
Dietary and Nutraceutical Interventions as an Adjunct to Non-Surgical Periodontal Therapy—A Systematic Review

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
- -
- RCT;
- -
- Blinding of the participants and/or examiners;
- -
- Generally healthy subjects with periodontitis;
- -
- Periodontal examination with at least PPD;
- -
- An intervention within the study through a modified, defined diet regarding its containing food compilation or administration of supplements/nutraceutical, used as an adjunct to non-surgical periodontal therapy;
- -
- Follow-up period of at least 2 months.
- -
- Studies examining other forms of periodontitis, such as periodontic-endodontic lesions or apical periodontitis as a main research question;
- -
- Studies applying nutraceuticals on the periodontium only locally;
- -
- Studies that included participants under conditions like pregnancy or breastfeeding;
- -
- Studies with participants who were on a combined intake of medications with the nutritional intervention;
- -
- Use of adjuncts like antibiotics or antiseptics;
- -
- Other study designs, such as case series, cohort studies, or animal studies.
2.2. Search Strategy
2.3. Risk of Bias of the Included Studies
2.4. Quality of Evidence
2.5. Meta-Analysis
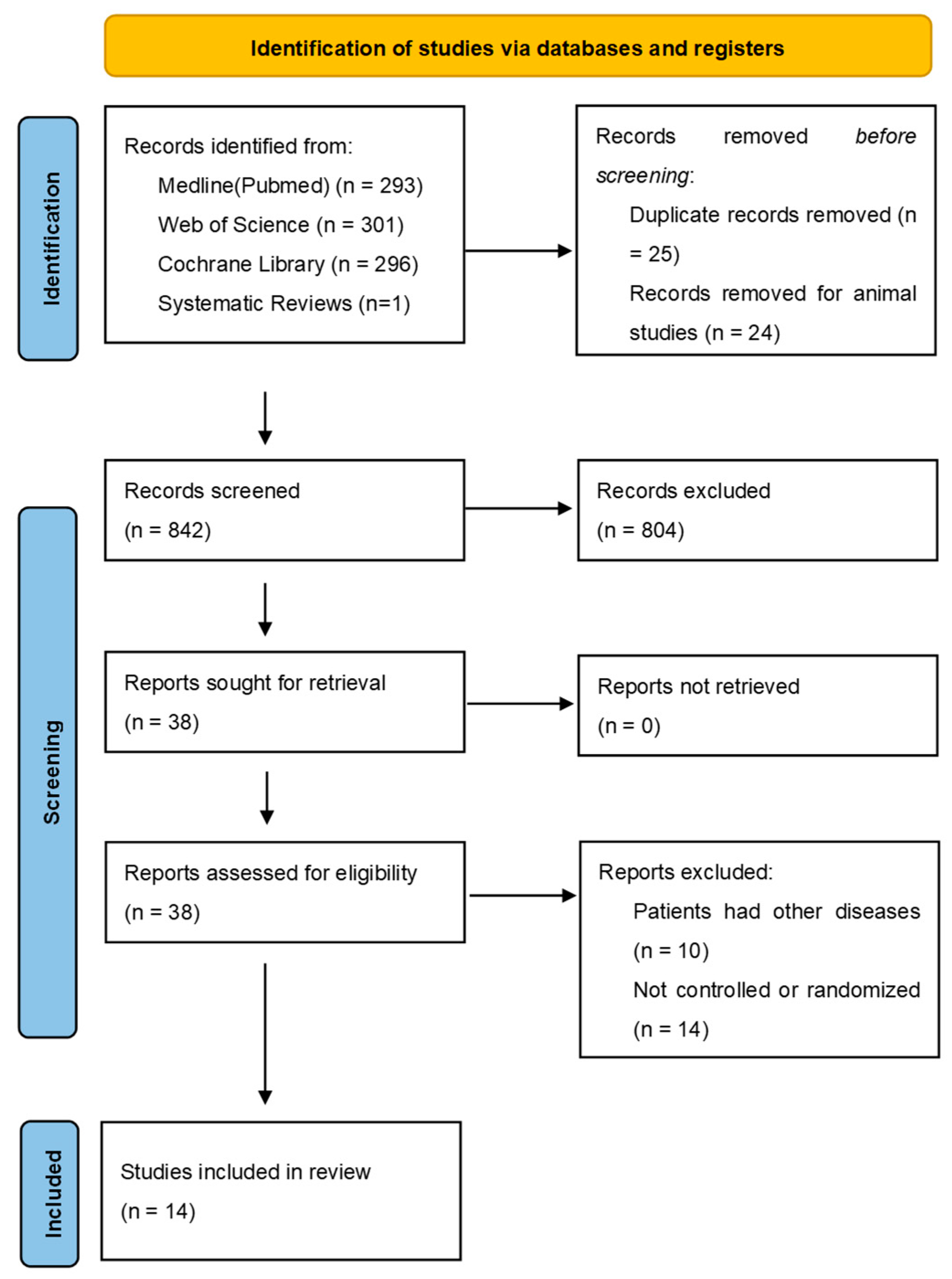
3. Results
3.1. Included Studies
3.2. Characteristics of the Included Studies
- -
- Daily intake of 2 mg lycopene capsules with additional micronutrients over 2 months [26].
- -
- Chicory extract capsules over a period of 2 months [27].
- -
- Folic acid capsules over a period of 6 months [28].
- -
- Daily consumption of oolong tea for 30 days [29].
- -
- Fruit–vegetable or fruit–vegetable–berry capsules given over a period of 8 months [30].
- -
- -
- -
- -
- The effects of twice daily consumption of green tea over 3 months was examined by one study [38].
