.; Valero, T.; Del Pozo, S.; Rodríguez, P.; Aranceta, J.; Varela, G. Ingesta, perfil y fuentes dietéticas de energía en la población española: Resultados del estudio ANIBES. Nutrientes 2015, 7, 4739–4762. [Google Scholar] [CrossRef]
- Moncada, R.; Norte, A.; Zaragoza, A.; Fernández, J.; Davó, M. ¿Siguen patrones de dieta mediterránea los universitarios españoles? Nutr. Hosp. 2012, 27, 1952–1959. [Google Scholar]
- Pastor, R.; Bibiloni, M.D.M.; Tur, J.A. Patrones de consumo de alimentos en estudiantes universitarios de Zamora. Nutr. Hosp. 2017, 34, 1424–1431. [Google Scholar]
- Pérez, L.; Mingo, T.; Bayona, I.; Ferrer, M.; Márquez, E.; Ramírez, R.; Navas, C.; Navas, F. Calidad de la dieta en estudiantes universitarios con distinto perfil académico. Nutr. Hosp. 2015, 31, 2230–2239. [Google Scholar]
- Redondo, M.P.; Mateo, B.; Carreño, L.; Marugán, J.M.; Fernández, M.; Camina, M. Ingesta dietética y adherencia a la dieta mediterránea en un grupo de estudiantes universitarios en función de la práctica deportiva. Nutr. Hosp. 2016, 33, 1172–1178. [Google Scholar] [CrossRef]
- Sánchez, V.; Aguilar Martínez, A. Hábitos alimentarios y conductas relacionadas con la salud en una población universitaria. Nutr. Hosp. 2015, 31, 449–457. [Google Scholar]
- Tárraga, A.; Panisello, J.M.; Carbayo, J.A.; López, J.F.; García, E.; Tárraga, P.J. Valoración de la adherencia a la dieta mediterránea en estudiantes universitarios de Ciencias de la Salud y su relación con el nivel de actividad física. Nutr. Hosp. 2021, 38, 814–820. [Google Scholar]
- Sánchez, M.A.; Gutiérrez, A.; Rizo, M.; Cortés, E. Estudio longitudinal sobre la adherencia al patrón de Dieta Mediterránea en estudiantes de Ciencias de la salud. Rev. Esp. Nutr. Hum. Diet. 2018, 22, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Mieziene, B.; Emeljanovas, A.; Fatkulina, N.; Stukas, R. Dietary pattern and its correlates among Lithuanian young adults: Mediterranean diet approach. Nutrients 2020, 12, 2025. [Google Scholar] [CrossRef] [PubMed]
- Santomauro, F.; Lorini, C.; Tanini, T.; Indiani, L.; Lastrucci, V.; Comodo, N.; Bonaccorsi, G. Adherence to Mediterranean diet in a sample of Tuscan adolescents. Nutrition 2014, 30, 1379–1383. [Google Scholar] [CrossRef]
