
Dietary Inflammatory Index, Obesity, and the Incidence of Colorectal Cancer: Findings from a Hospital-Based Case-Control Study in Malaysia

 , , , and
, , , and
Abstract
1. Introduction
2. Materials and Methods
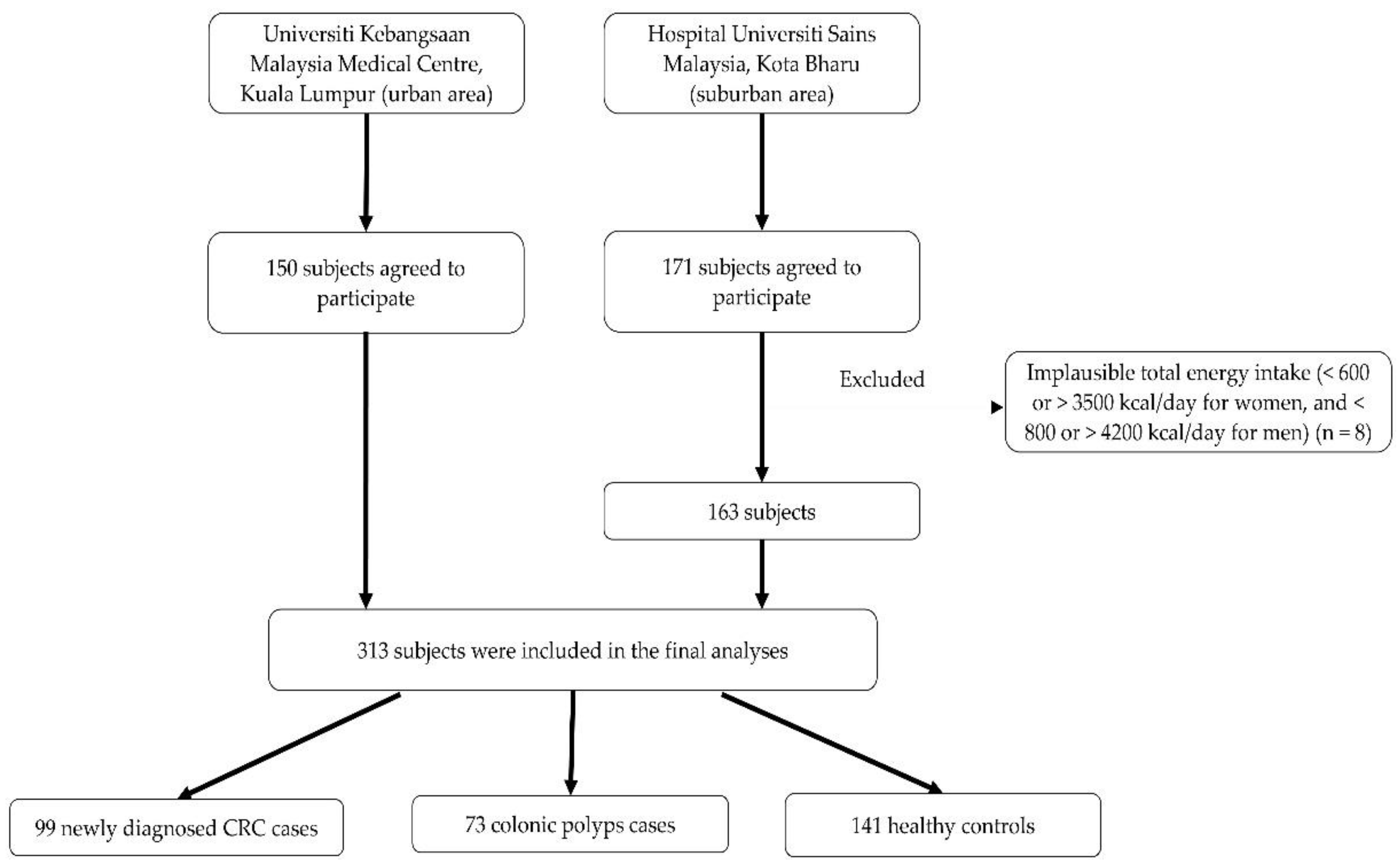
2.1. Study Design and Selection of Subjects
2.2. Data Collection
2.3. Anthropometric Measurements
2.4. Dietary Assessment
2.5. Dietary Inflammatory Index (DII) Score
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Azizah, A.M.; Hashimah, B.; Nirmal, K.; Siti Zubaidah, A.R.; Puteri, N.A.; Nabihah, A.; Sukumaran, R.; Balqis, B.; Nadia, S.M.R.; Sharifah, S.S.S.; et al. Malaysian National Cancer Registry Report (MNCR) 20122016, National Cancer Registry Department, National Cancer Institute, Malaysia. 2019. Available online: http://wwwmoh.gov.my/ (accessed on 20 October 2022).