- -
- Daily consumption of 200 mg vitamin E over a period of 3 months [39]
3.3. Clinical Results of the Studies
3.3.1. Pocket Probing Depths
3.3.2. Bleeding on Probing
3.3.3. Clinical Attachment Loss
3.3.4. Total Antioxidant Capacity
3.3.5. Cytokines in Serum and Saliva
TNF-α
CRP
Interleukins
Chemokines
3.3.6. Serum Lipid Levels
3.3.7. Superoxide Dismutase (SOD) Activity in Serum and Saliva
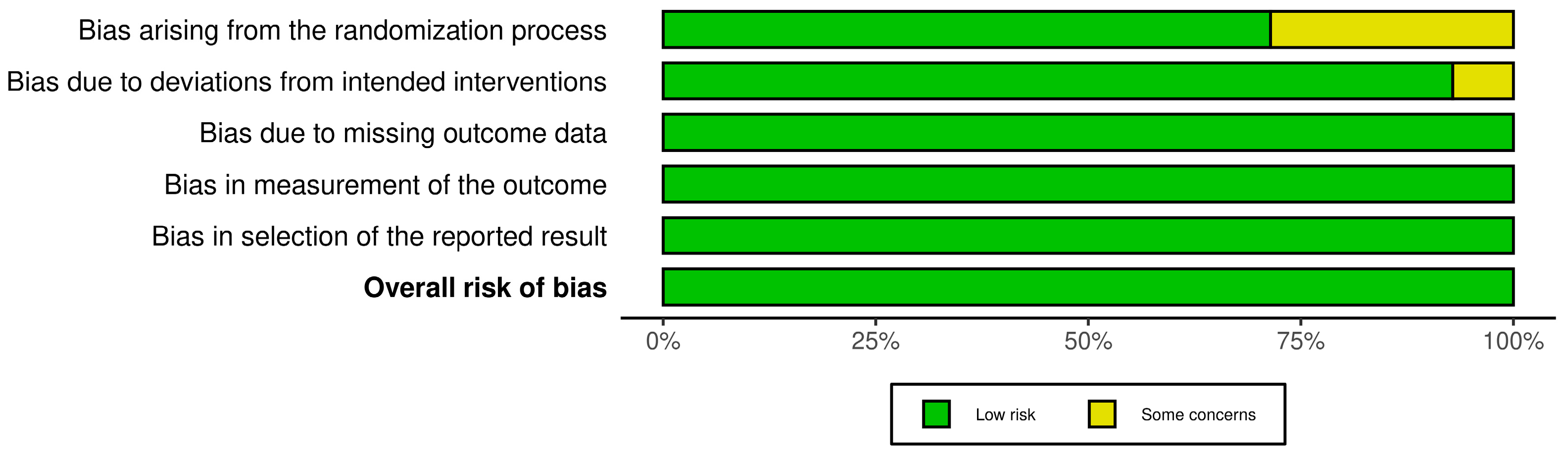
3.4. Risk of Bias
3.5. Meta-Analysis and Grading of Evidence
4. Discussion
4.1. Nutraceutical Interventions and Their Mechanisms in Context to the Literature
4.2. Biochemical Parameters
4.3. Considerations Regarding the Use of Nutraceuticals
4.4. Limitations
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus Report of Workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S173–S182. [Google Scholar] [CrossRef]
- Hajishengallis, G. Immunomicrobial Pathogenesis of Periodontitis: Keystones, Pathobionts, and Host Response. Trends Immunol. 2014, 35, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Nibali, L.; Bayliss-Chapman, J.; Almofareh, S.A.; Zhou, Y.; Divaris, K.; Vieira, A.R. What Is the Heritability of Periodontitis? A Systematic Review. J. Dent. Res. 2019, 98, 632–641. [Google Scholar] [CrossRef]
- Nibali, L.; Di Iorio, A.; Onabolu, O.; Lin, G.-H. Periodontal Infectogenomics: Systematic Review of Associations between Host Genetic Variants and Subgingival Microbial Detection. J. Clin. Periodontol. 2016, 43, 889–900. [Google Scholar] [CrossRef] [PubMed]
- Chapple, I.L.C.; Bouchard, P.; Cagetti, M.G.; Campus, G.; Carra, M.-C.; Cocco, F.; Nibali, L.; Hujoel, P.; Laine, M.L.; Lingstrom, P.; et al. Interaction of Lifestyle, Behaviour or Systemic Diseases with Dental Caries and Periodontal Diseases: Consensus Report of Group 2 of the Joint EFP/ORCA Workshop on the Boundaries between Caries and Periodontal Diseases. J. Clin. Periodontol. 2017, 44 (Suppl S18), S39–S51. [Google Scholar] [CrossRef] [PubMed]
- Sanz, M.; Herrera, D.; Kebschull, M.; Chapple, I.; Jepsen, S.; Beglundh, T.; Sculean, A.; Tonetti, M.S.; EFP Workshop Participants and Methodological Consultants. Treatment of Stage I-III Periodontitis-The EFP S3 Level Clinical Practice Guideline. J. Clin. Periodontol. 2020, 47 (Suppl S22), 4–60. [Google Scholar] [CrossRef]
- Casas, R.; Castro-Barquero, S.; Estruch, R.; Sacanella, E. Nutrition and Cardiovascular Health. Int. J. Mol. Sci. 2018, 19, 3988. [Google Scholar] [CrossRef]
- Mentella, M.C.; Scaldaferri, F.; Ricci, C.; Gasbarrini, A.; Miggiano, G.A.D. Cancer and Mediterranean Diet: A Review. Nutrients 2019, 11, 2059. [Google Scholar] [CrossRef] [PubMed]
- Sami, W.; Ansari, T.; Butt, N.S.; Hamid, M.R.A. Effect of Diet on Type 2 Diabetes Mellitus: A Review. Int. J. Health Sci. 2017, 11, 65–71. [Google Scholar]
- Eaton, S.; Eaton, S.; Konner, M. Review Paleolithic Nutrition Revisited: A Twelve-Year Retrospective on Its Nature and Implications. Eur. J. Clin. Nutr. 1997, 51, 207–216. [Google Scholar] [CrossRef]
- Poulsen, M.W.; Hedegaard, R.V.; Andersen, J.M.; de Courten, B.; Bügel, S.; Nielsen, J.; Skibsted, L.H.; Dragsted, L.O. Advanced Glycation Endproducts in Food and Their Effects on Health. Food Chem. Toxicol. 2013, 60, 10–37. [Google Scholar] [CrossRef]
- Tosti, V.; Bertozzi, B.; Fontana, L. Health Benefits of the Mediterranean Diet: Metabolic and Molecular Mechanisms. J. Gerontol. A Biol. Sci. Med. Sci. 2018, 73, 318–326. [Google Scholar] [CrossRef] [PubMed]
- Cordain, L.; Eaton, S.B.; Sebastian, A.; Mann, N.; Lindeberg, S.; Watkins, B.A.; O’Keefe, J.H.; Brand-Miller, J. Origins and Evolution of the Western Diet: Health Implications for the 21st Century. Am. J. Clin. Nutr. 2005, 81, 341–354. [Google Scholar] [CrossRef]
- Martinez, K.B.; Leone, V.; Chang, E.B. Western Diets, Gut Dysbiosis, and Metabolic Diseases: Are They Linked? Gut Microbes 2017, 8, 130–142. [Google Scholar] [CrossRef] [PubMed]
- Bartha, V.; Exner, L.; Schweikert, D.; Woelber, J.P.; Vach, K.; Meyer, A.L.; Basrai, M.; Bischoff, S.C.; Meller, C.; Wolff, D. Effect of the Mediterranean Diet on Gingivitis. A Randomized Controlled Trial. J. Clin. Periodontol. 2021, 49, 111–122. [Google Scholar] [CrossRef] [PubMed]
- Jenzsch, A.; Eick, S.; Rassoul, F.; Purschwitz, R.; Jentsch, H. Nutritional Intervention in Patients with Periodontal Disease: Clinical, Immunological and Microbiological Variables during 12 Months. Br. J. Nutr. 2009, 101, 879. [Google Scholar] [CrossRef]