- Barrios, R.; Navarrete, E.; García, M.; González, S.; Valera, D.; Checa, J.; Giménez, G.; Vioque, J. Una menor adherencia a la dieta mediterránea se asocia a una peor salud auto-percibida en población universitaria. Nutr. Hosp. 2015, 31, 785–792. [Google Scholar]
- Ramírez, R.; Márquez, E.M. Relación de la adherencia a la dieta mediterránea con el imc y la actividad física realizada en estudiantes universitarios. Rev. Int. Deportes Colect. 2016, 26, 36–43. [Google Scholar]
- Benítez, A.; Sánchez, S.; Franco, L.; Bermejo, M.; Cubero, J. Adhesión a la dieta mediterránea en estudiantes de la Universidad de Extremadura: Un recurso en educación para la salud. Rev. Fund. Educ. Méd. 2016, 19, 287–289. [Google Scholar] [CrossRef]
- Dernini, S.; Berry, E. Mediterranean diet: From a healthy diet to a sustainable dietary pattern. Front. Nutr. 2015, 2, 15. [Google Scholar] [CrossRef]
- Alonso, R.; García, L.; Patino, M.C.; Sánchez, N.; Gómez, M.; Recio, J. Effectiveness of a multifactorial intervention in increasing adherence to the Mediterranean diet among patients with diabetes mellitus type 2: A controlled and randomized study (EMID study). Nutrients 2019, 11, 162. [Google Scholar] [CrossRef]
- Talegawkar, S.A.; Bandinelli, S.; Bandeen-Roche, K.; Chen, P.; Milaneschi, Y.; Tanaka, T.; Semba, R.D.; Guralnik, J.M.; Ferrucci, L. A higher adherence to a Mediterranean-style diet is inversely associated with the development of frailty in community-dwelling elderly men and women. J. Nutr. 2012, 142, 2161–2166. [Google Scholar] [CrossRef] [PubMed]
- Chumacero Moscoso, J.L. El ser y el Deber ser de la Mujer y del Hombre en el Cuidado Remunerado de Ancianos en Segovia. Master’s Thesis, Universidad de Valladolid, Valladolid, Spain, 2018. [Google Scholar]
- Martínez, L.M.M.; Araiza, A.; Uriarte, A.G.; Cólera, M.C.P. Género, espacio doméstico y socialización del cuidado: Algunas perspectivas de cambio. Int. J. Dev. Educ. Psychol. Infad. Rev. Psicol. 2011, 5, 181–186. [Google Scholar]
- Abalde, N.; Pino, M. Familia, escuela y adherencia a la dieta mediterránea en infancia y adolescencia. Rev. Estud. Investig. Psicol. Educ. 2017, 5, 212–217. [Google Scholar]
- Frías Armenta, M.; Barrios Gaxiola, M.I. Recursos que contribuyen al desarrollo positivo en jóvenes. Escr. Psicol. 2016, 9, 37–44. [Google Scholar] [CrossRef]
