
Investigating the Dietary Intake Using the CyFFQ Semi-Quantitative Food Frequency Questionnaire in Cypriot Huntington’s Disease Patients

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
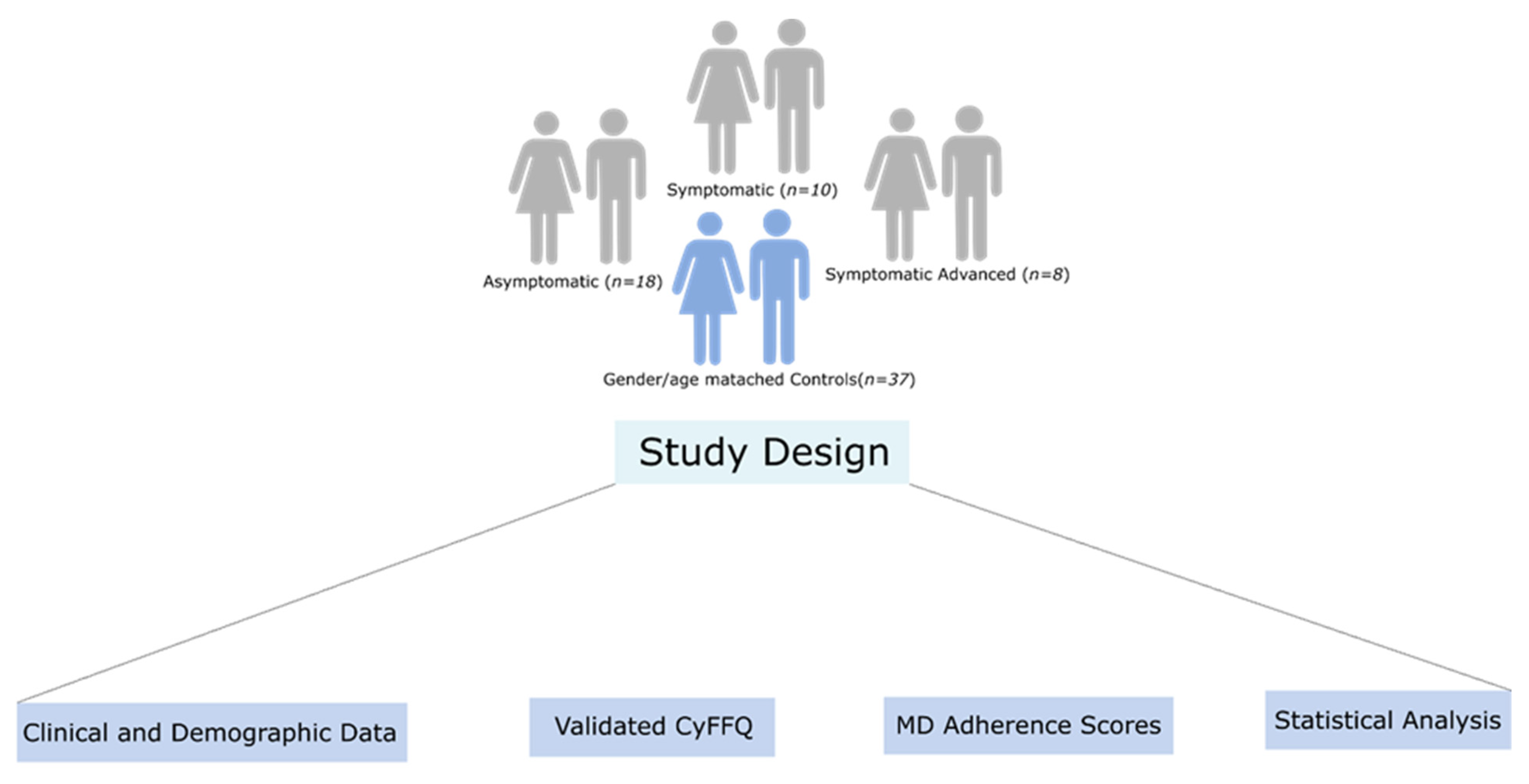
2.1. Study Design
- Demographics: sex, date of birth, birthplace and current city of residence, parents’ birthplace, family status (single, married, divorced or widowed) and occupation;
- Medical and family history of HD and their family as well as presence and age of HD symptoms family members diagnosed with HD and other chronic illnesses for patients and controls;
- Age of onset and symptoms, number of CAG repeat and current medical treatment;
- Anthropometrics: weight and height at least a year prior to HD diagnosis;
- Lifestyle, such as smoking, current smoking, physical exercise and hobbies;
- Medical history, CAG repeat counts, treatments and other co-morbidities were also obtained from the patients’ medical records, or via self-reporting for controls.
