

A Low Daily Intake of Simple Sugars in the Diet Is Associated with Improved Liver Function in Cirrhotic Liver Transplant Candidates

 , , , , ,
, , , , ,
Abstract
1. Introduction
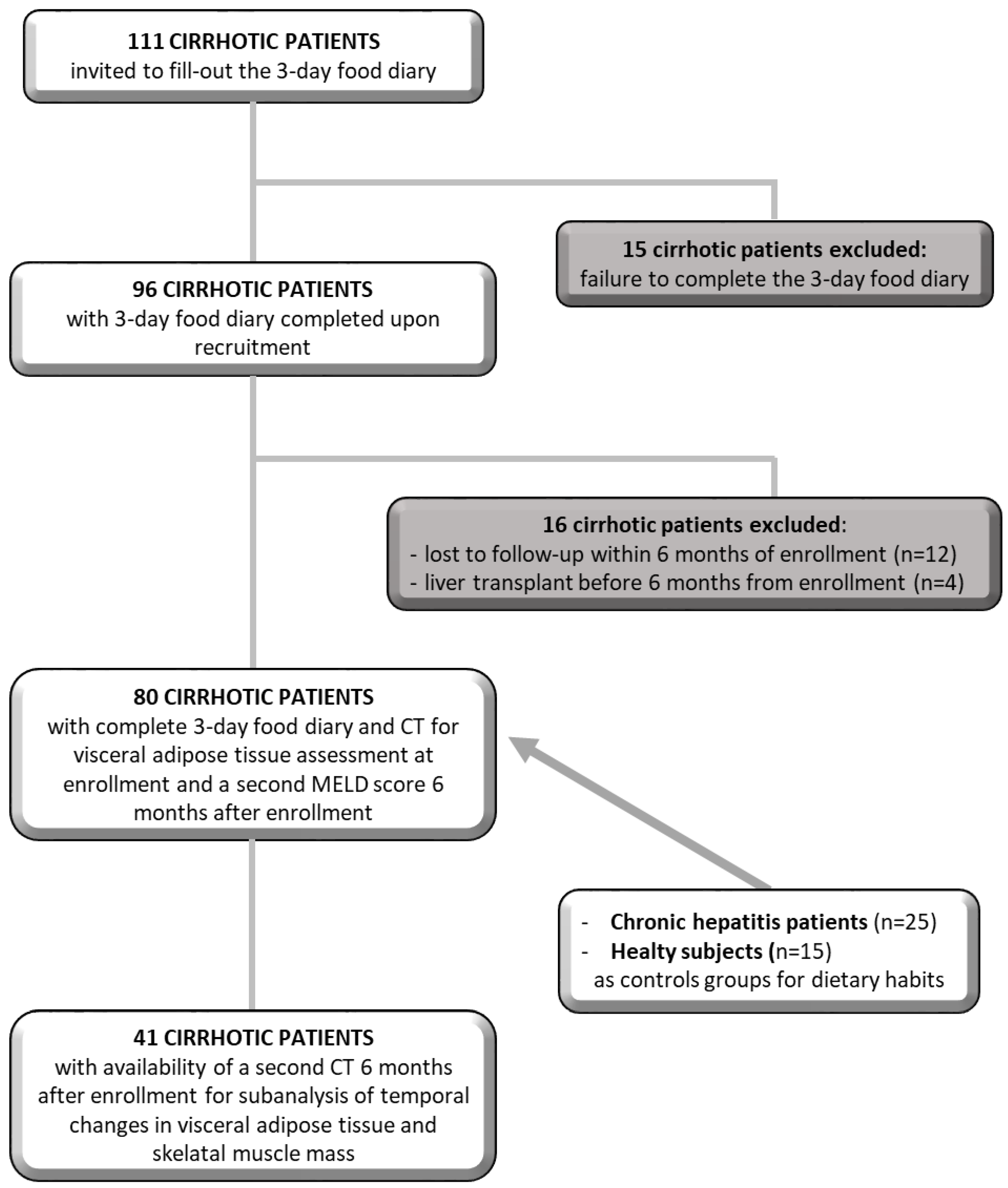
2. Materials and Methods
2.1. Anthropometric and Nutritional Assessment
2.2. Dietary Habits
2.3. DELTA-MELD Computation
2.4. Visceral Adipose Tissue and Skeletal Muscle Mass Evaluation
2.5. Statistical Analysis
3. Results
3.1. Dietary Nutrient Intake in Cirrhotic Patients Compared with That in Chronic Hepatitis Patients and Healthy Controls
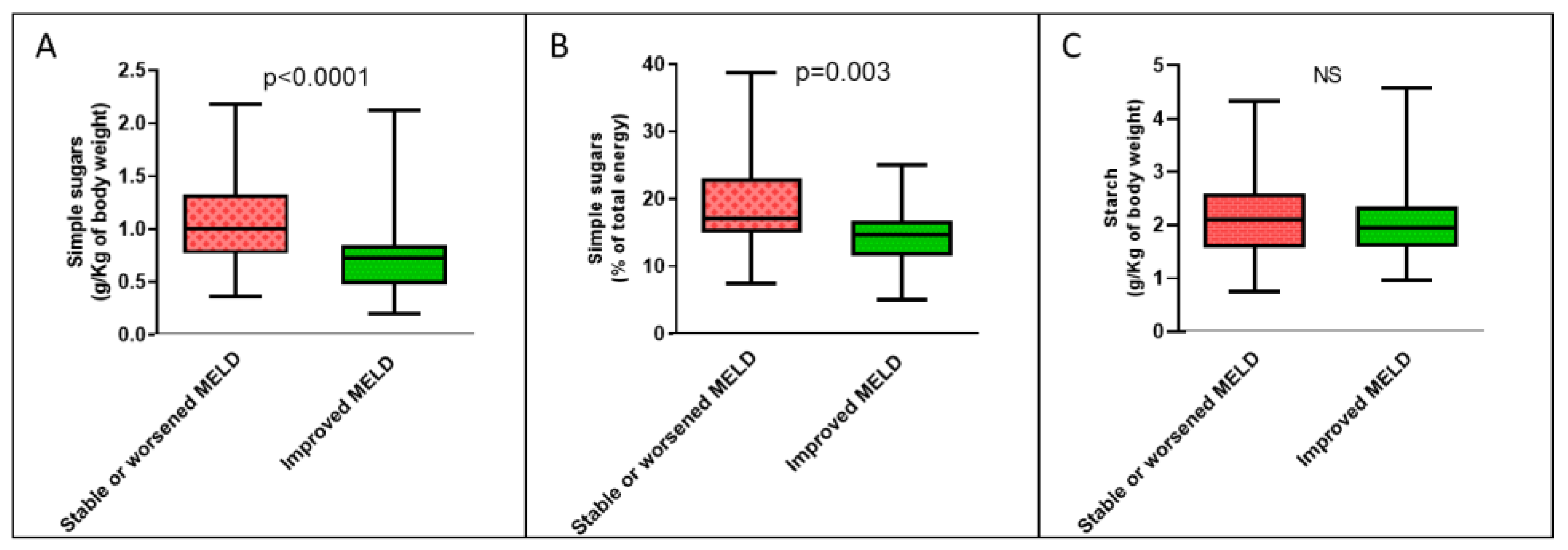
3.2. A Low Daily Intake of Simple Sugars in the Diet Is Associated with the Improvement of the MELD Score of Cirrhotic Patients over Time
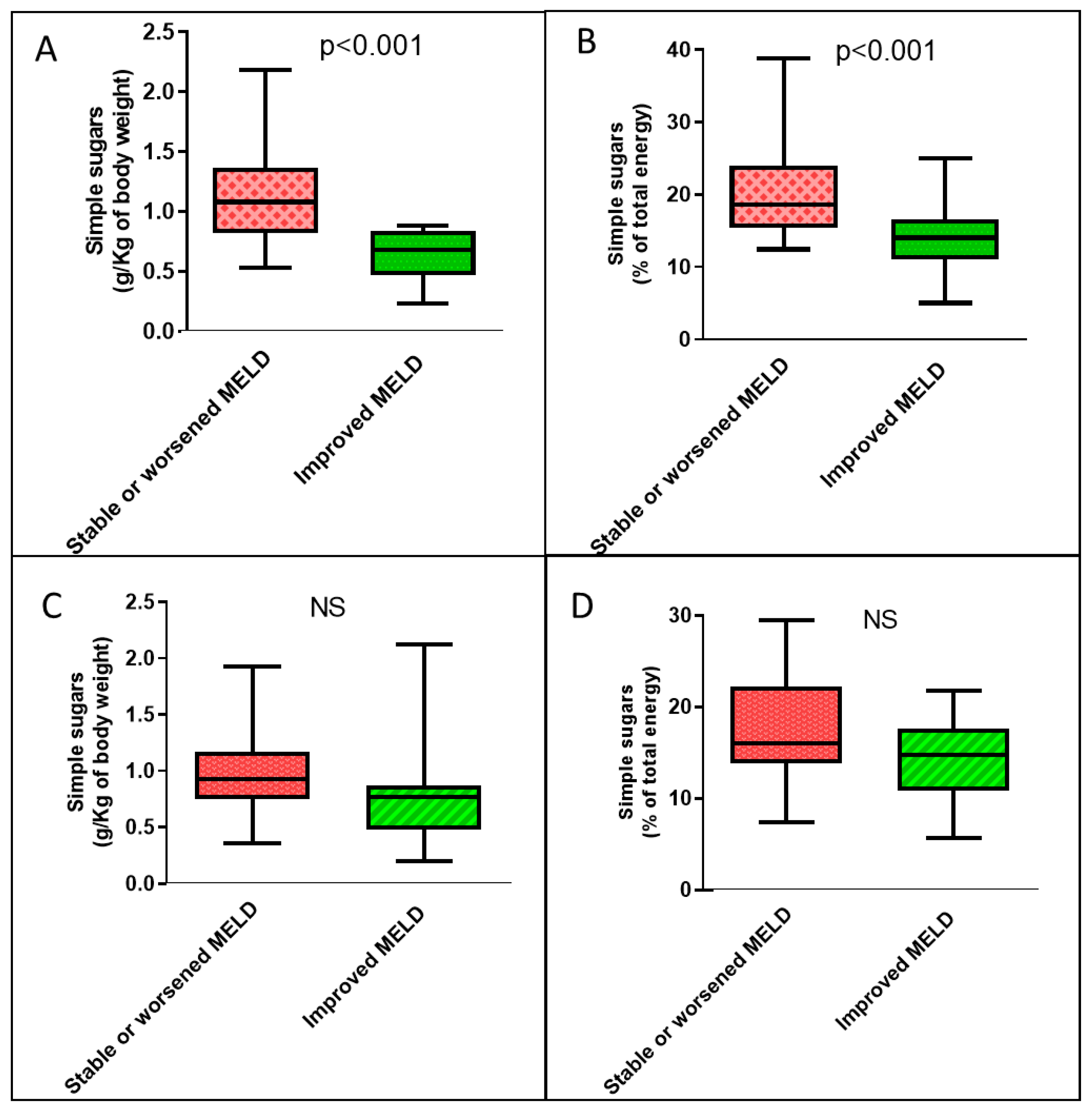
3.3. The Beneficial Effect of a Simple-Sugars-Restricted Diet on the MELD Score of Cirrhotic Patients Is More Pronounced in Patients with High Visceral Adipose Tissue
3.4. A Low Daily Intake of Simple Sugars in the Diet Is Associated with a Progressive Increase in the Ratio of Visceral Fat to Skeletal Muscle Mass in Cirrhotic Patients
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fang, K.; Yang, Q.; Lin, Y.; Zheng, L.; Wang, H.; Liang, W.J. Global cirrhosis prevalence trends and attributable risk factors—An ecological study using data from 1990–2019. Liver Int. 2022, 42, 2791–2799. [Google Scholar] [CrossRef]
- World Health Organization. 2023. Available online: https://www.who.int/data/global-health-estimates (accessed on 22 February 2023).
- Ye, F.; Zhai, M.; Long, J.; Gong, Y.; Ren, C.; Zhang, D.; Lin, X.; Liu, S. The burden of liver cirrhosis in mortality: Results from the global burden of disease study. Front. Public Health 2022, 11, 909455. [Google Scholar] [CrossRef]
- Kim, H.J.; Lee, H.W. Important predictor of mortality in patients with end-stage liver disease. Clin. Mol. Hepatol. 2013, 19, 105–115. [Google Scholar] [CrossRef]
- Györi, G.P.; Silberhumer, G.R.; Rahmel, A.; de Vries, E.; Soliman, T.; Zehetmayer, S.; Rogiers, X.; Berlakovich, G.A. Impact of dynamic changes in MELD score on survival after liver transplantation—A Eurotransplant registry analysis. Liver Int. 2016, 36, 1011–1017. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. EASL Clinical Practice Guidelines: Liver transplantation. J. Hepatol. 2016, 64, 433–485. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver. European Association for the Study of the Liver. EASL Clinical Practice Guidelines on nutrition in chronic liver disease. J. Hepatol. 2019, 70, 172–193. [Google Scholar] [CrossRef]