- Poulsen, S.K.; Due, A.; Jordy, A.B.; Kiens, B.; Stark, K.D.; Stender, S.; Holst, C.; Astrup, A.; Larsen, T.M. Health Effect of the New Nordic Diet in Adults with Increased Waist Circumference: A 6-Mo Randomized Controlled Trial. Am. J. Clin. Nutr. 2014, 99, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Woelber, J.P.; Gärtner, M.; Breuninger, L.; Anderson, A.; König, D.; Hellwig, E.; Al-Ahmad, A.; Vach, K.; Dötsch, A.; Ratka-Krüger, P.; et al. The Influence of an Anti-Inflammatory Diet on Gingivitis. A Randomized Controlled Trial. J. Clin. Periodontol. 2019, 46, 481–490. [Google Scholar] [CrossRef]
- Woelber, J.P.; Bremer, K.; Vach, K.; König, D.; Hellwig, E.; Ratka-Krüger, P.; Al-Ahmad, A.; Tennert, C. An Oral Health Optimized Diet Can Reduce Gingival and Periodontal Inflammation in Humans—A Randomized Controlled Pilot Study. BMC Oral Health 2016, 17, 28. [Google Scholar] [CrossRef]
- Watson, S.; Woodside, J.V.; Winning, L.; Wright, D.M.; Srinivasan, M.; McKenna, G. The Association between Self-Reported Periodontal Disease and Nutrient Intakes and Nutrient-Based Dietary Patterns in UK Biobank. J. Clin. Periodontol. 2022, 49, 428–438. [Google Scholar] [CrossRef]
- Altun, E.; Walther, C.; Borof, K.; Petersen, E.; Lieske, B.; Kasapoudis, D.; Jalilvand, N.; Beikler, T.; Jagemann, B.; Zyriax, B.-C.; et al. Association between Dietary Pattern and Periodontitis-A Cross-Sectional Study. Nutrients 2021, 13, 4167. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-Bias VISualization (Robvis): An R Package and Shiny Web App for Visualizing Risk-of-Bias Assessments. Res. Synth. Methods 2021, 12, 55–61. [Google Scholar] [CrossRef]
- Schünemann, H.J.; Higgins, J.P.; Vist, G.E.; Glasziou, P.; Akl, E.A.; Skoetz, N.; Guyatt, G.H.; on behalf of the Cochrane GRADEing Methods Group (formerly Applicability and Recommendations Methods Group) and the Cochrane Statistical Methods Group. Completing ‘Summary of Findings’ Tables and Grading the Certainty of the Evidence. In Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2019; pp. 375–402. ISBN 978-1-119-53660-4. [Google Scholar]
- Landis, J.R.; Koch, G.G. The Measurement of Observer Agreement for Categorical Data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed]
- Arora, N.; Avula, H.; Avula, J.K. The Adjunctive Use of Systemic Antioxidant Therapy (Lycopene) in Nonsurgical Treatment of Chronic Periodontitis: A Short-Term Evaluation. Quintessence Int. 2013, 44, 395–405. [Google Scholar] [CrossRef]
- Babaei, H.; Forouzandeh, F.; Maghsoumi-Norouzabad, L.; Yousefimanesh, H.A.; Ravanbakhsh, M.; Zare Javid, A. Effects of Chicory Leaf Extract on Serum Oxidative Stress Markers, Lipid Profile and Periodontal Status in Patients with Chronic Periodontitis. J. Am. Coll Nutr. 2018, 37, 479–486. [Google Scholar] [CrossRef]
- Keceli, H.G.; Ercan, N.; Karsiyaka Hendek, M.; Kisa, U.; Mesut, B.; Olgun, E. The Effect of the Systemic Folic Acid Intake as an Adjunct to Scaling and Root Planing on Clinical Parameters and Homocysteine and C-Reactive Protein Levels in Gingival Crevicular Fluid of Periodontitis Patients: A Randomized Placebo-Controlled Clinical Trial. J. Clin. Periodontol. 2020, 47, 602–613. [Google Scholar] [CrossRef]
- Nafade, S.; Agnihotri, R.; Kamath, S.U.; Shenoy, P.A.; Khadher, N.A.; Nayak, D.D. The Effect of Oolong Tea as an Adjunct to Nonsurgical Management of Chronic Periodontitis: A Randomized Controlled Clinical Trial. J. Herbmed Pharmacol. 2022, 11, 253–261. [Google Scholar] [CrossRef]
- Chapple, I.L.C.; Milward, M.R.; Ling-Mountford, N.; Weston, P.; Carter, K.; Askey, K.; Dallal, G.E.; De Spirt, S.; Sies, H.; Patel, D.; et al. Adjunctive Daily Supplementation with Encapsulated Fruit, Vegetable and Berry Juice Powder Concentrates and Clinical Periodontal Outcomes: A Double-Blind RCT. J. Clin. Periodontol. 2012, 39, 62–72. [Google Scholar] [CrossRef]
- Deore, G.D.; Gurav, A.N.; Patil, R.; Shete, A.R.; Naiktari, R.S.; Inamdar, S.P. Omega 3 Fatty Acids as a Host Modulator in Chronic Periodontitis Patients: A Randomised, Double-Blind, Palcebo-Controlled, Clinical Trial. J. Periodontal Implant. Sci. 2014, 44, 25–32. [Google Scholar] [CrossRef]
- Keskiner, I.; Saygun, I.; Bal, V.; Serdar, M.; Kantarci, A. Dietary Supplementation with Low-Dose Omega-3 Fatty Acids Reduces Salivary Tumor Necrosis Factor-α Levels in Patients with Chronic Periodontitis: A Randomized Controlled Clinical Study. J. Periodontal Res. 2017, 52, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Martinez, G.L.; Koury, J.C.; Martins, M.A.; Nogueira, F.; Fischer, R.G.; Gustafsson, A.; Figueredo, C.M.S. Serum Level Changes of Long Chain-Polyunsaturated Fatty Acids in Patients Undergoing Periodontal Therapy Combined with One Year of Omega-3 Supplementation: A Pilot Randomized Clinical Trial. J. Periodontal Implant. Sci. 2014, 44, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Stańdo, M.; Piatek, P.; Namiecinska, M.; Lewkowicz, P.; Lewkowicz, N. Omega-3 Polyunsaturated Fatty Acids EPA and DHA as an Adjunct to Non-Surgical Treatment of Periodontitis: A Randomized Clinical Trial. Nutrients 2020, 12, 2614. [Google Scholar] [CrossRef]