2.2. Huntington’s Disease Assessment
2.3. Food Frequency Questionnaire
2.4. Presentation of FFQ Data
2.5. Comparison of Intake with Dietary Reference Intakes
2.6. MD Adherence Scores
2.7. Statistical Analysis
3. Results
3.1. Demographic and Anthropometric Characteristics of Participants
3.2. Energy Intake, EA, Macronutrients and Micronutrients
3.3. MD Adherence Scores Using the MedDiet Score and the MEDAS Score
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Walker, F.O. Huntington’s Disease. Lancet 2007, 369, 218–228. [Google Scholar] [CrossRef]
- Johri, A.; Beal, M.F. Mitochondrial Dysfunction in Neurodegenerative Diseases. J. Pharmacol. Exp. Ther. 2012, 342, 619–630. [Google Scholar] [CrossRef] [PubMed]
- Roos, R.A.C. Huntington’s Disease: A Clinical Review. Orphanet J. Rare Dis. 2010, 5, 40. [Google Scholar] [CrossRef] [PubMed]
- Nance, M.A.; Myers, R.H. Juvenile Onset Huntington’s Disease—Clinical and Research Perspectives. MRDD Res. Rev. 2001, 7, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Manoharan, S.; Guillemin, G.J.; Abiramasundari, R.S.; Essa, M.M.; Akbar, M.; Akbar, M.D. The Role of Reactive Oxygen Species in the Pathogenesis of Alzheimer’s Disease, Parkinson’s Disease, and Huntington’s Disease: A Mini Review. Oxidative Med. Cell. Longev. 2016, 2016, 8590578. [Google Scholar] [CrossRef]
- Demetriou, C.A.; Heraclides, A.; Salafori, C.; Tanteles, G.A.; Christodoulou, K.; Christou, Y.; Zamba-Papanicolaou, E. Epidemiology of Huntington Disease in Cyprus: A 20-Year Retrospective Study. Clin. Genet. 2018, 93, 656–664. [Google Scholar] [CrossRef]
- Żukiewicz-Sobczak, W.; Król, R.; Wróblewska, P.; Piątek, J.; Gibas-Dorna, M. Huntington Disease—Principles and Practice of Nutritional Management. Neurol. Neurochir. Pol. 2014, 48, 442–448. [Google Scholar] [CrossRef]
- Brotherton, A.; Campos, L.; Rowell, A.; Zoia, V.; Simpson, S.A.; Rae, D. Nutritional Management of Individuals with Huntington’s Disease: Nutritional Guidelines. Neurodegener. Dis. Manag. 2012, 2, 33–43. [Google Scholar] [CrossRef]
- Russell, R.D.; Black, L.J.; Begley, A. Nutrition Education Programs for Adults with Neurological Diseases Are Lacking: A Scoping Review. Nutrients 2022, 14, 1577. [Google Scholar] [CrossRef]
- Christodoulou, C.C.; Demetriou, C.A.; Zamba-papanicolaou, E. Dietary Intake, Mediterranean Diet Adherence and Caloric Intake in Huntington’s Disease: A Review. Nutrients 2020, 12, 2946. [Google Scholar] [CrossRef]
- Marder, K.; Zhao, H.; Eberly, S.; Tanner, C.M.; Oakes, D.; Shoulson, I. Dietary Intake in Adults at Risk for Huntington Disease. Neurology 2009, 73, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Mochel, F.; Charles, P.; Seguin, F.; Barritault, J.; Coussieu, C.; Perin, L.; Le Bouc, Y.; Gervais, C.; Carcelain, G.; Vassault, A.; et al. Early Energy Deficit in Huntingdon Disease: Identification of a Plasma Biomarker Traceable during Disease Progression. PLoS ONE 2007, 2, e647. [Google Scholar] [CrossRef] [PubMed]
