
Alternate-Day Fasting Combined with Exercise: Effect on Sleep in Adults with Obesity and NAFLD

 , ,
, ,  , ,
, , 
Abstract
1. Introduction
2. Methods
2.1. Subject Selection
2.2. Alternate Day Fasting Protocol
2.3. Exercise Protocol
2.4. Control Group Protocol
2.5. Body Weight, Body Composition, Intrahepatic Triglyceride Content, and Liver Fibrosis
2.6. Energy Intake and Physical Activity
2.7. Sleep Measures
2.8. Statistical Analysis
3. Results
3.1. Subject Baseline Characteristics and Dropouts
3.2. Body Weight, Body Composition, Intrahepatic Triglyceride Content, and Liver Fibrosis
3.3. Energy Intake and Physical Activity
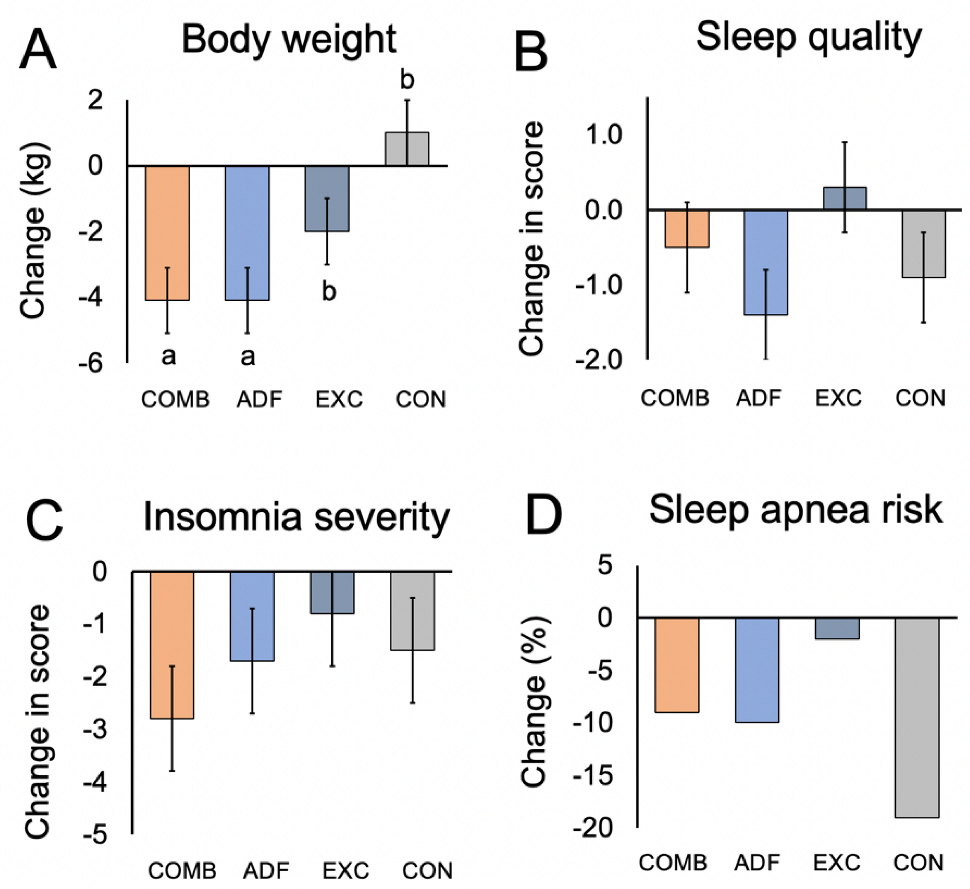
3.4. Sleep Measures
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- Arshad, T.; Golabi, P.; Henry, L.; Younossi, Z.M. Epidemiology of Non-alcoholic Fatty Liver Disease in North America. Curr. Pharm. Des. 2020, 26, 993–997. [Google Scholar] [CrossRef]
- Grandner, M.A.; Sands-Lincoln, M.R.; Pak, V.M.; Garland, S.N. Sleep duration, cardiovascular disease, and proinflammatory biomarkers. Nat. Sci. Sleep 2013, 5, 93–107. [Google Scholar] [CrossRef]
- Um, Y.J.; Chang, Y.; Jung, H.S.; Cho, I.Y.; Shin, J.H.; Shin, H.; Wild, S.H.; Byrne, C.D.; Ryu, S. Sleep Duration, Sleep Quality, and the Development of Nonalcoholic Fatty Liver Disease: A Cohort Study. Clin. Transl. Gastroenterol. 2021, 12, e00417. [Google Scholar] [CrossRef] [PubMed]
- Um, Y.J.; Chang, Y.; Jung, H.S.; Cho, I.Y.; Shin, J.H.; Shin, H.; Wild, S.H.; Byrne, C.D.; Ryu, S. Decrease in Sleep Duration and Poor Sleep Quality over Time Is Associated with an Increased Risk of Incident Non-Alcoholic Fatty Liver Disease. J. Pers. Med. 2022, 12, 92. [Google Scholar] [CrossRef]
- Aron-Wisnewsky, J.; Clement, K.; Pepin, J.L. Nonalcoholic fatty liver disease and obstructive sleep apnea. Metabolism 2016, 65, 1124–1135. [Google Scholar] [CrossRef] [PubMed]
- Thomasouli, M.A.; Brady, E.M.; Davies, M.J.; Hall, A.P.; Khunti, K.; Morris, D.H.; Gray, L.J. The impact of diet and lifestyle management strategies for obstructive sleep apnoea in adults: A systematic review and meta-analysis of randomised controlled trials. Sleep Breath 2013, 17, 925–935. [Google Scholar] [CrossRef] [PubMed]
- Cai, H.; Qin, Y.L.; Shi, Z.Y.; Chen, J.H.; Zeng, M.J.; Zhou, W.; Chen, R.Q.; Chen, Z.Y. Effects of alternate-day fasting on body weight and dyslipidaemia in patients with non-alcoholic fatty liver disease: A randomised controlled trial. BMC Gastroenterol. 2019, 19, 219. [Google Scholar] [CrossRef] [PubMed]
