

Feasibility of an Individualized mHealth Nutrition (iNutrition) Intervention for Post-Discharged Gastric Cancer Patients Following Gastrectomy: A Randomized Controlled Pilot Trial
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants and Recruitment
- histologically confirmed gastric adenocarcinoma;
- received D2 radical gastrectomy;
- access to broadband internet;
- patient’s age ≥ 18 years;
- patient agreed to participate in this trial through informed consent.
2.3. Randomization and Blinding
2.4. Common Intervention for Both Groups
2.5. Specific Intervention (iNutrition Intervention)
2.5.1. Intervention Details
- (i)
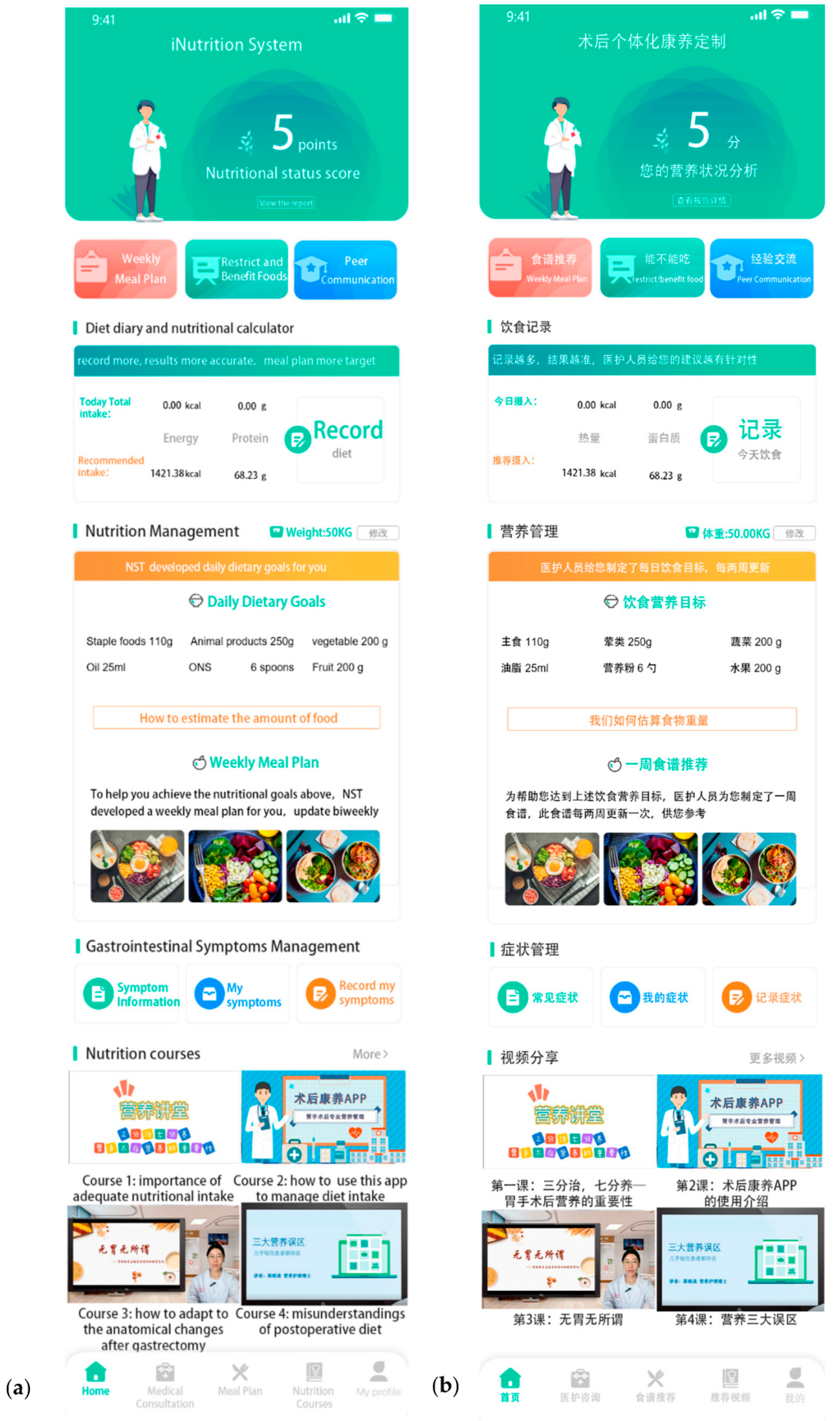
- The iNutrition applet
- a.
- Gastrointestinal symptoms management
- b.
- Nutrition management
- c.
- Nutrition Knowledge
- d.
- Communication center
- (ii)
- Telephone-delivered Nutrition Consultation
2.5.2. Health Action Process Approach Theory
2.6. Outcomes
2.6.1. Quantitative Feasibility Measures
- Recruitment rate: the percentage of the eligible study population who agree to participate.
- Retention rate: the percentage of enrolled participants who completed the post-intervention evaluation.
