
Factors Affecting the Vitamin C Dose-Concentration Relationship: Implications for Global Vitamin C Dietary Recommendations



Abstract
1. Introduction
2. Materials and Methods
2.1. The NHANES 2017–2018 Cohort
2.2. Demographic Information
2.3. Dietary Vitamin C Intakes
2.4. Serum Vitamin C Concentrations
2.5. Data Analyses
3. Results
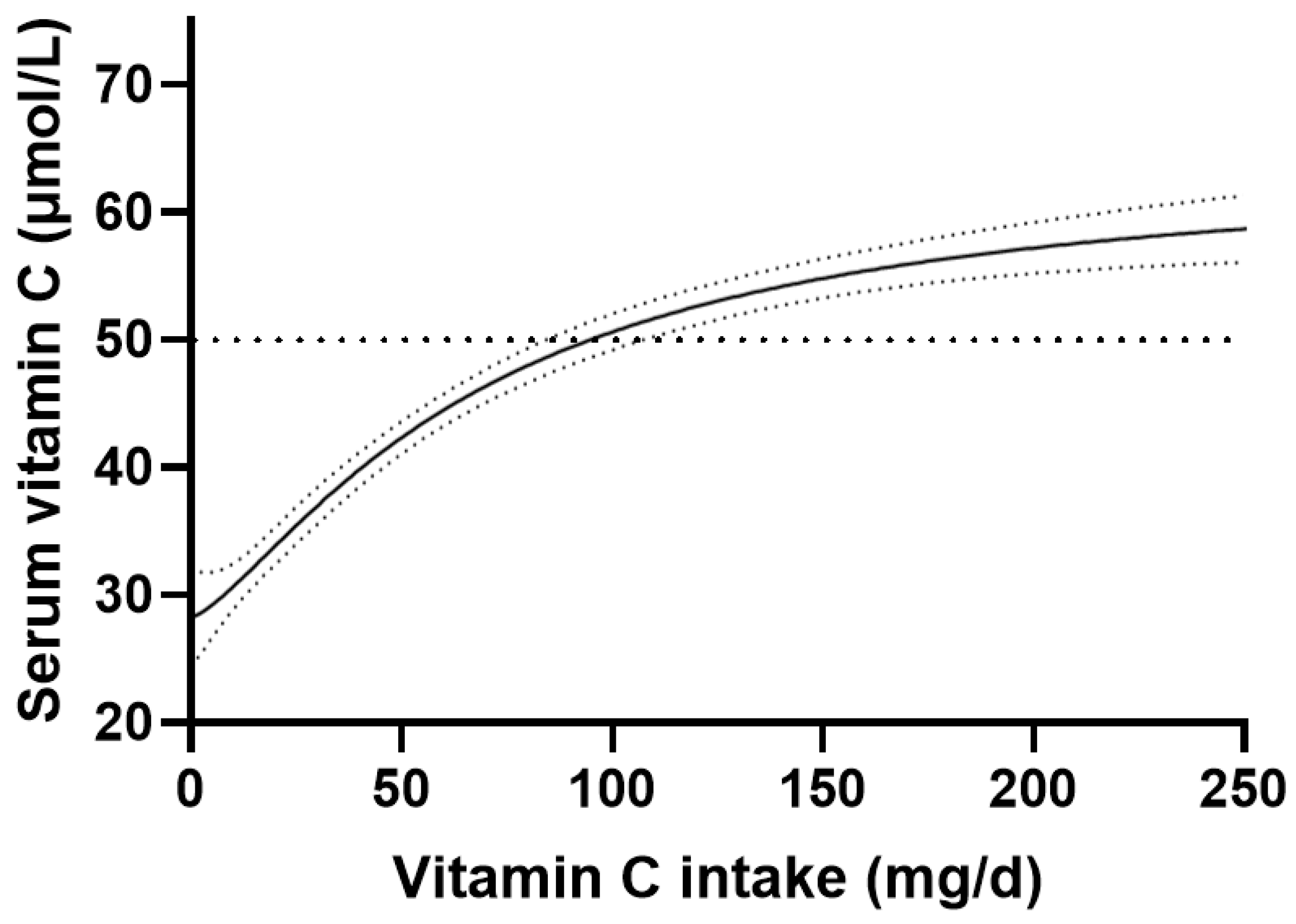
3.1. Vitamin C Dose-Concentration Relationship of the Total Cohort
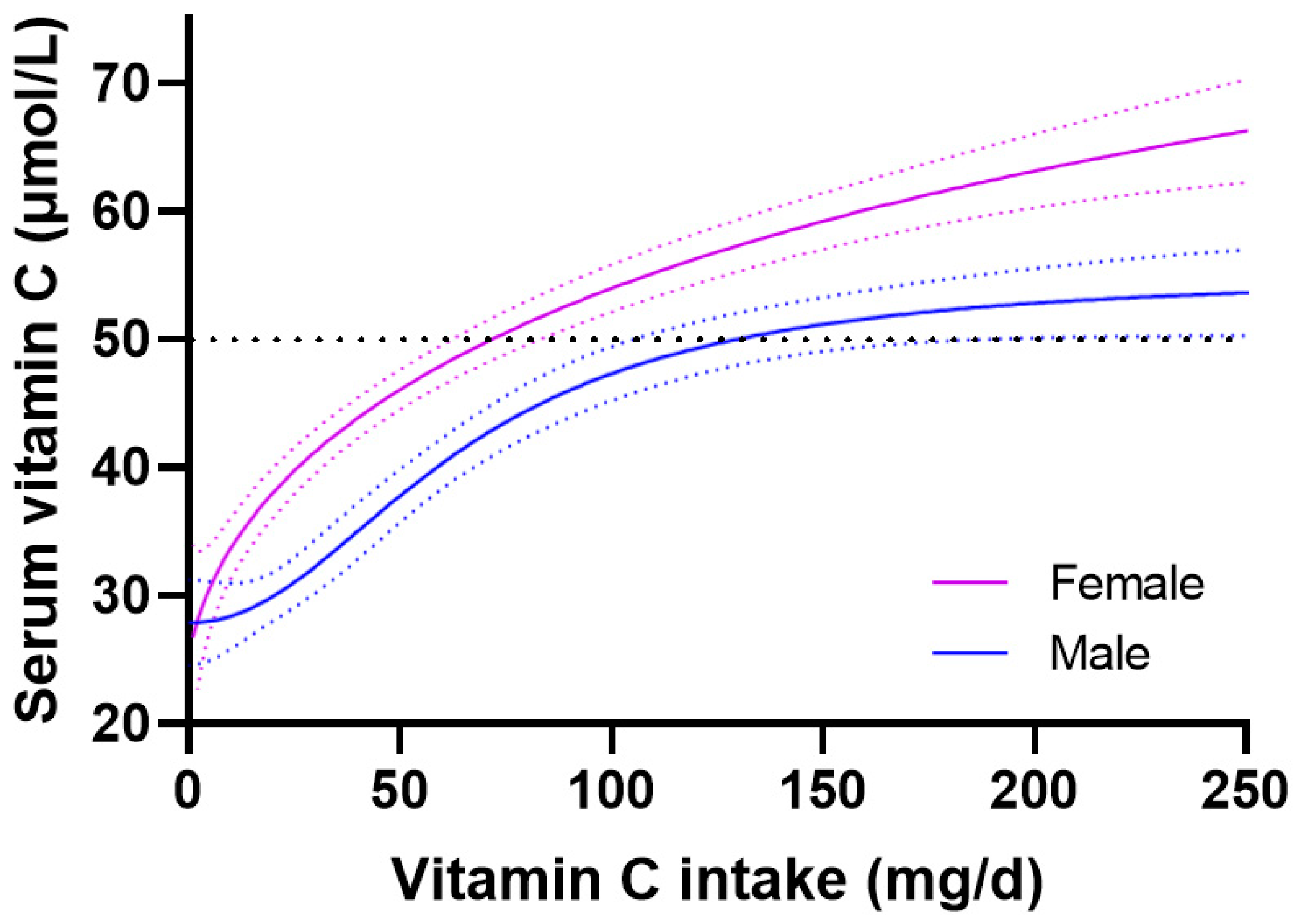
3.2. Vitamin C Dose-Concentration Relationship Relative to Gender
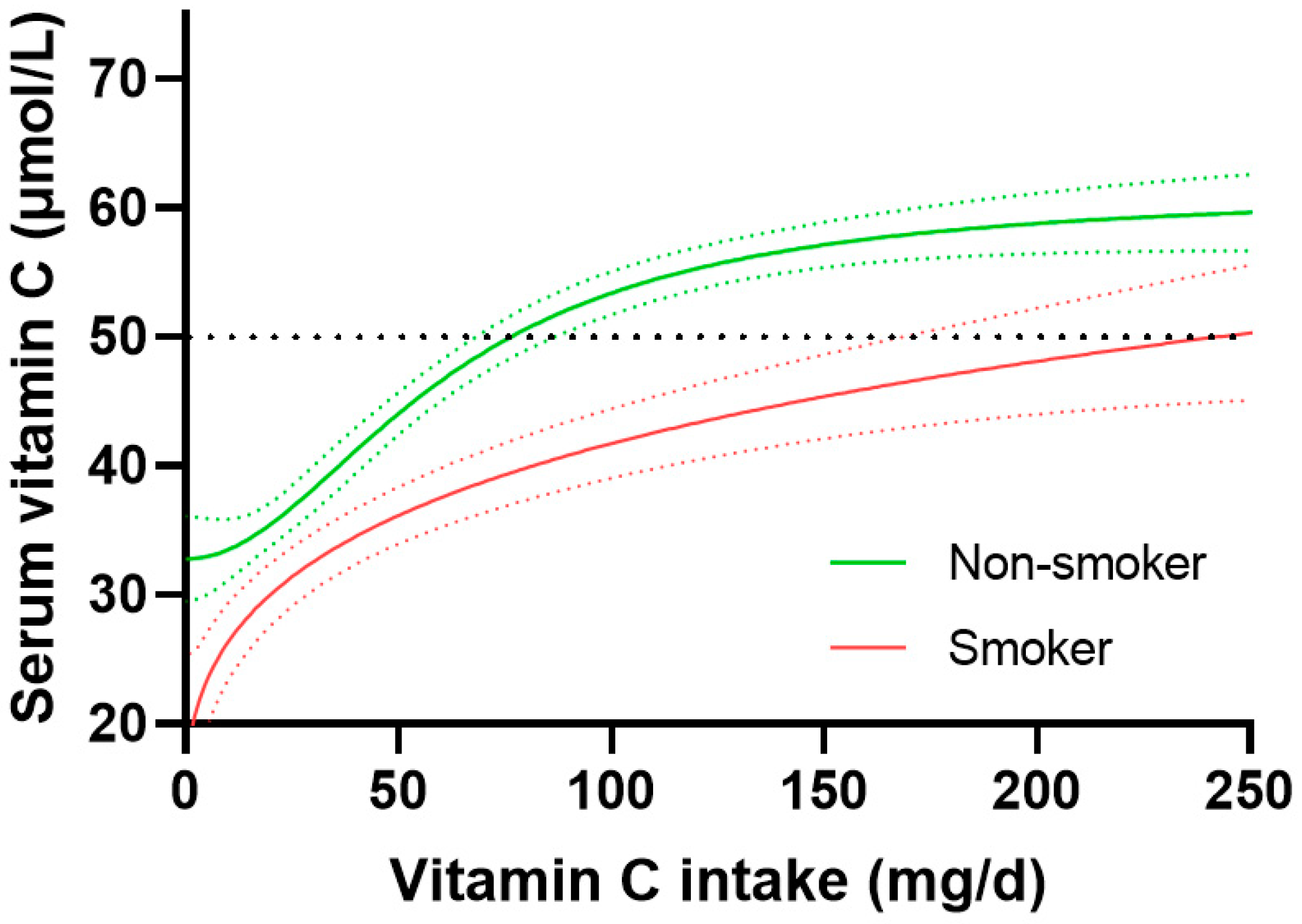
3.3. Vitamin C Dose-Concentration Relationship Relative to Smoking Status
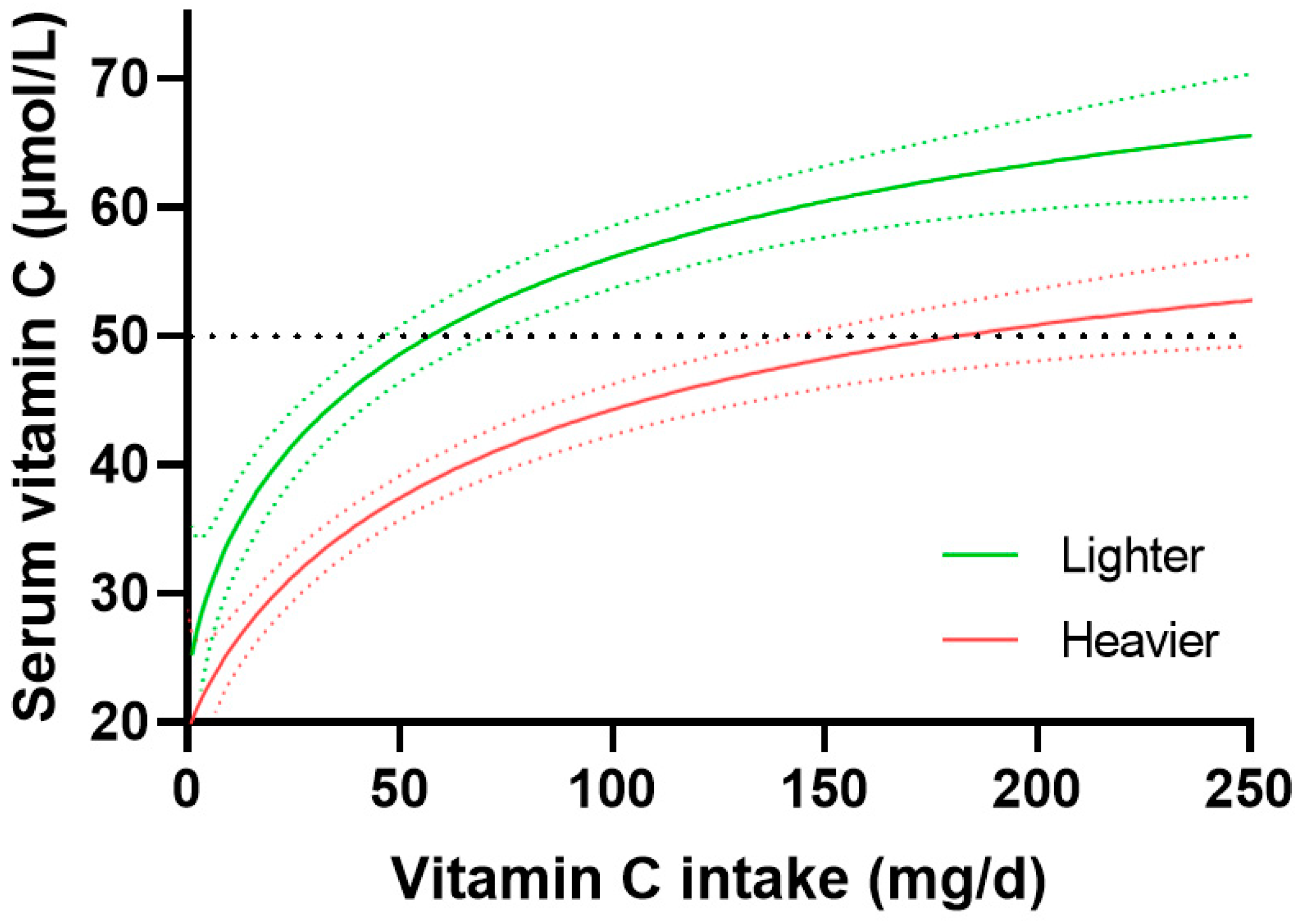
3.4. Vitamin C Dose-Concentration Relationship Relative to Body Weight
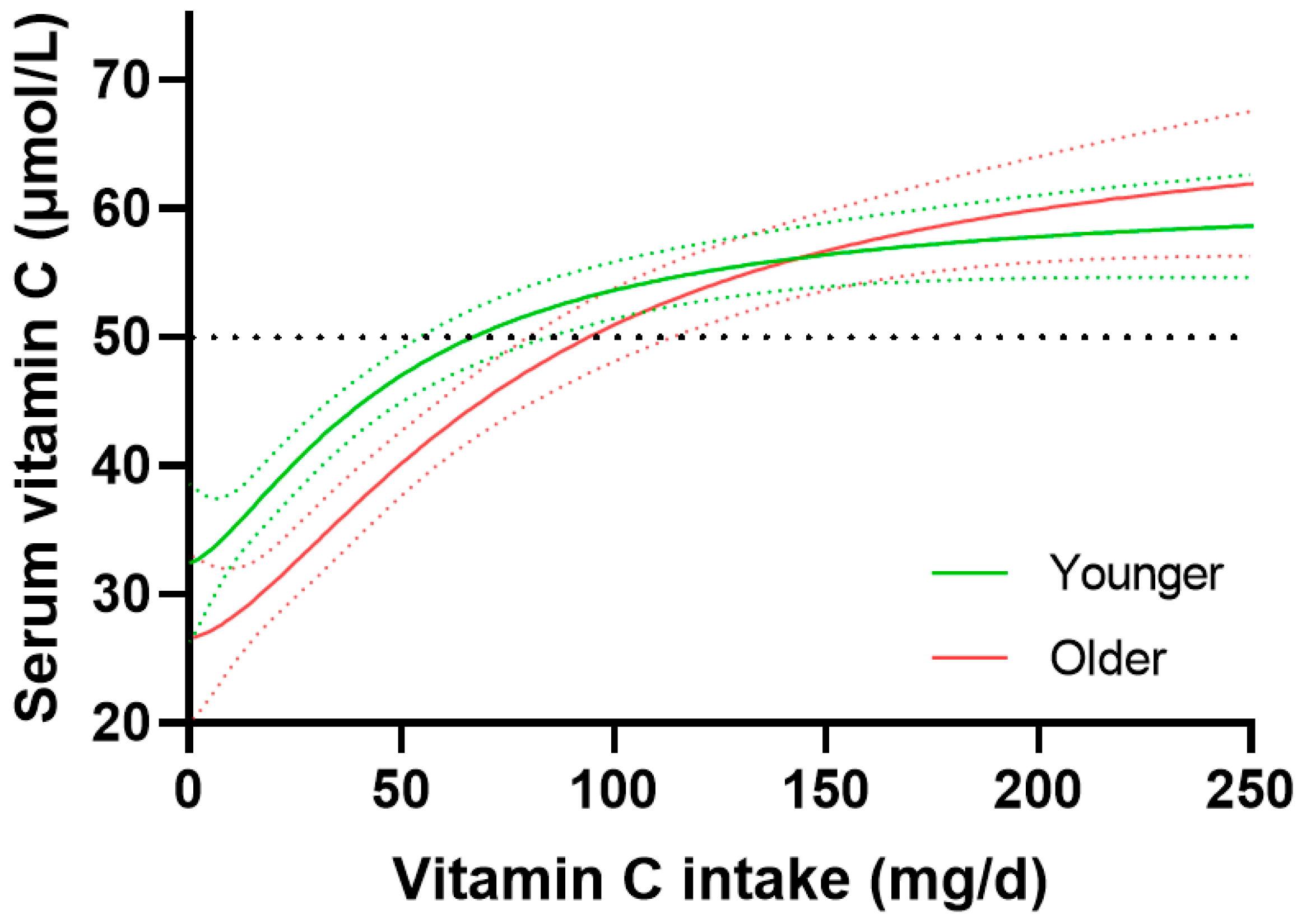
3.5. Vitamin C Dose-Concentration Relationship Relative to Age
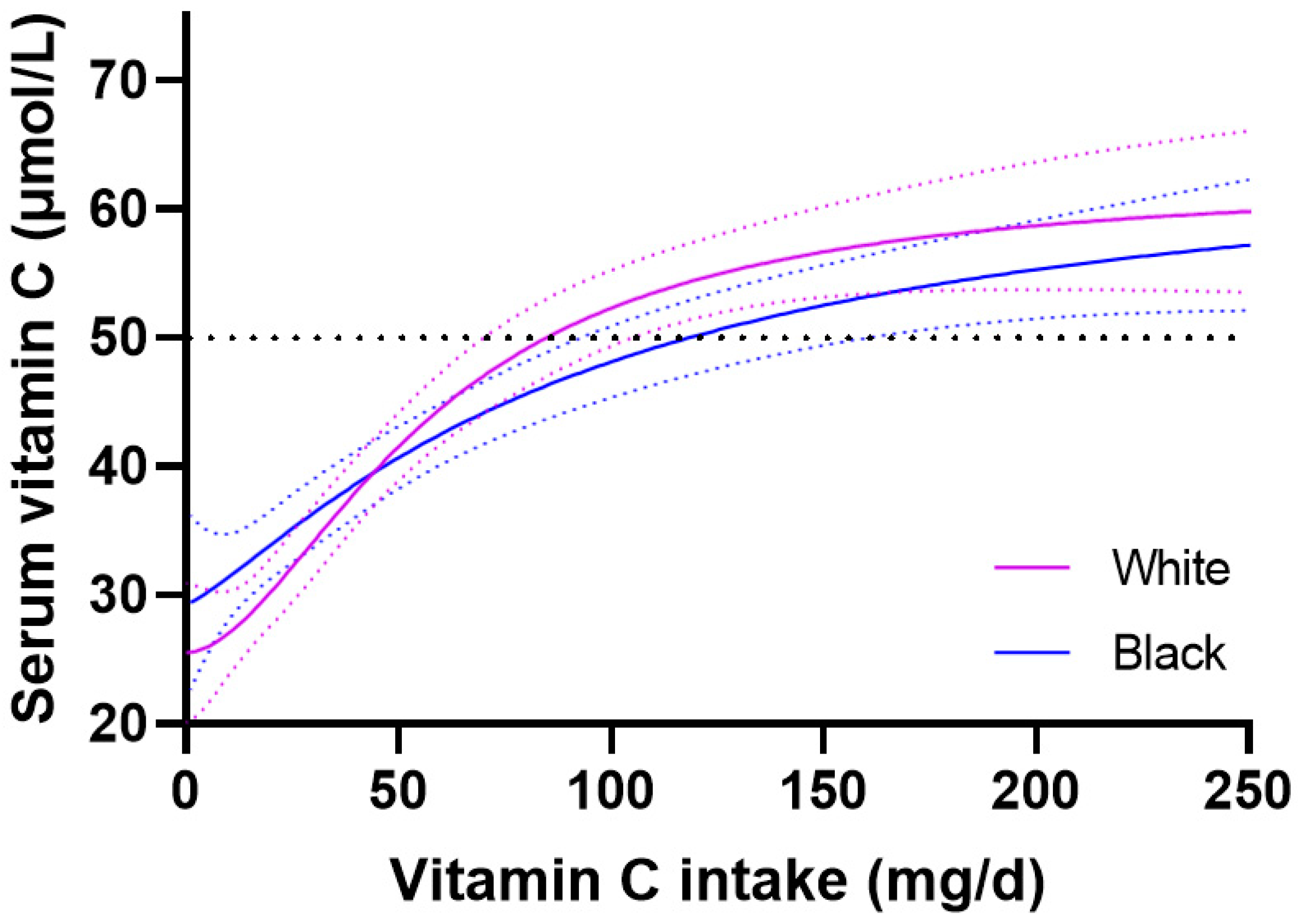
3.6. Vitamin C Dose-Response Relationship Relative to Ethnicity
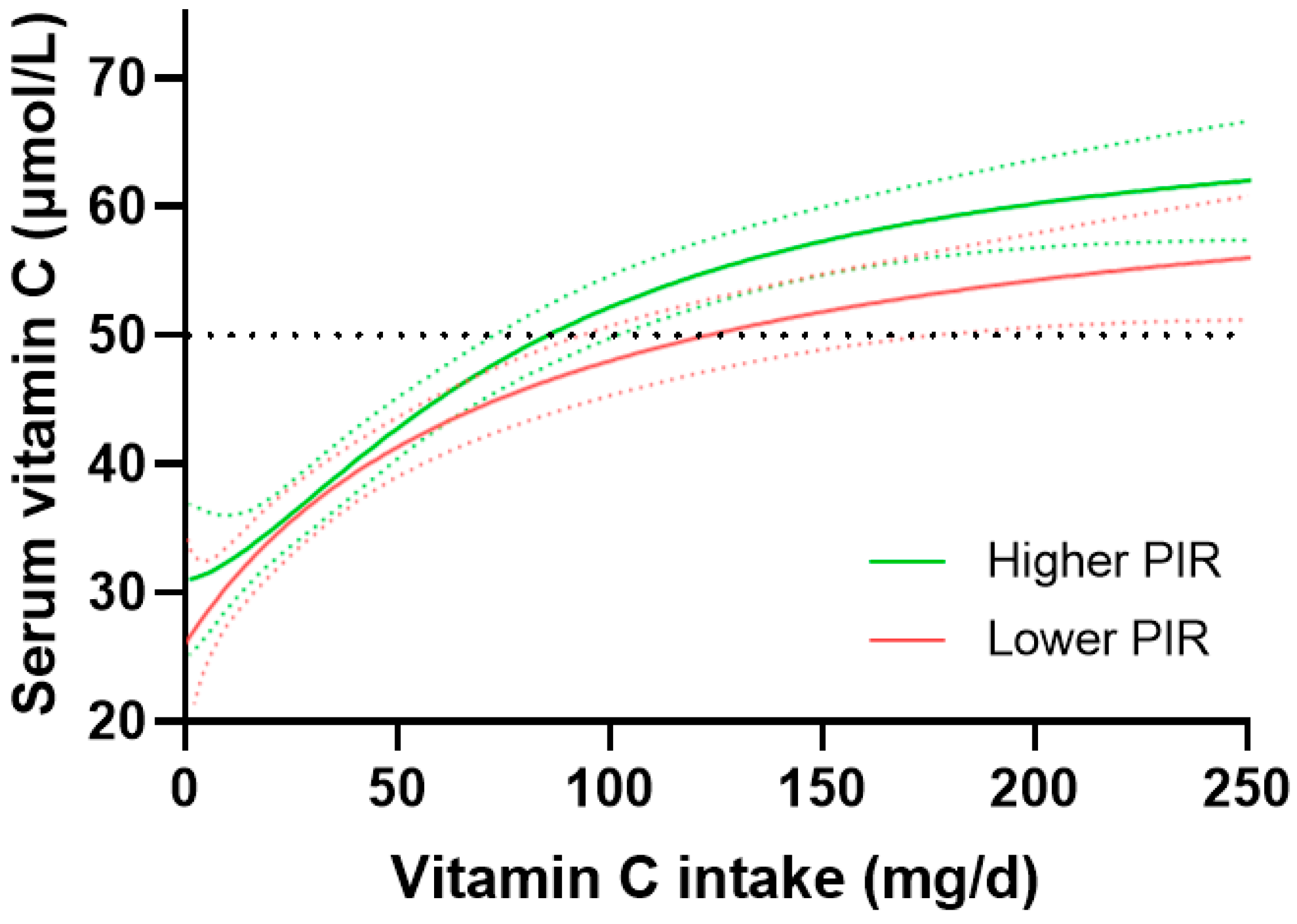
3.7. Vitamin C Dose-Response Relationship Relative to Socioeconomic Status
4. Discussion
4.1. Gender and Vitamin C Dose-Concentration Relationship
4.2. Smoking and Vitamin C Dose-Concentration Relationship