- González, G.; Padial, R.; Espejo, E.; Chacón, R.; Puertas, P.; Pérez, A.J. Relación entre clima motivacional hacia el deporte y adherencia a la dieta mediterránea en estudiantes universitarios de educación física. Int. J. Dev. Educ. Psychol. 2017, 4, 285–295. [Google Scholar] [CrossRef]
- Monserrat, M.; Arjona, Á.; Checa, J.C.; Salguero, D. Relationship between Negative Running Addiction and Eating Disorder Patterns in Runners. Nutrients 2021, 13, 4344. [Google Scholar] [CrossRef]
- Checa, J.C.; Arjona, Á.; Rocamora, P.; Monserrat, M. Protocolo de Actuación Programa ASASO-UAL. Inscrito en el Registro General de la Propiedad Intelectual el 4/3/2022 con Número de Asiento Registral 04/2022/3684. 2022. Available online: http://hdl.handle.net/10835/13980 (accessed on 23 March 2023).




{kind=link}
{kind=link}
{kind=link}
| % | ||
|---|---|---|
| Sex | Women | 64.7 |
| Men | 34.1 | |
| Origin | Spanish | 92.5 |
| International | 7.5 | |
| Role or profession | Students | 59.7 |
| Professors | 23 | |
| Administration and services personnel | 17.3 | |
| Work or study center | School of Engineering | 6.4 |
| Faculty of Education | 14.8 | |
| Faculty of Health Sciences | 14.8 | |
| Faculty of Economics and Business Sciences | 9.8 | |
| Faculty of Experimental Sciences | 14.1 | |
| Faculty of Law | 6.2 | |
| Faculty of Humanities | 4.9 | |
| Faculty of Psychology | 11.5 | |
| International School of Doctoral Programmes | 9.2 | |
| Management and Administration Services | 8.4 |
| Food Group | Servings Recommended (BEDCA *) | % Surveyed Who Follow Recommendations (Total) |
|---|---|---|
| Water | 1.5 to 2 L of water per day. | 8.8% |
| Vegetables | Minimum 2 servings per day. | 90.7% |
| Cereals | 1–2 servings per day, preferably the whole-grain variety. | 42.2% |
| Olive oil | 2–3 servings per day. | 56.4% |
| Fruit | 2–3 servings per day. | 24.7% |
| Dairy products | 2–3 servings per day. | 63.8% |
| Nuts and seeds | 1–2 servings per day. | 67.6% |
| Fish | 2–3 servings per week. ** | 64.5% oily fish; 83.4% white fish |
| White meat | 2 servings per week. | 58.2% |
| Red meat | No more than 2 servings per week. | 93.55% |
| Salt | To reduce consumption or avoid it by substituting it with spices. | 46% |
| Processed food | Less than once per week. | 40.2% |
| Sweets | Less than 2 servings per week. | 23.9% |