- Gao, W.; Tang, H.; Wang, D.; Zhou, X.; Song, Y.; Wang, Z. Effect of Short-Term Vitamin D Supplementation after Nonsurgical Periodontal Treatment: A Randomized, Double-Masked, Placebo-Controlled Clinical Trial. J. Periodontal Res. 2020, 55, 354–362. [Google Scholar] [CrossRef]
- Perić, M.; Maiter, D.; Cavalier, E.; Lasserre, J.F.; Toma, S. The Effects of 6-Month Vitamin D Supplementation during the Non-Surgical Treatment of Periodontitis in Vitamin-D-Deficient Patients: A Randomized Double-Blind Placebo-Controlled Study. Nutrients 2020, 12, 2940. [Google Scholar] [CrossRef] [PubMed]
- Graziani, F.; Discepoli, N.; Gennai, S.; Karapetsa, D.; Nisi, M.; Bianchi, L.; Rosema, N.A.M.; Van der Velden, U. The Effect of Twice Daily Kiwifruit Consumption on Periodontal and Systemic Conditions before and after Treatment: A Randomized Clinical Trial. J. Periodontol. 2018, 89, 285–293. [Google Scholar] [CrossRef] [PubMed]
- Chopra, A.; Thomas, B.S.; Sivaraman, K.; Prasad, H.K.; Kamath, S.U. Green Tea Intake as an Adjunct to Mechanical Periodontal Therapy for the Management of Mild to Moderate Chronic Periodontitis: A Randomized Controlled Clinical Trial. Oral. Health Prev. Dent. 2016, 14, 293–303. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Chander Narula, S.; Kumar Sharma, R.; Tewari, S.; Kumar Sehgal, P. Vitamin E Supplementation, Superoxide Dismutase Status, and Outcome of Scaling and Root Planing in Patients with Chronic Periodontitis: A Randomized Clinical Trial. J. Periodontol. 2014, 85, 242–249. [Google Scholar] [CrossRef]
- Vassalle, C.; Masini, S.; Carpeggiani, C.; L’Abbate, A.; Boni, C.; CarloZucchelli, G. In Vivo Total Antioxidant Capacity: Comparison of Two Different Analytical Methods. Clin. Chem. Lab. Med. (CCLM) 2004, 42, 84–89. [Google Scholar] [CrossRef]
- Schünemann, H.J. GRADE: Von der Evidenz zur Empfehlung.: Beschreibung des Systems und Lösungsbeitrag zur Übertragbarkeit von Studienergebnissen. Z. Evid. Fortbild. Qual. Gesundh. 2009, 103, 391–400. [Google Scholar] [CrossRef] [PubMed]
- Brock, G.R.; Butterworth, C.J.; Matthews, J.B.; Chapple, I.L.C. Local and Systemic Total Antioxidant Capacity in Periodontitis and Health. J. Clin. Periodontol. 2004, 31, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Castro, M.M.L.; Duarte, N.N.; Nascimento, P.C.; Magno, M.B.; Fagundes, N.C.F.; Flores-Mir, C.; Monteiro, M.C.; Rösing, C.K.; Maia, L.C.; Lima, R.R. Antioxidants as Adjuvants in Periodontitis Treatment: A Systematic Review and Meta-Analysis. Oxidative Med. Cell. Longev. 2019, 2019, 9187978. [Google Scholar] [CrossRef] [PubMed]
- Tóthová, L.; Celec, P. Oxidative Stress and Antioxidants in the Diagnosis and Therapy of Periodontitis. Front. Physiol. 2017, 8, 1055. [Google Scholar] [CrossRef] [PubMed]
- Reuter, S.; Gupta, S.C.; Chaturvedi, M.M.; Aggarwal, B.B. Oxidative Stress, Inflammation, and Cancer: How Are They Linked? Free Radic. Biol. Med. 2010, 49, 1603–1616. [Google Scholar] [CrossRef] [PubMed]
- Varela-López, A.; Giampieri, F.; Bullón, P.; Battino, M.; Quiles, J. Role of Lipids in the Onset, Progression and Treatment of Periodontal Disease. A Systematic Review of Studies in Humans. Int. J. Mol. Sci. 2016, 17, 1202. [Google Scholar] [CrossRef] [PubMed]
- Graham, H.N. Green Tea Composition, Consumption, and Polyphenol Chemistry. Prev. Med. 1992, 21, 334–350. [Google Scholar] [CrossRef] [PubMed]
- Unachukwu, U.J.; Ahmed, S.; Kavalier, A.; Lyles, J.T.; Kennelly, E.J. White and Green Teas (Camellia Sinensis Var. Sinensis): Variation in Phenolic, Methylxanthine, and Antioxidant Profiles. J. Food Sci. 2010, 75, C541–C548. [Google Scholar] [CrossRef]
- Sparrow, T.V.; Dodington, D.W.; Yumol, J.L.; Fritz, P.C.; Ward, W.E. Higher Intakes of Flavonoids Are Associated with Lower Salivary IL-1β and Maintenance of Periodontal Health 3-4 Years after Scaling and Root Planing. J. Clin. Periodontol. 2020, 47, 461–469. [Google Scholar] [CrossRef]
- Lamprecht, M.; Obermayer, G.; Steinbauer, K.; Cvirn, G.; Hofmann, L.; Ledinski, G.; Greilberger, J.F.; Hallstroem, S. Supplementation with a Juice Powder Concentrate and Exercise Decrease Oxidation and Inflammation, and Improve the Microcirculation in Obese Women: Randomised Controlled Trial Data. Br. J. Nutr. 2013, 110, 1685–1695. [Google Scholar] [CrossRef]