4.3. Weight and Vitamin C Dose-Concentration Relationship
4.4. Age and Vitamin C Dose-Concentration Relationship
4.5. Ethnicity and Vitamin C Dose-Concentration Relationship
4.6. Socioeconomic Status and Vitamin C Dose-Concentration Relationship
4.7. Study Limitations
4.8. Implications for Global Vitamin C Dietary Recommendations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Drouin, G.; Godin, J.R.; Pagé, B. The genetics of vitamin C loss in vertebrates. Curr. Genom. 2011, 12, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Maggini, S. Vitamin C and Immune Function. Nutrients 2017, 9, 1211. [Google Scholar] [CrossRef] [PubMed]
- Rowe, S.; Carr, A.C. Global vitamin C status and prevalence of deficiency: A cause for concern? Nutrients 2020, 12, 2008. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority Panel on Dietetic Products Nutrition and Allergies. Scientific opinion on dietary reference values for vitamin C. EFSA J. Eur. Food Saf. Auth. 2013, 11, 3418. [Google Scholar]
- Levine, M.; Conry-Cantilena, C.; Wang, Y.; Welch, R.W.; Washko, P.W.; Dhariwal, K.R.; Park, J.B.; Lazarev, A.; Graumlich, J.F.; King, J.; et al. Vitamin C pharmacokinetics in healthy volunteers: Evidence for a recommended dietary allowance. Proc. Natl. Acad. Sci. USA 1996, 93, 3704–3709. [Google Scholar] [CrossRef]
