
Clinical Impact of Enteral Protein Nutritional Therapy on Patients with Obesity Scheduled for Bariatric Surgery: A Focus on Safety, Efficacy, and Pathophysiological Changes

 , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Characteristics of the Study Patients at Baseline
2.2. Study Assessment and Endpoints
2.3. Safety
2.4. Dietary Interventions
2.5. Anthropometric Evaluation of the Study Population
2.6. Blood Tests of the Study Population
2.7. Ultrasound Measurement
2.8. Statistical Analysis
3. Results
3.1. Impact of NEP and NEI on BW, BMI, WC, HC, and NC
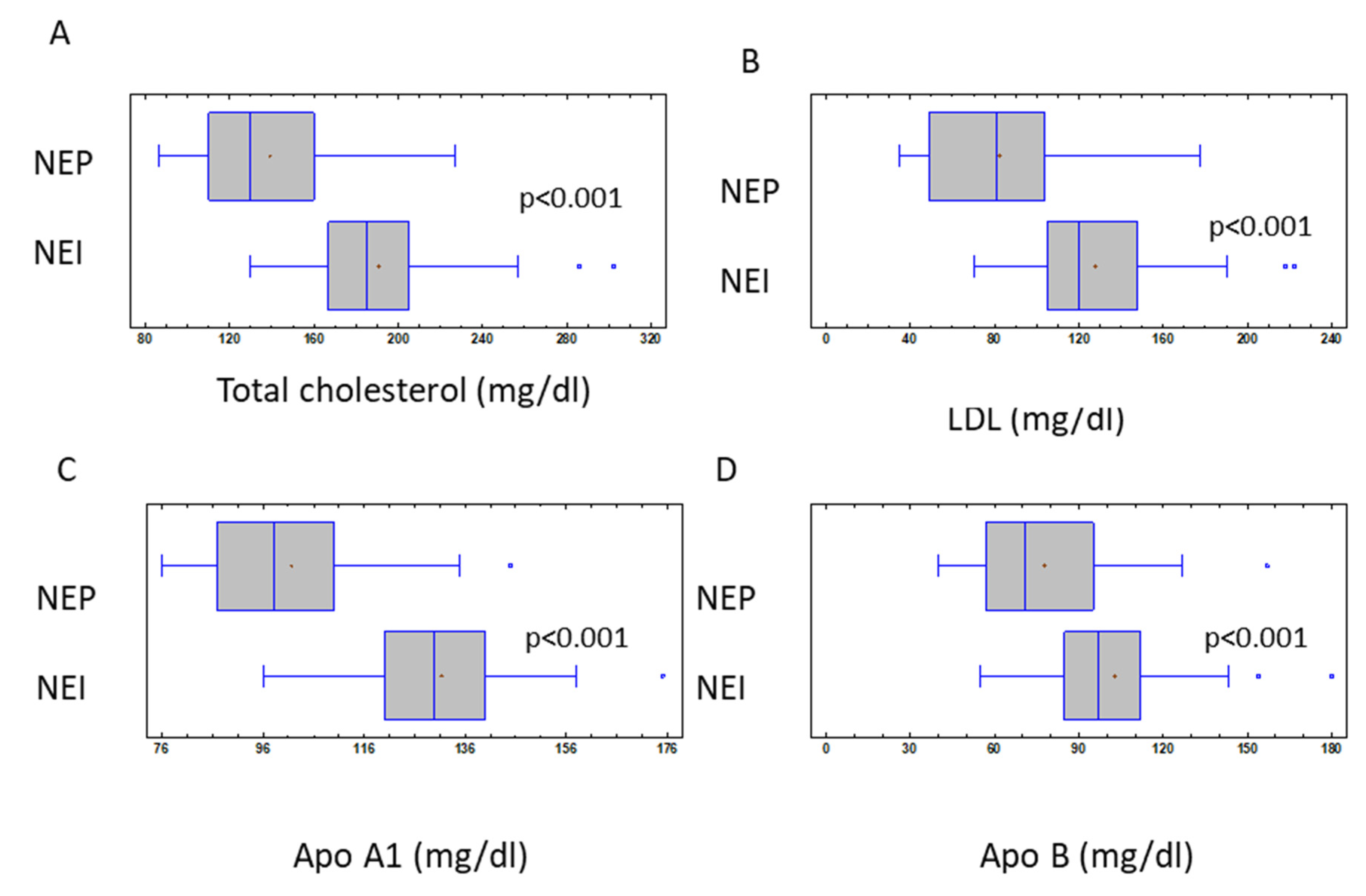
3.2. Impact of NEP and NEI on Patient’s Clinical Parameters and Safety
3.3. Impact of NEP and NEI on AMFT, Steatosis Grade, and Left Lobe Liver Volume
4. Discussion
- 1.
