
Association between Intra- and Extra-Cellular Water Ratio Imbalance and Natriuretic Peptides in Patients Undergoing Hemodialysis
 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Data Collection
2.3. Assessment of Body Fluid Composition
2.4. Statistical Analyses
3. Results
3.1. Population Characteristics
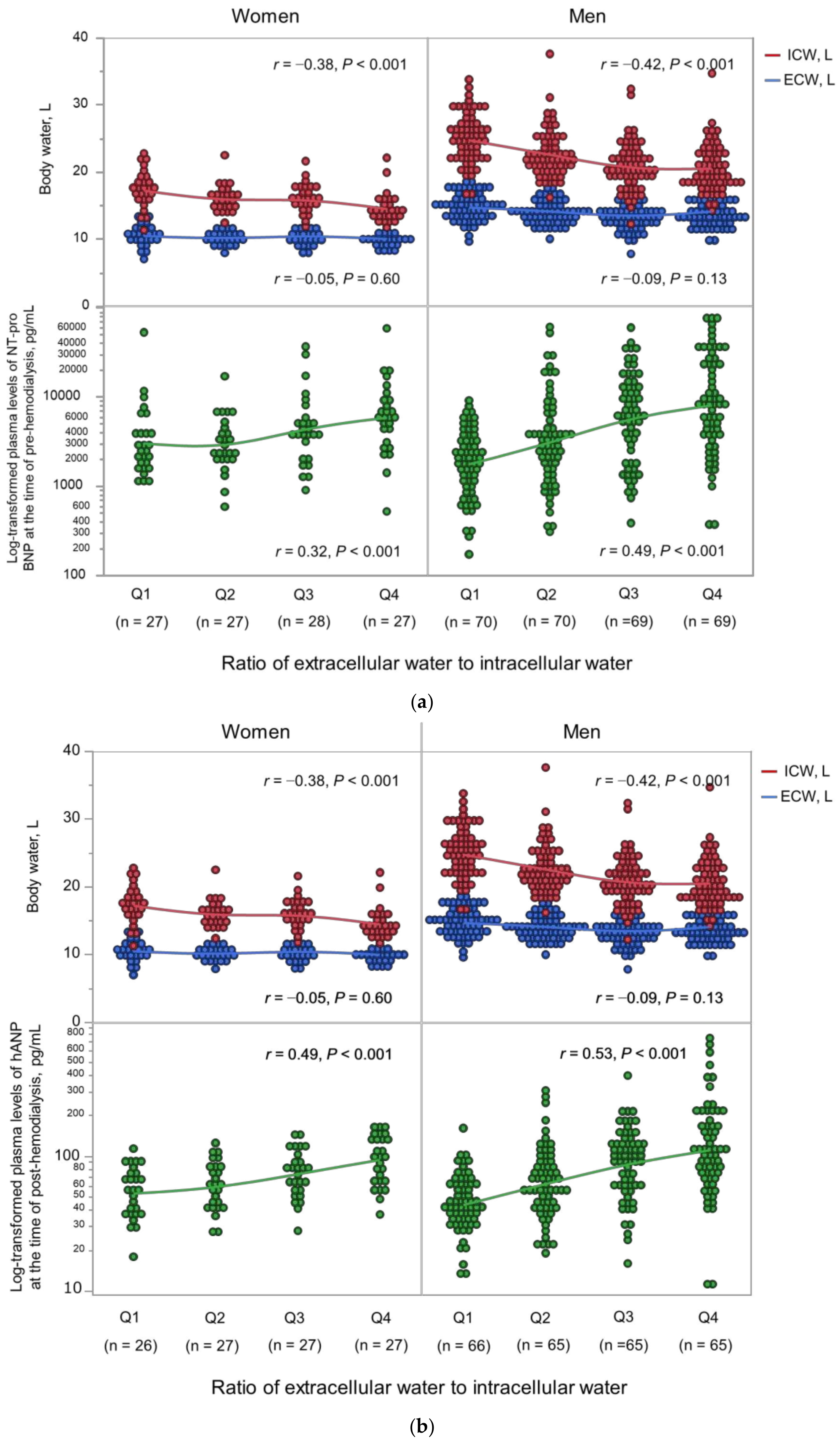
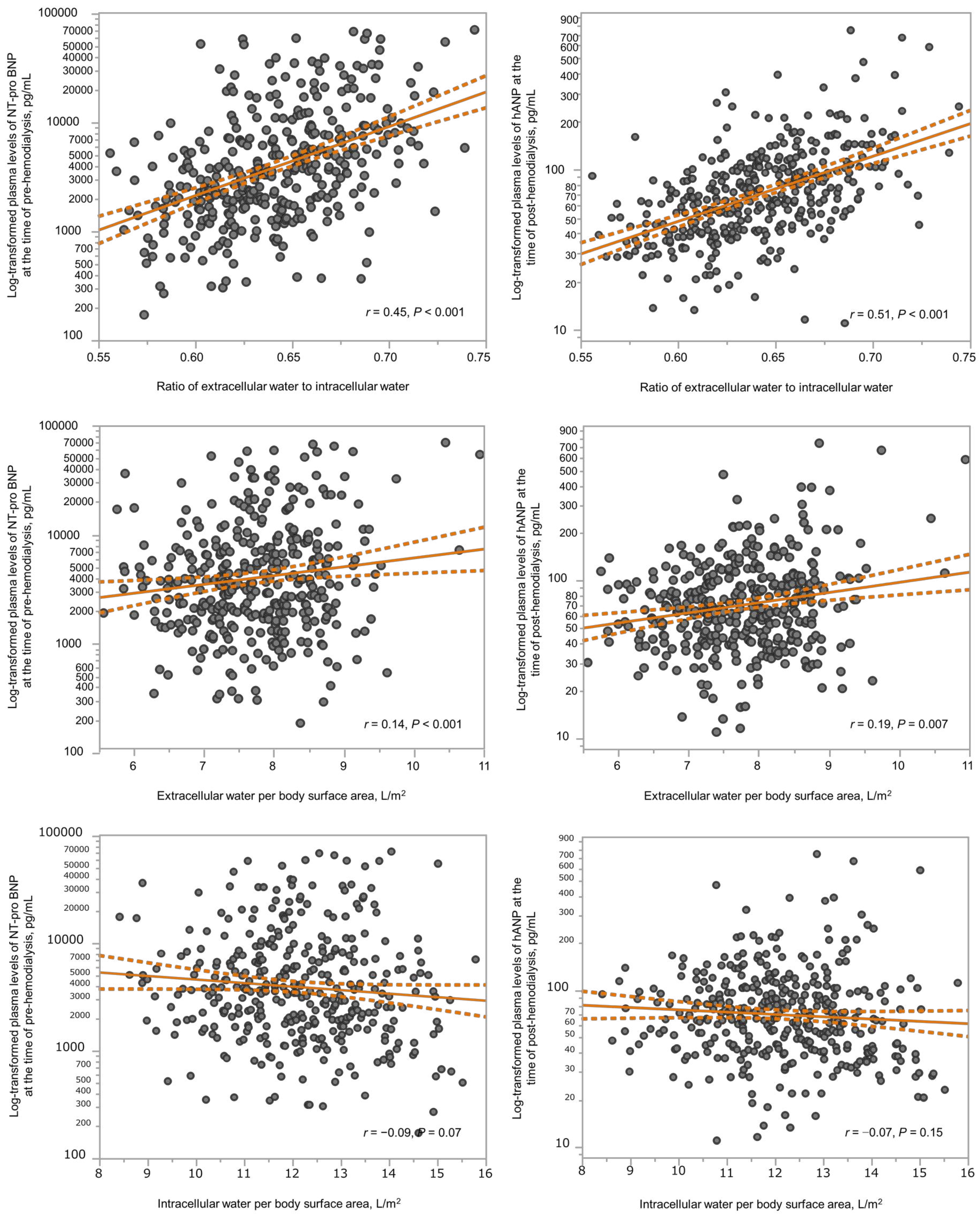
3.2. Association between Body Fluid Imbalance and Natriuretic Peptides
3.3. Association between Body Fluid Imbalance and Echocardiographic Findings
3.4. Body Fluid Imbalance Is an Independent Associated Factor for Natriuretic Peptides and LVMI
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dekker, M.J.E.; Marcelli, D.; Canaud, B.J.; Carioni, P.; Wang, Y.; Grassmann, A.; Konings, C.J.; Kotanko, P.; Leunissen, K.M.; Levin, N.W.; et al. MONDO Initiative. Impact of Fluid Status and Inflammation and their Interaction on Survival: A Study in an International Hemodialysis Patient Cohort. Kidney Int. 2017, 91, 1214–1223. [Google Scholar] [CrossRef] [PubMed]
- Zoccali, C.; Moissl, U.; Chazot, C.; Mallamaci, F.; Tripepi, G.; Arkossy, O.; Wabel, P.; Stuard, S. Chronic Fluid Overload and Mortality in ESRD. J. Am. Soc. Nephrol. 2017, 28, 2491–2497. [Google Scholar] [CrossRef] [PubMed]
- van der Sande, F.M.; van der Sande, F.M.; van de Wal-Visscher, E.R.; Stuard, S.; Moissl, U. Using Bioimpedance Spectroscopy to Assess Volume Status in Dialysis Patients. Blood Purif. 2020, 49, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Loutradis, C.; Sarafidis, P.A.; Ferro, C.J.; Zoccali, C. Volume Overload in Hemodialysis: Diagnosis, Cardiovascular Consequences, and Management. Nephrol. Dial. Transplant. 2021, 36, 2182–2193. [Google Scholar] [CrossRef] [PubMed]
- Sinha, A.D.; Agarwal, R. Can Chronic Volume Overload be Recognized and Prevented in Hemodialysis Patients? The Pitfalls of the Clinical Examination in Assessing Volume Status. Semin. Dial. 2009, 22, 480–482. [Google Scholar] [CrossRef] [PubMed]
- Sagayama, H.; Yoshimura, E.; Yamada, Y.; Tanaka, H. The Effects of Rapid Weight Loss and 3-H Recovery on Energy Expenditure, Carbohydrate, and Fat Oxidation in Boxing Athletes. J. Sports Med. Phys. Fitness 2019, 59, 1018. [Google Scholar] [CrossRef] [PubMed]