- Levine, M.; Wang, Y.; Padayatty, S.J.; Morrow, J. A new recommended dietary allowance of vitamin C for healthy young women. Proc. Natl. Acad. Sci. USA 2001, 98, 9842–9846. [Google Scholar] [CrossRef]
- Lykkesfeldt, J.; Tveden-Nyborg, P. The Pharmacokinetics of Vitamin C. Nutrients 2019, 11, 2412. [Google Scholar] [CrossRef]
- Lykkesfeldt, J.; Poulsen, H.E. Is vitamin C supplementation beneficial? Lessons learned from randomised controlled trials. Br. J. Nutr. 2010, 103, 1251–1259. [Google Scholar] [CrossRef]
- Carr, A.; Rowe, S. Factors Affecting Vitamin C Status and Prevalence of Deficiency: A Global Health Perspective. Nutrients 2020, 12, 1963. [Google Scholar] [CrossRef]
- Carr, A.C.; Zawari, M. Does aging have an impact on vitamin C status and requirements? Findings from comparative studies of aging and institutionalization. Nutrients 2023, 915. [Google Scholar] [CrossRef]
- Powers, C.D.; Sternberg, M.R.; Patel, S.B.; Pfeiffer, C.M.; Storandt, R.J.; Schleicher, R.L. Vitamin C status of US adults assessed as part of the National Health and Nutrition Examination Survey remained unchanged between 2003–2006 and 2017–2018. J. Appl. Lab. Med. 2023, 8, 272–284. