
Determinants of High Breastfeeding Self-Efficacy among Nursing Mothers in Najran, Saudi Arabia

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
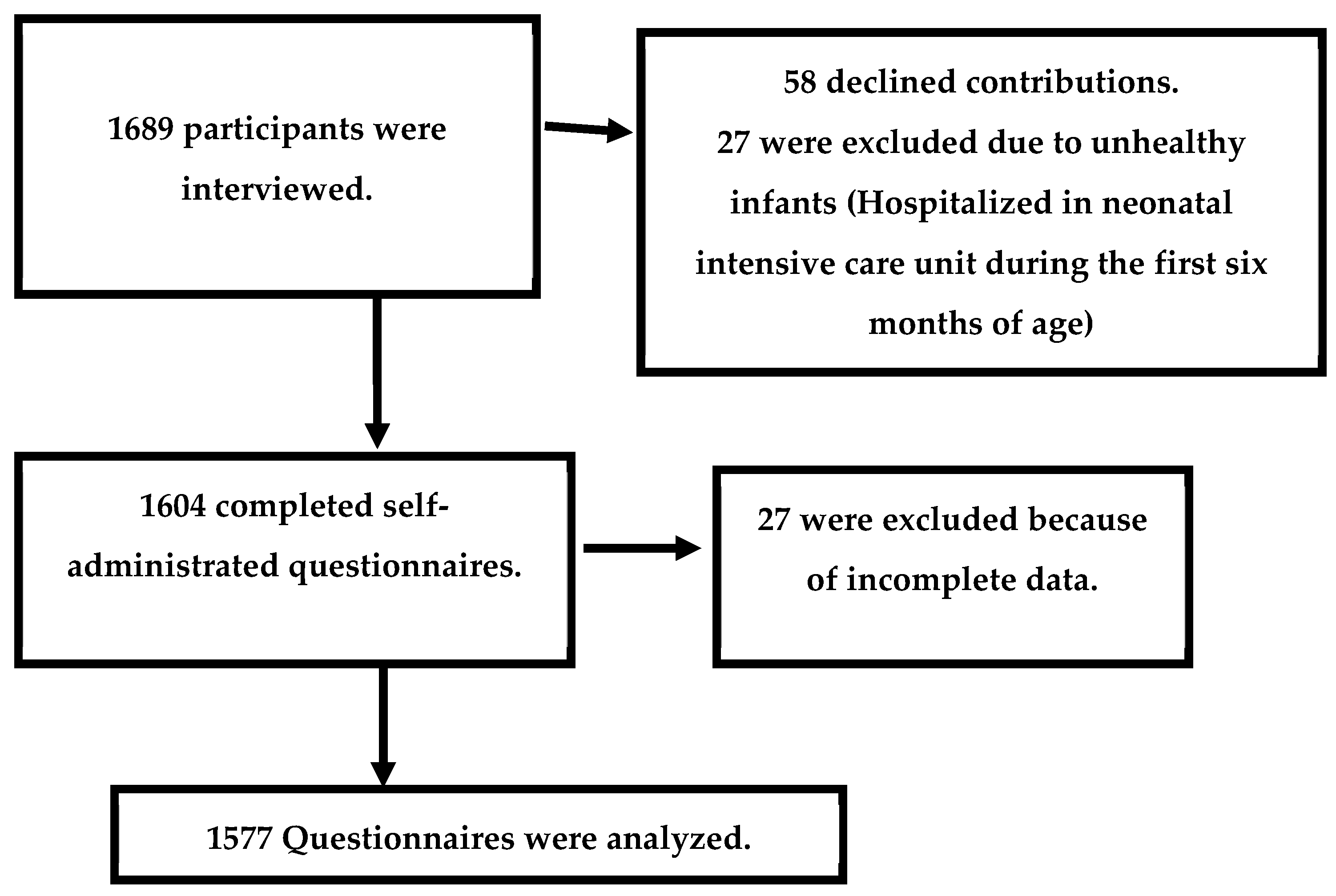
2.2. Study Participants
2.2.1. Sample Size Determinations and Sampling Procedures
2.2.2. Study Variables
2.3. Study Measurement Tools
2.4. Data Collection Procedures and Technique
2.5. Data Quality Control
2.6. Ethical Approval
2.7. Data Analysis
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AOR | Adjusted odds ratio |
| EBF | Exclusive breastfeeding |
| GFBKS | Gender-Friendly Breastfeeding Knowledge Scale |
| BSES-SF | Breastfeeding Self-Efficacy Scale—Short Form |
| BSE | Breastfeeding self-efficacy |
| IIFAS | Iowa Infant Feeding Attitude Scale |
References
- World Health Organization. WHO Breastfeeding [Internet]. Available online: https://www.who.int/health-topics/breastfeeding#tab=tab_1 (accessed on 25 January 2023).