- Sagayama, H.; Shizuma, K.; Toguchi, M.; Mizuhara, H. Effect of the Health Tourism Weight Loss Programme on Body Composition and Health Outcomes in Healthy and Excess-Weight Adults. Br. J. Nutr. 2018, 119, 1133–1141. [Google Scholar] [CrossRef]
- Kondo, E.; Sagayama, H.; Yamada, Y.; Shiose, K. Energy Deficit Required for Rapid Weight Loss in Elite Collegiate Wrestlers. Nutrients 2018, 10, 536. [Google Scholar] [CrossRef] [PubMed]
- Sagayama, H.; Jikumaru, Y.; Hirata, A.; Yamada, Y.; Yoshimura, E.; Ichikawa, M.; Hatamoto, Y.; Ebine, N.; Kiyonaga, A.; Tanaka, H.; et al. Measurement of Body Composition in Response to a Short Period of Overfeeding. J. Physiol. Anthropol. 2014, 33, 29. [Google Scholar] [CrossRef]
- Moissl, U.; Arias-Guillén, M.; Wabel, P.; Fontseré, N.; Carrera, M.; Campistol, J.M.; Maduell, F. Bioimpedance-Guided Fluid Management in Hemodialysis Patients. Clin. J. Am. Soc. Nephrol. 2013, 8, 1575–1582. [Google Scholar] [CrossRef]
- Buchholz, A.C.; Bartok, C.; Schoeller, D.A. The Validity of Bioelectrical Impedance Models in Clinical Populations. Nutr. Clin. Pract. 2004, 19, 433–446. [Google Scholar] [CrossRef] [PubMed]
- Huan-Sheng, C.; Yeong-Chang, C.; Ming-Hsing, H.; Fan-Lieh, T.; Chu-Cheng, L.; Tsai-Kun, W.; Hung-Ping, C.; Sze-Hung, H.; Hsien-Chang, C.; Chia-Chen, L.; et al. Application of Bioimpedance Spectroscopy in Asian Dialysis Patients (ABISAD-III): A Randomized Controlled Trial for Clinical Outcomes. Int. Urol. Nephrol. 2016, 48, 1897–1909. [Google Scholar] [CrossRef]
- Ohashi, Y.; Joki, N.; Yamazaki, K.; Kawamura, T.; Tai, R.; Oguchi, H.; Yuasa, R.; Sakai, K. Changes in the Fluid Volume Balance between Intra- and Extracellular Water in a Sample of Japanese Adults Aged 15–88 Yr Old: A Cross-Sectional Study. Am. J. Physiol. Ren. Physiol. 2018, 314, F614–F622. [Google Scholar] [CrossRef] [PubMed]
- Dekker, M.J.E.; Konings, C.; Canaud, B.; van der Sande, F.M.; Stuard, S.; Raimann, J.G.; Öztürk, E.; Usvyat, L.; Kotanko, P.; Kooman, J.P. Interactions between Malnutrition, Inflammation, and Fluid Overload and their Associations with Survival in Prevalent Hemodialysis Patients. J. Ren. Nutr. 2018, 28, 435–444. [Google Scholar] [CrossRef]