- The enteral nutrition strategies could represent a possible alternative to other methodologies, in particular when it is recommended to improve the patient’s adherence to following the prescribed diet before BS.
- 2.
- Enteral feeding is an effective and safe treatment before BS, with NEP warranting better clinical results than NEI on glycemic and lipid profiles.
- 3.
- Regarding safety, no important side effects were reported.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Carter, J.; Chang, J.; Birriel, T.J.; Moustarah, F.; Sogg, S.; Goodpaster, K.; Benson-Davies, S.; Chapmon, K.; Eisenberg, D. ASMBS position statement on preoperative patient optimization before metabolic and bariatric surgery. Surg. Obes. Relat. Dis. Off. J. Am. Soc. Bariatr. Surg. 2021, 17, 1956–1976. [Google Scholar] [CrossRef] [PubMed]
- Sarno, G.; Calabrese, P.; Frias-Toral, E.; Ceriani, F.; Fuchs-Tarlovsky, V.; Spagnuolo, M.; Cucalón, G.; Córdova, L.Á.; Schiavo, L.; Pilone, V. The relationship between preoperative weight loss and intra and post-bariatric surgery complications: An appraisal of the current preoperative nutritional strategies. Crit. Rev. Food Sci. Nutr. 2022, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Schiavo, L.; Pierro, R.; Asteria, C.; Calabrese, P.; Di Biasio, A.; Coluzzi, I.; Severino, L.; Giovanelli, A.; Pilone, V.; Silecchia, G. Low-Calorie Ketogenic Diet with Continuous Positive Airway Pressure to Alleviate Severe Obstructive Sleep Apnea Syndrome in Patients with Obesity Scheduled for Bariatric/Metabolic Surgery: A Pilot, Prospective, Randomized Multicenter Comparative Study. Obes. Surg. 2022, 32, 634–642. [Google Scholar] [CrossRef] [PubMed]
- Schiavo, L.; Pilone, V.; Rossetti, G.; Iannelli, A. The Role of the Nutritionist in a Multidisciplinary Bariatric Surgery Team. Obes. Surg. 2019, 29, 1028–1030. [Google Scholar] [CrossRef] [PubMed]
- Pilone, V.; Tramontano, S.; Renzulli, M.; Romano, M.; Cobellis, L.; Berselli, T.; Schiavo, L. Metabolic effects, safety, and acceptability of very low-calorie ketogenic dietetic scheme on candidates for bariatric surgery. Surg. Obes. Relat. Dis. Off. J. Am. Soc. Bariatr. Surg. 2018, 14, 1013–1019. [Google Scholar] [CrossRef]
- van Wissen, J.; Bakker, N.; Doodeman, H.J.; Jansma, E.P.; Bonjer, H.J.; Houdijk, A.P. Preoperative Methods to Reduce Liver Volume in Bariatric Surgery: A Systematic Review. Obes. Surg. 2016, 26, 251–256. [Google Scholar] [CrossRef]
- Iannelli, A.; Fontas, E.; Grec, L.; Nocca, D.; Robert, M.; Schiavo, L.; Schneck, A.S. Four-week omega-3 polyunsaturated fatty acids supplementation for liver left lateral section volume reduction in individuals with morbid obesity undergoing bariatric surgery: A double blind, multicenter, randomized placebo-controlled trial. Int. J. Surg. 2022, 101, 106614. [Google Scholar] [CrossRef]