- Johari, M.I.; Yusoff, K.; Haron, J.; Nadarajan, C.; Ibrahim, K.N.; Wong, M.S.; Hafidz, M.I.A.; Chua, B.E.; Hamid, N.; Arifin, W.N.; et al. A Randomised Controlled Trial on the Effectiveness and Adherence of Modified Alternate-day Calorie Restriction in Improving Activity of Non-Alcoholic Fatty Liver Disease. Sci. Rep. 2019, 9, 11232. [Google Scholar] [CrossRef] [PubMed]
- Ezpeleta, M.; Gabel, K.; Cienfuegos, S.; Kalam, F.; Lin, S.; Pavlou, V.; Song, Z.; Haus, J.M.; Koppe, S.; Alexandria, S.J.; et al. Effect of alternate day fasting combined with aerobic exercise on non-alcoholic fatty liver disease: A randomized controlled trial. Cell Metab. 2023, 35, 56–70.e3. [Google Scholar] [CrossRef]
- Vallet-Pichard, A.; Mallet, V.; Nalpas, B.; Verkarre, V.; Nalpas, A.; Dhalluin-Venier, V.; Fontaine, H.; Pol, S. FIB-4: An inexpensive and accurate marker of fibrosis in HCV infection. comparison with liver biopsy and fibrotest. Hepatology 2007, 46, 32–36. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef] [PubMed]
- Bastien, C.H.; Vallieres, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Chung, F.; Yegneswaran, B.; Liao, P.; Chung, S.A.; Vairavanathan, S.; Islam, S.; Khajehdehi, A.; Shapiro, C.M. Validation of the Berlin questionnaire and American Society of Anesthesiologists checklist as screening tools for obstructive sleep apnea in surgical patients. Anesthesiology 2008, 108, 822–830. [Google Scholar] [CrossRef]
- Alfaris, N.; Wadden, T.A.; Sarwer, D.B.; Diwald, L.; Volger, S.; Hong, P.; Baxely, A.; Minnick, A.M.; Vetter, M.L.; Berkowitz, R.I.; et al. Effects of a 2-year behavioral weight loss intervention on sleep and mood in obese individuals treated in primary care practice. Obesity (Silver Spring) 2015, 23, 558–564. [Google Scholar] [CrossRef]
- Martin, C.K.; Bhapkar, M.; Pittas, A.G.; Pieper, C.F.; Das, S.K.; Williamson, D.A.; Scott, T.; Redman, L.M.; Stein, R.; Gilhooly, C.H.; et al. Effect of Calorie Restriction on Mood, Quality of Life, Sleep, and Sexual Function in Healthy Nonobese Adults: The CALERIE 2 Randomized Clinical Trial. JAMA Intern. Med. 2016, 176, 743–752. [Google Scholar] [CrossRef]
- Kalam, F.; Gabel, K.; Cienfuegos, S.; Ezpeleta, M.; Wiseman, E.; Varady, K.A. Alternate Day Fasting Combined with a Low Carbohydrate Diet: Effect on Sleep Quality, Duration, Insomnia Severity and Risk of Obstructive Sleep Apnea in Adults with Obesity. Nutrients 2021, 13, 211. [Google Scholar] [CrossRef]
- Gabel, K.; Hoddy, K.K.; Burgess, H.J.; Varady, K.A. Effect of 8-h time-restricted feeding on sleep quality and duration in adults with obesity. Appl. Physiol. Nutr. Metab. 2019, 44, 903–906. [Google Scholar] [CrossRef]