- Farooqui, A.A.; Farooqui, T.; Nance, M.A.; Myers, R.H.; Philippou, E.; Demetriou, C.A.; Loucaides, G.; Solomonidou, N.; Critselis, E.; Franquesa, M.; et al. Mediterranean Diet and Cardiodiabesity: A Systematic Review through Evidence-Based Answers to Key Clinical Questions. Curr. Opin. Biotechnol. 2019, 11, 912–921. [Google Scholar] [CrossRef]
- Sofi, F.; Macchi, C.; Casini, A. Mediterranean Diet and Minimizing Neurodegeneration. Curr. Nutr. Rep. 2013, 2, 75–80. [Google Scholar] [CrossRef]
- Farooqui, A.A.; Farooqui, T. Effects of Mediterranean Diet Components on Neurodegenerative Diseases. In Role of the Mediterranean Diet in the Brain and Neurodegenerative Diseases; Elsevier: Amsterdam, The Netherlands, 2018; pp. 1–16. [Google Scholar]
- Rivadeneyra, J.; Cubo, E.; Gil, C.; Calvo, S.; Mariscal, N.; Martínez, A. Factors Associated with Mediterranean Diet Adherence in Huntington’s Disease. Clin. Nutr. ESPEN 2016, 12, e7–e13. [Google Scholar] [CrossRef]
- Philippou, E.; Demetriou, C.A.; Loucaides, G.; Solomonidou, N.; Critselis, E. Relative Validity and Reproducibility of the CyFFQ Semi-Quantitative Food Frequency Questionnaire for Assessing Dietary Intake in Cypriot Adults. J. Hum. Nutr. Diet. 2022, 36, 139–153. [Google Scholar] [CrossRef]
- Huntington Study Group Unified. Huntington’s Disease Rating Scale: Reliability and Consistency. Mov. Disord. 1996, 11, 136–142. [Google Scholar] [CrossRef]
- Otten, J.J.; Hellwig, J.P.; Linda, D. Dietary DRI Reference Intakes; The National Academic Press: Washington, DC, USA, 2006; ISBN 030965646X. [Google Scholar]
- Panagiotakos, D.B.; Pitsavos, C.; Arvaniti, F.; Stefanadis, C. Adherence to the Mediterranean Food Pattern Predicts the Prevalence of Hypertension, Hypercholesterolemia, Diabetes and Obesity, among Healthy Adults; the Accuracy of the MedDietScore. Prev. Med. 2007, 44, 335–340. [Google Scholar] [CrossRef]
- Martínez-González, M.A.; García-Arellano, A.; Toledo, E.; Salas-Salvadó, J.; Buil-Cosiales, P.; Corella, D.; Covas, M.I.; Schröder, H.; Arós, F.; Gómez-Gracia, E.; et al. A 14-Item Mediterranean Diet Assessment Tool and Obesity Indexes among High-Risk Subjects: The PREDIMED Trial. PLoS ONE 2012, 7, e43134. [Google Scholar] [CrossRef]
- Puri, B.K.; Bydder, G.M.; Manku, M.S.; Clarke, A.; Waldman, A.D.; Beckmann, C.F. Reduction in Cerebral Atrophy Associated with Ethyl-Eicosapentaenoic Acid Treatment in Patients with Huntington’s Disease. J. Int. Med. Res. 2008, 36, 896–905. [Google Scholar] [CrossRef]
