

Vitamin D in Depression: A Potential Bioactive Agent to Reduce Suicide and Suicide Attempt Risk

 , ,
, ,  , ,
, ,
Abstract
1. Introduction
2. Material and Methods
3. Vitamin D
3.1. Vitamin D Sources and References Levels
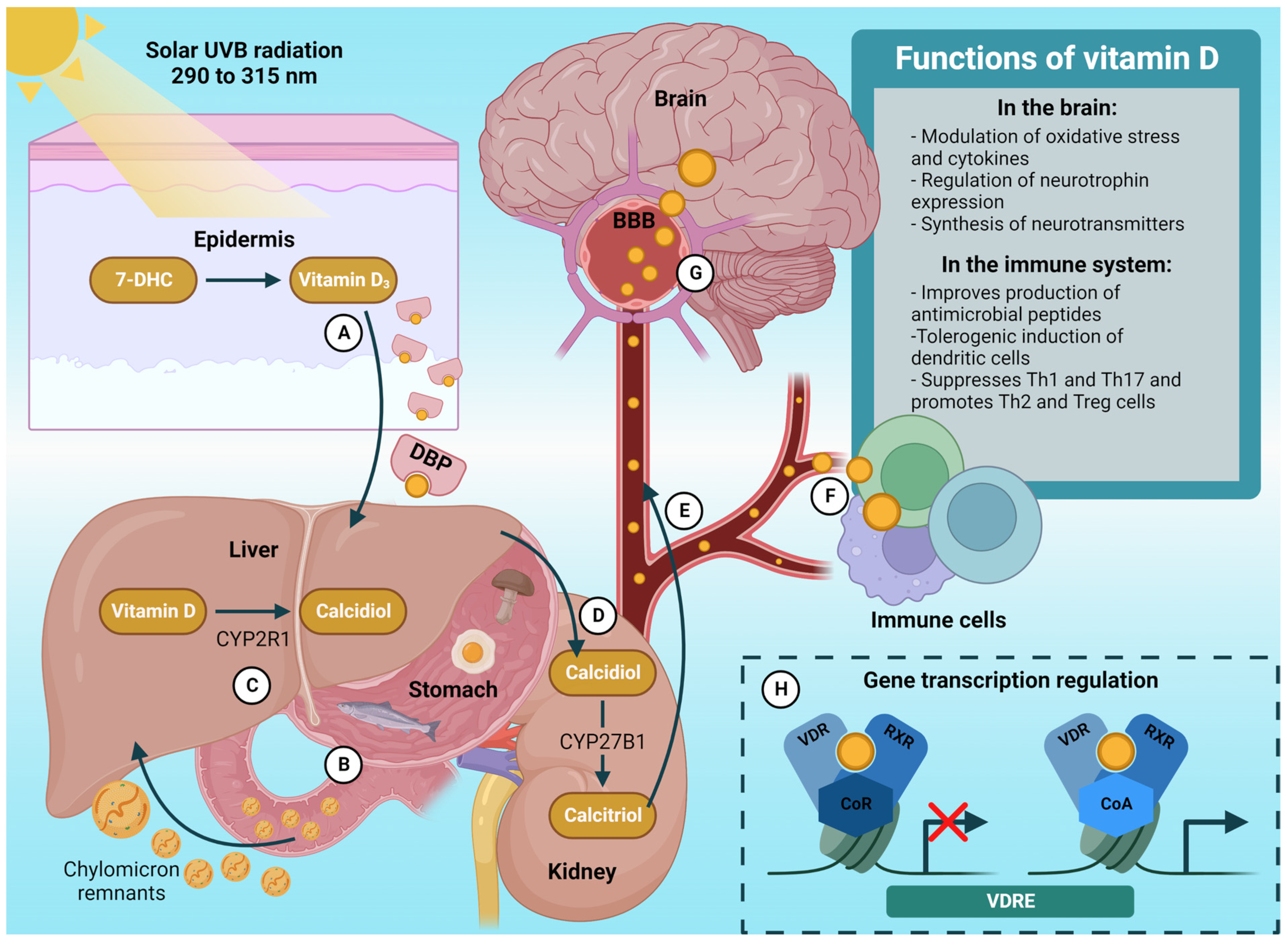
3.2. Vitamin D Metabolism
3.3. Vitamin D Is a Bioactive Agent in the Brain
4. Depression: A Significant Risk Factor for Suicide and Suicide Attempt
4.1. Neurological Mechanisms Associated with Depression and Suicide
4.2. Inflammatory Mechanisms Associated with Depression and Suicide
5. Vitamin D, Depression, and Suicide: Interrelated Evidence and Mechanisms
5.1. Sun and Depression
5.2. Vitamin D Levels, Depression, and Suicide

{kind=link}
{kind=link}
| Author, Year | Country; N; Age | Objective(s) | Vitamin D Measure | Depression Measure | Suicidal Behavior | Additional Outcomes | Results/Conclusion |
|---|---|---|---|---|---|---|---|
| Grudet et al., 2014 [90] | Sweden; 59 suicide attempters (25 men and 34 women): non-suicidal depressed patients (n = 17) and healthy controls (n = 14); 18–73 years old | Asses the association between suicide attempt, vitamin D, and inflammatory changes | Calcidiol was measured in plasma using liquid chromatography–mass spectrometry (LC–MS) | Diagnosis according to the Diagnostic and Statistical Manual of Mental Disorders IV (DSM-IV) as schizoaffective disorder (n = 2), Psychotic Disorder (n = 1), Major Depressive Disorder (n = 10), Bipolar I Disorder (n = 3), Bipolar II Disorder (n = 12), Anxiety disorder (n = 4), Generalized Anxiety Disorder (n = 1), Dysthymic Disorder (n = 4), Alcohol Dependence (n = 6), Substance Dependence (n = 2), Adjustment Disorder (n = 7), Adjustment Disorder with Depressed Mood (n = 3), and Depressive Disorder | Suicide attempt | Vitamin D’s association with plasma IL-1β, IL-6, and TNF-α | In comparison to depressed non-suicidal patients and healthy controls, patients with suicide attempts had significantly lower mean vitamin D levels. Clinically, 58% of the suicide attempters had vitamin D deficiency. Increased levels of IL-6 and IL-1β in the blood were associated with low vitamin D. A deficiency in vitamin D was found in suicide attempters. The results suggest this deficiency might contribute to higher proinflammatory cytokines previously found in suicidal individuals. |
| Il Park et al., 2016 [92] | Republic of Korea; 15,695 subjects; 20 years and older | Explore the relationship among depressive symptoms, suicidal ideation, and vitamin D in a representative sample of the general population | Serum calcidiol levels were measured by radioimmunoassay (DiaSorin, Stillwater, MN, USA) using a gamma counter (1470 Wizard; Perkin Elmer) | Depressive symptoms (“yes” vs. “no”) were evaluated by asking, “Have you felt so sad or hopeless for at least two consecutive weeks during the past year that you had difficulty performing your usual activities?” | Self-reported information about suicidal ideation (‘‘yes’’ vs. ‘‘no’’) was evaluated by asking, “Did you ever feel like committing. suicide during the past year?” | Sociodemographic and health-related factors | No significant differences in serum 25-hydroxyvitamin D concentrations were found among depressive symptoms and suicidal ideation. Vitamin D, depressive symptoms, and suicidal ideation were not significantly associated. Further studies could help elucidate further the association or lack of association between vitamin D, depressive symptoms, and suicidal ideation. |
| Grudet et al., 2020 [24] | USA; 48 un-medicated major depressive disorder (MDD) subjects and 54 healthy controls; 39.3 ± 14.9 years old | Asses the association between suicide ideation, vitamin D, and inflammatory markers in patients with MDD | Analyses of calcidiol were conducted by liquid chromatography–mass spectrometry, model Sciex API 4000 LC/MS/MS | The Structured Clinical Interview for DSM-IV-TR Axis I Disorders (SCID); clinical interview with a board-certified psychiatrist. Depression severity: 17-item version of the Hamilton Depression Rating Scale (HDRS). | MDD subjects were categorized as “non-Suicidal Ideation group” or “Suicidal Ideation group” based on their HDRS suicidality item score. Subjects indicating a suicide attempt or current suicidal intent within the past week were excluded from the study. | Inflammatory markers IL-6 and TNF-α, neutrophil-to-lymphocyte ratio (NLR), and white blood cell count (WBC) | Patients with MDD with and without suicidal ideation (SI) did not display significant differences in calcidiol levels when compared between them and controls. All the measured inflammatory markers were negatively correlated with calcidiol; these correlations were more significant in MDD subjects, especially in the SI group. Even though calcidiol levels did not discriminate MDD with or without SI or vs. controls, indicators of immune activation in MDD were associated with lower calcidiol, particularly in cases with SI. |