- Gheorghe, L.; Iacob, R.; Vãdan, R.; Iacob, S.; Gheorghe, C. High-protein high-calorie diet for hepatic encephalopathy Improvement of Hepatic Encephalopathy Using a Modified High-Calorie High-Protein Diet. Rom. J. Gastroenterol. 2005, 14, 231–238. [Google Scholar]
- Yoshida, T.; Muto, Y.; Moriwaki, H.; Yamato, M. Effect of long-term oral supplementation with branched-chain amino acid granules on the prognosis of liver cirrhosis. Gastroenterol. Jpn. 1989, 24, 692–698. [Google Scholar] [CrossRef]
- Morando, F.; Rosi, S.; Gola, E.; Nardi, M.; Piano, S.; Fasolato, S.; Stanco, M.; Cavallin, M.; Romano, A.; Sticca, A.; et al. Adherence to a moderate sodium restriction diet in outpatients with cirrhosis and ascites: A real-life cross-sectional study. Liver Int. 2015, 35, 1508–1515. [Google Scholar] [CrossRef]
- Bischoff, S.C.; Bernal, W.; Dasarathy, S.; Merli, M.; Plank, L.D.; Schütz, T.; Plauth, M. ESPEN practical guideline: Clinical nutrition in liver disease. Clin. Nutr. 2020, 39, 3533–3562. [Google Scholar] [CrossRef]
- Lai, J.C.; Tandon, P.; Bernal, W.; Tapper, E.B.; Ekong, U.; Dasarathy, S.; Carey, E.J. Malnutrition, Frailty, and Sarcopenia in Patients with Cirrhosis: 2021 Practice Guidance by the American Association for the Study of Liver Diseases. Hepatology 2021, 74, 1611–1644. [Google Scholar] [CrossRef]
- Puri, P.; Dhiman, R.K.; Taneja, S.; Tandon, P.; Merli, M.; Anand, A.C.; Arora, A.; Acharya, S.K.; Benjamin, J.; Chawla, Y.K.; et al. Nutrition in Chronic Liver Disease: Consensus Statement of the Indian National Association for Study of the Liver. J. Clin. Exp. Hepatol. 2021, 11, 97–143. [Google Scholar] [CrossRef]
- Bémeur, C.; Butterworth, R.F. Reprint of: Nutrition in the Management of Cirrhosis and its Neurological Complications. J. Clin. Exp. Hepatol. 2015, 5, S131–S140. [Google Scholar] [CrossRef]
- Palmese, F.; Bolondi, I.; Giannone, F.A.; Zaccherini, G.; Tufoni, M.; Baldassarre, M.; Caraceni, P. The Analysis of Food Intake in Patients with Cirrhosis Waiting for Liver Transplantation: A Neglected Step in the Nutritional Assessment. Nutrients 2019, 15, 2462. [Google Scholar] [CrossRef]
- Zelber-Sagi, S.; Ivancovsky-Wajcman, D.; Rabinowich, L.; Bentov, I.; Deutsch, L. Nutritional Evaluation and Treatment of the Cirrhotic Patient. Clin. Liver Dis. 2021, 25, 373–392. [Google Scholar] [CrossRef]
- Warner, E.R., II; Aloor, F.Z.; Satapathy, S.K. A narrative review of nutritional abnormalities, complications, and optimization in the cirrhotic patient. Transl. Gastroenterol. Hepatol. 2022, 7, 5. [Google Scholar] [CrossRef]
- World Health Organization. Guideline: Sugar Intake for Adults and Children; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Paik, J.M.; Golabi, P.; Younossi, Y.; Mishra, A.; Younossi, Z.M. Changes in the Global Burden of Chronic Liver Diseases From 2012 to 2017: The Growing Impact of NAFLD. Hepatology 2020, 72, 1605–1616. [Google Scholar] [CrossRef]