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Lykkesfeldt, J. Does Aging Affect Vitamin C Status Relative to Intake? Findings from NHANES 2017–2018. Nutrients 2023, 15, 892. [Google Scholar] [CrossRef] [PubMed]
- Carr, A.C.; Block, G.; Lykkesfeldt, J. Estimation of Vitamin C Intake Requirements Based on Body Weight: Implications for Obesity. Nutrients 2022, 14, 1460. [Google Scholar] [CrossRef] [PubMed]
- Jungert, A.; Neuhäuser-Berthold, M. The lower vitamin C plasma concentrations in elderly men compared with elderly women can partly be attributed to a volumetric dilution effect due to differences in fat-free mass. Br. J. Nutr. 2015, 113, 859–864. [Google Scholar] [CrossRef]
- Lykkesfeldt, J.; Loft, S.; Nielsen, J.B.; E Poulsen, H. Ascorbic acid and dehydroascorbic acid as biomarkers of oxidative stress caused by smoking. Am. J. Clin. Nutr. 1997, 65, 959–963. [Google Scholar] [CrossRef]
- Lykkesfeldt, J.; Prieme, H.; Loft, S.; Poulsen, H.E. Effect of smoking cessation on plasma ascorbic acid concentration. BMJ 1996, 313, 91. [Google Scholar] [CrossRef] [PubMed]