| Grudet et al., 2022 [18] | Sweden; 202 patients and 41 healthy Controls; 18–77 years old | (a) Compare calcidiol levels between clinically depressed individuals with insufficient treatment response and healthy controls; (b) assess the association between different affective disorder diagnoses, grade of suicidal ideation, and calcidiol levels | Analyses of calcidiol were conducted by liquid chromatography–mass spectrometry, model Sciex API 4000 (LC/MS/MS) | Diagnosis made according to the DSM-IV-TR; International Neuropsychiatric Interview (MINI) 6.0; SCID-II. Current psychiatric symptoms were assessed using the Comprehensive Psychopathological Rating Scale (CPRS), and the Montgomery-Åsberg Depression Rating Scale (MADRS) was extracted. Patients were divided into four groups based on their diagnosis: major depressive disorder (MDD) single episode (n = 17), MDD recurrent episode (n = 101), chronic MDD (n = 59), or dysthymia (n = 18). | Suicidal ideation (SI) was assessed by the Suicide Assessment Scale (SUAS-S). Subjects are divided into high-grade suicidal ideation and low-grade suicidal ideation. | Patients with depression that had not remitted with previous and ongoing treatments at the moment of the study had significantly lower levels of calcidiol than healthy controls. Only 5% of the controls were calcidiol deficient (<50 nmol/L), while 30% of the depressed patients were. The odds of being depressed decreased 17% per 10 nmol/L increase of calcidiol, which is significant. Symptom severity in dysthymic patients correlated with calcidiol but not in other groups. No significant differences were found in mean calcidiol levels between the four affective disorder diagnoses groups. | |
| Calderon-Espinoza et al., 2022 [91] | Mexico; 72 patients were classified into three groups according to their vitamin D levels; 50.6 ± 12.76 years old | Determine the frequency of depression, anxiety symptoms, and suicidal risk or ideation, and associate it with vitamin D serum levels in patients with rheumatoid arthritis | Vitamin D quantification was determined using the chemiluminescence immunoassay technique (Liaison 25-OH Vitamin D Total Assay, Stillwater, MN) | Hospital Anxiety and Depression Scale (HADS) | Spanish adaptation of the self-applied Plutchik scale | Simplified Disease Activity Index (SDAI), Clinical Disease Activity Index (CDAI), Rheumatoid Arthritis Quality-of-Life Questionnaire, e-Health Assessment Questionnaire–Disability Index (HAQ–DI) | The Plutchik score and suicidal risk were inversely correlated with inadequate vitamin D levels but not with the Hospital Anxiety and Depression Scale. Higher scores on the Rheumatoid Arthritis Quality-of-Life Questionnaire were associated with suicidal ideation. Inadequate vitamin D serum levels correlated with a Plutchik low correlation coefficient. Regarding the covariance analysis, vitamin D levels persist associated with decreasing suicide ideation. |
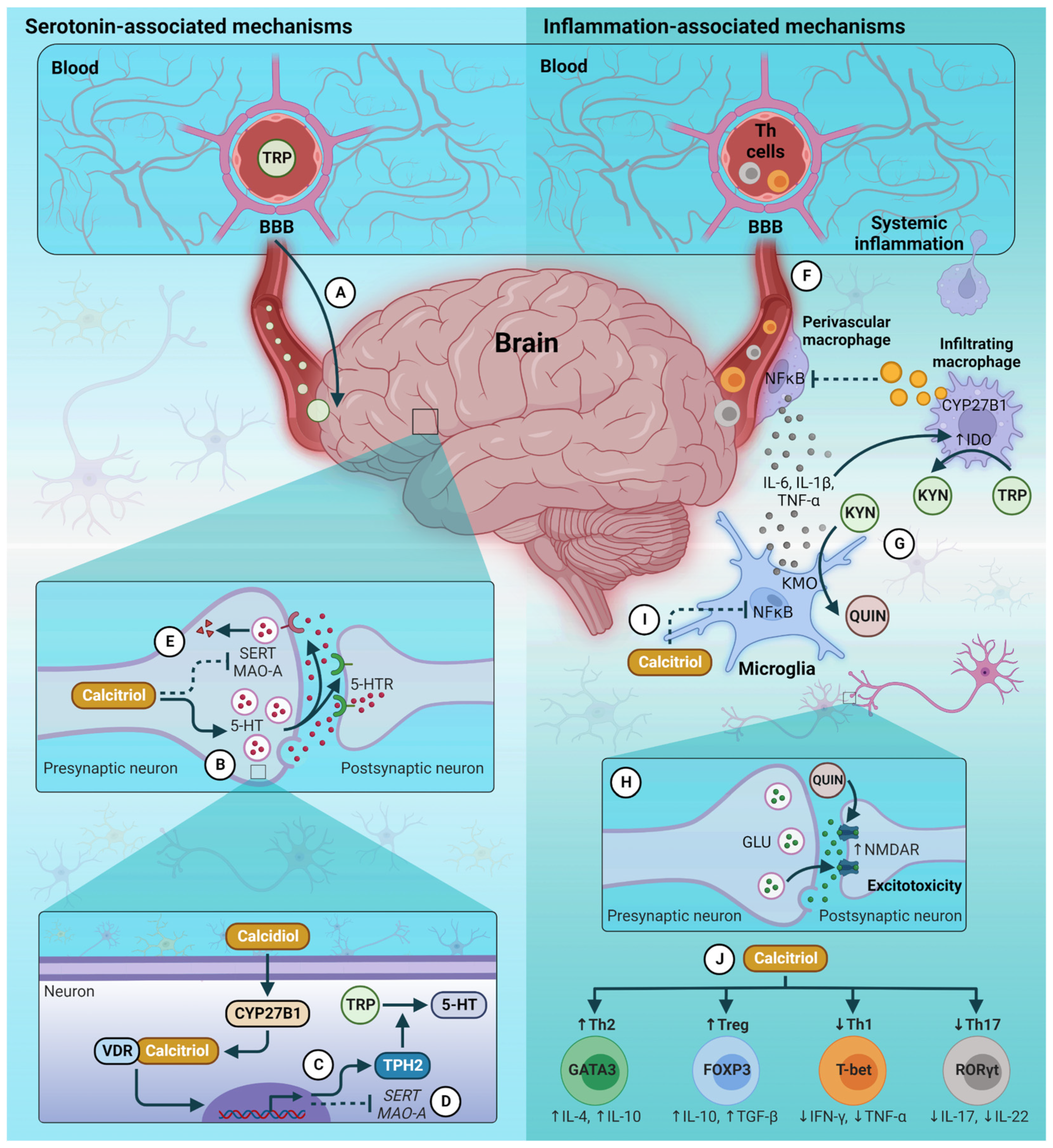
5.3. Vitamin D and Neurological Mechanisms Associated with Depression and Suicide
| Author, Year | Country; N; Age | Objective | Vitamin D Measure | Depression Measure | Intervention | Additional Outcomes | Results/Conclusion |
|---|---|---|---|---|---|---|---|
| Lansdowne et al., 1998 [95] | Australia; 44 healthy students; 18 to 43 years old | Test the efficiency of vitamin D supplementation on participants’ mood during winter | No measurement | The Positive and Negative Affect Schedule (PANAS) was used as a self-report measure of positive affectivity (PA) and negative affectivity (NA) | Subjects were given 400 IU, 800 IU, or no vitamin D3 for five days during late winter in a random double-blind study | None | Both doses (400 IU and 800 IU) increased their reported PA by almost a full standard deviation above their population mean. NA did not decrease significantly for either dose group compared to the placebo. Even though it did not reach significance, the trend for NA was a decrease in both dose groups. The placebo group remained practically matched the population means. |
| Hoogendijk et al., 2008 [94] | The Netherlands; 1282 residents; 65 to 95 years old | Explore if there is an association between altered calcidiol and parathyroid hormone (PTH) levels and depression | Serum calcidiol concentration was determined using a competitive binding protein assay (Nichols Institute Diagnostics Inc, San Juan Capistrano, California) | Depression was measured using self-reports (Centre for Epidemiologic Studies–Depression scale) and diagnostic interviews (Diagnostic Interview Schedule) | None | Potentially confounding factors and explanatory factors were also measured | Compared to 1087 control individuals, calcidiol levels were 14% lower in 169 persons with minor depression, whereas their PTH was 5% higher. Twenty-six persons with MDD also had a lower calcidiol level by 14% and higher PTH by 33%. Decreased serum calcidiol levels and increased serum PTH levels were significantly associated with depression severity (Center for Epidemiologic Studies Depression Scale). |
| Jorde et al., 2008 [96] | Norway; 441 subjects (BMI 28–47 kg/m); 21–70 years old | Serum calcidiol was determined by immunometric (electrochemiluminescence) using an automated clinical chemistry analyzer (Modular E170; Roche Diagnostics®) | Depressed mood was judged with the Beck Depression Inventory (BDI) at inclusion and the end of the study | 20,000 or 40,000 IU vitamin D per week or placebo for one year in a random double-blind study | Blood samples were drawn for analysis of serum calcium, creatinine, and parathyroid hormone (PTH) | Patients with < 40 nmol L(-1) calcidiol levels had significantly more depressive traits as measured by the total and subscales of the BDI than patients with serum levels ≥ 40 nmol L(-1) calcidiol levels. The BDI scores improved significantly after one year in both groups with vitamin D supplementation but not in the placebo group. | |