- Lamprecht, M.; Oettl, K.; Schwaberger, G.; Hofmann, P.; Greilberger, J.F. Several Indicators of Oxidative Stress, Immunity, and Illness Improved in Trained Men Consuming an Encapsulated Juice Powder Concentrate for 28 Weeks. J. Nutr. 2007, 137, 2737–2741. [Google Scholar] [CrossRef]
- Lietz, G.; Lange, J.; Rimbach, G. Molecular and Dietary Regulation of Beta,Beta-Carotene 15,15′-Monooxygenase 1 (BCMO1). Arch. Biochem. Biophys. 2010, 502, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Vissers, M.C.M.; Carr, A.C.; Pullar, J.M.; Bozonet, S.M. Chapter Seven—The Bioavailability of Vitamin C from Kiwifruit. In Advances in Food and Nutrition Research; Boland, M., Moughan, P.J., Eds.; Nutritional Benefits of Kiwifruit; Academic Press: Cambridge, MA, USA, 2013; Volume 68, pp. 125–147. [Google Scholar]
- Leggott, P.J.; Robertson, P.B.; Jacob, R.A.; Zambon, J.J.; Walsh, M.; Armitage, G.C. Effects of Ascorbic Acid Depletion and Supplementation on Periodontal Health and Subgingival Microflora in Humans. J. Dent. Res. 1991, 70, 1531–1536. [Google Scholar] [CrossRef] [PubMed]
- Amaliya, A.; Risdiana, A.S.; Van der Velden, U. Effect of Guava and Vitamin C Supplementation on Experimental Gingivitis: A Randomized Clinical Trial. J. Clin. Periodontol. 2018, 45, 959–967. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Q.; Im, S.; Wagner, J.G.; Hernandez, M.L.; Peden, D.B. Gamma-Tocopherol, a Major Form of Vitamin E in Diets: Insights into Antioxidant and Anti-Inflammatory Effects, Mechanisms, and Roles in Disease Management. Free Radic. Biol. Med. 2022, 178, 347–359. [Google Scholar] [CrossRef]
- Singh, U.; Devaraj, S.; Jialal, I. Vitamin E, Oxidative Stress, and Inflammation. Annu. Rev. Nutr. 2005, 25, 151–174. [Google Scholar] [CrossRef]
- Lewis, E.D.; Meydani, S.N.; Wu, D. Regulatory Role of Vitamin E in the Immune System and Inflammation. IUBMB Life 2019, 71, 487–494. [Google Scholar] [CrossRef]
- Shadisvaaran, S.; Chin, K.-Y.; Shahida, M.-S.; Ima-Nirwana, S.; Leong, X.-F. Effect of Vitamin E on Periodontitis: Evidence and Proposed Mechanisms of Action. J. Oral Biosci. 2021, 63, 97–103. [Google Scholar] [CrossRef]
- Fassio, A.; Adami, G.; Rossini, M.; Giollo, A.; Caimmi, C.; Bixio, R.; Viapiana, O.; Milleri, S.; Gatti, M.; Gatti, D. Pharmacokinetics of Oral Cholecalciferol in Healthy Subjects with Vitamin D Deficiency: A Randomized Open-Label Study. Nutrients 2020, 12, 1553. [Google Scholar] [CrossRef]
- Ish-Shalom, S.; Segal, E.; Salganik, T.; Raz, B.; Bromberg, I.L.; Vieth, R. Comparison of Daily, Weekly, and Monthly Vitamin D3 in Ethanol Dosing Protocols for Two Months in Elderly Hip Fracture Patients. J. Clin. Endocrinol. Metab. 2008, 93, 3430–3435. [Google Scholar] [CrossRef]
- Wu, F.; Xiao, C.; Aitken, D.; Jones, G.; Winzenberg, T. The Optimal Dosage Regimen of Vitamin D Supplementation for Correcting Deficiency in Adolescents: A Pilot Randomized Controlled Trial. Eur. J. Clin. Nutr. 2018, 72, 534–540. [Google Scholar] [CrossRef]
- Machado, V.; Lobo, S.; Proença, L.; Mendes, J.J.; Botelho, J. Vitamin D and Periodontitis: A Systematic Review and Meta-Analysis. Nutrients 2020, 12, 2177. [Google Scholar] [CrossRef] [PubMed]
- Esaki, M.; Morita, M.; Akhter, R.; Akino, K.; Honda, O. Relationship between Folic Acid Intake and Gingival Health in Non-Smoking Adults in Japan. Oral Dis. 2010, 16, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Sumona, B.; Sheetal, S.; Anil, M.; Suvarna, P. Comparative Evaluation of Serum Folic Acid Levels in Smokers and Non-Smokers with Chronic Periodontitis. Bangladesh J. Med. Sci. 2011, 10, 83–90. [Google Scholar] [CrossRef]
- Yu, Y.-H.; Kuo, H.-K.; Lai, Y.-L. The Association Between Serum Folate Levels and Periodontal Disease in Older Adults: Data from the National Health and Nutrition Examination Survey 2001/02. J. Am. Geriatr. Soc. 2007, 55, 108–113. [Google Scholar] [CrossRef]
- Asbaghi, O.; Ghanavati, M.; Ashtary-Larky, D.; Bagheri, R.; Rezaei Kelishadi, M.; Nazarian, B.; Nordvall, M.; Wong, A.; Dutheil, F.; Suzuki, K.; et al. Effects of Folic Acid Supplementation on Oxidative Stress Markers: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Antioxidants 2021, 10, 871. [Google Scholar] [CrossRef]
- Simopoulos, A.P. The Importance of the Ratio of Omega-6/Omega-3 Essential Fatty Acids. Biomed. Pharmacother. 2002, 56, 365–379. [Google Scholar] [CrossRef]
- Naqvi, A.Z.; Buettner, C.; Phillips, R.S.; Davis, R.B.; Mukamal, K.J. N-3 Fatty Acids and Periodontitis in US Adults. J. Am. Diet. Assoc. 2010, 110, 1669–1675. [Google Scholar] [CrossRef]