- Kallner, A.B.; Hartmann, D.; Hornig, D.H. On the requirements of ascorbic acid in man: Steady-state turnover and body pool in smokers. Am. J. Clin. Nutr. 1981, 34, 1347–1355. [Google Scholar] [CrossRef]
- Lykkesfeldt, J.; Christen, S.; Wallock, L.M.; Chang, H.H.; A Jacob, R.; Ames, B.N. Ascorbate is depleted by smoking and repleted by moderate supplementation: A study in male smokers and nonsmokers with matched dietary antioxidant intakes. Am. J. Clin. Nutr. 2000, 71, 530–536. [Google Scholar] [CrossRef]
- Carr, A.C.; Lykkesfeldt, J. Discrepancies in global vitamin C recommendations: A review of RDA criteria and underlying health perspectives. Crit. Rev. Food Sci. Nutr. 2021, 61, 742–755. [Google Scholar] [CrossRef]
- Martin, A. Apports Nutritionnels Conseilles Pour la Population Francaise (Recommended Dietary Intakes for the French Population); Tec & Doc: Paris, France, 2001. [Google Scholar]
- GBD 2015 Obesity Collaborators. Health effects of overweight and obesity in 195 countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef]
- Carr, A.C.; Lykkesfeldt, J. Vitamin C. 2023. Available online: https://www.helsedirektoratet.no/horinger/nordic-nutrition-recommendations-2022-nnr2022 (accessed on 21 February 2023).