- Zhu, J.; Dingess, K.A. The Functional Power of the Human Milk Proteome. Nutrients 2019, 11, 1834. [Google Scholar] [CrossRef] [PubMed]
- Wesolowska, A.; Brys, J.; Barbarska, O.; Strom, K.; Szymanska-Majchrzak, J.; Karzel, K.; Pawlikowska, E.; Zielinska, M.A.; Hamulka, J.; Oledzka, G. Lipid Profile, Lipase Bioactivity, and Lipophilic Antioxidant Content in High Pressure Processed Donor Human Milk. Nutrients 2019, 11, 1972. [Google Scholar] [CrossRef] [PubMed]
- Oddy, W.H. Breastfeeding, Childhood Asthma, and Allergic Disease. Ann. Nutr. Metab. 2017, 70 (Suppl. S2), 26–36. [Google Scholar] [CrossRef] [PubMed]
- Nuzzi, G.; Trambusti, I.; DICicco, M.E.; Peroni, D.G. Breast milk: More than just nutrition! Minerva Pediatr. 2021, 73, 111–114. [Google Scholar] [CrossRef]
- da Silva, M.d.C.; Oliveira Assis, A.M.; Pinheiro, S.M.; de Oliveira, L.P.; da Cruz, T.R. Breastfeeding and maternal weight changes during 24 months postpartum: A cohort study. Matern. Child Nutr. 2015, 11, 780–791. [Google Scholar] [CrossRef] [PubMed]
- Calik-Ksepka, A.; Stradczuk, M.; Czarnecka, K.; Grymowicz, M.; Smolarczyk, R. Lactational Amenorrhea: Neuroendocrine Pathways Controlling Fertility and Bone Turnover. Int. J. Mol. Sci. 2022, 23, 1633. [Google Scholar] [CrossRef]
- Binns, C.; Lee, M.; Low, W.Y. The Long-Term Public Health Benefits of Breastfeeding. Asia-Pac. J. Public Health 2016, 28, 7–14. [Google Scholar] [CrossRef]
- Al Juaid, D.A.; Binns, C.W.; Giglia, R.C. Breastfeeding in Saudi Arabia: A review. Int. Breastfeed J. 2014, 9, 1. [Google Scholar] [CrossRef]
- Rosenblad, A.K.; Funkquist, E.L. Self-efficacy in breastfeeding predicts how mothers perceive their preterm infant’s state-regulation. Int. Breastfeed J. 2022, 17, 44. [Google Scholar] [CrossRef]
- Dennis, C.L. Theoretical underpinnings of breastfeeding confidence: A self-efficacy framework. J. Hum. Lact. 1999, 15, 195–201. [Google Scholar] [CrossRef]
- Anaba, U.C.; Johansson, E.W.; Abegunde, D.; Adoyi, G.; Umar-Farouk, O.; Abdu-Aguye, S.; Hewett, P.C.; Hutchinson, P.L. The role of maternal ideations on breastfeeding practices in northwestern Nigeria: A cross-section study. Int. Breastfeed. J. 2022, 17, 63. [Google Scholar] [CrossRef]
- You, H.; Lei, A.; Xiang, J.; Wang, Y.; Luo, B.; Hu, J. Effects of breastfeeding education based on the self-efficacy theory on women with gestational diabetes mellitus: A CONSORT-compliant randomized controlled trial. Medicine 2020, 99, e19643. [Google Scholar] [CrossRef] [PubMed]
- Vieira, E.S.; Caldeira, N.T.; Eugênio, D.S.; Lucca MM, D.; Silva, I.A. Breastfeeding self-efficacy and postpartum depression: A cohort study. Rev. Lat.-Am. Enferm. 2018, 26, e3035. [Google Scholar] [CrossRef] [PubMed]
- Galipeau, R.; Baillot, A.; Trottier, A.; Lemire, L. Effectiveness of interventions on breastfeeding self-efficacy and perceived insufficient milk supply: A systematic review and meta-analysis. Matern. Child Nutr. 2018, 14, e12607. [Google Scholar] [CrossRef]