- Puri, B.K.; Leavitt, B.R.; Hayden, M.R.; Ross, C.A.; Rosenblatt, A.; Greenamyre, J.T.; Hersch, S.; Vaddadi, K.S.; Sword, A.; Horrobin, D.F.; et al. Ethyl-EPA in Huntington Disease. Neurology 2005, 65, 286–292. [Google Scholar] [CrossRef] [PubMed]
- Goetz, C.G.; Tanner, C.M.; Cohen, J.A.; Thelen, J.A.; Carroll, V.S.; Klawans, H.L.; Fariello, R.G. L-Acetyl-Carnitine in Huntington Disease: Double Blind Placebo Controlled Cross-over Study of Drug Effects on Movement Disorder and Dementia. Mov. Disord. 1990, 5, 263–265. [Google Scholar] [CrossRef]
- Auinger, P.; Kieburtz, K.; McDermott, M.P. The Relationship between Uric Acid Levels and Huntington’s Disease Progression. Mov. Disord. 2010, 25, 224–228. [Google Scholar] [CrossRef] [PubMed]
- Trejo, A.; Boll, M.-C.; Alonso, M.E.; Ochoa, A.; Velásquez, L. Use of Oral Nutritional Supplements in Patients with Huntington’s Disease. Nutrition 2005, 21, 889–894. [Google Scholar] [CrossRef] [PubMed]
- Cubo, E.; Rivadeneyra, J.; Armesto, D.; Mariscal, N.; Martinez, A.; Camara, R.J.; Martínez, D.; Ramos, M.A.; Pastor, B.V.; Párez, R.; et al. Relationship between Nutritional Status and the Severity of Huntington’s Disease. A Spanish Multicenter Dietary Intake Study. J. Huntingt. Dis. 2015, 4, 75–85. [Google Scholar] [CrossRef]
- Mochel, F.; Haller, R.G. Energy Deficit in Huntington Disease: Why It Matters. J. Clin. Investig. 2011, 121, 493–499. [Google Scholar] [CrossRef]
- Sarikaya, B. Unbalanced Distribution of Food. Soc. Regist. 2017, 1, 199–208. [Google Scholar] [CrossRef]
- Skoczek-Rubińska, A.; Bajerska, J. The Consumption of Energy Dense Snacks and Some Contextual Factors of Snacking May Contribute to Higher Energy Intake and Body Weight in Adults. Nutr. Res. 2021, 96, 20–36. [Google Scholar] [CrossRef]


{kind=link}
| Cases (n = 36) | Controls (n = 37) | ||||
|---|---|---|---|---|---|
| Median | IQR | Median | IQR | p-Value | |
| Energy (kcal/day) | 4592 | 3376 | 2488 | 1917 | 0.0002 * |
| Protein (% energy) | 17.3 | 3.7 | 17.0 | 4.0 | 0.675 |
| Fat (% energy) | 41.8 | 7.8 | 42.4 | 10.9 | 0.651 |
| CHO (% energy) | 39.0 | 6.7 | 36.6 | 8.5 | 0.426 |
| Starch (% energy) | 13.5 | 6.6 | 12.2 | 4.6 | 0.284 |
| Tot sug (% energy) | 15.2 | 8.0 | 15.6 | 8.3 | 0.487 |
| Sat fats (% energy) | 13.5 | 3.6 | 13.4 | 3.2 | 0.903 |
| MUFA (% energy) | 15.0 | 4.1 | 15.5 | 5.7 | 0.089 |
| PUFA (% energy) | 6.4 | 2.8 | 6.4 | 1.7 | 0.304 |
| Trans fats (% energy) | 0.4 | 0.2 | 0.4 | 0.2 | 0.643 |
| NSP (% energy) | 1.1 | 0.6 | 1.6 | 0.8 | 0.034 * |
| Alcohol (% energy) | 2.1 | 7.4 | 2.6 | 11.3 | 0.441 |
| Cholesterol (mg/1000 kcal) | 132.6 | 31.7 | 106.8 | 58.8 | 0.095 |
| NSP (g/1000 kcal) | 5.5 | 3.2 | 8.1 | 4.1 | 0.034 * |
| Fibre (g/1000 kcal) | 6.9 | 4.1 | 9.9 | 5.5 | 0.028 * |
| Sodium (mg/1000 kcal) | 990.9 | 269.3 | 915.9 | 344.0 | 0.142 |
| Potassium (mg/1000 kcal) | 1170.1 | 314.1 | 1377.8 | 292.0 | 0.053 |