| Kaviani et al., 2020 [23] | Iran; 56 subjects with mild to moderate depression and no other psychiatric disorder; 18–60 years old | Assess the effects of vitamin D supplementation on consequent serum calcidiol, depression severity, and serotonin and oxytocin in patients with mild to moderate depression | The enzyme immunoassay (EIA) method was employed for assessing serum calcidiol (Euroimmun EIA kit, Lubeck, Germany) | Structural clinical diagnostic interview based on the DSM–IV criteria and Beck Depression Inventory-II (BDI-II) score | 50,000 IU cholecalciferol/2 weeks and control (placebo) in an 8-week double-blind, randomized clinical trial | Intact parathormone (iPTH), serum oxytocin, and platelet serotonin | After eight weeks, significant changes in the calcidiol concentrations and BDI-II scores were observed in the intervention group compared to the controls. Differences between groups were not significant for oxytocin and serotonin, but oxytocin concentrations were significantly reduced in controls, and platelet serotonin increased more in controls. |
| Rhee et al., 2020 [104] | Republic of Korea; 1736 subjects; 19 to 76 years old | Explore the association between specific domains of depressive symptoms and serum calcidiol concentrations by each sex | 25-Hydroxyvitamin D 125I RIA Kit (DiaSorin, Stillwater, MN, USA) using a 1470 WIZARD Gamma Counter (PerkinElmer, Turku, Finland) | Patient Health Questionnaire-9 (PHQ-9) | None | Other covariates such as sociodemographic information, lifestyle behaviors, and health factors | Log-transformed serum calcidiol concentrations and total PHQ-9 scores were associated significantly only in men after adjusting for various covariates. Moreover, the association between the cognitive and affective subscales and the serum calcidiol concentrations was significant only in men. No association was found in the somatic subscale. |
5.4. Vitamin D and Inflammatory Mechanisms Associated with Depression and Suicide
6. Relationship between VDR Gene, Depression, and Suicide
7. Vitamin D Supplementation for the Treatment of Depression
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| 1,25(OH)2D | calcitriol |
| 25(OH)D | calcidiol |
| 7-DHC | 7-dehydrocholesterol |
| ACC | anterior cingulate cortex |
| BBB | blood-brain barrier |
| BDNF | brain-derived neurotrophic factor |
| CRP | C-reactive protein |
| CYP27B1 | 25-hydroxyvitamin D-1 alpha hydroxylase |
| CYP2R1 | 25-hydroxylase |
| DBP | vitamin D binding protein |
| dlPFC | dorsolateral prefrontal cortex |
| HPA | hypothalamic–pituitary–adrenal |
| IDO | indoleamine 2,3-dioxygenase |
| IL | interleukin |
| KYN | kynurenine |
| LPS | lipopolysaccharide |
| MAO-A | monoamine oxidase-A |
| MDD | major depressive disorder |
| NF-κB | nuclear factor κB |
| NGF | nerve growth factor |
| NLR | neutrophile-to-lymphocyte ratio |
| NT | neurotrophin |
| QUIN | quinolinic acid |
| RCT | randomized clinical trials |
| RXR | retinoid X receptor |
| SAD | seasonal affective disorder |
| SERT | serotonin reuptake transporter |
| SSRI | selective serotonin reuptake inhibitors |
| TPH2 | tryptophan hydroxylase 2 |
| UVB | ultraviolet-B |
| VDR | vitamin D receptor |
| VDREs | vitamin D response elements |
| WBC | white blood cell count |
| WHO | World Health Organization |
References
- Turecki, G.; Brent, D.A. Suicide and Suicidal Behaviour. Lancet 2016, 387, 1227–1239. [Google Scholar] [CrossRef]
- Nock, M.K.; Borges, G.; Bromet, E.J.; Cha, C.B.; Kessler, R.C.; Lee, S. Suicide and Suicidal Behavior. Epidemiol. Rev. 2008, 30, 133–154. [Google Scholar] [CrossRef]
- World Health Organization. Suicide. Available online: https://www.who.int/news-room/fact-sheets/detail/suicide (accessed on 17 June 2022).
- Pathirathna, M.L.; Nandasena, H.M.R.K.G.; Atapattu, A.M.M.P.; Weerasekara, I. Impact of the COVID-19 Pandemic on Suicidal Attempts and Death Rates: A Systematic Review. BMC Psychiatry 2022, 22, 506. [Google Scholar] [CrossRef] [PubMed]
- Bilsen, J. Suicide and Youth: Risk Factors. Front. Psychiatry 2018, 9, 540. [Google Scholar] [CrossRef]
- Soreff, S.M.; Basit, H.; Attia, F.N. Suicide Risk. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK441982/ (accessed on 25 June 2022).
- Bachmann, S. Epidemiology of Suicide and the Psychiatric Perspective. Int. J. Environ. Res. Public Health 2018, 15, 1425. [Google Scholar] [CrossRef] [PubMed]
- Gili, M.; Castellví, P.; Vives, M.; de la Torre-Luque, A.; Almenara, J.; Blasco, M.J.; Cebrià, A.I.; Gabilondo, A.; Pérez-Ara, M.A.; A, M.-M.; et al. Mental disorders as risk factors for suicidal behavior in young people: A meta-analysis and systematic review of longitudinal studies. J. Affect. Disord. 2019, 245, 152–162. [Google Scholar] [CrossRef]
- Chand, S.P.; Arif, H. Depression. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK430847/ (accessed on 25 June 2022).