- National Center for Health Statistics. National Health and Nutrition Examination Survey: NHANES 2017–2018 USA: Centers for Disease Control and Prevention 2017–2018. Available online: https://www.cdc.gov/nchs/nhanes/index.htm (accessed on 10 November 2022).
- Pirkle, J.L. Laboratory Procedure Manual: Vitamin C (Ascorbic Acid) NHANES 2017–2018; CDC Environmental Health: Atlanta, GA, USA, 2020; p. 26.
- Schectman, G.; Byrd, J.C.; Gruchow, H.W. The influence of smoking on vitamin C status in adults. Am. J. Public Health 1989, 79, 158–162. [Google Scholar] [CrossRef] [PubMed]
- Lykkesfeldt, J.; Viscovich, M.; Poulsen, H.E. Ascorbic acid recycling in human erythrocytes is induced by smoking in vivo. Free Radic. Biol. Med. 2003, 35, 1439–1447. [Google Scholar] [CrossRef]
- Carr, A.; Frei, B. Does vitamin C act as a pro-oxidant under physiological conditions? FASEB J. 1999, 13, 1007–1024. [Google Scholar] [CrossRef] [PubMed]
- Block, G.; Mangels, A.R.; Patterson, B.H.; Levander, O.A.; Norkus, E.P.; Taylor, P.R. Body weight and prior depletion affect plasma ascorbate levels attained on identical vitamin C intake: A controlled-diet study. J. Am. Coll. Nutr. 1999, 18, 628–637. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Sánchez, A.; Madrigal-Santillán, E.; Bautista, M.; Esquivel-Soto, J.; Morales-González, Á.; Esquivel-Chirino, C.; Durante-Montiel, I.; Sánchez-Rivera, G.; Valadez-Vega, C.; Morales-González, J.A. Inflammation, oxidative stress, and obesity. Int. J. Mol. Sci. 2011, 12, 3117–3132. [Google Scholar] [CrossRef]
- Blanchard, J.; A Conrad, K.; Garry, P.J. Effects of age and intake on vitamin C disposition in females. Eur. J. Clin. Nutr. 1990, 44, 447–460. [Google Scholar]
- Blanchard, J.; A Conrad, K.; A Mead, R.; Garry, P.J. Vitamin C disposition in young and elderly men. Am. J. Clin. Nutr. 1990, 51, 837–845. [Google Scholar] [CrossRef]
- Prince, M.J.; Wu, F.; Guo, Y.; Robledo, L.M.G.; O’Donnell, M.; Sullivan, R.; Yusuf, S. The burden of disease in older people and implications for health policy and practice. Lancet 2015, 385, 549–562. [Google Scholar] [CrossRef]
- Corpe, C.P.; Tu, H.; Eck, P.; Wang, J.; Faulhaber-Walter, R.; Schnermann, J.; Margolis, S.; Padayatty, S.; Sun, H.; Wang, Y.; et al. Vitamin C transporter Slc23a1 links renal reabsorption, vitamin C tissue accumulation, and perinatal survival in mice. J. Clin. Investig. 2010, 120, 1069–1083. [Google Scholar] [CrossRef]
- Michels, A.J.; Hagen, T.M.; Frei, B. Human Genetic Variation Influences Vitamin C Homeostasis by Altering Vitamin C Transport and Antioxidant Enzyme Function. Annu. Rev. Nutr. 2013, 33, 45–70. [Google Scholar] [CrossRef]
- Schleicher, R.L.; Carroll, M.D.; Ford, E.S.; Lacher, D.A. Serum vitamin C and the prevalence of vitamin C deficiency in the United States: 2003–2004 National Health and Nutrition Examination Survey (NHANES). Am. J. Clin. Nutr. 2009, 90, 1252–1263. [Google Scholar] [CrossRef] [PubMed]
- McCall, S.J.; Clark, A.B.; Luben, R.N.; Wareham, N.J.; Khaw, K.T.; Myint, P.K. Plasma vitamin C levels: Risk factors for deficiency and association with self-reported functional health in the European Prospective Investigation into Cancer-Norfolk. Nutrients 2019, 11, 1552. [Google Scholar] [CrossRef] [PubMed]
- Pearson, J.F.; Pullar, J.M.; Wilson, R.; Spittlehouse, J.K.; Vissers, M.C.M.; Skidmore, P.M.L.; Willis, J.; Cameron, V.A.; Carr, A.C. Vitamin C Status Correlates with Markers of Metabolic and Cognitive Health in 50-Year-Olds: Findings of the CHALICE Cohort Study. Nutrients 2017, 9, 831. [Google Scholar] [CrossRef]
- Bates, C.J.; Prentice, A.; Cole, T.J.; van der Pols, J.C.; Doyle, W.; Finch, S.; Smithers, G.; Clarke, P.C. Micronutrients: Highlights and research challenges from the 1994–5 National Diet and Nutrition Survey of people aged 65 years and over. Br. J. Nutr. 1999, 82, 7–15. [Google Scholar] [CrossRef]
- Darmon, N.; Drewnowski, A. Contribution of food prices and diet cost to socioeconomic disparities in diet quality and health: A systematic review and analysis. Nutr. Rev. 2015, 73, 643–660. [Google Scholar] [CrossRef]
- Hiscock, R.; Bauld, L.; Amos, A.; Fidler, J.A.; Munafo, M. Socioeconomic status and smoking: A review. Ann. N. Y. Acad. Sci. 2012, 1248, 107–123. [Google Scholar] [CrossRef]
- German Nutrition Society. New Reference Values for Vitamin C Intake. Ann. Nutr. Metab. 2015, 67, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine Panel on Dietary Antioxidants and Related Compounds. Dietary Reference Intakes for Vitamin C, Vitamin E, Selenium, and Carotenoids; National Academies Press: Washington, DC, USA, 2000; 529p.