| Calcium (mg/1000 kcal) | 372.1 | 134.4 | 402.6 | 159.4 | 0.274 |
| Magnesium (mg/1000 kcal) | 130.2 | 35.9 | 141.4 | 33.7 | 0.145 |
| Phosphorus (mg/1000 kcal) | 571.2 | 133.6 | 619.8 | 158.3 | 0.127 |
| Iron (mg/1000 kcal) | 5.2 | 1.6 | 5.7 | 2.8 | 0.185 |
| Zinc (mg/1000 kcal) | 4.2 | 1.2 | 4.0 | 1.1 | 0.956 |
| Selenium (ug/1000 kcal) | 18.8 | 7.1 | 16.8 | 6.4 | 0.125 |
| Vit D (ug/1000 kcal) | 0.7 | 0.2 | 0.7 | 0.5 | 0.947 |
| Vit E (mg/1000 kcal) | 3.6 | 2.1 | 3.4 | 3.1 | 0.956 |
| Thiamin (mg/1000 kcal) | 0.6 | 0.2 | 0.7 | 0.2 | 0.401 |
| Riboflavin (mg/1000 kcal) | 0.6 | 0.2 | 0.6 | 0.3 | 0.508 |
| Vit B6 (mg/1000 kcal) | 0.7 | 0.4 | 0.8 | 0.3 | 1.000 |
| Vit B12 (ug/1000 kcal) | 1.6 | 0.6 | 1.4 | 0.4 | 0.216 |
| Trypto60 (mg/1000 kcal) | 6.2 | 2.6 | 5.7 | 1.7 | 0.182 |
| Folate (ug/1000 kcal) | 64.7 | 29.8 | 79.5 | 33.0 | 0.077 |
| Pantothenic acid (ug/1000 kcal) | 2.1 | 0.5 | 2.0 | 0.5 | 0.920 |
| Vit C (mg/1000 kcal) | 27.1 | 30.1 | 34.5 | 36.4 | 0.145 |
| Asymptomatic (n = 18) | Controls (n = 37) | ||||
|---|---|---|---|---|---|
| Median | IQR | Median | IQR | p-Value | |
| Energy (kcal/day) | 3751 | 1894 | 2488 | 1917 | 0.028 * |
| Protein (% energy) | 18.8 | 3.1 | 17.0 | 4.0 | 0.184 |
| Fat (% energy) | 42.8 | 6.4 | 42.4 | 10.9 | 0.628 |
| CHO (% energy) | 39.0 | 8.2 | 36.6 | 8.5 | 0.900 |
| Starch (% energy) | 12.5 | 7.0 | 12.2 | 4.6 | 0.698 |
| Tot sug (% energy) | 16.1 | 5.8 | 15.6 | 8.3 | 0.885 |
| Sat fats (% energy) | 14.5 | 3.8 | 13.4 | 3.2 | 0.419 |
| MUFA (% energy) | 15.7 | 2.9 | 15.5 | 5.7 | 0.590 |
| PUFA (% energy) | 7.5 | 2.6 | 6.4 | 1.7 | 0.032 * |
| Trans fats (% energy) | 0.4 | 0.2 | 0.4 | 0.2 | 0.332 |
| NSP (% energy) | 1.3 | 0.6 | 1.6 | 0.8 | 0.156 |
| Alcohol (% energy) | 1.5 | 4.7 | 2.6 | 11.3 | 0.340 |
| Cholesterol (mg/1000 kcal) | 135.8 | 55.4 | 106.8 | 58.8 | 0.023 * |
| NSP (g/1000 kcal) | 6.4 | 3.2 | 8.1 | 4.1 | 0.156 |
| Fibre (g/1000 kcal) | 8.0 | 4.3 | 9.9 | 5.5 | 0.161 |
| Sodium (mg/1000 kcal) | 1028.6 | 290.2 | 915.9 | 344.0 | 0.044 * |
| Potassium (mg/1000 kcal) | 1219.2 | 450.2 | 1377.8 | 292.0 | 0.451 |
| Calcium (mg/1000 kcal) | 410.2 | 138.4 | 402.6 | 159.4 | 0.628 |
| Magnesium (mg/1000 kcal) | 132.8 | 32.3 | 141.4 | 33.7 | 0.928 |
| Phosphorus (mg/1000 kcal) | 615.8 | 141.9 | 619.8 | 158.3 | 0.578 |
| Iron (mg/1000 kcal) | 5.1 | 1.6 | 5.7 | 2.8 | 0.332 |
| Zinc (mg/1000 kcal) | 4.4 | 0.6 | 4.0 | 1.1 | 0.151 |
| Manganese (mg/1000 kcal) | 0.9 | 0.4 | 0.9 | 0.4 | 0.900 |
| Selenium (ug/1000 kcal) | 19.7 | 6.8 | 16.9 | 6.4 | 0.023 * |
| Vit D (ug/1000 kcal) | 0.8 | 0.4 | 0.7 | 0.5 | 0.281 |
| Vit E (mg/1000 kcal) | 4.1 | 2.7 | 3.4 | 3.1 | 0.409 |
| Thiamin (mg/1000 kcal) | 0.7 | 0.3 | 0.7 | 0.2 | 0.928 |
| Riboflavin (mg/1000 kcal) | 0.7 | 0.2 | 0.6 | 0.3 | 0.389 |
| Vit B6 (mg/1000 kcal) | 0.7 | 0.3 | 0.8 | 0.3 | 0.857 |