- Quail, D.F.; Dannenberg, A.J. The Obese Adipose Tissue Microenvironment in Cancer Development and Progression. Nat. Rev. Endocrinol. 2019, 15, 139–154. [Google Scholar] [CrossRef] [PubMed]
- Deng, T.; Lyon, C.J.; Bergin, S.; Caligiuri, M.A.; Hsueh, W.A. Obesity, Inflammation, and Cancer. Annu. Rev. Pathol. 2016, 11, 421–449. [Google Scholar] [CrossRef] [PubMed]
- Kolb, R.; Sutterwala, F.S.; Zhang, W. Obesity and Cancer: Inflammation Bridges the Two. Curr. Opin. Pharmacol. 2016, 29, 77–89. [Google Scholar] [CrossRef] [PubMed]
- World Cancer Research Fund/American Institute for Cancer Research. Continuous Update Project Report: Meat, Fish and Dairy Products and the Risk of Cancer; World Cancer Research Fund International: London UK, 2018; pp. 1–78. [Google Scholar]
- Aykan, N.F. Red Meat and Colorectal Cancer. Onco. Rev. 2015, 9, 288. [Google Scholar] [CrossRef]
- Song, M.; Garrett, W.S.; Chan, A.T. Nutrients, Foods, and Colorectal Cancer Prevention. Gastroenterology 2015, 148, 1244–1260.e16. [Google Scholar] [CrossRef]
- Seiwert, N.; Adam, J.; Stenberg, P.; Wirtz, S.; Schwerdtle, T.; Adams-Quack, P.; Hövelmeyer, N.; Kaina, B.; Foersch, S.; Fahrer, J. Chronic Intestinal Inflammation Drives Colorectal Tumor Formation Triggered by Dietary Heme Iron In Vivo. Arch. Toxicol. 2021, 95, 2507–2522. [Google Scholar] [CrossRef]
- Donovan, M.G.; Selmin, O.I.; Doetschman, T.C.; Romagnolo, D.F. Mediterranean Diet: Prevention of Colorectal Cancer. Front. Nutr. 2017, 4, 59. [Google Scholar] [CrossRef]
- Muhammad Nawawi, K.N.; Mokhtar, N.M.; Wong, Z.; Mohd Azman, Z.A.; Hsin Chew, D.C.; Rehir, R.; Leong, J.; Ismail, F.; Mohamed Rose, I.; Yaacob, Y.; et al. Incidence and Clinicopathological Features of Colorectal Cancer among Multi-Ethnic Patients in Kuala Lumpur, Malaysia: A Hospital-Based Retrospective Analysis over Two Decades. PeerJ 2021, 9, e12425. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hébert, J.R. Designing. Designing and Developing a Literature-Derived, Population-Based Dietary Inflammatory Index. Public Health Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef]
- Tabung, F.K.; Steck, S.E.; Ma, Y.; Liese, A.D.; Zhang, J.; Caan, B.; Hou, L.; Johnson, K.C.; Mossavar-Rahmani, Y.; Shivappa, N.; et al. The Association between Dietary Inflammatory Index and Risk of Colorectal Cancer among Postmenopausal Women: Results from the Women’s Health Initiative. Cancer Causes Control 2015, 26, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Harmon, B.E.; Wirth, M.D.; Boushey, C.J.; Wilkens, L.R.; Draluck, E.; Shivappa, N.; Steck, S.E.; Hofseth, L.; Haiman, C.A.; Le Marchand, L.; et al. The Dietary Inflammatory Index is Associated with Colorectal Cancer Risk in the Multi-Ethnic Cohort. J. Nutr. 2017, 147, 430–438. [Google Scholar] [CrossRef] [PubMed]