- Burra, P.; Becchetti, C.; Germani, G. NAFLD and liver transplantation: Disease burden, current management and future challenges. JHEP Rep. 2020, 2, 100192. [Google Scholar] [CrossRef]
- Eslam, M.; Sanyal, A.J.; George, J.; on behalf of the International Consensus Panel. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 1999.e1991–2014.e1991. [Google Scholar] [CrossRef]
- Gill, M.G.; Majumdar, A. Metabolic associated fatty liver disease: Addressing a new era in liver transplantation. World J. Hepatol. 2020, 12, 1168–1181. [Google Scholar] [CrossRef]
- Legaz, I.; Navarro-Noguera, E.; Bolarín, J.M.; García-Alonso, A.M.; Maldonado, A.L.; Mrowiec, A.; Campillo, J.A.; Gimeno, L.; Moya-Quiles, R.; Álvarez-López, M.D.R.; et al. Epidemiology, Evolution, and Long-Term Survival of Alcoholic Cirrhosis Patients Submitted to Liver Transplantation in Southeastern Spain. Alcohol. Clin. Exp. Res. 2016, 40, 794–805. [Google Scholar] [CrossRef]
- Haldar, D.; Kern, B.; Hodson, J.; Armstrong, M.J.; Adam, R.; Berlakovich, G.; Fritz, J.; Feurstein, B.; Popp, W.; Karam, V.; et al. Outcomes of liver transplantation for non-alcoholic steatohepatitis: A European Liver Transplant Registry study. J. Hepatol. 2019, 71, 313–322. [Google Scholar] [CrossRef]
- Muriel, P.; López-Sánchez, P.; Ramos-Tovar, E. Fructose and the Liver. Int. J. Mol. Sci. 2021, 22, 6969. [Google Scholar] [CrossRef]
- Coronati, M.; Baratta, F.; Pastori, D.; Ferro, D.; Angelico, F.; Del Ben, M. Added Fructose in Non-Alcoholic Fatty Liver Disease and in Metabolic Syndrome: A Narrative Review. Nutrients 2022, 14, 1127. [Google Scholar] [CrossRef]
- Geidl-Flueck, B.; Hochuli, M.; Németh, Á.; Eberl, A.; Derron, N.; Köfeler, H.C.; Tappy, L.; Berneis, K.; Spinas, G.A.; Gerber, P.A. Fructose- and sucrose- but not glucose-sweetened beverages promote hepatic de novo lipogenesis: A randomized controlled trial. J. Hepatol. 2021, 75, 46–54. [Google Scholar] [CrossRef]
- Alami, F.; Alizadeh, M.; Shateri, K. The effect of a fruit-rich diet on liver biomarkers, insulin resistance, and lipid profile in patients with non-alcoholic fatty liver disease: A randomized clinical trial. Scand. J. Gastroenterol. 2022, 57, 1238–1249. [Google Scholar] [CrossRef]
- Abdelmalek, M.F.; Suzuki, A.; Guy, C.; Unalp-Arida, A.; Colvin, R.; Johnson, R.J.; Diehl, A.M. Nonalcoholic Steatohepatitis Clinical Research Network. Increased fructose consumption is associated with fibrosis severity in patients with nonalcoholic fatty liver disease. Hepatology 2010, 51, 1961–1971. [Google Scholar] [CrossRef]