| Vit B12 (ug/1000 kcal) | 1.7 | 0.3 | 1.4 | 0.4 | 0.052 |
| Trypto60 (mg/1000 kcal) | 6.8 | 2.1 | 5.7 | 1.7 | 0.007 * |
| Folate (ug/1000 kcal) | 68.2 | 30.6 | 79.5 | 33.0 | 0.131 |
| Pantothenic acid (ug/1000 kcal) | 2.2 | 0.6 | 2.0 | 0.5 | 0.167 |
| Vit C (mg/1000 kcal) | 21.8 | 49.9 | 34.5 | 36.4 | 0.136 |
| Symptomatic (n = 18) | Controls (n = 37) | ||||
|---|---|---|---|---|---|
| Median | IQR | Median | IQR | p-Value | |
| Energy (kcal/day) | 5511 | 2907 | 2488 | 1917 | 0.0001 * |
| Protein (% energy) | 16.5 | 4.2 | 17.0 | 4.0 | 0.518 |
| Fat (% energy) | 39.4 | 6.8 | 42.4 | 10.9 | 0.222 |
| CHO (% energy) | 38.8 | 5.5 | 36.6 | 8.5 | 0.243 |
| Starch (% energy) | 13.5 | 5.3 | 12.2 | 4.6 | 0.178 |
| Tot sug (% energy) | 14.6 | 8.5 | 15.6 | 8.3 | 0.323 |
| Sat fats (% energy) | 13.0 | 4.5 | 13.4 | 3.2 | 0.541 |
| MUFA (% energy) | 13.4 | 5.2 | 15.5 | 5.7 | 0.026 * |
| PUFA (% energy) | 6.0 | 2.4 | 6.4 | 1.7 | 0.640 |
| Trans fats (% energy) | 0.4 | 0.2 | 0.4 | 0.2 | 0.829 |
| Fibre (% energy) | 1.3 | 0.7 | 1.9 | 1.1 | 0.031 * |
| Alcohol (% energy) | 3.5 | 9.8 | 2.6 | 11.3 | 0.766 |
| Cholesterol (g/1000 kcal) | 125.6 | 35.6 | 106.9 | 58.8 | 0.653 |
| NSP (g/1000 kcal) | 5.5 | 2.9 | 8.1 | 4.1 | 0.042 * |
| Fibre (g/1000 kcal) | 6.7 | 3.7 | 9.9 | 5.5 | 0.031 * |
| Sodium (mg/1000 kcal) | 968.7 | 270.2 | 916.0 | 344.0 | 0.706 |
| Potassium (mg/1000 kcal) | 1155.7 | 185.3 | 1377.8 | 291.9 | 0.017 * |
| Calcium (mg/1000 kcal) | 348.2 | 99.3 | 402.6 | 159.4 | 0.023 * |
| Magnesium (mg/1000 kcal) | 115.8 | 38.1 | 141.7 | 33.7 | 0.022 * |
| Phosphorus (mg/1000 kcal) | 503.8 | 84.2 | 619.8 | 158.4 | 0.002 * |
| Iron (mg/1000 kcal) | 5.3 | 1.5 | 5.6 | 2.7 | 0.236 |
| Zinc (mg/1000 kcal) | 3.5 | 1.3 | 4.0 | 1.1 | 0.127 |
| Manganese (mg/1000 kcal) | 0.8 | 0.5 | 0.9 | 0.4 | 0.222 |
| Vit D (ug/1000 kcal) | 0.7 | 0.3 | 0.7 | 0.5 | 0.236 |
| Vit E (mg/1000 kcal) | 2.8 | 2.1 | 3.4 | 3.1 | 0.360 |
| Thiamin (mg/1000 kcal) | 0.6 | 0.2 | 0.7 | 0.2 | 0.146 |
| Riboflavin (mg/1000 kcal) | 0.5 | 0.1 | 0.6 | 0.3 | 0.052 |
| Vit B6 (mg/1000 kcal) | 0.7 | 0.5 | 0.8 | 0.3 | 0.857 |
| Vit B12 (ug/1000 kcal) | 1.3 | 0.8 | 1.4 | 0.4 | 0.942 |
| Folate (ug/1000 kcal) | 63.9 | 26.8 | 79.5 | 33.0 | 0.172 |
| Pantothenic acid (ug/1000 kcal) | 1.9 | 0.6 | 2.041 | 0.5 | 0.222 |
| Vit C (mg/1000 kcal) | 31.2 | 26.6 | 34.5 | 36.4 | 0.379 |
| Cases (n = 36) | Controls (n = 37) | |||||||
|---|---|---|---|---|---|---|---|---|
| Recommendation * | % within Recommendation | Lower 95% CI | Upper 95% CI | % within Recommendation | Lower 95% CI | Upper 95% CI | p-Value (Fisher’s Exact Test) | |
| Energy (kcal/day) | Males: 2500 kcal/day Females: 2000 kcal/day | 8.3 | 2.6 | 23.6 | 29.7 | 16.9 | 46.7 | 0.035 * |
| Protein (% energy) | 10–35% of E | 97.2 | 81.7 | 99.6 | 97.3 | 82.2 | 99.6 | 1.000 |