- Maleki, A.; Faghihzadeh, E.; Youseflu, S. The Effect of Educational Intervention on Improvement of Breastfeeding Self-Efficacy: A Systematic Review and Meta-Analysis. Obstet. Gynecol. Int. 2021, 2021, 5522229. [Google Scholar] [CrossRef]
- Melo, L.C.O.; Bonelli, M.C.P.; Lima, R.V.A.; Gomes-Sponholz, F.A.; Monteiro, J.C.D.S. Anxiety and its influence on maternal breastfeeding self-efficacy. Rev. Lat.-Am. Enferm. 2021, 29, e3485. [Google Scholar] [CrossRef]
- Li, L.; Wu, Y.; Wang, Q.; Du, Y.; Friesen, D.; Guo, Y.; Dill, S.E.; Medina, A.; Rozelle, S.; Zhou, H. Determinants of breastfeeding self-efficacy among postpartum women in rural China: A cross-sectional study. PLoS ONE 2022, 17, e0266273. [Google Scholar] [CrossRef] [PubMed]
- Piro, S.S.; Ahmed, H.M. Impacts of antenatal nursing interventions on mothers’ breastfeeding self-efficacy: An experimental study. BMC Pregnancy Childbirth 2020, 20, 19. [Google Scholar] [CrossRef]
- Mosher, C.; Sarkar, A.; Hashem, A.A.; Hamadah, R.E.; Alhoulan, A.; AlMakadma, Y.A.; Khan, T.A.; Al-Hamdani, A.K.; Senok, A. Self-reported breast feeding practices and the Baby Friendly Hospital Initiative in Riyadh, Saudi Arabia: Prospective cohort study. BMJ Open 2016, 6, e012890. [Google Scholar] [CrossRef] [PubMed]
- Khresheh, R.M.; Ahmad, N.M. Breastfeeding self efficacy among pregnant women in Saudi Arabia. Saudi Med. J. 2018, 39, 1116–1122. [Google Scholar] [CrossRef]
- Ministry of Municipal and Rural Affairs and United Nations Human Settlements Programme. 2018. Revised on: 5/1/2023. Available online: https://unhabitat.org/sites/default/files/2020/04/cpi_profile_for_najran_2019.pdf (accessed on 20 January 2023).
- Amini, P.; Omani-Samani, R.; Sepidarkish, M.; Almasi-Hashiani, A.; Hosseini, M.; Maroufizadeh, S. The Breastfeeding Self-Efficacy Scale-Short Form (BSES-SF): A validation study in Iranian mothers. BMC Res. Notes 2019, 12, 622. [Google Scholar] [CrossRef] [PubMed]
- Radwan, H.; Fakhry, R.; Boateng, G.O.; Metheny, N.; Bani Issa, W.; Faris, M.E.; Obaid, R.S.; Al Marzooqi, S.; Al Ghazal, H.; Dennis, C.L. Translation and Psychometric Evaluation of the Arabic Version of the Breastfeeding Self-Efficacy Scale-Short Form among Women in the United Arab Emirates. J. Hum. Lact. Off. J. Int. Lact. Consult. Assoc. 2023, 39, 40–50. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Aravindakshan, R.; Sathiyanarayanan, S.; Naidu, N.K.; Santhoshi, K.N.K.S.; Kakkar, R. Validation of Gender Friendly Breastfeeding Knowledge scale among young adults. J. Prev. Med. Hyg. 2022, 62, E892–E903. [Google Scholar] [CrossRef] [PubMed]
- Tamim, H.; Ghandour, L.A.; Shamsedine, L.; Charafeddine, L.; Nasser, F.; Khalil, Y.; Nabulsi, M. Adaptation and Validation of the Arabic Version of the Infant Breastfeeding Knowledge Questionnaire among Lebanese Women. J. Hum. Lact. 2016, 32, 682–688. [Google Scholar] [CrossRef]