- Schwartz, M.L.; Drew, R.L.; Chazin-Caldie, M. Factors determining conversion from laparoscopic to open Roux-en-Y gastric bypass. Obes. Surg. 2004, 14, 1193–1197. [Google Scholar] [CrossRef]
- Colangeli, L.; Gentileschi, P.; Sbraccia, P.; Guglielmi, V. Ketogenic Diet for Preoperative Weight Reduction in Bariatric Surgery: A Narrative Review. Nutrients 2022, 14, 3610. [Google Scholar] [CrossRef]
- Leonetti, F.; Campanile, F.C.; Coccia, F.; Capoccia, D.; Alessandroni, L.; Puzziello, A.; Coluzzi, I.; Silecchia, G. Very low-carbohydrate ketogenic diet before bariatric surgery: Prospective evaluation of a sequential diet. Obes. Surg. 2015, 25, 64–71. [Google Scholar] [CrossRef]
- Lorenzo, P.M.; Sajoux, I.; Izquierdo, A.G.; Gomez-Arbelaez, D.; Zulet, M.A.; Abete, I.; Castro, A.I.; Baltar, J.; Portillo, M.P.; Tinahones, F.J.; et al. Immunomodulatory effect of a very-low-calorie ketogenic diet compared with bariatric surgery and a low-calorie diet in patients with excessive body weight. Clin. Nutr. 2022, 41, 1566–1577. [Google Scholar] [CrossRef]
- Schiavo, L.; De Stefano, G.; Persico, F.; Gargiulo, S.; Di Spirito, F.; Griguolo, G.; Petrucciani, N.; Fontas, E.; Iannelli, A.; Pilone, V. A Randomized, Controlled Trial Comparing the Impact of a Low-Calorie Ketogenic vs a Standard Low-Calorie Diet on Fat-Free Mass in Patients Receiving an Elipse™ Intragastric Balloon Treatment. Obes. Surg. 2021, 31, 1514–1523. [Google Scholar] [CrossRef]
- Sarno, G.; Schiavo, L.; Calabrese, P.; Álvarez Córdova, L.; Frias-Toral, E.; Cucalón, G.; Garcia-Velasquez, E.; Fuchs-Tarlovsky, V.; Pilone, V. The Impact of Bariatric-Surgery-Induced Weight Loss on Patients Undergoing Liver Transplant: A Focus on Metabolism, Pathophysiological Changes, and Outcome in Obese Patients Suffering NAFLD-Related Cirrhosis. J. Clin. Med. 2022, 11, 5293. [Google Scholar] [CrossRef]
- Schiavo, L.; Pilone, V.; Rossetti, G.; Barbarisi, A.; Cesaretti, M.; Iannelli, A. A 4-Week Preoperative Ketogenic Micronutrient-Enriched Diet Is Effective in Reducing Body Weight, Left Hepatic Lobe Volume, and Micronutrient Deficiencies in Patients Undergoing Bariatric Surgery: A Prospective Pilot Study. Obes. Surg. 2018, 28, 2215–2224. [Google Scholar] [CrossRef]
- Albanese, A.; Prevedello, L.; Markovich, M.; Busetto, L.; Vettor, R.; Foletto, M. Pre-operative Very Low Calorie Ketogenic Diet (VLCKD) vs. Very Low Calorie Diet (VLCD): Surgical Impact. Obes. Surg. 2019, 29, 292–296. [Google Scholar] [CrossRef]
- Kumar, N.K.; Merrill, J.D.; Carlson, S.; German, J.; Yancy, W.S., Jr. Adherence to Low-Carbohydrate Diets in Patients with Diabetes: A Narrative Review. Diabetes Metab. Syndr. Obes. Targets Ther. 2022, 15, 477–498. [Google Scholar] [CrossRef]