- Wirth, M.D.; Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hébert, J.R. The Dietary Inflammatory Index is Associated with Colorectal Cancer in the National Institutes of Health-American Association of Retired Persons Diet and Health Study. Br. J. Nutr. 2015, 113, 1819–1827. [Google Scholar] [CrossRef] [PubMed]
- Sharma, I.; Zhu, Y.; Woodrow, J.R.; Mulay, S.; Parfrey, P.S.; Mclaughlin, J.R.; Hebert, J.R.; Shivappa, N.; Li, Y.; Zhou, X.; et al. Inflammatory Diet and Risk for Colorectal Cancer: A Population-Based Case-Control Study in Newfoundland, Canada. Nutrition 2017, 42, 69–74. [Google Scholar] [CrossRef]
- Shivappa, N.; Prizment, A.E.; Blair, C.K.; Jacobs, D.R., Jr.; Steck, S.E.; Hébert, J.R. Dietary Inflammatory Index and Risk of Colorectal Cancer in the Iowa Women’s Health Study. Cancer Epidemiol. Biomark. Prev. 2014, 23, 2383–2392. [Google Scholar] [CrossRef]
- Tabung, F.K.; Steck, S.E.; Ma, Y.; Liese, A.D.; Zhang, J.; Lane, D.S.; Ho, G.Y.F.; Hou, L.; Snetselaar, L.; Ockene, J.K.; et al. Changes in the Inflammatory Potential of Diet Over Time and Risk of Colorectal Cancer in Postmenopausal Women. Am. J. Epidemiol. 2017, 186, 514–523. [Google Scholar] [CrossRef]
- Niclis, C.; Pou, S.A.; Shivappa, N.; Hébert, J.R.; Steck, S.E.; Díaz, M.D.P. Proinflammatory Dietary Intake is Associated with Increased Risk of Colorectal Cancer: Results of a Case-Control Study in Argentina Using a Multilevel Modeling Approach. Nutr. Cancer 2018, 70, 61–68. [Google Scholar] [CrossRef]
- Zamora-Ros, R.; Shivappa, N.; Steck, S.E.; Canzian, F.; Landi, S.; Alonso, M.H.; Hébert, J.R.; Moreno, V. Dietary Inflammatory Index and Inflammatory Gene Interactions in Relation to Colorectal Cancer Risk in the Bellvitge Colorectal Cancer Case-Control Study. Genes Nutr. 2015, 10, 447. [Google Scholar] [CrossRef]
- Shivappa, N.; Zucchetto, A.; Montella, M.; Serraino, D.; Steck, S.E.; La Vecchia, C.; Hébert, J.R. Inflammatory Potential of Diet and Risk of Colorectal Cancer: A Case-Control Study from Italy. Br. J. Nutr. 2015, 114, 152–158. [Google Scholar] [CrossRef]
- Obón-Santacana, M.; Romaguera, D.; Gracia-Lavedan, E.; Molinuevo, A.; Molina-Montes, E.; Shivappa, N.; Hebert, J.R.; Tardón, A.; Castaño-Vinyals, G.; Moratalla, F.; et al. Dietary Inflammatory Index, Dietary Non-Enzymatic Antioxidant Capacity, and Colorectal and Breast Cancer Risk (MCC-Spain Study). Nutrients 2019, 11, 1406. [Google Scholar] [CrossRef]
- Abulimiti, A.; Zhang, X.; Shivappa, N.; Hébert, J.R.; Fang, Y.J.; Huang, C.Y.; Feng, X.L.; Chen, Y.M.; Zhang, C.X. The Dietary Inflammatory Index is Positively Associated with Colorectal Cancer Risk in a Chinese Case-Control Study. Nutrients 2020, 12, 232. [Google Scholar] [CrossRef] [PubMed]