- De la Mora, A.; Russell, D.W.; Dungy, C.I.; Losch, M.; Dusdieker, L. The Iowa Infant Feeding Attitude Scale: Analysis of reli-ability and validity. J. Appl. Soc. Psychol. 1999, 29, 2362–2380. [Google Scholar] [CrossRef]
- Charafeddine, L.; Tamim, H.; Soubra, M.; de la Mora, A.; Nabulsi, M. Research and Advocacy Breastfeeding Team. Validation of the Arabic Version of the Iowa Infant Feeding Attitude Scale among Lebanese Women. J. Hum. Lact. 2016, 32, 309–314. [Google Scholar] [CrossRef]
- Almadani, M.; Vydelingum, V.; Lawrence, J. Saudi Mothers’ Expected Intentions and Attitudes Toward Breast-Feeding. Infant Child Adolesc. Nutr. 2010, 2, 187–198. [Google Scholar] [CrossRef]
- Economou, M.; Kolokotroni, O.; Paphiti-Demetriou, I.; Kouta, C.; Lambrinou, E.; Hadjigeorgiou, E.; Hadjiona, V.; Middleton, N. The association of breastfeeding self-efficacy with breastfeeding duration and exclusivity: Longitudinal assessment of the pre-dictive validity of the Greek version of the BSES-SF tool. BMC Pregnancy Childbirth 2021, 21, 421. [Google Scholar] [CrossRef]
- Mercan, Y.; Tari Selcuk, K. Association between postpartum depression level, social support level and breastfeeding attitude and breastfeeding self-efficacy in early postpartum women. PLoS ONE 2021, 16, e0249538. [Google Scholar] [CrossRef]
- Ip, W.Y.; Gao, L.L.; Choi, K.C.; Chau, J.P.; Xiao, Y. The Short Form of the Breastfeeding Self-Efficacy Scale as a Prognostic Factor of Exclusive Breastfeeding among Mandarin-Speaking Chinese Mothers. J. Hum. Lact. Off. J. Int. Lact. Consult. Assoc. 2016, 32, 711–720. [Google Scholar] [CrossRef]
- Alyousefi, N.; Alemam, A.; Altwaijri, D.; Alarifi, S.; Alessa, H. Predictors of Prenatal Breastfeeding Self-Efficacy in Expectant Mothers with Gestational Diabetes Mellitus. Int. J. Environ. Res. Public Health 2022, 19, 4115. [Google Scholar] [CrossRef] [PubMed]
- Colombo, L.; Crippa, B.L.; Consonni, D.; Bettinelli, M.E.; Agosti, V.; Mangino, G.; Bezze, E.N.; Mauri, P.A.; Zanotta, L.; Roggero, P.; et al. Breastfeeding Determinants in Healthy Term Newborns. Nutrients 2018, 10, 48. [Google Scholar] [CrossRef] [PubMed]
- Waits, A.; Guo, C.Y.; Chien, L.Y. Evaluation of factors contributing to the decline in exclusive breastfeeding at 6 months postpartum: The 2011–2016 National Surveys in Taiwan. Birth 2018, 45, 184–192. [Google Scholar] [CrossRef]
- Bandura, A.; Pastorelli, C.; Barbaranelli, C.; Caprara, G.V. Self-efficacy pathways to childhood depression. J. Pers. Soc. Psychol. 1999, 76, 258–269. [Google Scholar] [CrossRef] [PubMed]
- Elgzar, W.T.; Al-Thubaity, D.D.; Alshahrani, M.A.; Essa, R.M.; Ibrahim, H.A. The Relationship between Maternal Ideation and Exclusive Breastfeeding Practice among Saudi Nursing Mothers: A Cross-Sectional Study. Nutrients 2023, 15, 1719. [Google Scholar] [CrossRef]
- Gerhardsson, E.; Nyqvist, K.H.; Mattsson, E.; Volgsten, H.; Hildingsson, I.; Funkquist, E.L. The Swedish Version of the Breastfeeding Self-Efficacy Scale-Short Form: Reliability and Validity Assessment. J. Hum. Lact. Off. J. Int. Lact. Consult. Assoc. 2014, 30, 340–345. [Google Scholar] [CrossRef]