- Adherence of the intervention participants: (1) number of planned nutrition consultations completed and average duration of the consultations; (2) register rate—participants registered on the iNutrition applet and participants were allocated to the intervention group × 100%; (3) number of logins into iNutrition applet from baseline to post-test; (4) the percentage of days that participants were active on the iNutrition applet during the 12-week intervention period; (5) percentage of registered participants who visited each module of the iNutrition applet. Adherence was recorded through the analytics function of the iNutrition applet, and records of attended nutrition consultations were kept.
- Acceptability of the participants of the intervention arm: this was determined through the System Usability Scale (SUS) and the Net Promoter Score (NPS) findings. The SUS is a valid and reliable 10-item usability measurement scale designed to evaluate software products, such as websites and applets, and was graded on a 5-point Likert scale [28]. The NPS is a validated one-item questionnaire (“How likely would you be to recommend iNutrition applet to a friend?”) on a scale of 1 to 10, with 1 being the least-probable and 10 being the most-probable for recommending this applet to others. Respondents with scores ranging from 0 to 6 are considered detractors, those with 7 or 8 are considered passive, and those with 9 or 10 are considered promoters. To compute the total NPS score, we divided the percentage of detractors by the percentage of promoters, yielding a single number ranging from −100% to +100%. Overall, a total NPS score greater than 0% indicated a stronger inclination to recommend the applet to others [29].
2.6.2. Embedded Qualitative Feasibility Measures
2.6.3. Secondary Outcomes
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics
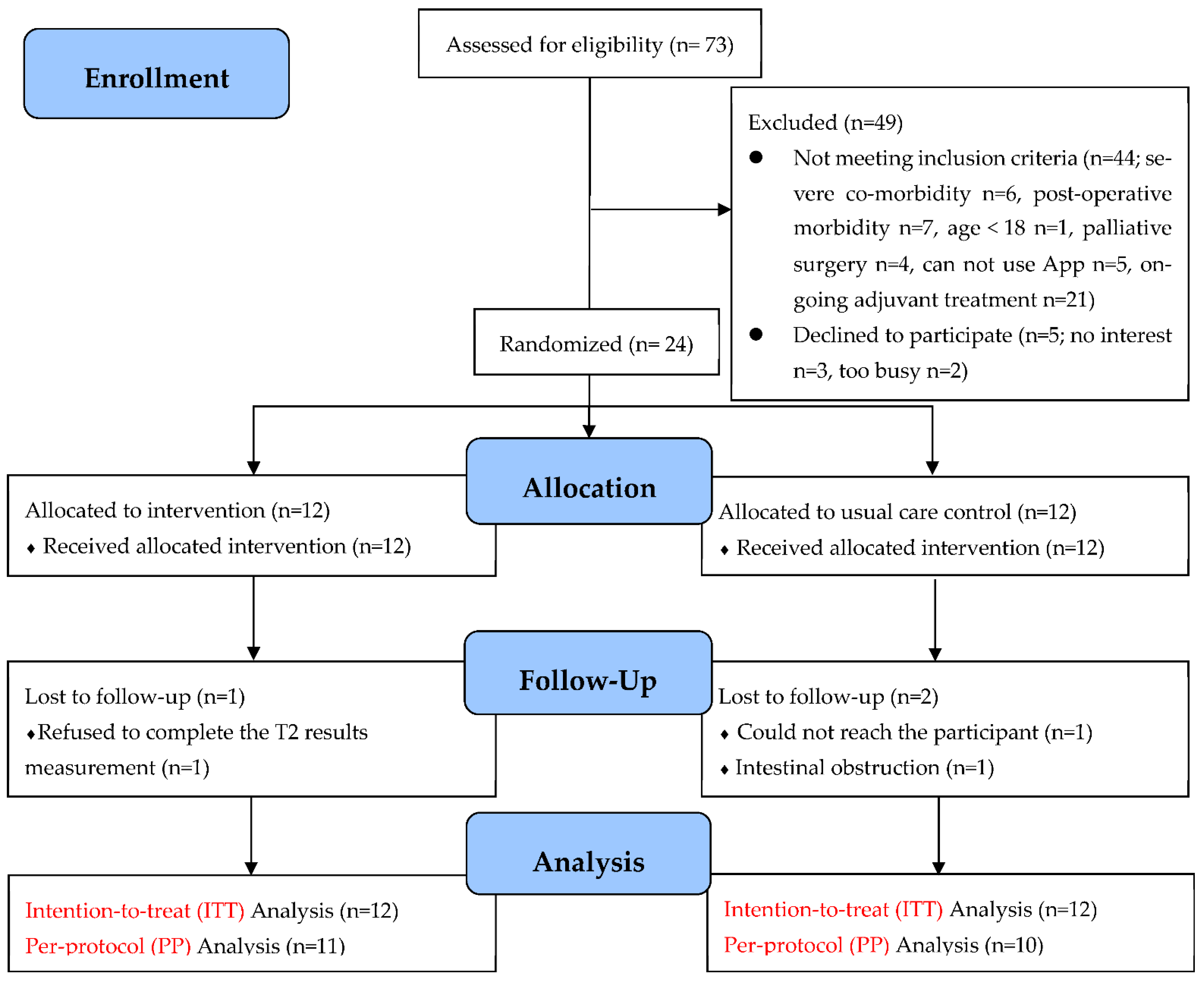
3.2. Recruitment and Retention
3.3. Adherence and Acceptability
3.3.1. Adherence
3.3.2. System Usability Scale
3.3.3. Net Promoter Score
3.4. Qualitative Feasibility Data
3.5. Secondary Measures
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: Globocan Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Sun, W.; Haller, D.G. Recent Advances in the Treatment of Gastric Cancer. Drugs 2001, 61, 1545–1551. [Google Scholar] [CrossRef] [PubMed]
- Taleghani, F.; Ehsani, M.; Farzi, S.; Farzi, S.; Adibi, P.; Moladoost, A.; Shahriari, M.; Tabakhan, M. Nutritional Challenges of Gastric Cancer Patients from the Perspectives of Patients, Family Caregivers, and Health Professionals: A Qualitative Study. Support. Care Cancer 2021, 29, 3943–3950. [Google Scholar] [CrossRef] [PubMed]
- Guo, Z.Q.; Yu, J.M.; Li, W.; Fu, Z.M.; Lin, Y.; Shi, Y.Y.; Hu, W.; Ba, Y.; Li, S.Y.; Li, Z.N.; et al. Survey and Analysis of the Nutritional Status in Hospitalized Patients with Malignant Gastric Tumors and Its Influence on the Quality of Life. Support. Care Cancer 2020, 28, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Reece, L.; Hogan, S.; Allman-Farinelli, M.; Carey, S. Oral Nutrition Interventions in Patients Undergoing Gastrointestinal Surgery for Cancer: A Systematic Literature Review. Support. Care Cancer 2020, 28, 5673–5691. [Google Scholar] [CrossRef]