- Detsky, A.S.; McLaughlin, J.R.; Baker, J.P.; Johnston, N.; Whittaker, S.; Mendelson, R.A.; Jeejeebhoy, K.N. What is subjective global assessment of nutritional status? JPEN J. Parenter. Enter. Nutr. 1987, 11, 8–13. [Google Scholar] [CrossRef]
- Durnin, J.V.; Womersley, J. Body fat assessed from total body density and its estimation from skinfold thickness: Measurements on 481 men and women aged from 16 to 72 years. Br. J. Nutr. 1974, 32, 77–97. [Google Scholar] [CrossRef]
- Altomare, A.; Del Chierico, F.; Rocchi, G.; Emerenziani, S.; Nuglio, C.; Putignani, L.; Angeletti, S.; Presti, A.L.; Ciccozzi, M.; Russo, A.; et al. Association between Dietary Habits and Fecal Microbiota Composition in Irritable Bowel Syndrome Patients: A Pilot Study. Nutrients 2021, 13, 1479. [Google Scholar] [CrossRef]
- Fantuzzi, A.L.; Chiuchiù, M.; Bedogni, G. Atlante Fotografico delle Porzioni degli Alimenti; SICS: Milan, Italy, 2005. [Google Scholar]
- Ricerca Epidemiologia e Biostatistica. Available online: https://www.ieo.it/it/ricerca/aree-di-ricerca/Ricerca-Epidemiologia-Biostatistica1/ (accessed on 20 December 2022).
- Gianfredi, V.; Nucci, D.; Ceccarelli, F.; Villarini, M.; Moretti, M. PILATES (Physical Activity and Diet Survey): An Italian Self-Administered Questionnaire Evaluating Diet Habits of Gym-Goers. Validation Process. J. Diet. Suppl. 2019, 16, 307–317. [Google Scholar] [CrossRef]
- Società Italiana di Nutrizione Umana (SINU). LARN: Livelli di Assunzione di Riferimento di Nutrienti ed Energia, 4th ed.; SICS: Milan, Italy, 2014. [Google Scholar]
- O’Keefe, J.H.; Gheewala, N.M.; O’Keefe, J.O. Dietary Strategies for Improving Post-Prandial Glucose, Lipids, Inflammation, and Cardiovascular Health. J. Am. Coll. Cardiol. 2008, 51, 249–255. [Google Scholar] [CrossRef]
- Cariou, B. The metabolic triad of non-alcoholic fatty liver disease, visceral adiposity and type 2 diabetes: Implications for treatment. Diabetes Obes. Metab. 2022, 24 (Suppl. S2), 15–27. [Google Scholar] [CrossRef]
- Fan, Y.; Zhang, Y.; Chen, C.; Ying, Z.; Su, Q.; Li, X.; Chen, Y. Fasting serum fructose is associated with metabolic dysfunction-associated fatty liver disease: A prospective study. Hepatol. Res. 2023, 6, 1–10. [Google Scholar] [CrossRef]
- Srikureja, W.; Kyulo, N.L.; Runyon, B.A.; Hu, K.Q. MELD score is a better prognostic model than Child-Turcotte-Pugh score or Discriminant Function score in patients with alcoholic hepatitis. J. Hepatol. 2005, 42, 700–706. [Google Scholar] [CrossRef]
- Morales-Arráez, D.; Ventura-Cots, M.; Altamirano, J.; Abraldes, J.G.; Cruz-Lemini, M.; Thursz, M.R.; Atkinson, S.R.; Sarin, S.K.; Kim, W.; Chavez-Araujo, R.; et al. The MELD Score Is Superior to the Maddrey Discriminant Function Score to Predict Short-Term Mortality in Alcohol-Associated Hepatitis: A Global Study. Am. J. Gastroenterol. 2022, 117, 301–310. [Google Scholar] [CrossRef]