- Tsaras, K.; Sorokina, T.; Papathanasiou, I.V.; Fradelos, E.C.; Papagiannis, D.; Koulierakis, G. Breastfeeding Self-efficacy and Related Socio-demographic, Perinatal and Psychological Factors: A Cross-sectional Study Among Postpartum Greek Women. Mater. Socio-Med. 2021, 33, 206–212. [Google Scholar] [CrossRef]
- Amin, T.; Hablas, H.; Al Qader, A.A. Determinants of initiation and exclusivity of breastfeeding in Al Hassa, Saudi Arabia. Breastfeed. Med. Off. J. Acad. Breastfeed. Med. 2011, 6, 59–68. [Google Scholar] [CrossRef]
- Rocha, I.S.; Lolli, L.F.; Fujimaki, M.; Gasparetto, A.; Rocha NB, D. Influence of maternal confidence on exclusive breastfeeding until six months of age: A systematic review. Influência da autoconfiança materna sobre o aleitamento materno exclusivo aos seis meses de idade: Uma revisão sistemática. Cienc. Saude Coletiva 2018, 23, 3609–3619. [Google Scholar] [CrossRef]
- Monteiro, J.C.D.S.; Guimarães, C.M.S.; Melo, L.C.O.; Bonelli, M.C.P. Breastfeeding self-efficacy in adult women and its relationship with exclusive maternal breastfeeding. Rev. Lat.-Am. Enferm. 2020, 28, e3364. [Google Scholar] [CrossRef]
- Moraes, G.G.W.; Christoffel, M.M.; Toso, B.R.G.O.; Viera, C.S. Association between duration of exclusive breastfeeding and nursing mothers’ self-efficacy for breastfeeding. Rev. Esc. Enferm. USP 2021, 55, e03702. [Google Scholar] [CrossRef] [PubMed]
- Titaley, C.R.; Dibley, M.J.; Ariawan, I.; Mu’asyaroh, A.; Alam, A.; Damayanti, R.; Do, T.T.; Ferguson, E.; Htet, K.; Li, M.; et al. Determinants of low breastfeeding self-efficacy amongst mothers of children aged less than six months: Results from the BADUTA study in East Java, Indonesia. Int. Breastfeed. J. 2021, 16, 12. [Google Scholar] [CrossRef]
- Titaley, C.R.; Loh, P.C.; Prasetyo, S.; Ariawan, I.; Shankar, A.H. Socio-economic factors and use of maternal health services are associated with delayed initiation and non-exclusive breastfeeding in Indonesia: Secondary analysis of Indonesia Demographic and Health Surveys 2002/2003 and 2007. Asia Pac. J. Clin. Nutr. 2014, 23, 91–104. [Google Scholar] [CrossRef] [PubMed]
- AlSedra, H.; AlQurashi, A.A. Exploring the Experience of Breastfeeding Among Working Mothers at Healthcare Facility in Saudi Arabia: A Qualitative Approach. Cureus 2022, 14, e25510. [Google Scholar] [CrossRef]
- Awoke, N.; Tekalign, T.; Lemma, T. Predictors of optimal breastfeeding practices in Worabe town, Silte zone, South Ethiopia. PLoS ONE 2020, 15, e0232316. [Google Scholar] [CrossRef]
- Dodt, R.C.; Joventino, E.S.; Aquino, P.S.; Almeida, P.C.; Ximenes, L.B. An experimental study of an educational intervention to promote maternal self-efficacy in breastfeeding. Rev. Lat.-Am. Enferm. 2015, 23, 725–732. [Google Scholar] [CrossRef]