- Cho, Y.A.; Lee, J.; Oh, J.H.; Shin, A.; Kim, J. Dietary Inflammatory Index and Risk of Colorectal Cancer: A Case-Control Study in Korea. Nutrients 2016, 8, 469. [Google Scholar] [CrossRef] [PubMed]
- Rafiee, P.; Shivappa, N.; Hébert, J.R.; Nasab, S.J.; Bahrami, A.; Hekmatdoost, A.; Rashidkhani, B.; Sadeghi, A.; Houshyari, M.; Hejazi, E. Dietary Inflammatory Index and Odds of Colorectal Cancer and Colorectal Adenomatous Polyps in a Case-Control Study from Iran. Nutrients 2019, 11, 1213. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Hébert, J.R.; Steck, S.E.; Safari, A.; Sedaghat, F.; Rashidkhani, B. Dietary Inflammatory Index and Odds of Colorectal Cancer in a Case- Control Study from Iran. Asian Pac. J. Cancer Prev. 2018, 19, 1999–2006. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Hébert, J.R.; Steck, S.E.; Hofseth, L.J.; Shehadah, I.; Bani-Hani, K.E.; Al-Jaberi, T.; Al-Nusairr, M.; Heath, D.; Tayyem, R. Dietary Inflammatory Index and odds of colorectal cancer in a case-control study from Jordan. Appl. Physiol. Nutr. Metab. 2017, 42, 744–749. [Google Scholar] [CrossRef]
- Press Release Current Population Estimates, Malaysia, 2021 [Internet]. Department of Statistics Malaysia Press Release 2021. Available online: https://www.dosm.gov.my/v1/index.php?r=column/cthemeByCat&cat=155&bul_id=ZjJOSnpJR21sQWVUcUp6ODRudm5JZz09&menu_id=L0pheU43NWJwRWVSZklWdzQ4TlhUUT09 (accessed on 10 July 2022).
- Safari, A.; Shariff, Z.M.; Kandiah, M.; Rashidkhani, B.; Fereidooni, F. Dietary Patterns and Risk of Colorectal Cancer in Tehran Province: A Case-Control Study. BMC Public Health 2013, 13, 222. [Google Scholar] [CrossRef]
- Nimptsch, K.; Zhang, X.; Cassidy, A.; Song, M.; O’Reilly, É.J.; Lin, J.H.; Pischon, T.; Rimm, E.B.; Willett, W.C.; Fuchs, C.S.; et al. Habitual Intake of Flavonoid Subclasses and Risk of Colorectal Cancer in 2 Large Prospective Cohorts. Am. J. Clin. Nutr. 2016, 103, 184–191. [Google Scholar] [CrossRef]
- Banna, J.C.; McCrory, M.A.; Fialkowski, M.K.; Boushey, C. Examining Plausibility of Self-Reported Energy Intake Data: Considerations for Method Selection. Front. Nutr. 2017, 4, 45. [Google Scholar] [CrossRef]
- WHO Expert Consultation. Appropriate Body Mass Index for Asia Populations and Its Implications for Policy and Intervention Strategies. Lancet 2004, 363, 157–163. [Google Scholar] [CrossRef]
- World Health Organization. Waist Circumference and Waist-Hip Ratio: Report of a WHO Expert Consultation, Geneva. 2008. Available online: https://apps.who.int/iris/handle/10665/44583 (accessed on 10 September 2022).