| Wine | With moderation and respecting customs. | 46% |
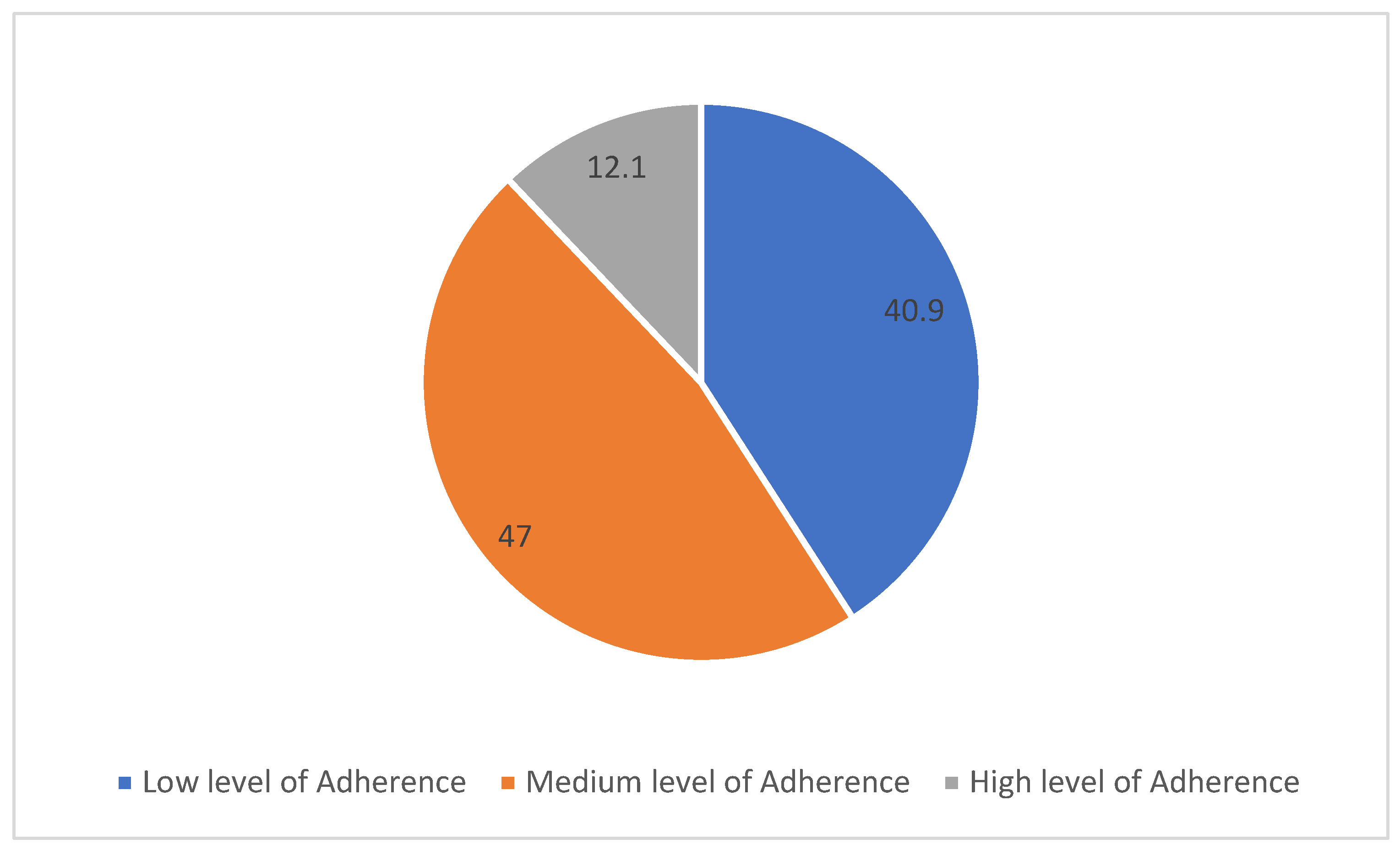
| Score | N | % |
|---|---|---|
| 1.00 | 153 | 25.1 |
| 2.00 | 34 | 5.6 |
| 3.00 | 62 | 10.2 |
| 4.00 | 92 | 15.1 |
| 5.00 | 105 | 17.2 |
| 6.00 | 90 | 14.8 |
| 7.00 | 48 | 7.9 |
| 8.00 | 26 | 4.3 |
| Total | 610 | 100.0 |
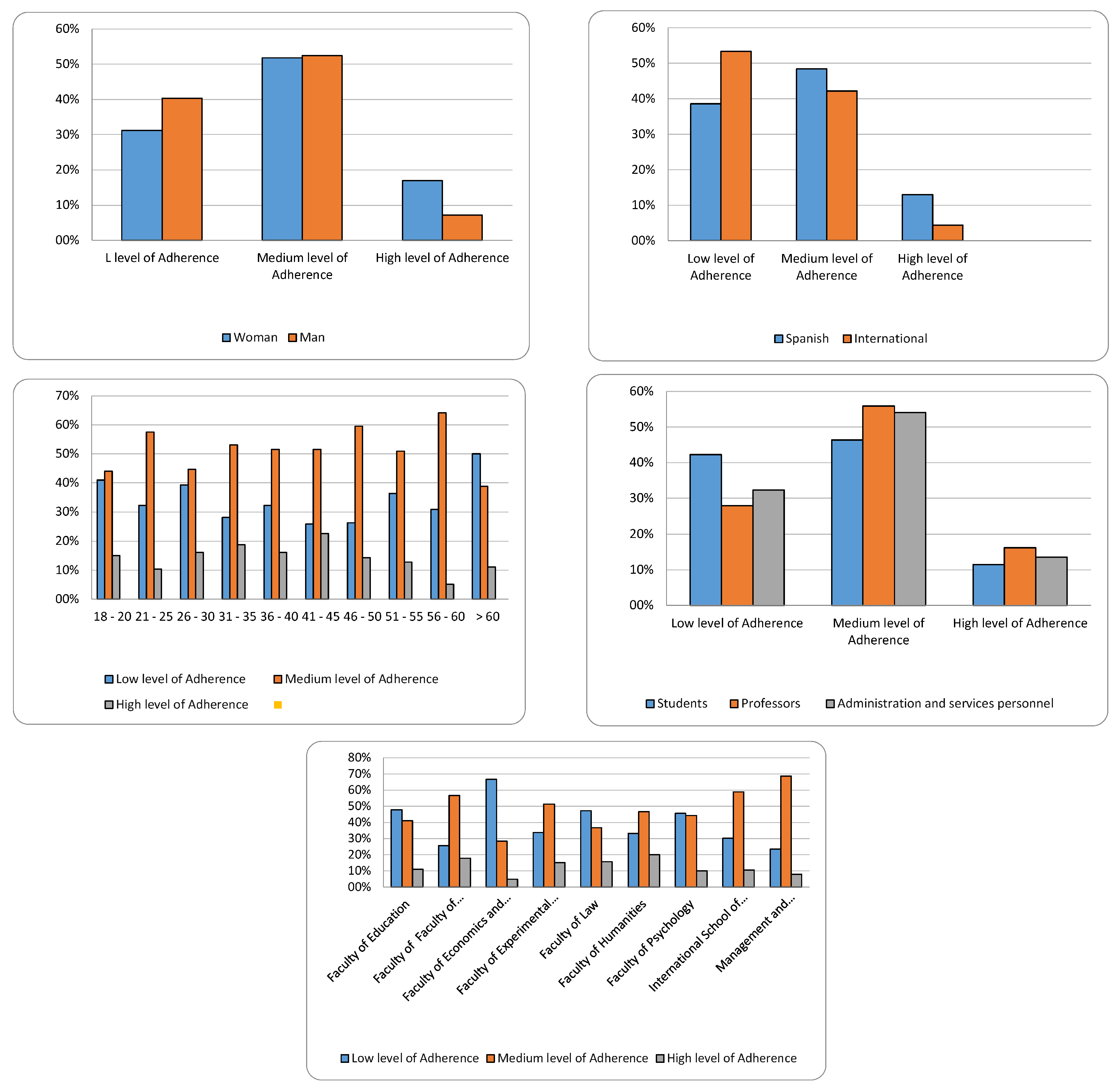
| Low Level of Adherence | Medium Level of Adherence | High Level of Adherence | ||
|---|---|---|---|---|
| Sex | Woman | 31.2% | 51.8% | 17.0% |
| Man | 40.4% | 52.5% | 7.1% | |
| Origin | Spanish | 38.6% | 48.4% | 13.0% |
| International | 53.3% | 42.2% | 4.4% | |
| Age | 18–20 | 41.0% | 44.0% | 15.0% |
| 21–25 | 32.2% | 57.5% | 10.3% | |
| 26–30 | 39.3% | 44.6% | 16.1% | |
| 31–35 | 28.1% | 53.1% | 18.8% | |
| 36–40 | 32.3% | 51.6% | 16.1% | |
| 41–45 | 25.8% | 51.6% | 22.6% | |
| 46–50 | 26.2% | 59.5% | 14.3% | |
| 51–55 | 36.4% | 50.9% | 12.7% | |
| 56–60 | 30.8% | 64.1% | 5.1% | |
| >60 | 50.0% | 38.9% | 11.1% | |
| Role or activity | Students | 42.3% | 46.3% | 11.5% |
| Professors | 27.9% | 55.9% | 16.2% | |
| Administration and services personnel | 32.4% | 54.1% | 13.5% | |
| Centre of study or work | School of Engineering | 64.1% | 28.2% | 7.7% |
| Faculty of Education | 47.8% | 41.1% | 11.1% | |
| Faculty of Health Sciences | 25.6% | 56.7% | 17.8% | |
| Faculty of Economics and Business Sciences | 66.7% | 28.3% | 5.0% | |
| Faculty of Experimental Sciences | 33.7% | 51.2% | 15.1% | |
| Faculty of Law | 47.4% | 36.8% | 15.8% | |
| Faculty of Humanities | 33.3% | 46.7% | 20.0% | |
| Faculty of Psychology | 45.7% | 44.3% | 10.0% | |
| International School of Doctoral Programmes | 30.4% | 58.9% | 10.7% | |
| Management and Administration Services | 23.5% | 68.6% | 7.8% |
| Personal Variables | Model 1 | Model 2 | Model 3 | Model 4 | |
|---|---|---|---|---|---|
| Sex (female) | 0.295 * | 0.257 * | 0.254 * | 0.264 | |
| Household type (alone) | −0.144 ** | −0.123 ** | −0.096 ** | −0.103 | |
| Origin (Spanish) | 0.179 * | 0.148 * | 0.154 * | 0.141 | |
| Role (student) | −0.097 ** | −0.083 ** | 0.044 *** | 0.038 | |
| Age | −0.054 ** | −0.050 ** | −0.155 ** | −0.141 ** | |
| School of Engineering | 0.065 *** | 0.065 *** | 0.064 *** | 0.067 | |