- Sheth, M.; Riggs, M.; Patel, T. Utility of the Mayo End-Stage Liver Disease (MELD) score in assessing prognosis of patients with alcoholic hepatitis. BMC Gastroenterol. 2002, 22, 2. [Google Scholar] [CrossRef]
- Wang, M.; Chen, W.; Zhang, J.; Gobejishvili, L.; Barve, S.S.; McClain, C.J.; Joshi-Barve, S. Elevated Fructose and Uric Acid Through Aldose Reductase Contribute to Experimental and Human Alcoholic Liver Disease. Hepatology 2020, 72, 1617–1637. [Google Scholar] [CrossRef]
- Brown, K.E.; A Broadhurst, K.; Mathahs, M.M.; Kladney, R.D.; Fimmel, C.J.; Srivastava, S.K.; Brunt, E.M. Immunodetection of aldose reductase in normal and diseased human liver. Histol. Histopathol. 2005, 20, 429–436. [Google Scholar] [CrossRef]
- Afzali, A.; Weiss, N.S.; Boyko, E.J.; Ioannou, G.N. Association between serum uric acid level and chronic liver disease in the United States. Hepatology 2010, 52, 578–589. [Google Scholar] [CrossRef]
- Georgiou, A.; Yannakoulia, M.; Papatheodoridis, G.V.; Deutsch, M.; Alexopoulou, A.; Vlachogiannakos, J.; Ioannidou, P.; Papageorgiou, M.-V.; Voulgaris, T.; Papadopoulos, N.; et al. Assessment of dietary habits and the adequacy of dietary intake of patients with cirrhosis-the KIRRHOS study. Clin. Nutr. 2021, 40, 3992–3998. [Google Scholar] [CrossRef]
- Buscail, C.; Bourcier, V.; Fezeu, L.K.; Roulot, D.; Brulé, S.; Ben-Abdesselam, Z.; Cagnot, C.; Hercberg, S.; Nahon, P.; Ganne-Carrié, N.; et al. Eating Patterns in Patients with Compensated Cirrhosis: A Case-Control Study. Nutrients 2018, 10, 60. [Google Scholar] [CrossRef]
- Schulte-Frohlinde, E.; Wagenpfeil, S.; Willis, J.; Lersch, C.; Eckel, F.; Schmid, R.; Schusdziarra, V. Role of meal carbohydrate content for the imbalance of plasma amino acids in patients with liver cirrhosis. J. Gastroenterol. Hepatol. 2007, 22, 1241–1248. [Google Scholar] [CrossRef]
- Ha, N.B.; Fan, B.; Shui, A.M.; Huang, C.Y.; Brandman, D.; Lai, J.C. CT-quantified sarcopenic visceral obesity is associated with poor transplant waitlist mortality in patients with cirrhosis. Liver Transplant. 2023, 3. [Google Scholar] [CrossRef]
- Shida, T.; Oshida, N.; Oh, S.; Okada, K.; Shoda, J. Progressive reduction in skeletal muscle mass to visceral fat area ratio is associated with a worsening of the hepatic conditions of non-alcoholic fatty liver disease. Diabetes Metab Syndr Obes. 2019, 12, 495–503. [Google Scholar] [CrossRef]