- Muscogiuri, G.; El Ghoch, M.; Colao, A.; Hassapidou, M.; Yumuk, V.; Busetto, L. Obesity Management Task Force (OMTF) of the European Association for the Study of Obesity (EASO) European Guidelines for Obesity Management in Adults with a Very Low-Calorie Ketogenic Diet: A Systematic Review and Meta-Analysis. Obes. Facts 2021, 14, 222–245. [Google Scholar] [CrossRef]
- Landry, M.J.; Crimarco, A.; Perelman, D.; Durand, L.R.; Petlura, C.; Aronica, L.; Robinson, J.L.; Kim, S.H.; Gardner, C.D. Adherence to Ketogenic and Mediterranean Study Diets in a Crossover Trial: The Keto-Med Randomized Trial. Nutrients 2021, 13, 967. [Google Scholar] [CrossRef]
- Sukkar, S.G.; Signori, A.; Borrini, C.; Barisione, G.; Ivaldi, C.; Romeo, C.; Gradaschi, R.; Machello, N.; Nanetti, E.; Vaccaro, A.L. Feasibility of protein-sparing modified fast by tube (ProMoFasT) in obesity treatment: A phase II pilot trial on clinical safety and efficacy (appetite control, body composition, muscular strength, metabolic pattern, pulmonary function test). Mediterr. J. Nutr. Metab. 2013, 6, 165–176. [Google Scholar] [CrossRef]
- Castaldo, G.; Monaco, L.; Castaldo, L.; Galdo, G.; Cereda, E. An observational study of sequential protein-sparing, very low-calorie ketogenic diet (Oloproteic diet) and hypocaloric Mediterranean-like diet for the treatment of obesity. Int. J. Food Sci. Nutr. 2016, 67, 696–706. [Google Scholar] [CrossRef]
- Fried, M.; Yumuk, V.; Oppert, J.M.; Scopinaro, N.; Torres, A.; Weiner, R.; Yashkov, Y.; Frühbeck, G. International Federation for Surgery of Obesity and Metabolic Disorders-European Chapter (IFSO-EC), European Association for the Study of Obesity (EASO), European Association for the Study of Obesity Obesity Management Task Force (EASO OMTF) Interdisciplinary European guidelines on metabolic and bariatric surgery. Obes. Surg. 2014, 24, 42–55. [Google Scholar] [PubMed]
- Eisenberg, D.; Shikora, S.A.; Aarts, E.; Aminian, A.; Angrisani, L.; Cohen, R.V.; de Luca, M.; Faria, S.L.; Goodpaster, K.P.S.; Haddad, A.; et al. 2022 American Society of Metabolic and Bariatric Surgery (ASMBS) and International Federation for the Surgery of Obesity and Metabolic Disorders (IFSO) Indications for Metabolic and Bariatric Surgery. Obes. Surg. 2023, 33, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Gershuni, V.M.; Yan, S.L.; Medici, V. Nutritional Ketosis for Weight Management and Reversal of Metabolic Syndrome. Curr. Nutr. Rep. 2018, 7, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Paoli, A.; Rubini, A.; Volek, J.S.; Grimaldi, K.A. Beyond weight loss: A review of the therapeutic uses of very-low-carbohydrate (ketogenic) diets. Eur. J. Clin. Nutr. 2013, 67, 789–796. [Google Scholar] [CrossRef] [PubMed]