- Mirghafourvand, M.; Malakouti, J.; Mohammad-Alizadeh-Charandabi, S.; Faridvand, F. Predictors of Breastfeeding Self-efficacy in Iranian Women: A Cross-Sectional Study. Int. J. Womens Health Reprod. Sci. 2018, 6, 380–385. [Google Scholar] [CrossRef]
- Hegazi, M.A.; Allebdi, M.; Almohammadi, M.; Alnafie, A.; Al-Hazmi, L.; Alyoubi, S. Factors associated with exclusive breastfeeding in relation to knowledge, attitude and practice of breastfeeding mothers in Rabigh community, Western Saudi Arabia. World J. Pediatr. WJP 2019, 15, 601–609. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total Sample N = 1577 | Breastfeeding Self-Efficacy | X2/FET | p | ||||
|---|---|---|---|---|---|---|---|---|
| Low n = (520) | High n = (1057) | |||||||
| n | % | n | % | n | % | |||
| Age (years) | ||||||||
| 79 | 5.0 | 34 | 6.5 | 45 | 4.3 | 3.835 | 0.147 |
| 1242 | 78.8 | 404 | 77.7 | 838 | 79.3 | ||
| 256 | 16.2 | 82 | 15.8 | 174 | 16.5 | ||
| Residence | 0.081 | 0.775 | ||||||
| 101 | 6.4 | 32 | 6.2 | 69 | 6.5 | ||
| 1476 | 93.6 | 488 | 93.8 | 988 | 93.5 | ||
| Occupational status | 51.462 | 0.000 ** | ||||||
| 696 | 44.1 | 296 | 56.9 | 400 | 37.8 | ||
| 881 | 55.9 | 224 | 43.1 | 657 | 62.2 | ||
| Education | 542.085 | 0.000 ** | ||||||
| 867 | 55.0 | 198 | 38.1 | 669 | 63.3 | ||
| 375 | 23.8 | 51 | 9.8 | 324 | 30.7 | ||
| 335 | 21.2 | 271 | 52.1 | 64 | 6.1 | ||
| Husband education | 3.267 | 0.195 | ||||||
| 1050 | 66.6 | 353 | 67.9 | 697 | 65.9 | ||
| 487 | 30.9 | 159 | 30.6 | 328 | 31.0 | ||
| 40 | 2.5 | 8 | 1.5 | 32 | 3.0 | ||
| Monthly income | 5.445 | 0.066 | ||||||
| 197 | 12.5 | 65 | 12.5 | 132 | 12.5 | ||
| 810 | 51.4 | 247 | 47.5 | 563 | 53.3 | ||
| 570 | 36.1 | 208 | 40.0 | 362 | 34.2 | ||
| Variables | Total Sample N = 1577 | Breastfeeding Self-Efficacy | X2/FET | p | ||||
|---|---|---|---|---|---|---|---|---|
| Low n = (520) | High n = (1057) | |||||||
| n | % | n | % | n | % | |||
| breastfeeding experience | 15.085 | 0.000 ** | ||||||
| 506 | 32.1 | 133 | 25.6 | 373 | 35.3 | ||
| 1071 | 67.9 | 387 | 74.4 | 684 | 64.7 | ||
| Parity | 64.942 | 0.000 ** | ||||||
| 510 | 32.3 | 228 | 43.8 | 282 | 26.7 | ||
| 1067 | 67.7 | 292 | 56.2 | 775 | 73.3 | ||
| Mode of delivery | 0.804 | 0.370 | ||||||
| 1055 | 66.9 | 340 | 65.4 | 715 | 67.6 | ||
| 522 | 33.1 | 180 | 34.6 | 342 | 32.4 | ||
| Complications during the last delivery | 2.017 | 0.165 | ||||||
| 1266 | 80.3 | 428 | 82.3 | 838 | 79.3 | ||
| 311 | 19.7 | 92 | 17.7 | 219 | 20.7 | ||
| Duration of pregnancy for the last child | 2.469 | 0.116 | ||||||
| 1430 | 90.7 | 463 | 89.0 | 967 | 91.5 | ||
| 147 | 9.3 | 57 | 11.0 | 90 | 8.5 | ||
| Overall knowledge | 124.376 | 0.000 ** | ||||||
| 628 | 39.8 | 309 | 59.4 | 319 | 30.2 | ||
| 949 | 60.2 | 211 | 40.6 | 738 | 69.8 | ||
| Overall attitude | 96.397 | 0.000 ** | ||||||
| 680 | 43.1 | 315 | 60.6 | 365 | 34.5 | ||
| 897 | 56.9 | 205 | 39.4 | 692 | 65.5 | ||
| BSES-SF Items | Mean | SD |
|---|---|---|
| 3.32 | 0.95 |
| 3.37 | 0.90 |
| 3.23 | 0.94 |