- Antlanger, M.; Hecking, M.; Haidinger, M.; Werzowa, J.; Kovarik, J.J.; Paul, G.; Eigner, M.; Bonderman, D.; Hörl, W.H.; Säemann, M.D. Fluid Overload in Hemodialysis Patients: A Cross-Sectional Study to Determine its Association with Cardiac Biomarkers and Nutritional Status. BMC Nephrol. 2013, 14, 266. [Google Scholar] [CrossRef] [PubMed]
- Booth, J.; Pinney, J.; Davenport, A. N-Terminal proBNP—Marker of Cardiac Dysfunction, Fluid Overload, or Malnutrition in Hemodialysis Patients? Clin. J. Am. Soc. Nephrol. 2010, 5, 1036–1040. [Google Scholar] [CrossRef] [PubMed]
- Shinzato, T.; Shinzato, T.; Nakai, S.; Fujita, Y.; Takai, I.; Morita, H.; Nakane, K.; Maeda, K. Determination of Kt/V and Protein Catabolic Rate using Pre- and Postdialysis Blood Urea Nitrogen Concentrations. Nephron 1994, 67, 280–290. [Google Scholar] [CrossRef]
- Bouillanne, O.; Morineau, G.; Dupont, C.; Coulombel, I.; Vincent, J.P.; Nicolis, I.; Benazeth, S.; Cynober, L.; Aussel, C. Geriatric nutritional risk index: A new index for evaluating at-risk elderly medical patients. Am. J. Clin. Nutr. 2005, 82, 777–783. [Google Scholar] [CrossRef]
- Devereux, R.B.; Alonso, D.R.; Lutas, E.M.; Gottlieb, G.J.; Campo, E.; Sachs, I.; Reichek, N. Echocardiographic Assessment of Left Ventricular Hypertrophy: Comparison to Necropsy Findings. Am. J. Cardiol. 1986, 57, 450–458. [Google Scholar] [CrossRef]
- Hirakata, H.; Nitta, K.; Inaba, M.; Shoji, T.; Fujii, H.; Kobayashi, S.; Tabei, K.; Joki, N.; Hase, H.; Nishimura, M.; et al. Japanese Society for Dialysis Therapy guidelines for management of cardiovascular diseases in patients on chronic hemodialysis. Ther. Apher. Dial. 2012, 16, 387–435. [Google Scholar] [CrossRef]
- Eriguchi, M.; Tsuruya, K.; Lopes, M.; Bieber, B.; McCullough, K.; Pecoits-Filho, R.; Robinson, B.; Pisoni, R.; Kanda, E.; Iseki, K.; et al. Routinely Measured Cardiac Troponin I and N-terminal pro-B-type Natriuretic Peptide as Predictors of Mortality in Haemodialysis Patients. ESC Heart Fail. 2022, 9, 1138–1151. [Google Scholar] [CrossRef] [PubMed]