- Sun, V.; Kim, J.; Kim, J.Y.; Raz, D.J.; Merchant, S.; Chao, J.; Chung, V.; Jimenez, T.; Wittenberg, E.; Grant, M.; et al. Dietary Alterations and Restrictions Following Surgery for Upper Gastrointestinal Cancers: Key Components of a Health-Related Quality of Life Intervention. Eur. J. Oncol. Nurs. 2015, 19, 343–348. [Google Scholar] [CrossRef]
- Weimann, A.; Braga, M.; Carli, F.; Higashiguchi, T.; Hübner, M.; Klek, S.; Laviano, A.; Ljungqvist, O.; Lobo, D.N.; Martindale, R.G.; et al. Espen Practical Guideline: Clinical Nutrition in Surgery. Clin. Nutr. 2021, 40, 4745–4761. [Google Scholar] [CrossRef]
- Muscaritoli, M.; Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. Espen Practical Guideline: Clinical Nutrition in Cancer. Clin. Nutr. 2021, 40, 2898–2913. [Google Scholar] [CrossRef]
- Rinninella, E.; Cintoni, M.; Raoul, P.; Pozzo, C.; Strippoli, A.; Bria, E.; Tortora, G.; Gasbarrini, A.; Mele, M.C. Effects of Nutritional Interventions on Nutritional Status in Patients with Gastric Cancer: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Clin. Nutr. ESPEN 2020, 38, 28–42. [Google Scholar] [CrossRef]
- Li, K.; Wang, D.; Zhang, X.; Yang, J.; Chen, X. Efficacy of Early Enteral Nutrition Versus Total Parenteral Nutrition for Patients with Gastric Cancer Complicated with Diabetes Mellitus: A Systematic Review and Meta-Analysis. Nutr. Diet. 2022, 79, 129–139. [Google Scholar] [CrossRef]
- Wu, J.M.; Yu, H.J.; Ho, T.W.; Su, X.Y.; Lin, M.T.; Lai, F. Tablet Pc-Enabled Application Intervention for Patients with Gastric Cancer Undergoing Gastrectomy. Comput. Methods Programs Biomed. 2015, 119, 101–109. [Google Scholar] [CrossRef]
- Furness, K.; Sarkies, M.N.; Huggins, C.E.; Croagh, D.; Haines, T.P. Impact of the Method of Delivering Electronic Health Behavior Change Interventions in Survivors of Cancer on Engagement, Health Behaviors, and Health Outcomes: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2020, 22, e16112. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Observatory for Mhealth: New Horizons for Health through Mobile Technologies: Second Global Survey on Ehealth; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Lunde, P.; Nilsson, B.B.; Bergland, A.; Kvaerner, K.J.; Bye, A. The Effectiveness of Smartphone Apps for Lifestyle Improvement in Noncommunicable Diseases: Systematic Review and Meta-Analyses. J. Med. Internet Res. 2018, 20, e162. [Google Scholar] [CrossRef]
- DiFilippo, K.N.; Huang, W.H.; Andrade, J.E.; Chapman-Novakofski, K.M. The Use of Mobile Apps to Improve Nutrition Outcomes: A Systematic Literature Review. J. Telemed. Telecare 2015, 21, 243–253. [Google Scholar] [CrossRef] [PubMed]
- Breton, E.R.; Fuemmeler, B.F.; Abroms, L.C. Weight Loss-There Is an App for That! But Does It Adhere to Evidence-Informed Practices? Transl. Behav. Med. 2011, 1, 523–529. [Google Scholar] [CrossRef] [PubMed]