- Cienfuegos, S.; Gabel, K.; Kalam, F.; Ezpeleta, M.; Pavlou, V.; Lin, S.; Wiseman, E.; Varady, K.A. The effect of 4-h versus 6-h time restricted feeding on sleep quality, duration, insomnia severity and obstructive sleep apnea in adults with obesity. Nutr. Health 2022, 28, 5–11. [Google Scholar] [CrossRef]
- Wilkinson, M.J.; Manoogian, E.N.C.; Zadourian, A.; Lo, H.; Fakhouri, S.; Shoghi, A.; Wang, X.; Fleischer, J.G.; Navlakha, S.; Panda, S.; et al. Ten-Hour Time-Restricted Eating Reduces Weight, Blood Pressure, and Atherogenic Lipids in Patients with Metabolic Syndrome. Cell Metab. 2020, 31, 92–104.e5. [Google Scholar] [CrossRef]
- Banno, M.; Harada, Y.; Taniguchi, M.; Tobita, R.; Tsujimoto, H.; Tsujimoto, Y.; Kataoka, Y.; Noda, A. Exercise can improve sleep quality: A systematic review and meta-analysis. PeerJ 2018, 6, e5172. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Liu, S.; Chen, X.J.; Yu, H.H.; Yang, Y.; Wang, W. Effects of Exercise on Sleep Quality and Insomnia in Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Front. Psychiatry 2021, 12, 664499. [Google Scholar] [CrossRef]
- Casagrande, M.; Forte, G.; Tambelli, R.; Favieri, F. The Coronavirus Pandemic: A Possible Model of the Direct and Indirect Impact of the Pandemic on Sleep Quality in Italians. Nat. Sci. Sleep 2021, 13, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Hirshkowitz, M.; Whiton, K.; Albert, S.M.; Alessi, C.; Bruni, O.; DonCarlos, L.; Hazen, N.; Herman, J.; Katz, E.S.; Kheirandish-Gozal, L.; et al. National Sleep Foundation’s sleep time duration recommendations: Methodology and results summary. Sleep Health 2015, 1, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Dolezal, B.A.; Neufeld, E.V.; Boland, D.M.; Martin, J.L.; Cooper, C.B. Interrelationship between Sleep and Exercise: A Systematic Review. Adv. Prev. Med. 2017, 2017, 1364387. [Google Scholar] [CrossRef]
- Peppard, P.E.; Young, T.; Palta, M.; Dempsey, J.; Skatrud, J. Longitudinal study of moderate weight change and sleep-disordered breathing. JAMA 2000, 284, 3015–3021. [Google Scholar] [CrossRef]


{kind=link}
| Combination | ADF | Exercise | Control | |||||
|---|---|---|---|---|---|---|---|---|
| Baseline | Month 3 | Baseline | Month 3 | Baseline | Month 3 | Baseline | Month 3 | |
| Demographics | ||||||||
| n | 20 | 20 | 20 | 19 | 20 | 15 | 20 | 20 |
| Age | 44 ± 3 | -- | 44 ± 3 | -- | 44 ± 3 | -- | 44 ± 3 | -- |
| Sex (Female/Male) | 17/3 | -- | 16/4 | -- | 16/4 | -- | 16/4 | -- |
| Body weight | ||||||||
| Body weight (kg) | 101 ± 4 | 97 ± 4 a | 96 ± 5 | 92 ± 4 a | 100 ± 5 | 99 ± 5 b | 100 ± 5 | 99 ± 5 b |
| Fat mass (kg) | 46 ± 3 | 43 ± 3 a | 40 ± 2 | 37 ± 3 a | 45 ± 3 | 43 ± 11 b | 45 ± 3 | 44 ± 11 b |