- Shida, T.; Akiyama, K.; Oh, S.; Sawai, A.; Isobe, T.; Okamoto, Y.; Ishige, K.; Mizokami, Y.; Yamagata, K.; Onizawa, K.; et al. Skeletal muscle mass to visceral fat area ratio is an important determinant affecting hepatic conditions of non-alcoholic fatty liver disease. J. Gastroenterol. 2018, 53, 535–547. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Cirrhotic Patients (n = 80) | Chronic Hepatitis Patients (n = 25) | Healthy Controls (n = 15) | p-Value Cirrhotic vs. Chronic Hepatitis Patients | p-Value Cirrhotic Patients vs. Healthy Controls | |
|---|---|---|---|---|---|
| Age in years, median (IQR) | 59.5 (53.3–63.0) | 59.0 (52.6–70.8) | 58.0 (51.0–63.0) | 0.158 | 0.810 |
| Gender, M (%) | 70 (87.5) | 17 (68.0) | 12 (80) | 0.024 | 0.426 |
| BMI (kg/m2), median (IQR) | 27.5 (24.6–31.3) | 24.6(23.3–27.6) | 24.9 (23.2–27.0) | 0.006 | 0.017 |
| Overweight/Obesity, n (%) | 59 (73.8) | 11 (44.0) | 7 (46.7) | 0.006 | 0.037 |
| Diabetes, n (%) | 21 (26.3) | 0 (0) | 0 (0) | <0.001 | <0.001 |
| Dyslipidemia, n (%) | 13 (16.3) | 0 (0) | 0 (0) | <0.001 | <0.001 |
| Arterial hypertension, n (%) | 19 (23.8) | 0 (0) | 0 (0) | <0.001 | <0.001 |
| Nutritional assessment: | |||||
| 73 (91.3) | 25 (100) | 15 (100) | 0.491 | 0.650 |
| 6 (7.5) | 0 (0) | 0 (0) | ||
| 1 (1.3) | 0 (0) | 0 (0) | ||
| MAC (cm), median (IQR) | 30.0 (27.0–35.0) | 29.3 (28.0–31.9) | 32.0 (30.0–34.0) | 0.582 | 0.417 |
| Triceps skinfold measurements (mm), median (IQR) | 13.6 (7.7–20.1) | 13.6 (11.8–15.9) | 9.9 (7.5–14.9) | 0.972 | 0.111 |
| Energy (Kcal/Kg/day), median (IQR) | 20.8 (17.3–27.1) | 23.5 (17.7–28.9) | 25.8 (24.5–33.5) | 0.232 | 0.005 |
| Proteins dietary daily intake (g/Kg of body weight), median (IQR) | 0.86 (0.66–1.11) | 0.94 (0.78–1.12) | 1.08 (0.86–1.41) | 0.254 | 0.017 |
| Fats dietary daily intake (g/Kg of body weight), median (IQR) | 0.73 (0.56–1.06) | 0.95 (0.66–1.14) | 1.06 (0.81–1.29) | 0.062 | 0.002 |
| Carbohydrates dietary daily intake (g/Kg of body weight), median (IQR) | 2.91 (2.24–3.68) | 2.96 (2.33–3.53) | 3.10 (2.64–3.80) | 0.897 | 0.401 |
| Starch dietary daily intake (g/Kg of body weight), median (IQR) | 2.04 (1.60–2.45) | 2.00 (1.57–2.28) | 2.11 (1.54–2.70) | 0.518 | 0.713 |
| Simple sugars dietary daily intake (g/Kg of body weight), median (IQR) | 0.84 (0.66–1.16) | 0.92 (0.63–1.15) | 0.99 (0.68–1.30) | 0.712 | 0.307 |
| Simple sugars dietary daily intake (% of total energy), median (IQR) | 16.2 (13.5–21.2) | 15.5 (12.1–20.9) | 15.5 (10.6–20.4) | 0.685 | 0.358 |
| Vegetables (servings/day), median (IQR) | 1.24 (0.71–1.90) | 0.58 (0.32–1.08) | 0.63 (0.42–1.10) | 0.002 | 0.016 |
| Fruit (servings/day), median (IQR) | 1.56 (0.83–2.33) | 1.49 (0.72–2.24) | 0.47 (0.23–1.87) | 0.741 | 0.011 |
| Sum of added sugar, jam, and honey (servings/day), median (IQR) | 0.67 (0.00–1.66) | 0.67 (0.00–1.33) | 0.33 (0.00–1.07) | 0.988 | 0.813 |