- Maraj, M.; Kuśnierz-Cabala, B.; Dumnicka, P.; Gala-Błądzińska, A.; Gawlik, K.; Pawlica-Gosiewska, D.; Ząbek-Adamska, A.; Mazur-Laskowska, M.; Ceranowicz, P.; Kuźniewski, M. Malnutrition, Inflammation, Atherosclerosis Syndrome (MIA) and Diet Recommendations among End-Stage Renal Disease Patients Treated with Maintenance Hemodialysis. Nutrients 2018, 10, 69. [Google Scholar] [CrossRef] [PubMed]
- Sarafidis, P.A.; Loutradis, C.; Karpetas, A.; Tzanis, G.; Bikos, A.; Raptis, V.; Syrgkanis, C.; Liakopoulos, V.; Papagianni, A.; Bakris, G.; et al. The Association of Interdialytic Blood Pressure Variability with Cardiovascular Events and all-Cause Mortality in Haemodialysis Patients. Nephrol. Dial. Transplant. 2019, 34, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Hecking, M.; Karaboyas, A.; Antlanger, M.; Saran, R.; Wizemann, V.; Chazot, C.; Rayner, H.; Hörl, W.H.; Pisoni, R.L.; Robinson, B.M. Significance of Interdialytic Weight Gain Versus Chronic Volume Overload: Consensus Opinion. Am. J. Nephrol. 2013, 38, 78–90. [Google Scholar] [CrossRef] [PubMed]
- Clarys, J.P.; Martin, A.D.; Marfell-Jones, M.J.; Janssens, V.; Caboor, D.; Drinkwater, D.T. Human Body Composition: A Review of Adult Dissection Data. Am. J. Hum. Biol. 1999, 11, 167–174. [Google Scholar] [CrossRef]
- Kyle, U.G.; Genton, L.; Hans, D.; Karsegard, L.; Slosman, D.O.; Pichard, C. Age-Related Differences in Fat-Free Mass, Skeletal Muscle, Body Cell Mass and Fat Mass between 18 and 94 Years. Eur. J. Clin. Nutr. 2001, 55, 663–672. [Google Scholar] [CrossRef]
- Nass, R.; Pezzoli, S.S.; Oliveri, M.C.; Patrie, J.T.; Harrell, F.E., Jr.; Clasey, J.L.; Heymsfield, S.B.; Bach, M.A.; Vance, M.L.; Thorner, M.O. Effects of an Oral Ghrelin Mimetic on Body Composition and Clinical Outcomes in Healthy Older Adults: A Randomized Trial. Ann. Intern. Med. 2008, 149, 601–611. [Google Scholar] [CrossRef]
- Yamada, Y.; Ikenaga, M.; Takeda, N.; Morimura, K.; Miyoshi, N.; Kiyonaga, A.; Kimura, M.; Higaki, Y.; Tanaka, H.; Nakagawa Study. Estimation of Thigh Muscle Cross-Sectional Area by Single- and Multifrequency Segmental Bioelectrical Impedance Analysis in the Elderly. J. Appl. Physiol. 2014, 116, 176–182. [Google Scholar] [CrossRef]