- WHO Expert Committee. Physical status: The Use and Interpretation of Anthropometry. Report of a WHO Expert Committee. World Health Organ Tech. Rep. Ser. 1995, 854, 1–452. [Google Scholar]
- Institute for Public Health. National Health and Morbidity Survey 2014: Malaysian Adult Nutrition Survey (MANS). In Volume 1: Methodology and General Findings; Institute for Public Health: Kuala Lumpur, Malaysia, 2014. [Google Scholar]
- Abd Rashid, A.A.; Ashari, L.S.; Shafiee, N.H.; Raja Ali, R.A.; Lee, Y.Y.; Shahril, M.R.; Jan Mohamed, H.J. Validity and Reproducibility of Malaysian Food Frequency Questionnaire for Dietary Intake Related to Colorectal Cancer. J. Gizi Pangan 2022, 17, 77–86. [Google Scholar] [CrossRef]
- Tee, E.S.; Noor, M.I.; Azudin, M.N.; Idris, K. Nutrient Composition of Malaysian Foods, 4th ed.; Institute for Medical Research: Kuala Lumpur, Malaysia, 1997. [Google Scholar]
- Abdul Manaf, Z.; Shahar, S.; Safii, N.S.; Haron, H. Atlas of Food Exchanges & Portion Sizes, 3rd ed.; MDC: Kuala Lumpur, Malaysia, 2015; ISBN 9679677014587. [Google Scholar]
- Tahir, A.; Suhaila, A.G.; Azli, B.; Nadrah, M.H.; Yuhanis Auri, A.K.; Nurul Fatihah, H.G.; Anim Zakiah, M. (Eds.) Album Makanan Malaysia, 1st ed.; Institute for Public Health: Kuala Lumpur, Malaysia, 2011. [Google Scholar]
- Ministry of Health. Malaysian Food Composition Database (MyFCD); Ministry of Health: Putrajaya, Malaysia, 2017. Available online: http://myfcd.moh.gov.my/ (accessed on 1 October 2020).
- Norimah, A.K., Jr.; Safiah, M.; Jamal, K.; Haslinda, S.; Zuhaida, H.; Rohida, S.; Fatimah, S.; Norazlin, S.; Poh, B.K.; Kandiah, M.; et al. Food Consumption Patterns: Findings from the Malaysian Adult Nutrition Survey (MANS). Malays J. Nutr. 2008, 14, 25–39. [Google Scholar] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Tabung, F.; Hébert, J.R. A Population-Based Dietary Inflammatory Index Predicts Levels of C-Reactive Protein in the Seasonal Variation of Blood Cholesterol Study (SEASONS). Public Health Nutr. 2014, 17, 1825–1833. [Google Scholar] [CrossRef]
- Shivappa, N.; Godos, J.; Hébert, J.R.; Wirth, M.D.; Piuri, G.; Speciani, A.F.; Grosso, G. Dietary Inflammatory Index and Colorectal Cancer Risk-A Meta-Analysis. Nutrients 2017, 9, 1043. [Google Scholar] [CrossRef]
- Shivappa, N.; Hébert, J.R.; Rosato, V.; Rossi, M.; Libra, M.; Montella, M.; Serraino, D.; La Vecchia, C. Dietary Inflammatory Index and Risk of Bladder Cancer in a Large Italian Case-Control Study. Urology 2017, 100, 84–89. [Google Scholar] [CrossRef]
- Shivappa, N.; Niclis, C.; Coquet, J.B.; Román, M.D.; Hébert, J.R.; Diaz, M.D.P. Increased Inflammatory Potential of Diet is Associated with Increased Odds of Prostate Cancer in Argentinian Men. Cancer Causes Control 2018, 29, 803–813. [Google Scholar] [CrossRef] [PubMed]