| Faculty of Health Sciences | 0.011 *** | 0.039 *** | 0.030 *** | 0.064 *** | |
| Faculty of Economics and Business Sciences | 0.106 *** | 0.131 *** | 0.135 *** | 0.162 *** | |
| Faculty of Experimental Sciences | −0.004 *** | −0.011 *** | 0.003 *** | 0.27 *** | |
| Faculty of Law | −0.069 *** | −0.037 *** | −0.044 *** | −0.029 *** | |
| Faculty of Humanities | 0.019 *** | 0.040 *** | 0.035 *** | 0.054 *** | |
| Faculty of Psychology | −0.090 *** | −0.042 *** | −0.036 *** | −0.035 *** | |
| International School of Doctoral Programmes | −0.006 *** | −0.044 *** | −0.056 *** | −0.045 *** | |
| Management and Administration Services | −0.058 *** | −0.043 *** | −0.040 *** | −0.034 *** | |
| Consumption habits | Read the labels | 0.159 * | 0.155 * | 0.129 * | |
| I like cooking | 0.097 ** | 0.089 ** | 0.095 ** | ||
| Snacking between meals | −0.123 ** | −0.128 ** | −0.122 ** | ||
| Plan a meal | 0.030 *** | 0.026 *** | 0.016 *** | ||
| Regular exercise | 0.149 * | 0.140 * | 0.132 * | ||
| Knowledge/ awareness | Healthy Dish | 0.123 ** | 0.015 ** | ||
| Omega-rich salmon | 0.084 *** | 0.080 *** | |||
| High GI egg | 0.019 *** | 0.015 *** | |||
| Healthy Labelling | 0.041 *** | 0.024 *** | |||
| Sustainability | Throwing food away | −0.108 ** | |||
| Interest in learning about the environment | 0.007 *** | ||||
| Recycle waste | 0.121 ** | ||||
| Type of bags I use | −0.92 *** | ||||
| Coefficient/ratio R2 | 0.241 | 0.309 | 0.318 | 0.344 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arjona Garrido, Á.; Monserrat Hernández, M.; Checa Olmos, J.C. Healthy Eating in the Spanish University Community: A Case Study. Nutrients 2023, 15, 2053. https://doi.org/10.3390/nu15092053
Arjona Garrido Á, Monserrat Hernández M, Checa Olmos JC. Healthy Eating in the Spanish University Community: A Case Study. Nutrients. 2023; 15(9):2053. https://doi.org/10.3390/nu15092053
Chicago/Turabian StyleArjona Garrido, Ángeles, Montserrat Monserrat Hernández, and Juan Carlos Checa Olmos. 2023. "Healthy Eating in the Spanish University Community: A Case Study" Nutrients 15, no. 9: 2053. https://doi.org/10.3390/nu15092053
APA StyleArjona Garrido, Á., Monserrat Hernández, M., & Checa Olmos, J. C. (2023). Healthy Eating in the Spanish University Community: A Case Study. Nutrients, 15(9), 2053. https://doi.org/10.3390/nu15092053