- Liu, M.H.; Wang, C.H.; Huang, Y.Y.; Tung, T.H.; Lee, C.M.; Yang, N.I.; Liu, P.C.; Cherng, W.J. Edema index established by a segmental multifrequency bioelectrical impedance analysis provides prognostic value in acute heart failure. J. Cardiovasc. Med. (Hagerstown) 2012, 13, 299–306. [Google Scholar] [CrossRef]
- Tsai, Y.C.; Tsai, H.J.; Lee, C.S.; Chiu, Y.W.; Kuo, H.T.; Lee, S.C.; Chen, T.H.; Kuo, M.C. The Interaction between N-Terminal Pro-Brain Natriuretic Peptide and Fluid Status in Adverse Clinical Outcomes of Late Stages of Chronic Kidney Disease. PLoS ONE 2018, 13, e0202733. [Google Scholar] [CrossRef]
- Stenberg, J.; Melin, J.; Lindberg, M.; Furuland, H. Brain Natriuretic Peptide Reflects Individual Variation in Hydration Status in Hemodialysis Patients. Hemodial. Int. 2019, 23, 402–413. [Google Scholar] [CrossRef] [PubMed]
- Das, S.R.; Drazner, M.H.; Dries, D.L.; Vega, G.L.; Stanek, H.G.; Abdullah, S.M.; Canham, R.M.; Chung, A.K.; Leonard, D.; Wians, F.H., Jr.; et al. Impact of Body Mass and Body Composition on Circulating Levels of Natriuretic Peptides: Results from the Dallas Heart Study. Circulation 2005, 112, 2163–2168. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Larson, M.G.; Levy, D.; Benjamin, E.J.; Leip, E.P.; Wilson, P.W.; Vasan, R.S. Impact of Obesity on Plasma Natriuretic Peptide Levels. Circulation 2004, 109, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Ikeda, M.; Honda, H.; Takahashi, K.; Shishido, K.; Shibata, T. N-Terminal Pro-B-Type Natriuretic Peptide as a Biomarker for Loss of Muscle Mass in Prevalent Hemodialysis Patients. PLoS ONE 2016, 11, e0166804. [Google Scholar] [CrossRef]
- Luce, M.; Bres, E.; Yi, D.; Pastural, M.; Granjon, S.; Szelag, J.C.; Laville, M.; Arkouche, W.; Bouchara, A.; Fouque, D.; et al. Natriuretic Peptides as Predictors of Protein-Energy Wasting in Hemodialysis Population. J. Ren. Nutr. 2022, 32, 234–242. [Google Scholar] [CrossRef]
- Agarwal, R. Body Mass Index-Mortality Paradox in Hemodialysis: Can it be explained by blood pressure? Hypertension 2011, 58, 1014–1020. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patients Characteristics | Post-Dialysis ECW/ICW Ratio | p | |||