- Monaco, L.; Monaco, M.; Di Tommaso, L.; Stassano, P.; Castaldo, L.; Castaldo, G. Aortomesenteric fat thickness with ultrasound predicts metabolic diseases in obese patients. Am. J. Med. Sci. 2014, 347, 8–13. [Google Scholar] [CrossRef]
- Alarim, R.A.; Alasmre, F.A.; Alotaibi, H.A.; Alshehri, M.A.; Hussain, S.A. Effects of the Ketogenic Diet on Glycemic Control in Diabetic Patients: Meta-Analysis of Clinical Trials. Cureus 2020, 12, e10796. [Google Scholar] [CrossRef]
- Riad, W.; Vaez, M.N.; Raveendran, R.; Tam, A.D.; Quereshy, F.A.; Chung, F.; Wong, D.T. Neck circumference as a predictor of difficult intubation and difficult mask ventilation in morbidly obese patients: A prospective observational study. Eur. J. Anaesthesiol. 2016, 33, 244–249. [Google Scholar] [CrossRef]
- Castaldo, G.; Palmieri, V.; Galdo, G.; Castaldo, L.; Molettieri, P.; Vitale, A.; Monaco, L. Aggressive nutritional strategy in morbid obesity in clinical practice: Safety, feasibility, and effects on metabolic and haemodynamic risk factors. Obes. Res. Clin. Pract. 2016, 10, 169–177. [Google Scholar] [CrossRef]
- Castaldo, G.; Monaco, L.; Castaldo, L.; Sorrentino, P. A 2-Week Course of Enteral Treatment with a Very Low-Calorie Protein-Based Formula for the Management of Severe Obesity. Int. J. Endocrinol. 2015, 2015, 723735. [Google Scholar] [CrossRef]
- Schiavo, L.; Scalera, G.; Pilone, V.; De Sena, G.; Ciorra, F.R.; Barbarisi, A. Patient adherence in following a prescribed diet and micronutrient supplements after laparoscopic sleeve gastrectomy: Our experience during 1 year of follow-up. J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2017, 30, 98–104. [Google Scholar] [CrossRef]
- Keller, U. Nutritional Laboratory Markers in Malnutrition. J. Clin. Med. 2019, 8, 775. [Google Scholar] [CrossRef]
- Evans, D.C.; Corkins, M.R.; Malone, A.; Miller, S.; Mogensen, K.M.; Guenter, P.; Jensen, G.L. ASPEN Malnutrition Committee The Use of Visceral Proteins as Nutrition Markers: An ASPEN Position Paper. Nutr. Clin. Pract. Off. Publ. Am. Soc. Parenter. Enter. Nutr. 2021, 36, 22–28. [Google Scholar]



{kind=link}
{kind=link}
| NEP (n = 31) | NEI (n = 29) | p (NEP vs. NEI) | |
|---|---|---|---|
| Sex (male/female, n) | 6/25 | 6/23 | / |
| Age (mean ± SD, years) | 36.33 ± 10.20 | 39.31 ± 6.91 | 0.8013 |
| Body weight (mean ± SD, kg) | 130.47 ± 23.10 | 124.09 ± 17.20 | 0.5590 |
| BMI (mean ± SD, kg/m2) | 47.89 ± 6.99 | 45.19 ± 4.87 | 0.3827 |
| Clinical Parameters | Groups | Baseline | Follow-Up 4 Weeks | p (Baseline vs. Follow-Up) | p (NEP vs. NEI) |
|---|---|---|---|---|---|
| BW, Kg | NEP NEI | 130.47 ± 23.10 124.09 ± 17.20 | 119.70 ± 21.71 117.23 ± 16.57 | <0.001 * <0.001 * | 0.559 |
| BMI, Kg/m2 | NEP NEI | 47.89 ± 6.99 45.19 ± 4.87 | 43.95 ± 6.57 42.68 ± 4.58 | <0.001 * <0.001 * | 0.383 |
| WC, cm | NEP NEI | 137.52 ± 14.47 132.14 ± 11.02 | 127.45 ± 14.09 126.60 ± 10.99 | <0.001 * <0.001 * | 0.779 |