| Milk and yogurt (servings/day), median (IQR) | 0.80 (0.00–1.50) | 1.66 (0.55–2.17) | 1.07 (0.33–2.00) | 0.009 | 0.490 |
| Soft drinks (servings/day), median (IQR) | 0.00 (0.00–0.18) | 0.00 (0.00–0.00) | 0.00 (0.00–0.25) | 0.011 | 0.861 |
| Fruit juice (servings/day), median (IQR) | 0.00 (0.00–0.33) | 0.00 (0.00–0.00) | 0.00 (0.00–0.33) | 0.020 | 0.564 |
| Sugary sweets (servings/day), median (IQR) | 0.53 (0.11–1.00) | 0.33 (0.00–1.07) | 1.13 (0.33–1.47) | 0.578 | 0.029 |
| Stable or Worsened MELD Score (n = 51) | Improved MELD Score (n = 29) | p-Value | |
|---|---|---|---|
| Age in years, median (IQR) | 60.0 (56.0–63.0) | 59.0 (51.0–62.5) | 0.170 |
| Gender, M (%) | 47 (92.2) | 23 (79.3) | 0.157 |
| BMI, kg/m2, median (IQR) | 27.6 (24.1–31.5) | 27.4 (25.3–30.7) | 0.964 |
| Overweight/Obesity, n (%) | 36 (70.6) | 23 (79.3) | 0.394 |
| Diabetes, n (%) | 14 (27.5) | 7 (24.1) | 0.746 |
| Dyslipidemia, n (%) | 9 (17.6) | 4 (13.8) | 0.760 |
| Arterial hypertension, n (%) | 16 (31.4) | 3 (10.3) | 0.054 |
| Cirrhosis etiology: | |||
| 24 (47.1) | 14 (48.3) | 0.917 |
| 25 (49) | 18 (62.1) | 0.260 |
| 41 (80.4) | 25 (86.2) | 0.760 |
| HCC, yes (%) | 24 (47.1) | 11 (37.9) | 0.429 |
| Ascites, n (%) | 22 (43.1) | 11 (37.9) | 0.649 |
| Serum AST, UI/L, median (IQR) | 44.0 (32.0–77.0) | 49.0 (33.5–69.0) | 0.741 |
| Serum ALT, UI/L, median (IQR) | 34.0 (20.0–62.0) | 31.0 (20.5–43.5) | 0.814 |
| MELD at baseline, median (IQR) | 12.6 (10.0–14.8) | 12.0 (11.0–14.9) | 0.864 |
| MELD after 6 months, median (IQR) | 15.0 (12.0–19.0) | 11.0 (9.0–13.0) | <0.001 |
| Δ-MELD, median (IQR) | 1.54 (0.39–3.19) | −0.80 (–2.36–−0.39) | <0.001 |
| Charlson modified comorbidity index: | |||
| 20 (39.2) | 17 (58.6) | 0.229 |
| 25 (49) | 9 (31) | |
| 6 (11.8) | 3 (10.3) | |
| Nutritional assessment: | |||
| 47 (92.2) | 26 (89.7) | 0.585 |
| 3 (5.9) | 3 (10.3) | |
| 1 (2) | 0 (0) | |
| MAC (cm), median (IQR) | 30.0 (27.0–33.0) | 31.0 (27.0–36.0) | 0.868 |
| Triceps skinfold measurements (mm), median (IQR) | 13.8 (8.8–20.0) | 11.8 (6.4–20.2) | 0.386 |
| VATI (cm2/m2), median (IQR) | 38.1 (30.5–54.5) | 41.1 (30.1–46.6) | 0.572 |
| Stable or Worsened MELD Score (n = 51) | Improved MELD Score (n = 29) | p-Values | |
|---|---|---|---|
| Daily servings of the sum of added sugar, jam, and honey, median (IQR) | 1.0 (0.00–2.0) | 0.0(0.0–1.0) | 0.002 |
| Daily servings of fruit, median (IQR) | 1.60 (1.0–2.55) | 1.46 (0.60–1.80) | 0.118 |
| Daily servings of added sugar, jam, honey, and fruit, median (IQR) | 2.91 (2.06–3.97) | 1.66 (0.76–2.80) | 0.002 |
| Daily servings of sugary sweets, median (IQR) | 0.67 (0.33–1.06) | 0.27 (0.00–0.61) | 0.005 |
| Daily servings of added sugar, jam, honey, fruit, and sugary sweets, median (IQR) | 3.66 (2.62–4.68) | 2.33 (1.02–2.23) | <0.001 |