- Cesari, M.; Incalzi, R.A.; Zamboni, V.; Pahor, M. Vitamin D Hormone: A Multitude of Actions Potentially Influencing the Physical Function Decline in Older Persons. Geriatr. Gerontol. Int. 2011, 11, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Hossein-nezhad, A.; Holick, M.F. Vitamin D for Health: A Global Perspective. Mayo Clin. Proc. 2013, 88, 720–755. [Google Scholar] [CrossRef]
- Ellison, D.L.; Moran, H.R. Vitamin D: Vitamin or Hormone? Nurs. Clin. N. Am. 2021, 56, 47–57. [Google Scholar] [CrossRef] [PubMed]
- Nair, R.; Maseeh, A. Vitamin D: The “Sunshine” Vitamin. J. Pharmacol. Pharmacother. 2012, 3, 118–126. [Google Scholar]
- Khammissa, R.A.G.; Fourie, J.; Motswaledi, M.H.; Ballyram, R.; Lemmer, J.; Feller, L. The Biological Activities of Vitamin D and Its Receptor in Relation to Calcium and Bone Homeostasis, Cancer, Immune and Cardiovascular Systems, Skin Biology, and Oral Health. BioMed Res. Int. 2018, 2018, 9276380. [Google Scholar] [CrossRef]
- Prietl, B.; Treiber, G.; Pieber, T.R.; Amrein, K. Vitamin D and Immune Function. Nutrients 2013, 5, 2502–2521. [Google Scholar] [CrossRef] [PubMed]
- Eyles, D.W. Vitamin D: Brain and Behavior. JBMR Plus 2020, 5, e10419. [Google Scholar] [CrossRef]
- Ceolin, G.; Matsuo, L.H.; Confortin, S.C.; D’Orsi, E.; Rieger, D.K.; Moreira, J.D. Lower Serum 25-Hydroxycholecalciferol Is Associated with Depressive Symptoms in Older Adults in Southern Brazil. Nutr. J. 2020, 19, 123. [Google Scholar] [CrossRef] [PubMed]
- Grudet, C.; Lindqvist, D.; Malm, J.; Westrin, Å.; Ventorp, F. 25(OH)D Levels Are Decreased in Patients with Difficult-to-Treat Depression. Compr. Psychoneuroendocrinol. 2022, 10, 100126. [Google Scholar] [CrossRef]
- Gokalp, G. The Association between Low Vitamin D Levels and Suicide Attempts in Adolescents. Ann. Clin. Psychiatry Off. J. Am. Acad. Clin. Psychiatr. 2020, 32, 106–113. [Google Scholar]
- Umhau, J.C.; George, D.T.; Heaney, R.P.; Lewis, M.D.; Ursano, R.J.; Heilig, M.; Hibbeln, J.R.; Schwandt, M.L. Low Vitamin D Status and Suicide: A Case-Control Study of Active Duty Military Service Members. PLoS ONE 2013, 8, e51543. [Google Scholar] [CrossRef]
- Eyles, D.W.; Burne, T.H.J.; McGrath, J.J. Vitamin D, Effects on Brain Development, Adult Brain Function and the Links between Low Levels of Vitamin D and Neuropsychiatric Disease. Front. Neuroendocrinol. 2013, 34, 47–64. [Google Scholar] [CrossRef]
- Khalighi Sikaroudi, M.; Mokhtare, M.; Shidfar, F.; Janani, L.; Faghihi Kashani, A.; Masoodi, M.; Agah, S.; Dehnad, A.; Shidfar, S. Effects of Vitamin D3 Supplementation on Clinical Symptoms, Quality of Life, Serum Serotonin (5-Hydroxytryptamine), 5-Hydroxy-Indole Acetic Acid, and Ratio of 5-HIAA/5-HT in Patients with Diarrhea-Predominant Irritable Bowel Syndrome: A Randomized Clinical Trial. EXCLI J. 2020, 19, 652–667. [Google Scholar] [CrossRef]
- Kaviani, M.; Nikooyeh, B.; Zand, H.; Yaghmaei, P.; Neyestani, T.R. Effects of Vitamin D Supplementation on Depression and Some Involved Neurotransmitters. J. Affect. Disord. 2020, 269, 28–35. [Google Scholar] [CrossRef]
- Grudet, C.; Wolkowitz, O.M.; Mellon, S.H.; Malm, J.; Reus, V.I.; Brundin, L.; Nier, B.M.; Dhabhar, F.S.; Hough, C.M.; Westrin, Å.; et al. Vitamin D and Inflammation in Major Depressive Disorder. J. Affect. Disord. 2020, 267, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Lindqvist, D.; Dhabhar, F.S.; James, S.J.; Hough, C.M.; Jain, F.A.; Bersani, F.S.; Reus, V.I.; Verhoeven, J.E.; Epel, E.S.; Mahan, L.; et al. Oxidative Stress, Inflammation and Treatment Response in Major Depression. Psychoneuroendocrinology 2017, 76, 197–205. [Google Scholar] [CrossRef]
- Borel, P.; Caillaud, D.; Cano, N.J. Vitamin D Bioavailability: State of the Art. Crit. Rev. Food Sci. Nutr. 2015, 55, 1193–1205. [Google Scholar] [CrossRef]
- Holick, M.F.; Smith, E.; Pincus, S. Skin as the Site of Vitamin D Synthesis and Target Tissue for 1,25-Dihydroxyvitamin D3. Use of Calcitriol (1,25-Dihydroxyvitamin D3) for Treatment of Psoriasis. Arch. Dermatol. 1987, 123, 1677–1683a. [Google Scholar] [CrossRef]
- Holick, M.F. Vitamin D Deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Farruggia, M.; Veronese, N.; Barbagallo, M. Vitamin D Sources, Metabolism, and Deficiency: Available Compounds and Guidelines for Its Treatment. Metabolites 2021, 11, 255. [Google Scholar] [CrossRef]
- Charoenngam, N.; Holick, M.F. Immunologic Effects of Vitamin D on Human Health and Disease. Nutrients 2020, 12, 2097. [Google Scholar] [CrossRef] [PubMed]
- Bleizgys, A. Vitamin D Dosing: Basic Principles and a Brief Algorithm (2021 Update). Nutrients 2021, 13, 4415. [Google Scholar] [CrossRef]
- Dudenkov, D.V.; Mara, K.C.; Petterson, T.M.; Maxson, J.A.; Thacher, T.D. Serum 25-Hydroxyvitamin D Values and Risk of All-Cause and Cause-Specific Mortality: A Population-Based Cohort Study. Mayo Clin. Proc. 2018, 93, 721–730. [Google Scholar] [CrossRef]
- Holick, M.F. Sunlight and Vitamin D for Bone Health and Prevention of Autoimmune Diseases, Cancers, and Cardiovascular Disease. Am. J. Clin. Nutr. 2004, 80, 1678S–1688S. [Google Scholar] [CrossRef] [PubMed]
- Brannon, P.M.; Fleet, J.C. Vitamin D. Adv. Nutr. 2011, 2, 365–367. [Google Scholar] [CrossRef] [PubMed]
- Bikle, D.D. Vitamin D: Production, Metabolism and Mechanisms of Action. In Endotext [Internet]; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W., Dhatariya, K., Dungan, K., Hershman, J.M., Hofland, J., Kalra, S., et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2000. [Google Scholar]
- Pilz, S.; Zittermann, A.; Trummer, C.; Theiler-Schwetz, V.; Lerchbaum, E.; Keppel, M.H.; Grübler, M.R.; März, W.; Pandis, M. Vitamin D Testing and Treatment: A Narrative Review of Current Evidence. Endocr. Connect. 2019, 8, R27–R43. [Google Scholar] [CrossRef]
- Wang, T.-T.; Tavera-Mendoza, L.E.; Laperriere, D.; Libby, E.; Burton MacLeod, N.; Nagai, Y.; Bourdeau, V.; Konstorum, A.; Lallemant, B.; Zhang, R.; et al. Large-Scale in Silico and Microarray-Based Identification of Direct 1,25-Dihydroxyvitamin D3 Target Genes. Mol. Endocrinol. 2005, 19, 2685–2695. [Google Scholar] [CrossRef]
- Carlberg, C. Nutrigenomics of Vitamin D. Nutrients 2019, 11, 676. [Google Scholar] [CrossRef]
- Balabanova, S.; Richter, H.P.; Antoniadis, G.; Homoki, J.; Kremmer, N.; Hanle, J.; Teller, W.M. 25-Hydroxyvitamin D, 24, 25-Dihydroxyvitamin D and 1,25-Dihydroxyvitamin D in Human Cerebrospinal Fluid. Klin. Wochenschr. 1984, 62, 1086–1090. [Google Scholar] [CrossRef]
- Holmøy, T.; Moen, S.M.; Gundersen, T.A.; Holick, M.F.; Fainardi, E.; Castellazzi, M.; Casetta, I. 25-Hydroxyvitamin D in Cerebrospinal Fluid during Relapse and Remission of Multiple Sclerosis. Mult. Scler. 2009, 15, 1280–1285. [Google Scholar] [CrossRef] [PubMed]
- Cui, X.; Eyles, D.W. Vitamin D and the Central Nervous System: Causative and Preventative Mechanisms in Brain Disorders. Nutrients 2022, 14, 4353. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, K.; Shahrokhi, M.; Huecker, M.R. Vitamin D. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK441912/ (accessed on 3 July 2022).