| HC, cm | NEP NEI | 141.31 ± 14.95 136.62 ± 13.00 | 133.58 ± 14.29 131.07 ± 12.31 | <0.001 * <0.001 * | 0.559 |
| NC, cm | NEP NEI | 41.53 ± 4.72 42.33 ± 3.19 | 38.58 ± 4.10 40.62 ± 3.11 | <0.001 * <0.001 * | 0.011 * |
| Clinical Parameters | Groups | Baseline | Follow-Up 4 Weeks | p (Baseline vs. Follow-Up) | p (NEP vs. NEI) |
|---|---|---|---|---|---|
| Hemoglobin, g/dL | NEP NEI | 13.94 ± 1.66 14.53 ± 4.40 | 13.71 ± 1.49 13.73 ± 1.34 | 0.1338 0.3283 | 0.8940 |
| Hematocrit, % | NEP NEI | 40.85 ± 4.13 40.86 ± 3.95 | 40.63 ± 3.81 41.23 ± 3.67 | 0.6128 0.1987 | 0.6895 |
| Glycated Hemoglobin, % | NEP NEI | 6.02 ± 0.92 5.73 ± 0.87 | 5.69 ± 0.64 5.51 ± 0.55 | <0.001 * 0.0104 * | 0.2686 |
| Glycemia, mg/dL | NEP NEI | 91.81 ± 25.14 95.38 ± 33.77 | 77.10 ± 9.31 87.24 ± 8.23 | 0.0012 * 0.2380 | <0.001 * |
| Insulin, µU/L | NEP NEI | 21.91 ± 16.66 19.07 ± 7.16 | 11.05 ± 9.60 15.68 ± 6.26 | <0.001 * 0.0172 * | 0.0028 * |
| HOMA Index | NEP NEI | 5.03 ± 4.53 4.54 ± 2.27 | 2.12 ± 1.94 3.41 ± 1.47 | <0.001 * 0.0126 * | <0.001 * |
| Azotemia, mg/dL | NEP NEI | 28.55 ± 6.19 30.31 ± 5.95 | 25.29 ± 6.64 27.41 ± 8.13 | 0.0611 0.0246 * | 0.2105 |
| Creatinine, mg/dL | NEP NEI | 0.69 ± 0.12 0.72 ± 0.12 | 0.67 ± 0.11 0.80 ± 0.22 | 0.1674 0.0267 * | 0.0076 * |
| Uricemia, mg/dL | NEP NEI | 5.11 ± 1.21 5.23 ± 1.20 | 6.24 ± 2.69 5.67 ± 1.24 | 0.0113 * 0.0134 * | 0.9233 |
| Total Cholesterol, mg/dL | NEP NEI | 184.00 ± 34.74 196.07 ± 32.57 | 139.32 ± 38.14 190.62 ± 40.06 | <0.001 * 0.3758 | <0.001 * |
| LDL, mg/dL | NEP NEI | 119.23 ± 38.46 130.31 ± 31.35 | 82.39 ± 35.76 127.76 ± 38.31 | <0.001 * 0.2567 | <0.001 * |
| HDL, mg/dL | NEP NEI | 49.26 ± 12.56 50.52 ± 12.23 | 39.10 ± 11.70 47.45 ± 11.84 | <0.001 * 0.0117 * | 0.0107 * |
| Triglycerides, mg/dL | NEP NEI | 120.10 ± 55.60 124.21 ± 70.15 | 100.68 ± 52.85 105.28 ± 44.88 | 0.0200 * 0.0920 | 0.5343 |
| Apo A1, mg/dL | NEP NEI | 133.97 ± 21.19 141.28 ± 18.44 | 101.58 ± 17.62 131.31 ± 17.80 | <0.001 * <0.001 * | <0.001 * |
| Apo B, mg/dL | NEP NEI | 100.94 ± 28.51 105.38 ± 26.60 | 77.65 ± 27.04 102.97 ± 26.74 | <0.001 * 0.5500 | <0.001 * |
| AST, U/L | NEP NEI | 20.45 ± 9.55 20.17 ± 9.45 | 25.35 ± 9.08 21.52 ± 7.19 | 0.0095 * 0.2999 | 0.0818 |
| ALT, U/L | NEP NEI | 28.48 ± 18.94 25.28 ± 14.20 | 35.00 ± 27.55 26.17 ± 11.19 | 0.1567 0.7116 | 0.4774 |
| γGT, U/L | NEP NEI | 25.55 ± 16.36 29.03 ± 10.07 | 16.19 ± 9.08 22.31 ± 12.14 | <0.001 * 0.0882 | 0.3420 |
| Sideremia, mcg/dL | NEP NEI | 67.71 ± 26.34 69.28 ± 19.60 | 52.74 ± 17.95 79.24 ± 27.42 | 0.0041 * 0.0123 * | <0.001 * |
| Total Proteins, g/dL | NEP NEI | 7.18 ± 0.35 7.08 ± 0.35 | 6.97 ± 0.86 7.17 ± 0.33 | 0.1440 0.1068 | 0.3936 |
| Transferrin, mg/dL | NEP NEI | 279.39 ± 45.87 274.79 ± 42.29 | 245.39 ± 53.56 261.25 ± 63.79 | <0.001 * 0.2117 | 0.0711 |