|---|---|---|---|---|---|
| Quartile 1 Men < 0.611 (n = 66) Women < 0.627 (n = 26) | Quartile 2 Men 0.611–0.637 (n = 65) Women 0.628–0.649 (n = 27) | Quartile 3 Men 0.638–0.662 (n = 65) Women 0.650–0.673 (n = 27) | Quartile 4 Men 0.663 ≦ (n = 65) Women 0.674 ≦ (n = 27) | ||
| Age, years | 56 (47–66) | 66 (56–72) | 71 (64–77) | 73 (66–80) | <0.001 |
| Diabetes mellitus, n (%) | 36 (39) | 40 (43) | 46 (50) | 46 (50) | 0.37 |
| Dialysis vintage, months | 58 (4–409) | 67 (8–446) | 83 (7–537) | 73 (6–549) | 0.001 |
| Cardiovascular disease, n (%) | 18 (20) | 9 (10) | 22 (24) | 21 (23) | 0.06 |
| Body mass index, kg/m2 | 24 (22–28) | 22 (20–25) | 21 (19–25) | 21 (19–23) | <0.001 |
| Ultrafiltration volume. L | 3.6 (2.8–4.4) | 2.7 (2.2–3.6) | 3.0 (2.3–3.6) | 2.6 (2.1–3.2) | <0.001 |
| Ultrafiltration volume, % of body weight | 5.5 (4.6–6.1) | 4.9 (3.9–5.8) | 5.3 (4.1–6.2) | 4.8 (3.8–5.8) | 0.044 |
| Pre-dialysis systolic BP, mmHg | 142 (128–160) | 148 (131–159) | 148 (132–165) | 141 (125–160) | 0.38 |
| Post-dialysis systolic BP, mmHg | 128 (118–138) | 142 (120–155) | 142 (124–163) | 150 (130–165) | <0.001 |
| Pre-dialysis diastolic BP, mmHg | 82 (71–91) | 78 (68–84) | 76 (68–84) | 72 (65–80) | <0.001 |
| Post-dialysis diastolic BP, mmHg | 75 (70–86) | 78 (68–88) | 76 (66–85) | 75 (65–85) | 0.31 |
| Pulse rate, /min | 72 (64–81) | 70 (64–78) | 70 (62–77) | 68 (60–74) | <0.001 |
| Serum albumin, mg/dL | 3.7 (3.5–3.9) | 3.6 (3.5–3.8) | 3.5 (3.4–3.7) | 3.5 (3.2–3.7) | <0.001 |
| Blood urea nitrogen, mg/dL | 65 (54–73) | 58 (47–69) | 57 (48–68) | 55 (45–62) | <0.001 |
| Serum creatinine, mg/dL | 12.14 (10.48–13.85) | 10.87 (9.79–12.06) | 9.51 (8.74–10.94) | 8.70 (7.54–971) | <0.001 |
| Serum sodium, mEq/L | 139 (137–141) | 139 (137–140) | 139 (137–141) | 139 (138–141) | 0.36 |
| Serum potassium, mEq/L | 4.8 (4.3–5.5) | 4.9 (4.4–5.4) | 4.4 (4.4–5.2) | 4.3 (4.3–5.2) | 0.25 |
| Serum chloride, mEq/L | 103 (100–104) | 103 (102–105) | 104 (102–106) | 104 (102–106) | <0.001 |
| Serum calcium, mg/dL | 8.7 (8.4–8.9) | 8.7 (8.3–8.9) | 8.6 (8.2–8.9) | 8.5 (8.1–8.9) | 0.06 |