- Dietary Reference Values for Food Energy and Nutrients for the United Kingdom. Report of the Panel on Dietary Reference Values of the Committee on Medical Aspects of Food Policy. Rep. Health Soc. Subj. 1991, 41, 210. [Google Scholar]
- GBD 2015 Tobacco Collaborators. Smoking prevalence and attributable disease burden in 195 countries and territories, 1990–2015: A systematic analysis from the Global Burden of Disease Study 2015. Lancet 2017, 389, 1885–1906. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total Cohort (n = 2828) |
|---|---|
| Age, years | 48 (32, 62) |
| Sex, n (%): | |
| Male | 1425 (50) |
| Female | 1402 (50) |
| Ethnicity: | |
| Non-Hispanic white | 940 (33) |
| Non-Hispanic black | 728 (26) |
| Mexican American | 399 (14) |
| Non-Hispanic Asian | 328 (12) |
| Other Hispanic | 281 (10) |
| Other/multi-race | 152 (5) |
| Income to poverty ratio 1 | 2.0 (1.1, 3.8) |
| Current smoker | 681 (25) |
| Body weight, kg | 80 (68, 97) |
| Body Mass Index, kg/m2 | 29 (25, 34) |
| Vitamin C intake, mg/d | 53 (24, 102) |
| Serum vitamin C, µmol/L | 43 (23, 60) |
| Characteristics | Males (n = 1425) | Females (n = 1403) | p Value |
|---|---|---|---|
| Age, years | 48 (32, 63) | 47 (32, 61) | 0.3 |
| Sex, n (%): | |||
| Male | 1425 (100) | 0 (0) | |
| Female | 0 (0) | 1403 (100) | <0.0001 |
| Ethnicity: | |||
| Non-Hispanic white | 490 (34) | 450 (32) | |
| Non-Hispanic black | 354 (25) | 374 (27) | |
| Mexican American | 189 (13) | 209 (15) | |
| Non-Hispanic Asian | 168 (12) | 160 (11) | |
| Other Hispanic | 141 (10) | 141 (10) | |
| Other/multi-race | 83 (6) | 69 (5) | 0.5 |
| Income to poverty ratio | 2.0 (1.1, 3.9) | 1.9 (1.0, 3.7) | 0.06 |
| Current smoker | 413 (29) | 268 (19) | <0.0001 |
| Body weight, kg | 85 (73, 100) | 76 (63, 92) | <0.0001 |
| Body Mass Index, kg/m2 | 28 (25, 33) | 30 (25,36) | <0.0001 |
| Vitamin C intake, mg/d | 55 (24, 107) | 52 (25, 97) | 0.1 |
| Serum vitamin C, µmol/L | 39 (21, 55) | 47 (27, 64) | <0.0001 |
| Characteristics | Non-Smokers (n = 2068) | Smokers (n = 681) | p Value |
|---|---|---|---|
| Age, years | 49 (32, 63) | 43 (31, 58) | <0.0001 |
| Sex, n (%): | |||
| Male | 980 (47) | 413 (61) | |
| Female | 1080 (53) | 268 (39) | <0.0001 |
| Ethnicity: | |||
| Non-Hispanic white | 654 (32) | 275 (40) | |
| Non-Hispanic black | 472 (23) | 232 (34) | |
| Mexican American | 336 (16) | 51 (7) | |
| Non-Hispanic Asian | 278 (13) | 31 (5) | |
| Other Hispanic | 229 (11) | 39 (6) | |
| Other/multi-race | 53 (8) | 99 (5) | <0.0001 |
| Income to poverty ratio | 2.2 (1.2, 4.2) | 1.5 (0.8, 2.5) | <0.0001 |
| Current smoker | 0 (0) | 681 (100) | <0.0001 |
| Body weight, kg | 80 (68, 96) | 81 (69, 98) | 0.3 |
| Body Mass Index, kg/m2 | 29 (25, 34) | 28 (24, 34) | 0.001 |
| Vitamin C intake, mg/d | 58 (27, 106) | 41 (18, 84) | <0.0001 |
| Serum vitamin C, µmol/L | 45 (28, 62) | 30 (13, 53) | <0.0001 |
| Characteristics | Lighter Tertile (n = 932) | Middle Tertile (n = 943) | Heavier Tertile (n = 930) | p Value |
|---|---|---|---|---|
| Age, years | 46 (28, 63) | 50 (34, 62) | 47 (33, 61) | 0.006 |
| Sex, n (%): | ||||
| Male | 322 (35) | 531 (56) | 560 (60) | |
| Female | 610 (65) | 410 (43) | 370 (40) | <0.0001 |
| Ethnicity: | ||||
| Non-Hispanic white | 296 (32) | 276 (29) | 362 (39) | |
| Non-Hispanic black | 188 (20) | 240 (25) | 295 (32) | |
| Mexican American | 113 (12) | 161 (17) | 121 (13) | |
| Non-Hispanic Asian | 193 (21) | 104 (11) | 30 (3) | |
| Other Hispanic | 111 (12) | 107 (11) | 60 (6) | |
| Other/multi-race | 31 (3) | 55 (6) | 62 (7) | 0.04 |
| Income to poverty ratio | 2.0 (1.1, 3.9) | 2.0 (1.1, 3.9) | 2.0 (1.1, 3.7) | 0.7 |
| Current smoker | 212 (23) | 226 (24) | 238 (26) | 0.5 |
| Body weight, kg | 63 (57, 68) | 80 (76, 85) | 105 (97, 118) | <0.0001 |
| Body Mass Index, kg/m2 | 24 (21, 26) | 29 (27, 32) | 36 (33, 41) | <0.0001 |
| Vitamin C intake, mg/d | 56 (28, 106) | 54 (25, 100) | 49 (21, 97) | 0.01 |
| Serum vitamin C, µmol/L | 50 (28, 67) | 44 (26, 59) | 36 (19, 53) | <0.0001 |
| Characteristics | Younger Tertile (n = 942) | Middle Tertile (n = 942) | Older Tertile (n = 944) | p Value |
|---|---|---|---|---|
| Age, years | 26 (25, 32) | 48 (42, 53) | 66 (62, 73) | <0.0001 |
| Sex, n (%): | ||||
| Male | 475 (50) | 452 (48) | 498 (53) | |