- Lozano-Lozano, M.; Cantarero-Villanueva, I.; Martin-Martin, L.; Galiano-Castillo, N.; Sanchez, M.J.; Fernandez-Lao, C.; Postigo-Martin, P.; Arroyo-Morales, M. A Mobile System to Improve Quality of Life via Energy Balance in Breast Cancer Survivors (Beneca Mhealth): Prospective Test-Retest Quasiexperimental Feasibility Study. JMIR mHealth uHealth 2019, 7, e14136. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Lu, X.L.; Xie, Z.C.; Jiang, T.T.; Song, C.L.; Wang, Z.X. Evaluation of a Novel Wechat Applet for Image-Based Dietary Assessment among Pregnant Women in China. Nutrients 2021, 13, 3158. [Google Scholar] [CrossRef]
- Xu, Z.D.; Geng, J.; Zhang, S.; Zhang, K.X.; Yang, L.; Li, J.; Li, J. A Mobile-Based Intervention for Dietary Behavior and Physical Activity Change in Individuals at High Risk for Type 2 Diabetes Mellitus: Randomized Controlled Trial. JMIR mHealth uHealth 2020, 8, e19869. [Google Scholar] [CrossRef]
- Moore, G.F.; Audrey, S.; Barker, M.; Bond, L.; Bonell, C.; Hardeman, W.; Moore, L.; O’Cathain, A.; Tinati, T.; Wight, D.; et al. Process Evaluation of Complex Interventions: Medical Research Council Guidance. BMJ 2015, 350, h1258. [Google Scholar] [CrossRef]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A. Consort 2010 Statement: Extension to Randomised Pilot and Feasibility Trials. BMJ 2016, 355, i5239. [Google Scholar] [CrossRef]
- Julious, S.A. Sample Size of 12 per Group Rule of Thumb for a Pilot Study. Pharm. Stat. J. Appl. Stat. Pharm. Ind. 2005, 4, 287–291. [Google Scholar] [CrossRef]
- Brennan, L.; Sadeghi, F.; O’Neill, L.; Guinan, E.; Smyth, L.; Sheill, G.; Smyth, E.; Doyle, S.L.; Timon, C.M.; Connolly, D.; et al. Telehealth Delivery of a Multi-Disciplinary Rehabilitation Programme for Upper Gastro-Intestinal Cancer: Restore@Home Feasibility Study. Cancers 2022, 14, 2707. [Google Scholar] [CrossRef] [PubMed]
- Martin-Alemany, G.; Perez-Navarro, M.; Wilund, K.R.; Garcia-Villalobos, G.; Gomez-Guerrero, I.; Cantu-Quintanilla, G.; Reyes-Caldelas, M.A.; Espinosa-Cuevas, A.; Escobedo, G.; Medeiros, M.; et al. Effect of Intradialytic Oral Nutritional Supplementation with or without Exercise Improves Muscle Mass Quality and Physical Function in Hemodialysis Patients: A Pilot Study. Nutrients 2022, 14, 2946. [Google Scholar] [CrossRef]
- Ding, Y.; Yang, Y.; Li, F.; Shao, Y.; Sun, Z.; Zhong, C.; Fan, P.; Li, Z.; Zhang, M.; Li, X.; et al. Development and Validation of a Photographic Atlas of Food Portions for Accurate Quantification of Dietary Intakes in China. J. Hum. Nutr. Diet. 2021, 34, 604–615. [Google Scholar] [CrossRef]
- National Institute for Nutrition; Health Care Center. China Food Composition Tables, 6th ed; Peking University Medical Press: Beijing, China, 2018. [Google Scholar]
- Schwarzer, R. Modeling Health Behavior Change: How to Predict and Modify the Adoption and Maintenance of Health Behaviors. Appl. Psychol. 2008, 57, 1–29. [Google Scholar] [CrossRef]
- Bangor, A.; Kortum, P.T.; Miller, J.T. An Empirical Evaluation of the System Usability Scale. Int. J. Hum.-Comput. Interact. 2008, 24, 574–594. [Google Scholar] [CrossRef]