- Dugué, P.A.; Hodge, A.M.; Brinkman, M.T.; Bassett, J.K.; Shivappa, N.; Hebert, J.R.; Hopper, J.L.; English, D.R.; Milne, R.L.; Giles, G.G. Association between Selected Dietary Scores and the Risk of Urothelial Cell Carcinoma: A Prospective Cohort Study. Int. J. Cancer 2016, 139, 1251–1260. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Blair, C.K.; Prizment, A.E.; Jacobs, D.R., Jr.; Hébert, J.R. Dietary Inflammatory Index and Risk of Renal Cancer in The Iowa Women’s Health Study. Eur. J. Nutr. 2018, 57, 1207–1213. [Google Scholar] [CrossRef] [PubMed]
- Bao, X.; Chen, F.; Lin, J.; Chen, Q.; Chen, L.; Wang, R.; Liu, F.; Wang, J.; Yan, L.; Lin, L.; et al. Association between Dietary Inflammatory Index and the Risk of Oral Cancer in the Southeast of China. Eur. J. Clin. Nutr. 2020, 74, 938–944. [Google Scholar] [CrossRef]
- Secchi, D.G.; Aballay, L.R.; Shivappa, N.; Hebert, J.R.; Galíndez Costa, M.F.; Brunotto, M. The Inflammatory Potential of Argentinian Diet and Oral Squamous Cell Carcinoma. Nutr. Hosp. 2019, 36, 1361–1367. [Google Scholar] [CrossRef]
- Mazul, A.L.; Shivappa, N.; Hébert, J.R.; Steck, S.E.; Rodriguez-Ormaza, N.; Weissler, M.; Olshan, A.F.; Zevallos, J.P. Proinflammatory Diet is Associated with Increased Risk of Squamous Cell Head and Neck Cancer. Int. J. Cancer 2018, 143, 1604–1610. [Google Scholar] [CrossRef]
- Shivappa, N.; Hébert, J.R.; Rosato, V.; Garavello, W.; Serraino, D.; La Vecchia, C. Inflammatory Potential of Diet and Risk of Oral and Pharyngeal Cancer in a Large Case-Control Study from Italy. Int. J. Cancer 2017, 141, 471–479. [Google Scholar] [CrossRef] [PubMed]
- Abe, M.; Shivappa, N.; Ito, H.; Oze, I.; Abe, T.; Shimizu, Y.; Hasegawa, Y.; Kiyohara, C.; Nomura, M.; Ogawa, Y.; et al. Dietary Inflammatory Index and Risk of Upper Aerodigestive Tract Cancer in Japanese Adults. Oncotarget 2018, 9, 24028–24040. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Shivappa, N.; Hebert, J.R.; Lee, A.H.; Xu, F.; Binns, C.W. Dietary Inflammatory Index and Risk of Oesophageal Cancer in Xinjiang Uyghur Autonomous Region, China. Br. J. Nutr. 2018, 119, 1068–1075. [Google Scholar] [CrossRef]
- Hajji-Louati, M.; Cordina-Duverger, E.; Laouali, N.; Mancini, F.R.; Guénel, P. A Case-Control Study in France Showing That a Pro-Inflammatory Diet is Associated with a Higher Risk of Breast Cancer. Sci. Rep. 2021, 11, 17019. [Google Scholar] [CrossRef] [PubMed]
- Tabung, F.K.; Steck, S.E.; Liese, A.D.; Zhang, J.; Ma, Y.; Caan, B.; Chlebowski, R.T.; Freudenheim, J.L.; Hou, L.; Mossavar-Rahmani, Y.; et al. Association between Dietary Inflammatory Potential and Breast Cancer Incidence and Death: Results from the Women’s Health Initiative. Br. J. Cancer 2016, 114, 1277–1285. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Hébert, J.R.; Rosato, V.; Montella, M.; Serraino, D.; La Vecchia, C. Association between the Dietary Inflammatory Index and Breast Cancer in a Large Italian Case-Control Study. Mol. Nutr. Food. Res. 2017, 61, 1600500. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Quiambao, A.L.; Lee, J.; Ro, J.; Lee, E.S.; Jung, S.Y.; Sung, M.K.; Kim, J. Dietary Inflammatory Index and Risk of Breast Cancer Based on Hormone Receptor Status: A Case-Control Study in Korea. Nutrients 2019, 11, 1949. [Google Scholar] [CrossRef]