| Serum phosphorus, mg/dL | 6.0 (5.2–6.9) | 5.4 (4.8–6.1) | 5.4 (5.0–6.1) | 5.4 (4.6–6.1) | <0.001 |
| Total cholesterol, mg/dL | 170 (153–195) | 167 (143–196) | 163 (142–196) | 149 (129–175) | <0.001 |
| Triglyceride, mg/dL | 139 (92–218) | 107 (69–151) | 99 (63–140) | 82 (63–104) | <0.001 |
| Blood glucose, mg/dL | 109 (91–154) | 118 (96–159) | 116 (98–151) | 112 (99–144) | 0.63 |
| Uric acid, mg/dL | 8.5 (7.5–9.6) | 7.9 (7.3–85) | 7.4 (6.7–8.2) | 7.2 (6.4–8.1) | <0.001 |
| Hemoglobin, g/dL | 11.4 (10.9–12.1) | 11.1 (10.7–11.9) | 11.2 (10.6–11.7) | 10.9 (10.3–11.4) | <0.001 |
| C-reactive protein, mg/dL | 0.13 (0.04–026) | 0.09 (0.04–0.27) | 0.09 (0.05–0.22) | 0.16 (0.06–0.40) | 0.046 |
| Intact PTH, pg/mL | 172 (111–226) | 142 (92–226) | 147 (88–210) | 164 (104–204) | 0.72 |
| β2MG, mg/L | 27 (24–29) | 27 (24–30) | 26 (23–32) | 26 (23–32) | 0.25 |
| Kt/Vurea | 1.73 (1.56–1.97) | 1.87 (1.67–2.13) | 1.85 (1.70–2.09) | 1.80 (1.68–2.05) | 0.06 |
| Geriatric nutritional risk index | 106 (95–109) | 96 (91–104) | 94 (89–100) | 92 (87–98) | <0.001 |
| NT-proBNP, pg/mL | 1995 (1210–3678) | 2810 (1795–5338) | 5010 (2080–11,000) | 6670 (3453–17,525) | <0.001 |
| hANP, pg/mL | 43 (34–66) | 58 (42–84) | 88 (59–118) | 103 (67–153) | <0.001 |
| CTR in men (n = 265), % | 49.3 ± 4.7 | 49.3 ± 5.6 | 50.7 ± 4.2 | 51.6 ± 4.9 | 0.006 |
| CTR in women (n = 107), % | 51.0 ± 4.0 | 52.2 ± 3.2 | 52.6 ± 4.5 | 54.6 ± 4.5 | <0.001 |
| Echocardiographic Findings | Post-Dialysis Extracellular Water to Intracellular Water Ratio | p | |||
|---|---|---|---|---|---|
| Quartile 1 Men < 0.611 (n = 66) Women < 0.628 (n = 27) | Quartile 2 Men 0.611–0.637 (n = 67) Women 0.628–0.649 (n = 26) | Quartile 3 Men 0.638–0.662 (n = 66) Women 0.650–0.673 (n = 27) | Quartile 4 Men 0.663 ≦ (n = 66) Women 0.674 ≦ (n = 27) | ||
| LAD, mm | 36 (33 to 38) | 37 (34 to 42) | 38 (34 to 42) | 38 (35 to 43) | 0.002 |
| LVDd, mm | 46.4 ± 7.3 | 45.2 ± 6.4 | 45.8 ± 7.1 | 45.2 ± 6.5 | 0.036 |
| LVDs, mm | 30.2 ± 5.8 | 29.5 ± 5.5 | 30.1± 6.1 | 30.0 ± 6.8 | 0.31 |
| PWT, mm | 10.5 (9.3 to 11.7) | 10.5 (9.1 to 12.0) | 11.0 (10.0 to 12.0) | 11.2 (9.6 to 12.8) | 0.005 |
| IVST, mm | 10.7 ± 2.2 | 11.0 ± 2.1 | 11.1 ± 2.0 | 11.5 ± 2.2 | 0.002 |