- Hamilton, D.F.; Lane, J.V.; Gaston, P.; Patton, J.T.; MacDonald, D.J.; Simpson, A.; Howie, C.R. Assessing Treatment Outcomes Using a Single Question the Net Promoter Score. Bone Jt. J. 2014, 96, 622–628. [Google Scholar] [CrossRef]
- Bauer, J.; Capra, S.; Ferguson, M. Use of the Scored Patient-Generated Subjective Global Assessment (Pg-Sga) as a Nutrition Assessment Tool in Patients with Cancer. Eur. J. Clin. Nutr. 2002, 56, 779–785. [Google Scholar] [CrossRef]
- Kondrup, J.; Allison, S.P.; Elia, M.; Vellas, B.; Plauth, M. Espen Guidelines for Nutrition Screening 2002. Clin. Nutr. 2003, 22, 415–421. [Google Scholar] [CrossRef]
- Renner, B.; Schwarzer, R. Risk and Health Behaviors: Documentation of the Scales of the Research Project “Risk Appraisal Consequences in Korea”(Rack); International University Bremen & Freie Universität Berlin: Berlin, Germany, 2005; pp. 1–55. [Google Scholar]
- Zhao, A.; Wang, M.C.; Szeto, I.M.Y.; Meng, L.P.; Wang, Y.; Li, T.; Zhang, Y.M. Gastrointestinal Discomforts and Dietary Intake in Chinese Urban Elders: A Cross-Sectional Study in Eight Cities of China. World J. Gastroenterol. 2019, 25, 6681–6692. [Google Scholar] [CrossRef]
- Aaronson, N.K.; Ahmedzai, S.; Bergman, B.; Bullinger, M.; Cull, A.; Duez, N.J.; Filiberti, A.; Flechtner, H.; Fleishman, S.B.; de Haes, J.C.; et al. The European Organization for Research and Treatment of Cancer Qlq-C30: A Quality-of-Life Instrument for Use in International Clinical Trials in Oncology. J. Natl. Cancer Inst. 1993, 85, 365–376. [Google Scholar] [CrossRef] [PubMed]
- Field, J.K.; Duffy, S.W.; Baldwin, D.R.; Brain, K.E.; Devaraj, A.; Eisen, T.; Green, B.A.; Holemans, J.A.; Kavanagh, T.; Kerr, K.M.; et al. The Uk Lung Cancer Screening Trial: A Pilot Randomised Controlled Trial of Low-Dose Computed Tomography Screening for the Early Detection of Lung Cancer. Health Technol. Assess. 2016, 20, 1. [Google Scholar] [CrossRef] [PubMed]
- Woolf, B.; Edwards, P. Does Advance Contact with Research Participants Increase Response to Questionnaires: An Updated Systematic Review and Meta-Analysis. BMC Med. Res. Methodol. 2021, 21, 265. [Google Scholar] [CrossRef] [PubMed]
- Gan, T.; Cheng, H.L.; Tse, M.M.Y. Feasibility, Acceptability, and Effects of Behavior Change Interventions for Improving Multiple Dietary Behaviors among Cancer Survivors: A Systematic Review. Support. Care Cancer 2022, 30, 2877–2889. [Google Scholar] [CrossRef] [PubMed]
- Mohamad, H.; Ntessalen, M.; Craig, L.C.A.; Clark, J.; Fielding, S.; N’dow, J.; Heys, S.D.; McNeill, G. A Self-Help Diet and Physical Activity Intervention with Dietetic Support for Weight Management in Men Treated for Prostate Cancer: Pilot Study of the Prostate Cancer Weight Management (Pro-Man) Randomised Controlled Trial. Br. J. Nutr. 2019, 122, 592–600. [Google Scholar] [CrossRef]
- O’Grady, H.K.; Farley, C.; Takaoka, A.; Mayens, E.; Bosch, J.; Turkstra, L.; Kho, M.E. Retention in Rcts of Physical Rehabilitation for Adults with Frailty: A Systematic Review and Meta-Analysis. Trials 2022, 23, 235. [Google Scholar] [CrossRef]