| Total fat (%energy) | 20–35% of E | 11.1 | 4.1 | 26.8 | 10.8 | 4.0 | 26.2 | 1.000 |
| CHO (% energy) | 45–65% of E | 13.9 | 5.7 | 30.0 | 21.6 | 10.9 | 38.3 | 0.543 |
| Sat Fats (% energy) | 10% of E | 5.6 | 1.3 | 20.5 | 8.1 | 2.5 | 23.0 | 1.000 |
| MUFA (% energy) | __ | __ | __ | __ | __ | __ | __ | __ |
| PUFA (% energy) | 6–11% of E | 55.6 | 38.8 | 71.2 | 56.8 | 40.1 | 72.0 | 1.000 |
| Trans Fats (% energy) | <1% of E | 100.0 | __ | __ | 100.0 | __ | __ | __ |
| Cholesterol (mg/day) | ≤300 mg/d | 8.3 | 2.6 | 23.6 | 51.4 | 35.1 | 67.3 | <0.0001 * |
| Fibre (g/day) | Males ≤50 years: ≥38 g/day (≥EAR) Males >50 years: ≥30 g/day (≥EAR) Females ≤50 years: ≥25 g/day (≥EAR) Females >50 years: ≥21 g/day (≥EAR) | 66.7 | 49.4 | 80.4 | 59.5 | 42.7 | 74.3 | 0.630 |
| Sodium (mg/day) | <2300 mg/day (≤UL) | 8.3 | 2.6 | 23.6 | 45.9 | 30.3 | 62.4 | <0.0001 * |
| Potassium (mg/day) | ≥4700 mg/day (≥AI) | 94.4 | 79.5 | 98.7 | 83.8 | 67.6 | 92.7 | 0.261 |
| Calcium (mg/day) | Males ≤50 years: 1000–2500 mg/day (≥RDA) Males ≤50 years: 1000–2500 mg/day (≤UL) Males >50 years: 1000–2000 mg/day (≥RDA) Males >50 years: 1000–2000 mg/day (≤UL) Females ≤50 years: 1000–2500 mg/day (≥RDA) Females ≤50 years: 1000–2500 mg/day (≤UL) Females >50 years: 1200–2000 mg/day (≥RDA) Females >50 years: 1200–2000 mg/day (≤UL) | 63.9 | 46.7 | 78.2 | 40.5 | 25.7 | 57.3 | 0.062 |
| Magnesium (mg/day) | Males: ≥420 mg/day (≥EAR) Females: ≥420 mg/day (≥EAR) | 80.6 | 63.8 | 90.7 | 56.8 | 40.1 | 72.0 | 0.043 * |
| Phosphorus (mg/day) | ≥700 mg/day (≥EAR) | 100.0 | __ | __ | 100.0 | __ | __ | __ |
| Iron (mg/day) | Males ≤50 years: 8–45 mg/day (≥RDA) Males ≤50 years: 8–45 mg/day (≤UL) Females ≤50 years: 18–45 mg/day (≥RDA) Females ≤50 years: 18–45 mg/day (≤UL) Females >50 years: 8–45 mg/day (≥RDA) Females >50 years: 8–45 mg/day (≤UL) | 75.0 | 57.9 | 86.8 | 62.2 | 45.2 | 76.6 | 0.315 |
| Zinc (mg/day) | Males: 11–40 mg/day (≥RDA) Males: 11–40 mg/day (≤UL) Females: 8–40 mg/day (≥RDA) Females: 8–40 mg/day (≤UL) | 83.3 | 66.9 | 92.5 | 54.1 | 37.6 | 69.7 | 0.011 * |
| Vit D (ug/day) | 15–100 ug/day (≥RDA) 15–100 ug/day (≤UL) | 0.0 | __ | __ | 0.0 | __ | __ | __ |
| Vit E (mg/day) | 15–100 mg/day (≥RDA) 15–100 mg/day (≤UL) | 61.1 | 44.0 | 75.9 | 21.6 | 10.9 | 38.3 | 0.010 * |
| Thiamin (mg/day) | Males: ≥1.2 mg/day (≥EAR) Females: ≥1.1 mg/day (≥EAR) | 94.4 | 79.5 | 98.7 | 89.2 | 73.8 | 96.0 | 0.674 |
| Riboflavin (mg/day) | Males: ≥1.3 mg/day (≥EAR) Females: ≥1.1 mg/day (≥EAR) | 94.4 | 79.5 | 98.7 | 81.1 | 64.7 | 90.9 | 0.152 |
| Niacin (mg/day) | Males: 16–35 mg/day (≥EAR) Males: 16–35 mg/day (≤UL) Females: 14–35 mg/day (≥RDA) Females: 14–35 mg/day (≤UL) | 47.2 | 31.2 | 63.8 | 56.8 | 40.1 | 72.0 | 0.486 |