- Pike, J.W.; Meyer, M.B.; Lee, S.-M.; Onal, M.; Benkusky, N.A. The Vitamin D Receptor: Contemporary Genomic Approaches Reveal New Basic and Translational Insights. J. Clin. Investig. 2017, 127, 1146–1154. [Google Scholar] [CrossRef]
- Gáll, Z.; Székely, O. Role of Vitamin D in Cognitive Dysfunction: New Molecular Concepts and Discrepancies between Animal and Human Findings. Nutrients 2021, 13, 3672. [Google Scholar] [CrossRef] [PubMed]
- Landel, V.; Stephan, D.; Cui, X.; Eyles, D.; Feron, F. Differential Expression of Vitamin D-Associated Enzymes and Receptors in Brain Cell Subtypes. J. Steroid Biochem. Mol. Biol. 2018, 177, 129–134. [Google Scholar] [CrossRef]
- Garcion, E.; Wion-Barbot, N.; Montero-Menei, C.N.; Berger, F.; Wion, D. New Clues about Vitamin D Functions in the Nervous System. Trends Endocrinol. Metab. 2002, 13, 100–105. [Google Scholar] [CrossRef]
- Latimer, C.S.; Brewer, L.D.; Searcy, J.L.; Chen, K.-C.; Popović, J.; Kraner, S.D.; Thibault, O.; Blalock, E.M.; Landfield, P.W.; Porter, N.M. Vitamin D Prevents Cognitive Decline and Enhances Hippocampal Synaptic Function in Aging Rats. Proc. Natl. Acad. Sci. USA 2014, 111, E4359–E4366. [Google Scholar] [CrossRef] [PubMed]
- Moore, M.E.; Piazza, A.; McCartney, Y.; Lynch, M.A. Evidence That Vitamin D3 Reverses Age-Related Inflammatory Changes in the Rat Hippocampus. Biochem. Soc. Trans. 2005, 33, 573–577. [Google Scholar] [CrossRef] [PubMed]
- Eyles, D.W.; Smith, S.; Kinobe, R.; Hewison, M.; McGrath, J.J. Distribution of the Vitamin D Receptor and 1 Alpha-Hydroxylase in Human Brain. J. Chem. Neuroanat. 2005, 29, 21–30. [Google Scholar] [CrossRef]
- Bertone-Johnson, E.R. Vitamin D and the Occurrence of Depression: Causal Association or Circumstantial Evidence? Nutr. Rev. 2009, 67, 481–492. [Google Scholar] [CrossRef] [PubMed]
- Sanchez, B.; Relova, J.L.; Gallego, R.; Ben-Batalla, I.; Perez-Fernandez, R. 1,25-Dihydroxyvitamin D3 Administration to 6-Hydroxydopamine-Lesioned Rats Increases Glial Cell Line-Derived Neurotrophic Factor and Partially Restores Tyrosine Hydroxylase Expression in Substantia Nigra and Striatum. J. Neurosci. Res. 2009, 87, 723–732. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.Y.; Wu, J.N.; Cherng, T.L.; Hoffer, B.J.; Chen, H.H.; Borlongan, C.V.; Wang, Y. Vitamin D(3) Attenuates 6-Hydroxydopamine-Induced Neurotoxicity in Rats. Brain Res. 2001, 904, 67–75. [Google Scholar] [CrossRef]
- Klonsky, E.D.; May, A.M.; Saffer, B.Y. Suicide, Suicide Attempts, and Suicidal Ideation. Annu. Rev. Clin. Psychol. 2016, 12, 307–330. [Google Scholar] [CrossRef] [PubMed]
- Park, E.H.; Hong, N.; Jon, D.I.; Hong, H.J.; Jung, M.H. Past Suicidal Ideation as an Independent Risk Factor for Suicide Behaviours in Patients with Depression. Int. J. Psychiatry Clin. Pract. 2017, 21, 24–28. [Google Scholar] [CrossRef]
- Walling, M.A. Suicide Contagion. Curr. Trauma Rep. 2021, 7, 103–114. [Google Scholar] [CrossRef]
- Ribeiro, J.D.; Huang, X.; Fox, K.R.; Franklin, J.C. Depression and Hopelessness as Risk Factors for Suicide Ideation, Attempts and Death: Meta-Analysis of Longitudinal Studies. Br. J. Psychiatry 2018, 212, 279–286. [Google Scholar] [CrossRef]
- Li, H.; Luo, X.; Ke, X.; Dai, Q.; Zheng, W.; Zhang, C.; Cassidy, R.M.; Soares, J.C.; Zhang, X.Y.; Ning, Y. Major Depressive Disorder and Suicide Risk among Adult Outpatients at Several General Hospitals in a Chinese Han Population. PLoS ONE 2017, 12, e0186143. [Google Scholar] [CrossRef] [PubMed]
- Orsolini, L.; Latini, R.; Pompili, M.; Serafini, G.; Volpe, U.; Vellante, F.; Fornaro, M.; Valchera, A.; Tomasetti, C.; Fraticelli, S.; et al. Understanding the Complex of Suicide in Depression: From Research to Clinics. Psychiatry Investig. 2020, 17, 207–221. [Google Scholar] [CrossRef]
- Kobeissy, F.H. Psychiatric Disorders, 2nd ed.; Methods in Molecular, Biology; Kobeissy, F.H., Ed.; Springer: New York, NY, USA, 2019; Volume 2011, ISBN 978-1-4939-9553-0. [Google Scholar]
- Perez-Caballero, L.; Torres-Sanchez, S.; Romero-López-Alberca, C.; González-Saiz, F.; Mico, J.A.; Berrocoso, E. Monoaminergic System and Depression. Cell Tissue Res. 2019, 377, 107–113. [Google Scholar] [CrossRef]
- Ushakova, V.M.; Morozova, A.Y.; Reznik, A.M.; Kostyuk, G.P.; Chekhonin, V.P. Molecular Biological Aspects of Depressive Disorders: A Modern View. Mol. Biol. 2020, 54, 639–660. [Google Scholar] [CrossRef]
- Patrick, R.P.; Ames, B.N. Vitamin D Hormone Regulates Serotonin Synthesis. Part 1: Relevance for Autism. FASEB J. 2014, 28, 2398–2413. [Google Scholar] [CrossRef] [PubMed]
- Miura, H.; Ozaki, N.; Sawada, M.; Isobe, K.; Ohta, T.; Nagatsu, T. A Link between Stress and Depression: Shifts in the Balance between the Kynurenine and Serotonin Pathways of Tryptophan Metabolism and the Etiology and Pathophysiology of Depression. Stress 2008, 11, 198–209. [Google Scholar] [CrossRef] [PubMed]