| Albumin, g/dL | NEP NEI | 4.15 ± 0.24 4.12 ± 0.32 | 4.21 ± 0.33 4.24 ± 0.32 | 0.3912 0.0108 * | 0.8590 |
| Sodium, mmol/L | NEP NEI | 138.52 ± 2.35 139.21 ± 1.59 | 138.06 ± 2.61 139.34 ± 2.00 | 0.3602 0.6626 | 0.0197 * |
| Potassium, mequ/L | NEP NEI | 4.54 ± 0.30 4.53 ± 0.30 | 4.55 ± 0.34 4.46 ± 0.31 | 0.7985 0.3108 | 0.0935 |
| Calcium, mg/dL | NEP NEI | 9.31 ± 0.45 9.31 ± 0.30 | 9.38 ± 0.46 9.46 ± 0.34 | 0.3790 0.0183 * | 0.7608 |
| Magnesium, mg/dL | NEP NEI | 2.07 ± 0.08 2.07 ± 0.15 | 2.02 ± 0.16 2.10 ± 0.13 | 0.1562 0.2171 | 0.0789 |
| Phosphorus, mg/dL | NEP NEI | 3.25 ± 0.56 3.38 ± 0.38 | 3.53 ± 0.51 3.35 ± 0.43 | 0.0155 * 0.6333 | 0.1562 |
| Ferritin, ng/mL | NEP NEI | 151.94 ± 66.79 91.97 ± 30.38 | 151.74 ± 69.60 104.07 ± 38.72 | 0.9798 0.0614 | 0.0019 * |
| Clinical Parameters | Groups | Baseline | Follow-Up 4 Weeks | p (Baseline vs. Follow-Up) | p (NEP vs. NEI) |
|---|---|---|---|---|---|
| AMFT, mm | NEP NEI | 22.32 ± 11.64 21.43 ± 7.72 | 15.86 ± 5.12 17.70 ± 6.87 | 0.0015 * <0.001 * | 0.3319 |
| Steatosis, grade | NEP NEI | 2.40 ± 0.42 2.36 ± 0.35 | 1.90 ± 0.45 1.98 ± 0.39 | <0.001 * <0.001 * | 0.6156 |
| Left hepatic lobe volume, cm3 | NEP NEI | 407.39 ± 125.77 385.14 ± 123.90 | 279.58 ± 99.68 313.72 ± 113.98 | <0.001 * <0.001 * | 0.2640 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Castaldo, G.; Schiavo, L.; Pagano, I.; Molettieri, P.; Conte, A.; Sarno, G.; Pilone, V.; Rastrelli, L. Clinical Impact of Enteral Protein Nutritional Therapy on Patients with Obesity Scheduled for Bariatric Surgery: A Focus on Safety, Efficacy, and Pathophysiological Changes. Nutrients 2023, 15, 1492. https://doi.org/10.3390/nu15061492
Castaldo G, Schiavo L, Pagano I, Molettieri P, Conte A, Sarno G, Pilone V, Rastrelli L. Clinical Impact of Enteral Protein Nutritional Therapy on Patients with Obesity Scheduled for Bariatric Surgery: A Focus on Safety, Efficacy, and Pathophysiological Changes. Nutrients. 2023; 15(6):1492. https://doi.org/10.3390/nu15061492
Chicago/Turabian StyleCastaldo, Giuseppe, Luigi Schiavo, Imma Pagano, Paola Molettieri, Aurelio Conte, Gerardo Sarno, Vincenzo Pilone, and Luca Rastrelli. 2023. "Clinical Impact of Enteral Protein Nutritional Therapy on Patients with Obesity Scheduled for Bariatric Surgery: A Focus on Safety, Efficacy, and Pathophysiological Changes" Nutrients 15, no. 6: 1492. https://doi.org/10.3390/nu15061492
APA StyleCastaldo, G., Schiavo, L., Pagano, I., Molettieri, P., Conte, A., Sarno, G., Pilone, V., & Rastrelli, L. (2023). Clinical Impact of Enteral Protein Nutritional Therapy on Patients with Obesity Scheduled for Bariatric Surgery: A Focus on Safety, Efficacy, and Pathophysiological Changes. Nutrients, 15(6), 1492. https://doi.org/10.3390/nu15061492