- Teague, S.; Youssef, G.J.; Macdonald, J.A.; Sciberras, E.; Shatte, A.; Fuller-Tyszkiewicz, M.; Greenwood, C.; McIntosh, J.; Olsson, C.A.; Hutchinson, D. Retention Strategies in Longitudinal Cohort Studies: A Systematic Review and Meta-Analysis. BMC Med. Res. Methodol. 2018, 18, 151. [Google Scholar] [CrossRef]
- Short, C.E.; DeSmet, A.; Woods, C.; Williams, S.L.; Maher, C.; Middelweerd, A.; Muller, A.M.; Wark, P.A.; Vandelanotte, C.; Poppe, L.; et al. Measuring Engagement in Ehealth and Mhealth Behavior Change Interventions: Viewpoint of Methodologies. J. Med. Internet Res. 2018, 20, e292. [Google Scholar] [CrossRef]
- Nedungadi, P.; Jayakumar, A.; Raman, R. Personalized Health Monitoring System for Managing Well-Being in Rural Areas. J. Med. Syst. 2018, 42, 1–11. [Google Scholar] [CrossRef]
- Huggins, C.E.; Hanna, L.; Furness, K.; Silvers, M.A.; Savva, J.; Frawley, H.; Croagh, D.; Cashin, P.; Low, L.; Bauer, J.; et al. Effect of Early and Intensive Telephone or Electronic Nutrition Counselling Delivered to People with Upper Gastrointestinal Cancer on Quality of Life: A Three-Arm Randomised Controlled Trial. Nutrients 2022, 14, 3234. [Google Scholar] [CrossRef]
- Carey, S.; Ferrie, S.; Ryan, R.; Beaton, J.; Young, J.; Allman-Farinelli, M. Long-Term Nutrition Intervention following Major Upper Gastrointestinal Surgery: A Prospective Randomized Controlled Trial. Eur. J. Clin. Nutr. 2013, 67, 324–329. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Intervention (n = 12) | Control (n = 12) | p-Value |
|---|---|---|---|
| Gender, n (%) | 1.00 b | ||
| Male | 8 (66.7%) | 8 (66.7%) | |
| Female | 4 (33.3%) | 4 (33.3%) | |
| Age (years), mean (SD) | 54.08 (10.54) | 55.67 (9.98) | 0.78 a |
| Education (years) | 14.17 ± 2.76 | 12.42 ± 3.73 | 0.76 c |
| Work situation, n (%) | 1.00 b | ||
| Employed | 6 (50%) | 5 (41.7%) | |
| Unemployed | 2 (16.7%) | 3 (25%) | |
| Retired | 4 (33.3%) | 4 (33.3%) | |
| Chronic illnesses, n (%) | 1.00 b | ||
| 0 | 3 (25%) | 2 (16.7%) | |
| 1–2 | 5 (41.7%) | 6 (50%) | |
| 3 or above | 4 (33.3%) | 4 (33.3%) | |
| Tumor location | 0.86 b | ||
| Proximal | 2 (16.7%) | 2 (16.7%) | |
| Middle | 3 (25%) | 5 (41.7%) | |
| Distal | 7 (58.3%) | 5 (41.7%) | |
| Pathological stage | 0.15 b | ||
| I | 2 (16.7%) | 3 (25%) | |
| II | 7 (58.3%) | 2 (16.7%) | |
| III | 2 (16.7%) | 6 (50%) | |
| IV | 1 (8.3%) | 1 (8.3%) | |
| Resection extended | 1.00 b | ||
| Partial gastrectomy | 9 (75%) | 9 (75%) | |
| Total gastrectomy | 3 (25%) | 3 (25%) | |
| Whether received Neoadjuvant treatment before the surgery | 1.00 b | ||
| Yes | 4 (33.3%) | 4 (33.3%) | |
| No | 8 (66.7%) | 8 (66.7%) | |
| Baseline secondary outcomes (mean, SD) | |||
| PG-SGA | 6.67 (2.23) | 7.58 (2.02) | 0.30 a |
| NRS2002 | 4.92 (0.67) | 4.83 (0.39) | 0.59 c |
| Weight | 60.52 (10.52) | 65.02 (9.85) | 0.29 a |
| BMI | 22.37 (3.43) | 24.72 (2.93) | 0.09 a |
| Energy intake | 225.07 (150.44) | 249.01 (100.34) | 0.20 c |
| Protein intake | 7.28 (7.96) | 7.90 (5.38) | 0.35 c |
| Compliance with energy requirements | 0.15 (0.10) | 0.15 (0.06) | 0.44 c |