| Vit B6 (mg/day) | Males ≤50 years: 1.3–100 mg/day (≥RDA) Males ≤50 years: 1.3–100 mg/day (≤UL) Males >50 years: 1.7–100 mg/day (≥RDA) Males >50 years: 1.7–100 mg/day (≤UL) Females ≤50 years: 1.3–100 mg/day (≥RDA) Females ≤50 years: 1.3–100 mg/day (≤UL) Females >50 years: 1.5–100 mg/day (≥RDA) Females >50 years: 1.5–100 mg/day (≤UL) | 94.4 | 79.5 | 98.7 | 75.7 | 58.9 | 87.1 | 0.046 * |
| Vit B12 (ug/day) | ≥2.4 ug/day (≥EAR) | 94.4 | 79.5 | 98.7 | 89.2 | 73.8 | 96.0 | 0.674 |
| Folate (ug/day) | 400–1000 ug/day (≥RDA) 400–1000 ug/day (≤UL) | 33.3 | 19.6 | 50.6 | 10.8 | 4.0 | 26.2 | 0.025 * |
| Pantothenic acid (ug/day) | ≥5 ug/day (≥AI) | 86.1 | 70.0 | 94.3 | 51.4 | 35.1 | 67.3 | 0.002 * |
| Vit C (mg/day) | Males: 90–2000 mg/day (≥EAR) Males: 90–2000 mg/day (≤UL) Females: 75–2000 mg/day (≥RDA) Females: 75–2000 mg/day (≤UL) | 69.4 | 52.2 | 82.6 | 59.5 | 42.7 | 74.3 | 0.465 |
| MedDiet Score | |||||
|---|---|---|---|---|---|
| Median | IQR | Mean | Std Dev. | Minimum and Maximum | |
| Cases and Controls (n = 73) | 32.1 | 7.1 | 31.5 | 5.4 | 12.0–42.0 |
| Controls (n = 37) | 31.1 | 8.1 | 31.2 | 4.5 | 23.0–40.0 |
| Asymptomatic (n = 18) a | 31.1 | 6.1 | 29.3 | 6.2 | 12.0–39.0 |
| Symptomatic (n = 18) b,c | 33.1 | 8.1 | 5.3 | 5.3 | 24.0–42.0 |
| MEDAS Score | ||||||
|---|---|---|---|---|---|---|
| Median | IQR | Mean | Std Dev. | Minimum and Maximum | p-Value | |
| Cases and Controls (n = 73) | 7.2 | 2.0 | 6.6 | 1.8 | 2.0–11.1 | |
| Controls (n = 37) | 8.2 | 2.0 | 7.2 | 1.8 | 3.0–11.1 | |
| Asymptomatic (n = 18) a | 5.5 | 3.0 | 5.7 | 2.1 | 2.0–10.1 | |
| Symptomatic (n = 18) b,c | 6.2 | 1.0 | 1.2 | 1.2 | 4.0–9.1 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Christodoulou, C.C.; Demetriou, C.A.; Philippou, E.; Papanicolaou, E.Z. Investigating the Dietary Intake Using the CyFFQ Semi-Quantitative Food Frequency Questionnaire in Cypriot Huntington’s Disease Patients. Nutrients 2023, 15, 1136. https://doi.org/10.3390/nu15051136
Christodoulou CC, Demetriou CA, Philippou E, Papanicolaou EZ. Investigating the Dietary Intake Using the CyFFQ Semi-Quantitative Food Frequency Questionnaire in Cypriot Huntington’s Disease Patients. Nutrients. 2023; 15(5):1136. https://doi.org/10.3390/nu15051136
Chicago/Turabian StyleChristodoulou, Christiana C., Christiana A. Demetriou, Elena Philippou, and Eleni Zamba Papanicolaou. 2023. "Investigating the Dietary Intake Using the CyFFQ Semi-Quantitative Food Frequency Questionnaire in Cypriot Huntington’s Disease Patients" Nutrients 15, no. 5: 1136. https://doi.org/10.3390/nu15051136
APA StyleChristodoulou, C. C., Demetriou, C. A., Philippou, E., & Papanicolaou, E. Z. (2023). Investigating the Dietary Intake Using the CyFFQ Semi-Quantitative Food Frequency Questionnaire in Cypriot Huntington’s Disease Patients. Nutrients, 15(5), 1136. https://doi.org/10.3390/nu15051136