- Kruse, A.B.; Kowalski, C.D.; Leuthold, S.; Vach, K.; Ratka-Krüger, P.; Woelber, J.P. What Is the Impact of the Adjunctive Use of Omega-3 Fatty Acids in the Treatment of Periodontitis? A Systematic Review and Meta-Analysis. Lipids Health Dis. 2020, 19, 100. [Google Scholar] [CrossRef]
- Van Ravensteijn, M.M.; Timmerman, M.F.; Brouwer, E.A.G.; Slot, D.E. The Effect of Omega-3 Fatty Acids on Active Periodontal Therapy: A Systematic Review and Meta-Analysis. J. Clin. Periodontol. 2022, 49, 1024–1037. [Google Scholar] [CrossRef]
- Castro Dos Santos, N.C.; Furukawa, M.V.; Oliveira-Cardoso, I.; Cortelli, J.R.; Feres, M.; Van Dyke, T.; Rovai, E.S. Does the Use of Omega-3 Fatty Acids as an Adjunct to Non-Surgical Periodontal Therapy Provide Additional Benefits in the Treatment of Periodontitis? A Systematic Review and Meta-Analysis. J. Periodontal Res. 2022, 57, 435–447. [Google Scholar] [CrossRef]
- Benzie, I.F.; Szeto, Y.T.; Strain, J.J.; Tomlinson, B. Consumption of Green Tea Causes Rapid Increase in Plasma Antioxidant Power in Humans. Nutr. Cancer 1999, 34, 83–87. [Google Scholar] [CrossRef] [PubMed]
- Saggu, S.; Sakeran, M.I.; Zidan, N.; Tousson, E.; Mohan, A.; Rehman, H. Ameliorating Effect of Chicory (Chichorium intybus L.) Fruit Extract against 4-Tert-Octylphenol Induced Liver Injury and Oxidative Stress in Male Rats. Food Chem. Toxicol. 2014, 72, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Nah, J.; Chun, S.; Park, H.; Yang, S.E.; Min, W.K. In Vivo Antioxidant Effect of Green Tea. Eur. J. Clin. Nutr. 2000, 54, 527–529. [Google Scholar] [CrossRef] [PubMed]
- Noack, B.; Genco, R.J.; Trevisan, M.; Grossi, S.; Zambon, J.J.; De Nardin, E. Periodontal Infections Contribute to Elevated Systemic C-Reactive Protein Level. J. Periodontol. 2001, 72, 1221–1227. [Google Scholar] [CrossRef] [PubMed]
- Pejcic, A.; Kesic, L.J.; Milasin, J. C-Reactive Protein as a Systemic Marker of Inflammation in Periodontitis. Eur. J. Clin. Microbiol. Infect. Dis. 2011, 30, 407–414. [Google Scholar] [CrossRef]
- Lai, J.; Bai, Y.-L.; Bai, Y.; Mei, J.; Zhang, Z.-W.; Tang, W.-J.; Huang, J. A Meta-analysis of the effect of non-surgical periodontal therapy on inflammatory factors in patients with chronic kidney disease and periodontitis. Hua Xi Kou Qiang Yi Xue Za Zhi 2020, 38, 672–680. [Google Scholar] [CrossRef]
- Nepomuceno, R.; Pigossi, S.C.; Finoti, L.S.; Orrico, S.R.P.; Cirelli, J.A.; Barros, S.P.; Offenbacher, S.; Scarel-Caminaga, R.M. Serum Lipid Levels in Patients with Periodontal Disease: A Meta-Analysis and Meta-Regression. J. Clin. Periodontol. 2017, 44, 1192–1207. [Google Scholar] [CrossRef]
- Fu, Y.-W.; Li, X.-X.; Xu, H.-Z.; Gong, Y.-Q.; Yang, Y. Effects of Periodontal Therapy on Serum Lipid Profile and Proinflammatory Cytokines in Patients with Hyperlipidemia: A Randomized Controlled Trial. Clin. Oral Investig. 2016, 20, 1263–1269. [Google Scholar] [CrossRef]
- Sandström, B. Micronutrient Interactions: Effects on Absorption and Bioavailability. Br. J. Nutr. 2001, 85 (Suppl S2), S181–S185. [Google Scholar] [CrossRef]
- Belludi, S.A.; Verma, S.; Banthia, R.; Bhusari, P.; Parwani, S.; Kedia, S.; Saiprasad, S.V. Effect of Lycopene in the Treatment of Periodontal Disease: A Clinical Study. J. Contemp. Dent. Pract. 2013, 14, 1054–1059. [Google Scholar] [CrossRef]
- Muñoz, C.A.; Kiger, R.D.; Stephens, J.A.; Kim, J.; Wilson, A.C. Effects of a Nutritional Supplement on Periodontal Status. Compend. Contin. Educ. Dent. 2001, 22, 425–428, 430, 432 passim; quiz 440. [Google Scholar] [PubMed]
- Lentjes, M.A.H. The Balance between Food and Dietary Supplements in the General Population. Proc. Nutr. Soc. 2019, 78, 97–109. [Google Scholar] [CrossRef] [PubMed]
- Myles, I.A. Fast Food Fever: Reviewing the Impacts of the Western Diet on Immunity. Nutr. J. 2014, 13, 61. [Google Scholar] [CrossRef]
- Woelber, J.P.; Tennert, C. Chapter 13: Diet and Periodontal Diseases. Monogr. Oral. Sci. 2020, 28, 125–133. [Google Scholar] [CrossRef]
- Né, Y.G.S.; Martins, B.V.; Castro, M.M.L.; Alvarenga, M.O.P.; Fagundes, N.C.F.; Magno, M.B.; Maia, L.C.; Lima, R.R. Is Nutritional Intervention an Improvement Factor in the Management of Periodontitis? A Systematic Review. Clin. Nutr. 2020, 39, 2639–2646. [Google Scholar] [CrossRef]
- Zare Javid, A.; Seal, C.J.; Heasman, P.; Moynihan, P.J. Impact of a Customised Dietary Intervention on Antioxidant Status, Dietary Intakes and Periodontal Indices in Patients with Adult Periodontitis. J. Hum. Nutr. Diet. 2014, 27, 523–532. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| First Author | Arora et al. | Babaei et al. | Keceli et al. | Nafade et al. | Chapple et al. | Chopra et al. | Graziani et al. |