| Compliance with protein requirement | 0.10 (0.11) | 0.10 (0.07) | 0.59 c |
| HAPA Scale | 3.73 (0.42) | 3.51 (0.29) | 0.14 a |
| GSRS | 6.58 (3.58) | 7.25 (3.47) | 0.65 a |
| QLQ-C30 | 78.60 (14.45) | 72.35 (12.29) | 0.27 a |
| Program Component | |
|---|---|
| Telephone-delivered nutrition consultation | |
| Attendance rate of nutrition consultation (mean ± SD) | 88.89% ± 12.98% |
| Average duration of the nutrition consultations | 23.60 ± 8.94 min |
| iNutrition applet | |
| Register rate (until T2), n (%) | 100 (100%) |
| Usage at T1, yes, n (%) | 11 (91.7%) |
| Usage at T2, yes, n (%) | 7 (58.33%) |
| Logins into the applet (T0-T2), Mdn (IQR) | 89 (98.25) |
| The number of days active on the applet, Mdn (IQR) | 56.5 (20) |
| Percentage of days active on the applet (T0-T2), Mean (SD) | 64.88% ± 28.04% |
| Visits per module, n (%) | |
| Module 1: Nutrition management | 12 (100%) |
| Module 2: Gastrointestinal symptoms management | 9 (75%) |
| Module 3: Nutrition Knowledge | 10 (83.33%) |
| Module 4: Communication center | 10 (83.33%) |
| Items | Mean Score (SD), Max = 5 |
|---|---|
| 1. I think that I would like to use this system frequently | 4.36 ± 0.67 |
| 2. I found the system unnecessarily complex | 2.27 ± 0.65 |
| 3. I thought the system was easy to use | 4.36 ± 0.51 |
| 4. I think that I would need the support of a technical person to be able to use this system | 2.09 ± 1.14 |
| 5. I found the various functions in this system were well integrated | 3.82 ± 0.75 |
| 6. I thought there was too much inconsistency in this system | 1.91 ± 0.75 |
| 7. I would imagine that most people would learn to use this system very quickly | 4 ± 0.63 |
| 8. I found the system very cumbersome to use | 1.73 ± 0.65 |
| 9. I felt very confident using the system | 4.27 ± 0.47 |
| 10. I needed to learn a lot of things before I could get going with this system. | 1.91 ± 0.70 |
| Measures | Intervention Group (n = 12) | Control Group (n = 12) | Group-by-Time Interaction Effects | Effect Size T0-T1 T1-T2 | |||
|---|---|---|---|---|---|---|---|
| Mean (SE) | Mean (SE) | Wald χ2 | β (95% CI) | p | d | ||
| PG-SGA | T0 | 6.67 (0.62) | 7.58 (0.56) | 0.99 | |||
| T1 | 7.83 (0.73) | 9.08 (0.79) | (p = 0.609) | −0.33 (−3.06, 2.39) | 0.811 | 0.10 | |
| T2 | 5.50 (0.85) | 7.50 (0.86) | −1.08 (−3.50, 1.33) | 0.379 | 0.38 | ||
| NRS2002 | T0 | 4.92 (0.19) | 4.83 (0.11) | 2.39 | |||
| T1 | 3.33 (0.30) | 3.50 (0.28) | (p = 0.303) | −0.25 (−1.17, 0.67) | 0.593 | 0.23 | |
| T2 | 2.75 (0.32) | 3.33 (0.25) | −0.67 (−1.60, 0.27) | 0.162 | 0.60 | ||
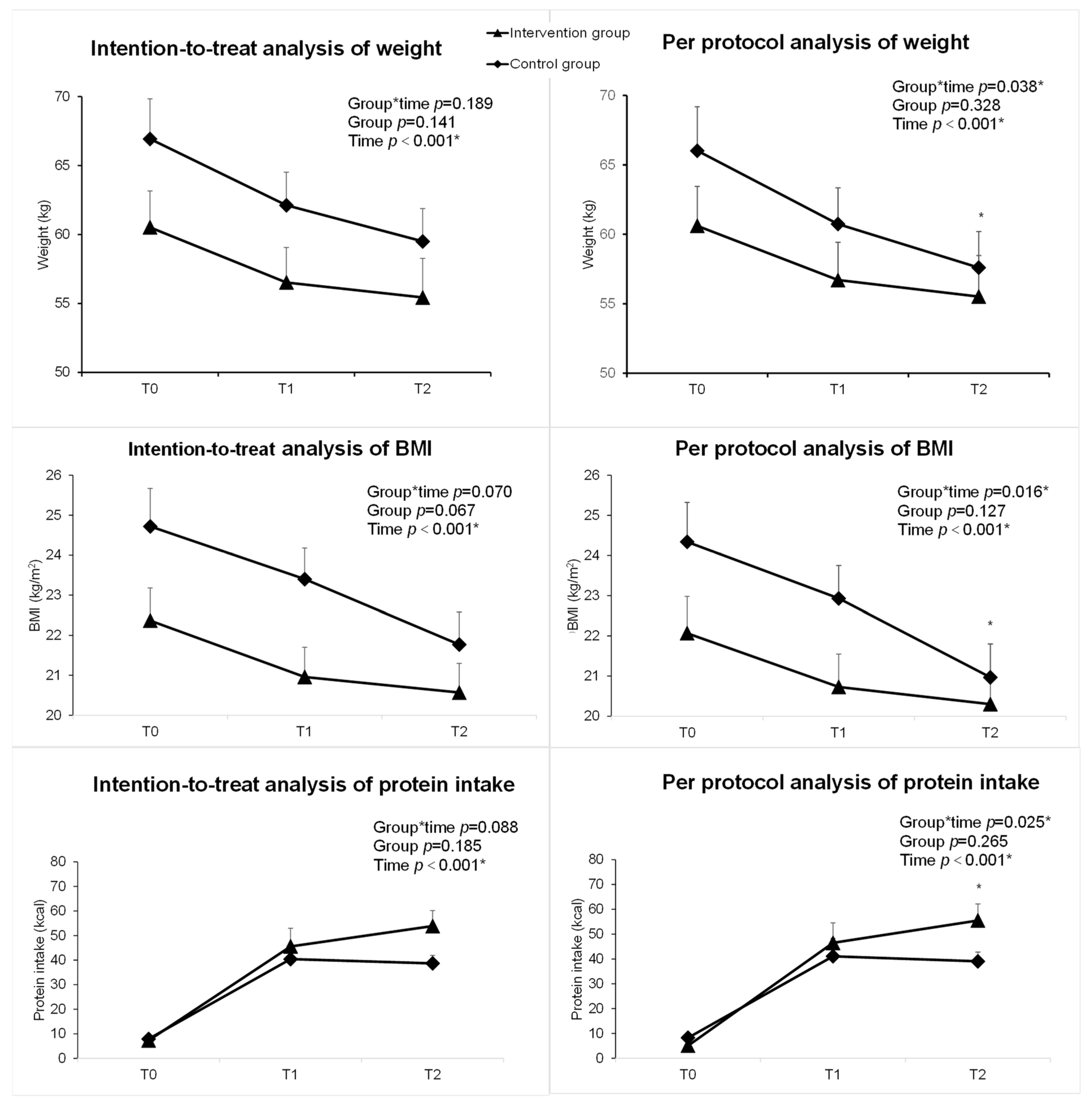
| Weight | T0 | 60.52 (2.91) | 66.93 (2.64) | 3.33 | |||
| T1 | 56.52 (2.40) | 62.12 (2.53) | (p = 0.189) | 0.82 (−1.48, 3.11) | 0.485 | 0.07 | |
| T2 | 55.43 (2.38) | 59.50 (2.84) | 2.34 (−0.40, 5.08) | 0.094 | 0.78 | ||
| BMI | T0 | 22.37 (0.95) | 24.72 (0.81) | 5.31 | |||
| T1 | 20.96 (0.78) | 23.40 (0.74) | (p = 0.070) | −0.09 (−1.18, 0.99) | 0.868 | 0.07 | |
| T2 | 20.57 (0.81) | 21.77 (0.73) | 1.15 (−0.07, 2.38) | 0.066 | 0.78 | ||