| Female | 467 (50) | 490 (52) | 446 (47) | 0.1 |
| Ethnicity: | ||||
| Non-Hispanic white | 298 (32) | 281 (30) | 361 (38) | |
| Non-Hispanic black | 225 (24) | 235 (25) | 268 (28) | |
| Mexican American | 143 (15) | 149 (16) | 107 (11) | |
| Non-Hispanic Asian | 130 (14) | 133 (14) | 65 (7) | |
| Other Hispanic | 85 (9) | 89 (9) | 107 (11) | |
| Other/multi-race | 61 (6) | 55 (6) | 36 (4) | 0.06 |
| Income to poverty ratio | 1.8 (1.0, 3.4) | 2.0 (1.1, 4.1) | 2.1 (1.2, 3.8) | 0.0007 |
| Current smoker | 246 (27) | 269 (29) | 166 (18) | <0.0001 |
| Body weight, kg | 79 (66, 96) | 83 (70, 100) | 80 (69, 95) | <0.0001 |
| BMI, kg/m3 | 28 (23, 34) | 30 (26, 35) | 29 (26,34) | <0.0001 |
| Vitamin C intake, mg/d | 50 (22, 96) | 54 (25, 106) | 55 (27, 103) | 0.07 |
| Serum vitamin C, µmol/L | 48 (29, 63) | 40 (21, 57) | 41 (21, 49) | <0.0001 |
| Characteristics | Non-Hispanic White (n = 940) | Total Hispanic 1 (n = 680) | Non-Hispanic Black (n = 728) | p Value |
|---|---|---|---|---|
| Age, years | 49 (33, 66) | 47 (31, 61) | 51 (32, 62) | 0.002 |
| Sex, n (%): | ||||
| Male | 490 (52) | 330 (49) | 352 (49) | |
| Female | 450 (48) | 350 (51) | 374 (51) | 0.2 |
| Ethnicity: | ||||
| Non-Hispanic white | 940 (100) | 0 (0) | 0 (0) | |
| Non-Hispanic black | 0 (0) | 0 (0) | 728 (100) | |
| Total Hispanic | 0 (0) | 680 (100) | 0 (0) | <0.0001 |
| Income to poverty ratio | 2.1 (1.2, 4.2) | 1.6 (0.9, 2.9) | 1.7 (1.0, 3.3) | <0.0001 |
| Current smoker | 275 (30) | 90 (14) | 232 (33) | <0.0001 |
| Body weight, kg | 83 (69, 100) | 80 (69, 92) | 85 (72, 103) | <0.0001 |
| Body Mass Index, kg/m2 | 29 (25, 35) | 30 (27, 34) | 30 (25, 36) | 0.005 |
| Vitamin C intake, mg/d | 42 (21, 86) | 64 (31, 117) | 51 (23, 99) | <0.0001 |
| Serum vitamin C, µmol/L | 36 (17, 60) | 46 (32, 63) | 42 (22, 57) | <0.0001 |
| Characteristics | Higher PIR (n = 840) | Medium PIR (n = 843) | Lower PIR (n = 843) | p Value |
|---|---|---|---|---|
| Age, years | 49 (34, 62) | 49 (32, 64) | 44 (29, 60) | <0.0001 |
| Sex, n (%): | 432 (51) | |||
| Male | 408 (49) | 440 (52) | 398 (47) | |
| Female | 445 (53) | 350 (51) | 445 (53) | 0.09 |
| Ethnicity: | ||||
| Non-Hispanic white | 317 (38) | 311 (37) | 259 (31) | |
| Non-Hispanic black | 175 (21) | 199 (24) | 245 (29) | |
| Mexican Hispanic | 79 (9) | 128 (15) | 137 (16) | |
| Non-Hispanic Asian | 174 (21) | 79 (9) | 45 (5) | |
| Other Hispanic | 59 (7) | 77 (9) | 102 (12) | |
| Other/multi-race | 36 (4) | 49 (6) | 55 (7) | <0.0001 |
| Income to poverty ratio 1 | 4.8 (3.8, 5.0) | 2.0 (1.7, 2.4) | 0.9 (0.6, 1.1) | <0.0001 |
| Current smoker | 120 (15) | 194 (23) | 286 (35) | <0.0001 |
| Body weight, kg | 80 (69, 96) | 82 (69, 97) | 80 (67, 97) | 0.4 |
| Body Mass Index, kg/m2 | 28 (25, 33) | 29 (25, 35) | 29 (24, 35) | 0.08 |
| Vitamin C intake, mg/d | 61 (29, 111) | 53 (25, 95) | 49 (20, 100) | <0.0001 |
| Serum vitamin C, µmol/L | 45 (28, 61) | 43 (23, 60) | 40 (21, 58) | 0.0003 |
| Factor | Curve 1 Intake (mg/Day) 1 | Curve 2 Intake (mg/Day) | ∆ 95% CI Intake (mg/Day) 2 | Increased Requirement (Fold) |
|---|---|---|---|---|
| Total cohort | 93 (83, 107) | |||
| Females vs. males | 72 (63, 84) | 127 (102, 174) | 18 | 1.2 |
| Smoking status: | ||||
| Non-smokers vs. smokers | 76 (67, 85) | 236 (167, NA) | 82 | 2.0 |
| Weight tertiles: 2 | ||||
| Lighter vs. heavier | 56 (45, 70) | 177 (140, NA) | 70 | 2.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carr, A.C.; Lykkesfeldt, J. Factors Affecting the Vitamin C Dose-Concentration Relationship: Implications for Global Vitamin C Dietary Recommendations. Nutrients 2023, 15, 1657. https://doi.org/10.3390/nu15071657
Carr AC, Lykkesfeldt J. Factors Affecting the Vitamin C Dose-Concentration Relationship: Implications for Global Vitamin C Dietary Recommendations. Nutrients. 2023; 15(7):1657. https://doi.org/10.3390/nu15071657
Chicago/Turabian StyleCarr, Anitra C., and Jens Lykkesfeldt. 2023. "Factors Affecting the Vitamin C Dose-Concentration Relationship: Implications for Global Vitamin C Dietary Recommendations" Nutrients 15, no. 7: 1657. https://doi.org/10.3390/nu15071657
APA StyleCarr, A. C., & Lykkesfeldt, J. (2023). Factors Affecting the Vitamin C Dose-Concentration Relationship: Implications for Global Vitamin C Dietary Recommendations. Nutrients, 15(7), 1657. https://doi.org/10.3390/nu15071657