- Sublette, M.E.; Galfalvy, H.C.; Fuchs, D.; Lapidus, M.; Grunebaum, M.F.; Oquendo, M.A.; Mann, J.J.; Postolache, T.T. Plasma Kynurenine Levels Are Elevated in Suicide Attempters with Major Depressive Disorder. Brain. Behav. Immun. 2011, 25, 1272–1278. [Google Scholar] [CrossRef]
- Brundin, L.; Erhardt, S.; Bryleva, E.Y.; Achtyes, E.D.; Postolache, T.T. The Role of Inflammation in Suicidal Behaviour. Acta Psychiatr. Scand. 2015, 132, 192–203. [Google Scholar] [CrossRef]
- Erhardt, S.; Lim, C.K.; Linderholm, K.R.; Janelidze, S.; Lindqvist, D.; Samuelsson, M.; Lundberg, K.; Postolache, T.T.; Träskman-Bendz, L.; Guillemin, G.J.; et al. Connecting Inflammation with Glutamate Agonism in Suicidality. Neuropsychopharmacology 2013, 38, 743–752. [Google Scholar] [CrossRef]
- Raison, C.L.; Dantzer, R.; Kelley, K.W.; Lawson, M.A.; Woolwine, B.J.; Vogt, G.; Spivey, J.R.; Saito, K.; Miller, A.H. CSF Concentrations of Brain Tryptophan and Kynurenines during Immune Stimulation with IFN-Alpha: Relationship to CNS Immune responses and Depression. Mol. Psychiatry 2010, 15, 393–403. [Google Scholar] [CrossRef] [PubMed]
- Spellman, T.; Liston, C. Toward Circuit Mechanisms of Pathophysiology in Depression. Am. J. Psychiatry 2020, 177, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Troubat, R.; Barone, P.; Leman, S.; Desmidt, T.; Cressant, A.; Atanasova, B.; Brizard, B.; El Hage, W.; Surget, A.; Belzung, C.; et al. Neuroinflammation and Depression: A Review. Eur. J. Neurosci. 2021, 53, 151–171. [Google Scholar] [CrossRef] [PubMed]
- Juruena, M.F. Early-Life Stress and HPA Axis Trigger Recurrent Adulthood Depression. Epilepsy Behav. 2014, 38, 148–159. [Google Scholar] [CrossRef]
- Berardelli, I.; Serafini, G.; Cortese, N.; Fiaschè, F.; O’Connor, R.C.; Pompili, M. The Involvement of Hypothalamus-Pituitary-Adrenal (HPA) Axis in Suicide Risk. Brain Sci. 2020, 10, 653. [Google Scholar] [CrossRef] [PubMed]
- Heim, C.; Nemeroff, C.B. The Role of Childhood Trauma in the Neurobiology of Mood and Anxiety Disorders: Preclinical and Clinical Studies. Biol. Psychiatry 2001, 49, 1023–1039. [Google Scholar] [CrossRef]
- Janelidze, S.; Mattei, D.; Westrin, Å.; Träskman-Bendz, L.; Brundin, L. Cytokine Levels in the Blood May Distinguish Suicide Attempters from Depressed Patients. Brain. Behav. Immun. 2011, 25, 335–339. [Google Scholar] [CrossRef]
- Lee, K.-M.; Kim, Y.-K. The Role of IL-12 and TGF-Β1 in the Pathophysiology of Major Depressive Disorder. Int. Immunopharmacol. 2006, 6, 1298–1304. [Google Scholar] [CrossRef]
- Yamasaki, K.; Hasegawa, T.; Takeda, M. Serum Level of Soluble Interleukin 6 Receptor Is a Useful Biomarker for Identification of Treatment-resistant Major Depressive Disorder. Neuropsychopharmacol. Rep. 2020, 40, 130–137. [Google Scholar] [CrossRef]
- Brundin, L.; Bryleva, E.Y.; Thirtamara Rajamani, K. Role of Inflammation in Suicide: From Mechanisms to Treatment. Neuropsychopharmacology 2017, 42, 271–283. [Google Scholar] [CrossRef]
- Calandre, E.P.; Rico-Villademoros, F.; Slim, M. Suicidal Behaviors in Patients with Rheumatic Diseases: A Narrative Review. Rheumatol. Int. 2018, 38, 537–548. [Google Scholar] [CrossRef]
- Miyaoka, H.; Otsubo, T.; Kamijima, K.; Ishii, M.; Onuki, M.; Mitamura, K. Depression from Interferon Therapy in Patients with Hepatitis C. Am. J. Psychiatry 1999, 156, 1120. [Google Scholar] [CrossRef]
- Yirmiya, R.; Pollak, Y.; Morag, M.; Reichenberg, A.; Barak, O.; Avitsur, R.; Shavit, Y.; Ovadia, H.; Weidenfeld, J.; Morag, A.; et al. Illness, Cytokines, and Depression. Ann. N. Y. Acad. Sci. 2000, 917, 478–487. [Google Scholar] [CrossRef] [PubMed]
- Steiner, J.; Bielau, H.; Brisch, R.; Danos, P.; Ullrich, O.; Mawrin, C.; Bernstein, H.-G.; Bogerts, B. Immunological Aspects in the Neurobiology of Suicide: Elevated Microglial Density in Schizophrenia and Depression Is Associated with Suicide. J. Psychiatr. Res. 2008, 42, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Black, C.; Miller, B.J. Meta-Analysis of Cytokines and Chemokines in Suicidality: Distinguishing Suicidal Versus Nonsuicidal Patients. Biol. Psychiatry 2015, 78, 28–37. [Google Scholar] [CrossRef]
- Nussbaumer-Streit, B.; Forneris, C.A.; Morgan, L.C.; Van Noord, M.G.; Gaynes, B.N.; Greenblatt, A.; Wipplinger, J.; Lux, L.J.; Winkler, D.; Gartlehner, G. Light Therapy for Preventing Seasonal Affective Disorder. Cochrane Database Syst. Rev. 2019, 3, CD011269. [Google Scholar] [CrossRef] [PubMed]
- Munir, S.; Abbas, M. Seasonal Depressive Disorder. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK568745/ (accessed on 7 July 2022).