| 3.33 | 0.99 |
| 3.30 | 1.05 |
| 3.25 | 0.97 |
| 3.38 | 1.07 |
| 3.41 | 1.06 |
| 3.28 | 1.11 |
| 3.40 | 1.05 |
| 3.31 | 1.09 |
| 3.24 | 1.09 |
| 3.26 | 1.07 |
| 3.24 | 1.11 |
| Overall mean of the BSES-SF score | 51.31 | 10.79 |
| Predictors | High Breastfeeding Self-Efficacy | |
|---|---|---|
| AOR (95% CI) | p | |
| Age (years) | 0.167 | |
| − <20 | Ref | |
| − 20–35 | 0.630 (0.18–2.12) | 0.456 |
| − ≥36 | 0.591 (0.34–1.02) | 0.059 |
| Residence | ||
| − Rural | Ref | |
| − Urban | 0.844 (0.48–1.48) | 0.556 |
| Occupational status | ||
| − Employee | Ref | |
| − Housewife | 1.686 (1.23–2.30) | 0.001 * |
| Education | 0.000 ** | |
| − Read and write | Ref | |
| − Secondary education | 45.140 (27.95–72.88) | 0.000 ** |
| − University education | 69.474 (39.52–122.11) | 0.000 ** |
| Husband education | 0.223 | |
| − Read and write | Ref | |
| − Secondary education | 1.180 (0.32–4.30) | 0.803 |
| − University education | 0.857 (0.24–3.01) | 0.810 |
| Monthly income | 0.055 | |
| − Insufficient | Ref | |
| − Sufficient | 0.965 (0.69–1.33) | 0.830 |
| − Sufficient and save | 1.909 (1.09–3.33) | 0.033 * |
| breastfeeding experience | ||
| - Nonexclusive | Ref | |
| - Exclusive | 5.949 (1.35–26.10) | 0.000 * |
| Parity | ||
| - Primiparous | Ref | |
| - Multiparous | 3.170 (1.96–5.120) | 0.000 ** |
| Mode of delivery | ||
| - Vaginal delivery | Ref | |
| - Cesarean section | 1.090 (0.77–1.532) | 0.622 |
| Complications during the last delivery | ||
| - No | Ref | |
| - Yes | 0.612 (0.34–1.10) | 0.102 |
| Duration of pregnancy for the last child | ||
| - Full-term | ||
| - Preterm | 1.095 (0.28–4.160) | 0.894 |
| Overall knowledge | ||
| - Inadequate (18–54) | Ref | |
| - Adequate (55–90) | 2.769 (1.88–4.064) | 0.000 ** |
| Overall attitude | ||
| - Negative (17–51) | Ref | |
| - Positive (52–85) | 4.803 (2.60–8.85) | 0.000 ** |
| −2 Log likelihood (1263.883) | Cox and Snell R Square (0.374) | Nagelkerke R Square (0.519) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Thubaity, D.D.; Alshahrani, M.A.; Elgzar, W.T.; Ibrahim, H.A. Determinants of High Breastfeeding Self-Efficacy among Nursing Mothers in Najran, Saudi Arabia. Nutrients 2023, 15, 1919. https://doi.org/10.3390/nu15081919
Al-Thubaity DD, Alshahrani MA, Elgzar WT, Ibrahim HA. Determinants of High Breastfeeding Self-Efficacy among Nursing Mothers in Najran, Saudi Arabia. Nutrients. 2023; 15(8):1919. https://doi.org/10.3390/nu15081919
Chicago/Turabian StyleAl-Thubaity, DaifAllah D., Mohammed A. Alshahrani, Wafaa T. Elgzar, and Heba A. Ibrahim. 2023. "Determinants of High Breastfeeding Self-Efficacy among Nursing Mothers in Najran, Saudi Arabia" Nutrients 15, no. 8: 1919. https://doi.org/10.3390/nu15081919
APA StyleAl-Thubaity, D. D., Alshahrani, M. A., Elgzar, W. T., & Ibrahim, H. A. (2023). Determinants of High Breastfeeding Self-Efficacy among Nursing Mothers in Najran, Saudi Arabia. Nutrients, 15(8), 1919. https://doi.org/10.3390/nu15081919