| EF | 64 (59 to 70) | 64 (60 to 70) | 63 (56 to 70) | 64 (59 to 69) | 0.58 |
| LVMI, g/m2 | 99 (79 to 127) | 102 (79 to 128) | 110 (95 to 132) | 115 (96 to 137) | <0.001 |
| Variables | Unstandardized B (95% CI) | Standardized β | p |
|---|---|---|---|
| Pre-dialysis Log10NT-proBNP | |||
| Unadjusted | 6.34 (5.05, 7.63) | 0.45 | <0.001 |
| Age and gender-adjusted | 6.15 (4.66, 7.63) | 0.44 | <0.001 |
| Multivariable-adjusted 1 | 4.66 (2.90, 6.42) | 0.34 | <0.001 |
| Post-dialysis Log10hANP | |||
| Unadjusted | 4.08 (3.38, 4.78) | 0.51 | <0.001 |
| Age and gender-adjusted | 3.98 (3.17, 4.78) | 0.50 | <0.001 |
| Multivariable-adjusted 2 | 3.15 (2.19, 4.10) | 0.40 | <0.001 |
| LVMI inechocardiography | |||
| Unadjusted | 163 (69, 308) | 0.17 | <0.001 |
| Age and gender-adjusted | 199 (91, 299) | 0.21 | <0.001 |
| Multivariable-adjusted 3 | 183 (70, 295) | 0.20 | 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nakayama, Y.; Yamada, Y.; Ishii, S.; Hitaka, M.; Yamazaki, K.; Masai, M.; Joki, N.; Sakai, K.; Ohashi, Y. Association between Intra- and Extra-Cellular Water Ratio Imbalance and Natriuretic Peptides in Patients Undergoing Hemodialysis. Nutrients 2023, 15, 1274. https://doi.org/10.3390/nu15051274
Nakayama Y, Yamada Y, Ishii S, Hitaka M, Yamazaki K, Masai M, Joki N, Sakai K, Ohashi Y. Association between Intra- and Extra-Cellular Water Ratio Imbalance and Natriuretic Peptides in Patients Undergoing Hemodialysis. Nutrients. 2023; 15(5):1274. https://doi.org/10.3390/nu15051274
Chicago/Turabian StyleNakayama, Yui, Yosuke Yamada, Shingo Ishii, Mai Hitaka, Keisuke Yamazaki, Motoyuki Masai, Nobuhiko Joki, Ken Sakai, and Yasushi Ohashi. 2023. "Association between Intra- and Extra-Cellular Water Ratio Imbalance and Natriuretic Peptides in Patients Undergoing Hemodialysis" Nutrients 15, no. 5: 1274. https://doi.org/10.3390/nu15051274
APA StyleNakayama, Y., Yamada, Y., Ishii, S., Hitaka, M., Yamazaki, K., Masai, M., Joki, N., Sakai, K., & Ohashi, Y. (2023). Association between Intra- and Extra-Cellular Water Ratio Imbalance and Natriuretic Peptides in Patients Undergoing Hemodialysis. Nutrients, 15(5), 1274. https://doi.org/10.3390/nu15051274