| Publication year | 2013 | 2018 | 2019 | 2022 | 2012 | 2016 | 2017 |
| n total n control n intervention | 46 23 23 | 40 20 20 | 37 20 17 | 60 30 30 | 61 21 Je 20 | 120 60 60 | 50 25 25 |
| Study design | RCT | RCT | RCT | RCT | RCT | RCT | RCT |
| Intervention group | 8 mg lycopene daily (2× daily 2 softgel capsules with 2 mg each) in the form of lycopene vitamin mineral capsules + SRP | 2× daily capsules with 1 g chicory extract + twice SRP | 400 mcg folic acid with calcium and vitamin D, 1× daily + single SRP | 4 g oolong tea per day for 30 days + SRP | 2× daily 3 fruit-vegetable or fruit-vegetable-berry juice powder capsules for 9 months + SRP | 2× daily a cup of green tea for + SRP | 2× daily one kiwi + SRP after 2 months |
| Control group | 2× daily 2 placebo each + SRP | 2× daily placebo for 8 weeks + twice SRP | 1× daily placebo + single SRP | No oolong tea + SRP | 2× daily 3 placebo + SRP | 2× daily a cup of cellulose tea (placebo) + SRP | No kiwis + SRP |
| Type of intervention | Lycopene vitamin mineral capsules + SRP | chicory extract capsules + twice SRP | Folic acid capsules + SRP | Oolong tea + SRP | Fruit-vegetable or fruit-vegetable-berry juice powder capsules + SRP | green tea + SRP | Kiwifruit + SRP |
| Duration of intervention | 2 months | 2 months | 6 months | 3 months | 9 months | 3 months | 5 months |
| Who carried out intervention? | Periodontist | Dentist | n.a. | n.a. | n.a. | n.a. | n.a. |
| Examination interval | Baseline, every 15 days until endpoint at 2 months. | Baseline, after 8 weeks | Baseline, after 1, 3, and 6 months | Baseline, after 1, 3 months | Baseline, after 2, 5, and 8 months. | Baseline, after 1 and 3 months | Baseline, 2, 3, 4, and 5 months. |
| Outcomes | PPD, CAL, salivary IL1ß, BOP, PI, MGI, serum TNFα, salivary uric acid. | PPD, BMI, TAC, MDA, uric acid, blood lipids (TC, TG, LDL-C, HDL-C) | PPD, CAL, PI, GI, GR, serum folic acid, GCF volume, Homocysteine, CRP | PPD, CAL, BOP, GI, PI, total antioxidants, glutathione peroxidase, malondialdehyde, CFUs in Plaque | PPD, CAL, BOP, GCF, gingival redness: MGI, cumulative plaque index (Lobene et al. 1982), recessions. | PPD, CAL, BI, GI, PI, antioxidant levels in GCF and plasma. | PPD, CAL, BOP, FMPS recessions, BMI, serum markers: CRP, HbA1c, HDL, LDL, TG, TC, serum vitamin C. |
| Drop-outs | Yes (n = 4) | No | Yes (n = 23) | n.a. | Yes (n = 6) | Yes (n = 5) | No |
| Results compared with test group | ↓PI, ↓MGI, ↓BOP ↓salivary IL1ß, ↓uric acid levels. | ↓PPD, ↑TAC | After 3 months: no sig. diff for PPD, GR; GI and PI, GCF and CRP, ↓CAL, ↑folic acid, ↓Homocysteine | After 3 months: no sig. diff for PPD and CAL, ↓PI, ↓GI, ↓BOP, ↑total antioxidants, ↓glutathione ↓peroxidase, ↓malondialdehyde, ↓CFUs in Plaque | After 2 months: ↓PPD (FV) After 5 months: ↓BOP (FV) ↓GCF (FVB). | ↓ PPD, ↓BOP, ↑TAC in sulcus fluid. | ↓CAL, FMPS, and FMBS of control group ↓Blood pressure, ↑Vitamin C. |
| Conclusions | + | + | + | + | + | + | - |
| First Author | Deore et al. | Stando et al. | Keskiner et al. | Martinez et al. | Singh et al. | Gao et al. | Peric et al. |
| Publication year | 2014 | 2020 | 2017 | 2014 | 2014 | 2020 | 2020 |
| n total n control n intervention | 60 30 30 | 40 20 20 | 30 15 15 | 15 8 7 | 38 19 19 | 360 120 240 | 27 14 13 |
| Study design | RCT | RCT | RCT | RCT | RCT | RCT | RCT |
| Intervention group | 1× daily 300 mg omega-3 fatty acids 180 mg EPA and 120 mg DHA + SRP | 2× daily 10 mL of fish oil (=2.6 g EPA, 1.8 g DHA, 1.4 g alkylglycerol, 1.4 g squalene, 240 µg vitamin A, 2 µg vitamin D3) + SRP | 2× daily low dose Omega 3 PUFA (6.25 mg EPA and 19.19 mg DHA in the form of fish oil) + SRP | 3× daily 300 mg omega-3 FS capsules (180 mg EPA, 120 mg DHA) for 12 months) + SRP | 1× daily 200 mg vitamin E + SRP | 1× daily 2000 IU resp. 1000 IU vitamin D3 + SRP | 1× weekly ampoule 25,000 IU vitamin D3 (=approx. 3571 IU daily) + SRP |
| Control group | 1× daily placebo: 300 mg liquid paraffin + SRP | SRP | 2× daily placebo + SRP | 3× daily placebo + SRP | SRP | 1× daily placebo + SRP | 1× weekly placebo + SRP |
| Type of intervention | Omega-3 fatty acids + SRP | Fish oil + SRP | Omega 3 fatty acids + SRP | Omega-3 fatty acids + SRP | Vitamin E + SRP | Vitamin D3 + SRP | Vitamin D3 + SRP |
| Duration of intervention | 3 months | 3 months | 6 months | 12 months | 3 months | 3 months | 6 months |
| Who carried out intervention? | Dentist/periodontist | Dentist/periodontist | n.a. | Nutritionist and periodontist | n.a. | n.a. | n.a. |