| Lean mass (kg) | 51 ± 3 | 51 ± 3 | 51 ± 2 | 49 ± 2 | 52 ± 3 | 51 ± 3 | 51 ± 2 | 50 ± 3 |
| Visceral fat (kg) | 1.6 ± 0.2 | 1.4 ± 0.2 | 1.6 ± 0.2 | 1.4 ± 0.1 | 1.7 ± 0.2 | 1.7 ± 0.2 | 1.7 ± 0.2 | 1.7 ± 0.2 |
| BMI (kg/m2) | 37 ± 5 | 35 ± 5 | 36 ± 8 | 34 ± 8 | 37 ± 6 | 36 ± 5 | 37 ± 5 | 37 ± 6 |
| Liver parameters | ||||||||
| IHTG (%) | 18 ± 2 | 13 ± 1 a | 16 ± 2 | 14 ± 1 a | 17 ± 2 | 16 ± 2 b | 17 ± 3 | 17 ± 3 b |
| Fibrosis score | 0.91 ± 0.08 | 0.75 ± 0.06 | 0.93 ± 0.13 | 0.85 ± 0.10 | 0.86 ± 0.08 | 0.80 ± 0.07 | 0.76 ± 0.05 | 0.75 ± 0.05 |
| Energy intake (kcal/d) | 2062 ± 287 | 1356 ± 162 a | 1940 ± 132 | 1285 ± 130 a | 1808 ± 170 | 1779 ± 175 b | 1810 ± 132 | 1833 ± 150 b |
| Steps/d | 7434 ± 943 | 7455 ± 942 | 7528 ± 1023 | 7041 ± 882 | 6754 ± 611 | 6936 ± 619 | 6497 ± 652 | 6004 ± 577 |
| PSQI | ||||||||
| Total score | 6.0 ± 0.7 | 5.6 ± 0.7 | 8.9 ± 1.0 | 7.5 ± 0.8 | 6.4 ± 0.6 | 6.7 ± 0.6 | 5.5 ± 0.7 | 4.6 ± 0.5 |
| Wake time (h:min) | 6:30 ± 0:15 | 7:15 ± 0:30 | 6:20 ± 0:25 | 6:00 ± 0:20 | 6:15 ± 0:15 | 6:30 ± 0:20 | 6:15 ± 0:15 | 6:10 ± 0:15 |
| Bedtime (h:min) | 22:50 ± 0:20 | 23:15 ± 0:20 | 22:40 + 0:20 | 22:40 ± 0:20 | 23:00 ± 0:15 | 22:45 ± 0:10 | 22:00 ± 0:50 | 22:40 ± 0:15 |
| Sleep duration (h) | 7.6 ± 1.2 | 8.0 ± 1.2 | 7.8 ± 1.7 | 7.3 ± 1.7 | 7.3 ± 1.0 | 7.7 ± 1.1 | 8.1 ± 1.4 | 7.5 ± 1.2 |
| Insomnia severity (ISI) | ||||||||
| Total score | 9.2 ± 1.5 | 6.4 ± 1.3 | 8.1 ± 1.2 | 6.4 ± 0.9 | 7.4 ± 0.9 | 6.7 ± 0.8 | 6.4 ± 1.1 | 4.9 ± 0.9 |
| Berlin questionnaire | ||||||||
| Risk obstructive sleep apnea | 30% | 21% | 75% | 65% | 40% | 38% | 75% | 56% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ezpeleta, M.; Gabel, K.; Cienfuegos, S.; Kalam, F.; Lin, S.; Pavlou, V.; Varady, K.A. Alternate-Day Fasting Combined with Exercise: Effect on Sleep in Adults with Obesity and NAFLD. Nutrients 2023, 15, 1398. https://doi.org/10.3390/nu15061398
Ezpeleta M, Gabel K, Cienfuegos S, Kalam F, Lin S, Pavlou V, Varady KA. Alternate-Day Fasting Combined with Exercise: Effect on Sleep in Adults with Obesity and NAFLD. Nutrients. 2023; 15(6):1398. https://doi.org/10.3390/nu15061398
Chicago/Turabian StyleEzpeleta, Mark, Kelsey Gabel, Sofia Cienfuegos, Faiza Kalam, Shuhao Lin, Vasiliki Pavlou, and Krista A. Varady. 2023. "Alternate-Day Fasting Combined with Exercise: Effect on Sleep in Adults with Obesity and NAFLD" Nutrients 15, no. 6: 1398. https://doi.org/10.3390/nu15061398
APA StyleEzpeleta, M., Gabel, K., Cienfuegos, S., Kalam, F., Lin, S., Pavlou, V., & Varady, K. A. (2023). Alternate-Day Fasting Combined with Exercise: Effect on Sleep in Adults with Obesity and NAFLD. Nutrients, 15(6), 1398. https://doi.org/10.3390/nu15061398