| Energy intake | T0 | 225.07 (41.58) | 249.01 (27.73) | 6.54 | |||
| T1 | 991.52 (115.78) | 770.00 (58.22) | (p = 0.038 *) | 245.47 (−18.18, 509.11) | 0.068 | 0.78 | |
| T2 | 1072.52 (86.94) | 811.72 (56.64) | 284.74 (65.31, 504.17) | 0.011 * | 1.08 | ||
| Protein intake | T0 | 7.28 (2.20) | 7.90 (1.49) | 4.85 | |||
| T1 | 45.55 (7.41) | 40.40 (6.02) | (p = 0.088) | 5.76 (−13.95, 25.47) | 0.567 | 0.24 | |
| T2 | 53.83 (6.33) | 38.68 (3.20) | 15.77 (0.26, 31.27) | 0.046 * | 0.85 | ||
| Compliance with energy requirement | T0 | 0.15 (0.03) | 0.15 (0.02) | 10.28 | |||
| T1 | 0.67 (0.07) | 0.51 (0.04) | (p = 0.006 *) | 0.17 (0.00, 0.33) | 0.046 * | 0.85 | |
| T2 | 0.73 (0.05) | 0.53 (0.03) | 0.20 (0.08, 0.33) | 0.001 * | 1.27 | ||
| Compliance with protein requirement | T0 | 0.10 (0.03) | 0.10 (0.02) | 9.57 | |||
| T1 | 0.63 (0.09) | 0.56 (0.09) | (p = 0.008 *) | 0.08 (−0.18, 0.34) | 0.563 | 0.25 | |
| T2 | 0.82 (0.08) | 0.52 (0.04) | 0.30 (0.09, 0.50) | 0.004 * | 1.19 | ||
| HAPA | T0 | 3.73 (0.11) | 3.50 (0.08) | 10.52 | |||
| T1 | 3.92 (0.08) | 3.03 (0.12) | (p = 0.005 *) | 0.67 (0.26, 1.07) | 0.001 * | 1.39 | |
| T2 | 3.94 (0.12) | 3.08 (0.13) | 0.64 (0.17, 1.12) | 0.008 * | 1.12 | ||
| GSRS | T0 | 6.58 (0.99) | 7.25 (0.96) | 1.02 | |||
| T1 | 6.33 (1.46) | 9.17 (1.30) | (p = 0.601) | −2.17 (−6.74, 2.41) | 0.353 | 0.40 | |
| T2 | 6.50 (1.41) | 8.92 (1.41) | −1.75 (−5.68, 2.18) | 0.382 | 0.37 | ||
| QoL | T0 | 78.60 (3.99) | 72.35 (3.40) | 0.73 | |||
| T1 | 77.08 (3.77) | 66.86 (3.46) | (p = 0.695) | 3.97 (−6.29, 14.23) | 0.448 | 0.32 | |
| T2 | 75.61 (3.45) | 68.48 (3.09) | 0.89 (−8.12, 9.90) | 0.847 | 0.08 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, X.; Chen, J.; Yuan, X.; Lin, Y.; Chen, Y.; Li, S.; Jiang, Q.; Yu, H.; Du, Q.; Peng, J. Feasibility of an Individualized mHealth Nutrition (iNutrition) Intervention for Post-Discharged Gastric Cancer Patients Following Gastrectomy: A Randomized Controlled Pilot Trial. Nutrients 2023, 15, 1883. https://doi.org/10.3390/nu15081883
Jiang X, Chen J, Yuan X, Lin Y, Chen Y, Li S, Jiang Q, Yu H, Du Q, Peng J. Feasibility of an Individualized mHealth Nutrition (iNutrition) Intervention for Post-Discharged Gastric Cancer Patients Following Gastrectomy: A Randomized Controlled Pilot Trial. Nutrients. 2023; 15(8):1883. https://doi.org/10.3390/nu15081883
Chicago/Turabian StyleJiang, Xiaohan, Jiamin Chen, Xiuhong Yuan, Yijia Lin, Yingliang Chen, Sijia Li, Qiuxiang Jiang, Hong Yu, Qianqian Du, and Junsheng Peng. 2023. "Feasibility of an Individualized mHealth Nutrition (iNutrition) Intervention for Post-Discharged Gastric Cancer Patients Following Gastrectomy: A Randomized Controlled Pilot Trial" Nutrients 15, no. 8: 1883. https://doi.org/10.3390/nu15081883
APA StyleJiang, X., Chen, J., Yuan, X., Lin, Y., Chen, Y., Li, S., Jiang, Q., Yu, H., Du, Q., & Peng, J. (2023). Feasibility of an Individualized mHealth Nutrition (iNutrition) Intervention for Post-Discharged Gastric Cancer Patients Following Gastrectomy: A Randomized Controlled Pilot Trial. Nutrients, 15(8), 1883. https://doi.org/10.3390/nu15081883