- Galima, S.V.; Vogel, S.R.; Kowalski, A.W. Seasonal Affective Disorder: Common Questions and Answers. Am. Fam. Physician 2020, 102, 668–672. [Google Scholar]
- Roecklein, K.A.; Rohan, K.J. Seasonal Affective Disorder: An Overview and Update. Psychiatry 2005, 2, 20–26. [Google Scholar]
- Sabir, M.S.; Haussler, M.R.; Mallick, S.; Kaneko, I.; Lucas, D.A.; Haussler, C.A.; Whitfield, G.K.; Jurutka, P.W. Optimal Vitamin D Spurs Serotonin: 1,25-Dihydroxyvitamin D Represses Serotonin Reuptake Transport (SERT) and Degradation (MAO-A) Gene Expression in Cultured Rat Serotonergic Neuronal Cell Lines. Genes Nutr. 2018, 13, 19. [Google Scholar] [CrossRef] [PubMed]
- Berk, M.; Williams, L.J.; Jacka, F.N.; O’Neil, A.; Pasco, J.A.; Moylan, S.; Allen, N.B.; Stuart, A.L.; Hayley, A.C.; Byrne, M.L.; et al. So Depression Is an Inflammatory Disease, but Where Does the Inflammation Come From? BMC Med. 2013, 11, 200. [Google Scholar] [CrossRef]
- Shin, Y.-C.; Jung, C.-H.; Kim, H.-J.; Kim, E.-J.; Lim, S.-W. The Associations among Vitamin D Deficiency, C-Reactive Protein, and Depressive Symptoms. J. Psychosom. Res. 2016, 90, 98–104. [Google Scholar] [CrossRef]
- Tariq, M.M.; Streeten, E.A.; Smith, H.A.; Sleemi, A.; Khabazghazvini, B.; Vaswani, D.; Postolache, T.T. Vitamin D: A Potential Role in Reducing Suicide Risk? Int. J. Adolesc. Med. Health 2011, 23, 157–165. [Google Scholar] [CrossRef]
- Grudet, C.; Malm, J.; Westrin, Å.; Brundin, L. Suicidal Patients Are Deficient in Vitamin D, Associated with a pro-Inflammatory Status in the Blood. Psychoneuroendocrinology 2014, 50, 210–219. [Google Scholar] [CrossRef]
- Calderón Espinoza, I.; Chavarria-Avila, E.; Pizano-Martinez, O.; Martínez-García, E.A.; Armendariz-Borunda, J.; Marquez-Aguirre, A.L.; Llamas-García, A.; Corona-Sánchez, E.G.; Toriz González, G.; Vazquez-Del Mercado, M. Suicide Risk in Rheumatoid Arthritis Patients is Associated With Suboptimal Vitamin D Levels. JCR J. Clin. Rheumatol. 2022, 28, 137–142. [Google Scholar] [CrossRef]
- Park, J.I.; Yang, J.C.; Park, T.W.; Chung, S.K. Is Serum 25-Hydroxyvitamin D Associated with Depressive Symptoms and Suicidal Ideation in Korean Adults? Int. J. Psychiatry Med. 2016, 51, 31–46. [Google Scholar] [CrossRef] [PubMed]
- Manicourt, D.-H.; Devogelaer, J.-P. Urban Tropospheric Ozone Increases the Prevalence of Vitamin D Deficiency among Belgian Postmenopausal Women with Outdoor Activities during Summer. J. Clin. Endocrinol. Metab. 2008, 93, 3893–3899. [Google Scholar] [CrossRef] [PubMed]
- Hoogendijk, W.J.G.; Lips, P.; Dik, M.G.; Deeg, D.J.H.; Beekman, A.T.F.; Penninx, B.W.J.H. Depression Is Associated with Decreased 25-Hydroxyvitamin D and Increased Parathyroid Hormone Levels in Older Adults. Arch. Gen. Psychiatry 2008, 65, 508–512. [Google Scholar] [CrossRef]
- Lansdowne, A.T.G.; Provost, S.C. Vitamin D3 Enhances Mood in Healthy Subjects during Winter. Psychopharmacology 1998, 135, 319–323. [Google Scholar] [CrossRef]
- Jorde, R.; Sneve, M.; Figenschau, Y.; Svartberg, J.; Waterloo, K. Effects of Vitamin D Supplementation on Symptoms of Depression in Overweight and Obese Subjects: Randomized Double Blind Trial. J. Intern. Med. 2008, 264, 599–609. [Google Scholar] [CrossRef] [PubMed]
- Kirsch, I.; Deacon, B.J.; Huedo-Medina, T.B.; Scoboria, A.; Moore, T.J.; Johnson, B.T. Initial Severity and Antidepressant Benefits: A Meta-Analysis of Data Submitted to the Food and Drug Administration. PLoS Med. 2008, 5, e45. [Google Scholar] [CrossRef]
- Kaneko, I.; Sabir, M.S.; Dussik, C.M.; Whitfield, G.K.; Karrys, A.; Hsieh, J.C.; Haussler, M.R.; Meyer, M.B.; Pike, J.W.; Jurutka, P.W. 1,25-DihydroxyVitamin D Regulates Expression of the Tryptophan Hydroxylase 2 and Leptin Genes: Implication for Behavioral Influences of Vitamin D. FASEB J. 2015, 29, 4023–4035. [Google Scholar] [CrossRef]
- Postolache, T.T.; Akram, F.; Lee, E.E.; Lowry, C.A.; Stiller, J.W.; Brenner, L.A.; Streeten, E.A.; Turecki, G.; Dwivedi, Y. Increased Brain Vitamin D Receptor Expression and Decreased Expression of Cathelicidin Antimicrobial Peptide in Individuals Who Died by Suicide. J. Psychiatr. Res. 2020, 125, 75–84. [Google Scholar] [CrossRef]
- Patrick, R.P.; Ames, B.N. Vitamin D and the Omega-3 Fatty Acids Control Serotonin Synthesis and Action, Part 2: Relevance for ADHD, Bipolar Disorder, Schizophrenia, and Impulsive Behavior. FASEB J. 2015, 29, 2207–2222. [Google Scholar] [CrossRef] [PubMed]
- Haussler, M.R.; Jurutka, P.W.; Mizwicki, M.; Norman, A.W. Vitamin D Receptor (VDR)-Mediated Actions of 1α,25(OH)2vitamin D3: Genomic and Non-Genomic Mechanisms. Best Pract. Res. Clin. Endocrinol. Metab. 2011, 25, 543–559. [Google Scholar] [CrossRef]
- Akpınar, Ş.; Karadağ, M.G. Is Vitamin D Important in Anxiety or Depression? What Is the Truth? Curr. Nutr. Rep. 2022, 11, 675–681. [Google Scholar] [CrossRef]
- Ceolin, G.; Mano, G.P.R.; Hames, N.S.; Antunes, L.D.C.; Brietzke, E.; Rieger, D.K.; Moreira, J.D. Vitamin D, Depressive Symptoms, and COVID-19 Pandemic. Front. Neurosci. 2021, 15, 670879. [Google Scholar] [CrossRef]
- Rhee, S.J.; Lee, H.; Ahn, Y.M. Serum Vitamin D Concentrations Are Associated With Depressive Symptoms in Men: The Sixth Korea National Health and Nutrition Examination Survey 2014. Front. Psychiatry 2020, 11, 653. [Google Scholar] [CrossRef]
- Farooq, R.K.; Asghar, K.; Kanwal, S.; Zulqernain, A. Role of Inflammatory Cytokines in Depression: Focus on Interleukin-1β. Biomed. Rep. 2017, 6, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Hashash, J.G.; Vachon, A.; Ramos Rivers, C.; Regueiro, M.D.; Binion, D.G.; Altman, L.; Williams, C.; Szigethy, E. Predictors of Suicidal Ideation Among IBD Outpatients. J. Clin. Gastroenterol. 2019, 53, e41–e45. [Google Scholar] [CrossRef]
- Dogan-Sander, E.; Mergl, R.; Willenberg, A.; Baber, R.; Wirkner, K.; Riedel-Heller, S.G.; Röhr, S.; Schmidt, F.M.; Schomerus, G.; Sander, C. Inflammation and the Association of Vitamin D and Depressive Symptomatology. Nutrients 2021, 13, 1972. [Google Scholar] [CrossRef] [PubMed]
- Nerhus, M.; Berg, A.O.; Kvitland, L.R.; Dieset, I.; Hope, S.; Dahl, S.R.; Weibell, M.A.; Romm, K.L.; Faerden, A.; Andreassen, O.A.; et al. Low Vitamin D Is Associated with Negative and Depressive Symptoms in Psychotic Disorders. Schizophr. Res. 2016, 178, 44–49. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, A.V.; Feldman, D. Molecular Pathways Mediating the Anti-Inflammatory Effects of Calcitriol: Implications for Prostate Cancer Chemoprevention and Treatment. Endocr. Relat. Cancer 2010, 17, R19–R38. [Google Scholar] [CrossRef]