| Examination interval | Baseline, 6 and 12 weeks | Baseline, after 3 months | Baseline, 1, 3, and 6 months | Baseline 4 and 12 months | Baseline, after 3 months | Baseline, after 3 months | Baseline, after 1, 3, and 6 months |
| Outcomes | PPD, CAL, SBI, PI, GI, OHIS (Oral Hygiene Index Simplified), serum CRP | n PPD ≥ 4 mm, PPD, CAL, REC, BOP, % of PPD ≤ 4 mm without BOP, Salivary cytokines, chemokines and growth factors | PPD; CAL BOP, PI, GI, saliva: TNF-α, SOD. | PPD, CAL, BOP, BMI, blood: lipid levels, CRP, omega-3 and omega-6 LC-PUFA (EPA, DHA, DPA, AA), plasma glucose, TAC, TC, HDL-c, LDL-c, VLDL-C, HbA-1c, insulin, and leukocytes. | PPD, CAL, BOP, GI, PI, Saliva SOD activity, Serum SOD activity | PPD, CAL, BI, PI, serum 25(OH)D level, ACH (alveolar crest height) | PPD, FMBS, FMPS, creatinine, osteocalcin, alkaline phosphatase, calcium, HDL, parathyroid hormone, neutrophils, lymphocytes |
| Drop-outs | Yes (n = 2) | Yes (n = 10) | No | No | No | Yes (n = 37) | Yes (n = 6) |
| Results compared with test group | ↓GI, ↓SBI, ↓PPD ↓CAL serum CRP no sig. Change | ↑REC, ↓CAL, ↓BOP, ↓FMPI ↑∆CAL, ↑∆% of PPD ≤ 4 mm without BOP, ↓IL-12, ↓IL-17, ↑IL-10, ↑CCL-5/RANTES, ↑CCL22/MDC, ↑CCL25TECK, ↑CX3CL1/Factalkine ↑CXCL8/IL-8 ↑FGF2, G-CSF | Perio parameters no sig. Differences between groups↓, TNF-α. | Perio parameters no sig. Differences, ↑EPA, ↓BOP in control group. | ↓PPD, ↓CAL, ↓BOP, ↓GI, ↓PI, ↓Saliva SOD activity, ↓Serum SOD activity in both groups ↑∆PPD, ↑∆CAL, ↑∆BOP, ↑∆GI, ↑∆PI, ↑∆Saliva ↑∆SOD, ↑∆Serum SOD | ↓AL, ↓PPD | Perio parameters no sig. Differences |
| Conclusions | + | + | - | - | + | + | - |
| Quality Assessment | Summary of Findings | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| N Patients | Effect | Evidence | |||||||||
| Topic | N Studies | Design (RCT) | Limitations/Risk of Bias | Inconsistency | Indirectness | Imprecision | Other Considerations | Experimental Group | Control Group | SMD [95% Conf. Interval] | |
| Vitamin D | 2 | Yes | No serious limitations | Some inconsistency | Some risk of indirectness * 1 | n/a | 225 | 119 | n/a | Low | |
| Omega-3 fatty acids | 4 | Yes | No serious limitations | Some inconsistency | Some risk of indirectness * 1 | n/a | 67 | 66 | n/a | Low | |
| Kiwi-fruit | 1 | Yes | No serious limitations | No serious inconsistency | Some risk of indirectness * 1 | No serious risk of imprecision | 25 | 25 | PPD: −1.62 [−2.27–−0.99] | Very low | |
| Grean tea/Oolong tea | 2 | Yes | Some limitations * 2 | No serious inconsistency | Some risk of indirectness * 1 | n/a | PROMs: less need for reinstrumentation | 86 | 89 | n/a | Low |
| Fruit & vegetable capsules | 1 | Yes | No serious limitations | Some inconsistency * 3 | Some risk of indirectness * 1 | n/a | 20 | 20 | n/a | Very low | |
| Chicory extract | 1 | Yes | No serious limitations | No serious inconsistency | No serious indirectness | n/a | 20 | 20 | n/a | Very low | |
| Lycopene mineral caspules | 1 | Yes | No serious limitations | No serious inconsistency | Some risk of indirectness * 1 | No serious risk of imprecision | 21 | 21 | PPD: 0.00 [−0.61–0.61] | Very low | |
| Folate | 1 | Yes | Some limitations * 4 | No serious inconsistency | Some risk of indirectness * 1 | n/a | 20 | 17 | Very low | ||
| Vitamin E | 1 | Yes | No serious limitations | No serious inconsistency | Some risk of indirectness * 1 | n/a | 19 | 19 | Very low | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Woelber, J.P.; Reichenbächer, K.; Groß, T.; Vach, K.; Ratka-Krüger, P.; Bartha, V. Dietary and Nutraceutical Interventions as an Adjunct to Non-Surgical Periodontal Therapy—A Systematic Review. Nutrients 2023, 15, 1538. https://doi.org/10.3390/nu15061538
Woelber JP, Reichenbächer K, Groß T, Vach K, Ratka-Krüger P, Bartha V. Dietary and Nutraceutical Interventions as an Adjunct to Non-Surgical Periodontal Therapy—A Systematic Review. Nutrients. 2023; 15(6):1538. https://doi.org/10.3390/nu15061538
Chicago/Turabian StyleWoelber, Johan Peter, Katharina Reichenbächer, Tara Groß, Kirstin Vach, Petra Ratka-Krüger, and Valentin Bartha. 2023. "Dietary and Nutraceutical Interventions as an Adjunct to Non-Surgical Periodontal Therapy—A Systematic Review" Nutrients 15, no. 6: 1538. https://doi.org/10.3390/nu15061538
APA StyleWoelber, J. P., Reichenbächer, K., Groß, T., Vach, K., Ratka-Krüger, P., & Bartha, V. (2023). Dietary and Nutraceutical Interventions as an Adjunct to Non-Surgical Periodontal Therapy—A Systematic Review. Nutrients, 15(6), 1538. https://doi.org/10.3390/nu15061538