| Daily servings of vegetables, median (IQR) | 1.26 (0.93–1.90) | 1.14 (0.33–1.95) | 0.198 |
| Daily servings of milk and yogurt, median (IQR) | 0.80 (0.0–1.50) | 1.16 (0.13–1.50) | 0.373 |
| Daily Dietary Intake | Unadjusted Analysis | Adjusted Analysis | ||||||
|---|---|---|---|---|---|---|---|---|
| B | 95% Lower CI | 95% Upper CI | p-Value | B | 95% Lower CI | 95% Upper CI | p-Value | |
| Simple sugars (g/Kg of body weight) | 1.544 | 0.327 | 2.761 | 0.014 | 1.602 | 0.390 | 2.814 | 0.010 |
| Simple sugars (% of total energy) | 0.148 | 0.064 | 0.233 | 0.001 | 0.158 | 0.074 | 0.242 | 0.0004 |
| Sum of added sugar, jam, and honey (servings/Kg of body weight) | 42.003 | 2.731 | 81.276 | 0.036 | 41.401 | 2.597 | 80.204 | 0.037 |
| Fruit (servings/Kg of body weight) | 36.806 | −1.407 | 75.018 | 0.059 | 39.964 | 1.916 | 78.012 | 0.040 |
| Sum of added sugar, jam, honey, and fruit (servings/Kg of body weight) | 41.328 | 14.071 | 68.585 | 0.003 | 42.083 | 14.954 | 69.213 | 0.003 |
| Sugary sweets (servings/Kg of body weight) | 13.486 | −49.766 | 76.737 | 0.672 | 4.829 | -59.462 | 69.119 | 0.881 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Parisse, S.; Carnevale, S.; Di Bartolomeo, F.; Poli, E.; Miceli, F.; Ferri, F.; Mischitelli, M.; Rocco, B.; Lai, Q.; Lucatelli, P.; et al. A Low Daily Intake of Simple Sugars in the Diet Is Associated with Improved Liver Function in Cirrhotic Liver Transplant Candidates. Nutrients 2023, 15, 1575. https://doi.org/10.3390/nu15071575
Parisse S, Carnevale S, Di Bartolomeo F, Poli E, Miceli F, Ferri F, Mischitelli M, Rocco B, Lai Q, Lucatelli P, et al. A Low Daily Intake of Simple Sugars in the Diet Is Associated with Improved Liver Function in Cirrhotic Liver Transplant Candidates. Nutrients. 2023; 15(7):1575. https://doi.org/10.3390/nu15071575
Chicago/Turabian StyleParisse, Simona, Sara Carnevale, Francesca Di Bartolomeo, Edoardo Poli, Francesca Miceli, Flaminia Ferri, Monica Mischitelli, Bianca Rocco, Quirino Lai, Pierleone Lucatelli, and et al. 2023. "A Low Daily Intake of Simple Sugars in the Diet Is Associated with Improved Liver Function in Cirrhotic Liver Transplant Candidates" Nutrients 15, no. 7: 1575. https://doi.org/10.3390/nu15071575
APA StyleParisse, S., Carnevale, S., Di Bartolomeo, F., Poli, E., Miceli, F., Ferri, F., Mischitelli, M., Rocco, B., Lai, Q., Lucatelli, P., Corona, M., Mennini, G., De Santis, A., Rossi, M., Muscaritoli, M., Cantafora, A., & Ginanni Corradini, S. (2023). A Low Daily Intake of Simple Sugars in the Diet Is Associated with Improved Liver Function in Cirrhotic Liver Transplant Candidates. Nutrients, 15(7), 1575. https://doi.org/10.3390/nu15071575