- Vaccaro, J.A.; Qasem, A.; Naser, S.A. Cathelicidin Mediates an Anti-Inflammatory Role of Active Vitamin D (Calcitriol) During M. Paratuberculosis Infection. Front. Cell. Infect. Microbiol. 2022, 12, 875772. [Google Scholar] [CrossRef] [PubMed]
- Cantorna, M.T.; Waddell, A. The Vitamin D Receptor Turns off Chronically Activated T Cells. Ann. N. Y. Acad. Sci. 2014, 1317, 70–75. [Google Scholar] [CrossRef] [PubMed]
- Berg, A.O.; Jørgensen, K.N.; Nerhus, M.; Athanasiu, L.; Popejoy, A.B.; Bettella, F.; Norbom, L.C.B.; Gurholt, T.P.; Dahl, S.R.; Andreassen, O.A.; et al. Vitamin D Levels, Brain Volume, and Genetic Architecture in Patients with Psychosis. PLoS ONE 2018, 13, e0200250. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.-Y.; Jeon, S.-W.; Lim, W.-J.; Oh, K.-S.; Shin, D.-W.; Cho, S.J.; Park, J.-H.; Kim, Y.H.; Shin, Y.-C. Vitamin D Deficiency and Suicidal Ideation: A Cross-Sectional Study of 157,211 Healthy Adults. J. Psychosom. Res. 2020, 134, 110125. [Google Scholar] [CrossRef]
- Wei, Y.X.; Liu, B.P.; Qiu, H.M.; Zhang, J.Y.; Wang, X.T.; Jia, C.X. Effects of Vitamin D-Related Gene Polymorphisms on Attempted Suicide. Psychiatr. Genet. 2021, 31, 230–238. [Google Scholar] [CrossRef]
- Pike, J.W.; Meyer, M.B. The Vitamin D Receptor: New Paradigms for the Regulation of Gene Expression by 1,25-Dihydroxyvitamin D3. Rheum. Dis. Clin. N. Am. 2012, 38, 13–27. [Google Scholar] [CrossRef]
- Eghtedarian, R.; Ghafouri-Fard, S.; Bouraghi, H.; Hussen, B.M.; Arsang-Jang, S.; Taheri, M. Abnormal Pattern of Vitamin D Receptor-Associated Genes and LncRNAs in Patients with Bipolar Disorder. BMC Psychiatry 2022, 22, 178. [Google Scholar] [CrossRef]
- Kuningas, M.; Mooijaart, S.P.; Jolles, J.; Slagboom, P.E.; Westendorp, R.G.J.; van Heemst, D. VDR Gene Variants Associate with Cognitive Function and Depressive Symptoms in Old Age. Neurobiol. Aging 2009, 30, 466–473. [Google Scholar] [CrossRef]
- Glocke, M.; Lang, F.; Schaeffeler, E.; Lang, T.; Schwab, M.; Lang, U.E. Impact of Vitamin D Receptor VDR Rs2228570 Polymorphism in Oldest Old. Kidney Blood Press. Res. 2013, 37, 311–322. [Google Scholar] [CrossRef] [PubMed]
- Valdivielso, J.M.; Fernandez, E. Vitamin D Receptor Polymorphisms and Diseases. Clin. Chim. Acta 2006, 371, 1–12. [Google Scholar] [CrossRef]
- Penckofer, S.; Ridosh, M.; Adams, W.; Grzesiak, M.; Woo, J.; Byrn, M.; Kouba, J.; Sheean, P.; Kordish, C.; Durazo-Arvizu, R.; et al. Vitamin D Supplementation for the Treatment of Depressive Symptoms in Women with Type 2 Diabetes: A Randomized Clinical Trial. J. Diabetes Res. 2022, 2022, 4090807. [Google Scholar] [CrossRef]
- Omidian, M.; Mahmoudi, M.; Abshirini, M.; Eshraghian, M.R.; Javanbakht, M.H.; Zarei, M.; Hasani, H.; Djalali, M. Effects of Vitamin D Supplementation on Depressive Symptoms in Type 2 Diabetes Mellitus Patients: Randomized Placebo-Controlled Double-Blind Clinical Trial. Diabetes Metab. Syndr. 2019, 13, 2375–2380. [Google Scholar] [CrossRef] [PubMed]
- Vellekkatt, F.; Menon, V.; Rajappa, M.; Sahoo, J. Effect of Adjunctive Single Dose Parenteral Vitamin D Supplementation in Major Depressive Disorder with Concurrent Vitamin D Deficiency: A Double-Blind Randomized Placebo-Controlled Trial. J. Psychiatr. Res. 2020, 129, 250–256. [Google Scholar] [CrossRef]
- Zhu, C.; Zhang, Y.; Wang, T.; Lin, Y.; Yu, J.; Xia, Q.; Zhu, P.; Zhu, D.-M. Vitamin D Supplementation Improves Anxiety but Not Depression Symptoms in Patients with Vitamin D Deficiency. Brain Behav. 2020, 10, e01760. [Google Scholar] [CrossRef]
- Okereke, O.I.; Reynolds, C.F., 3rd; Mischoulon, D.; Chang, G.; Vyas, C.M.; Cook, N.R.; Weinberg, A.; Bubes, V.; Copeland, T.; Friedenberg, G.; et al. Effect of Long-Term Vitamin D3 Supplementation vs. Placebo on Risk of Depression or Clinically Relevant Depressive Symptoms and on Change in Mood Scores: A Randomized Clinical Trial. JAMA 2020, 324, 471–480. [Google Scholar] [CrossRef]
- Choukri, M.A.; Conner, T.S.; Haszard, J.J.; Harper, M.J.; Houghton, L.A. Effect of Vitamin D Supplementation on Depressive Symptoms and Psychological Wellbeing in Healthy Adult Women: A Double-Blind Randomised Controlled Clinical Trial. J. Nutr. Sci. 2018, 7, e23. [Google Scholar] [CrossRef] [PubMed]
- Libuda, L.; Timmesfeld, N.; Antel, J.; Hirtz, R.; Bauer, J.; Führer, D.; Zwanziger, D.; Öztürk, D.; Langenbach, G.; Hahn, D.; et al. Effect of Vitamin D Deficiency on Depressive Symptoms in Child and Adolescent Psychiatric Patients: Results of a Randomized Controlled Trial. Eur. J. Nutr. 2020, 59, 3415–3424. [Google Scholar] [CrossRef] [PubMed]
- Mikola, T.; Marx, W.; Lane, M.M.; Hockey, M.; Loughman, A.; Rajapolvi, S.; Rocks, T.; O’Neil, A.; Mischoulon, D.; Valkonen-Korhonen, M.; et al. The Effect of Vitamin D Supplementation on Depressive Symptoms in Adults: A Systematic Review and Meta-analysis of Randomized Controlled Trials. Crit. Rev. Food Sci. Nutr. 2022, 371, 1–18. [Google Scholar] [CrossRef]


| Author, Year | Participants | Conclusions |
|---|---|---|
| Shin et al., 2016 [88] | 52,228 |
|
| Dogan-Sander et al., 2021 [107] | 7162 |
|
| Nerhus et al., 2016 [108] | 358 |
|
| Grudet et al., 2020 [24] | 102 |
|
| Grudet et al., 2014 [90] | 90 |
|
| Hashash et al., 2019 [106] | 1352 |
|
| Calderón-Espinoza et al., 2022 [91] | 72 |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Somoza-Moncada, M.M.; Turrubiates-Hernández, F.J.; Muñoz-Valle, J.F.; Gutiérrez-Brito, J.A.; Díaz-Pérez, S.A.; Aguayo-Arelis, A.; Hernández-Bello, J. Vitamin D in Depression: A Potential Bioactive Agent to Reduce Suicide and Suicide Attempt Risk. Nutrients 2023, 15, 1765. https://doi.org/10.3390/nu15071765
Somoza-Moncada MM, Turrubiates-Hernández FJ, Muñoz-Valle JF, Gutiérrez-Brito JA, Díaz-Pérez SA, Aguayo-Arelis A, Hernández-Bello J. Vitamin D in Depression: A Potential Bioactive Agent to Reduce Suicide and Suicide Attempt Risk. Nutrients. 2023; 15(7):1765. https://doi.org/10.3390/nu15071765
Chicago/Turabian StyleSomoza-Moncada, María Montserrat, Francisco Javier Turrubiates-Hernández, José Francisco Muñoz-Valle, Jesús Alberto Gutiérrez-Brito, Saúl Alberto Díaz-Pérez, Adriana Aguayo-Arelis, and Jorge Hernández-Bello. 2023. "Vitamin D in Depression: A Potential Bioactive Agent to Reduce Suicide and Suicide Attempt Risk" Nutrients 15, no. 7: 1765. https://doi.org/10.3390/nu15071765
APA StyleSomoza-Moncada, M. M., Turrubiates-Hernández, F. J., Muñoz-Valle, J. F., Gutiérrez-Brito, J. A., Díaz-Pérez, S. A., Aguayo-Arelis, A., & Hernández-Bello, J. (2023). Vitamin D in Depression: A Potential Bioactive Agent to Reduce Suicide and Suicide Attempt Risk. Nutrients, 15(7), 1765. https://doi.org/10.3390/nu15071765