- Tabung, F.K.; Steck, S.E.; Liese, A.D.; Zhang, J.; Ma, Y.; Johnson, K.C.; Lane, D.S.; Qi, L.; Snetselaar, L.; Vitolins, M.Z.; et al. Patterns of Change Over Time and History of the Inflammatory Potential of Diet and Risk of Breast Cancer Among Postmenopausal Women. Breast Cancer Res. Treat. 2016, 159, 139–149. [Google Scholar] [CrossRef]
- Lee, S.; Lee, J.; Ju Choi, I.; Kim, Y.; Won Ryu, K.; Kim, Y.; Oh, J.; Thang Tran, B.; Kim, J. Dietary Inflammatory Index and the Risk of Gastric Cancer in a Korean Population. Oncotarget 2017, 8, 85452–85462. [Google Scholar] [CrossRef]
- Vahid, F.; Shivappa, N.; Faghfoori, Z.; Khodabakhshi, A.; Zayeri, F.; Hebert, J.R.; Davoodi, S.H. Validation of a Dietary Inflammatory Index (DII) and Association with Risk of Gastric Cancer: A Case-Control Study. Asian Pac. J. Cancer Prev. 2018, 19, 1471–1477. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Hébert, J.R.; Zucchetto, A.; Montella, M.; Serraino, D.; La Vecchia, C.; Rossi, M. Dietary Inflammatory Index and Endometrial Cancer Risk in an Italian Case-Control Study. Br. J. Nutr. 2016, 115, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Wang, R.; Hébert, J.R.; Jin, A.; Koh, W.P.; Yuan, J.M. Association Between Inflammatory Potential of Diet and Risk of Lung Cancer among Smokers in a Prospective Study in Singapore. Eur. J. Nutr. 2019, 58, 2755–2766. [Google Scholar] [CrossRef] [PubMed]
- Castelló, A.; Amiano, P.; Fernández de Larrea, N.; Martín, V.; Alonso, M.H.; Castaño-Vinyals, G.; Pérez-Gómez, B.; Olmedo-Requena, R.; Guevara, M.; Fernandez-Tardon, G.; et al. Low Adherence to the Western and High Adherence to the Mediterranean Dietary Patterns Could Prevent Colorectal Cancer. Eur. J. Nutr. 2018, 58, 1495–1505. [Google Scholar] [CrossRef]
- Festa, A.; D’Agostino, R.; Howard, G.; Mykkänen, L.; Tracy, R.P.; Haffner, S.M. Chronic Subclinical Inflammation as Part of the Insulin Resistance Syndrome-The Insulin Resistance Atherosclerosis Study (IRAS). Circulation 2000, 102, 42–47. [Google Scholar] [CrossRef]
- Bruce, W.R.; Wolever, T.M.; Giacca, A. Mechanisms Linking Diet and Colorectal Cancer: The Possible Role of Insulin Resistance. Nutr. Cancer 2000, 37, 19–26. [Google Scholar] [CrossRef]
- Bruce, W.R.; Giacca, A.; Medline, A. Possible Mechanisms Relating Diet and Risk of Colon Cancer. Cancer Epidemiol. Biomark. Prev. 2000, 9, 1271–1279. [Google Scholar]
- Ahmad Kendong, S.M.; Raja Ali, R.A.; Nawawi, K.N.M.; Ahmad, H.F.; Mokhtar, N.M. Gut Dysbiosis and Intestinal Barrier Dysfunction: Potential Explanation for Early-Onset Colorectal Cancer. Front. Cell Infect. Microbiol. 2021, 11, 74460. [Google Scholar] [CrossRef]
- Fukui, H. Increased Intestinal Permeability and Decreased Barrier Function: Does It Really Influence the Risk of Inflammation? Inflamm. Intest. Dis. 2016, 1, 135–145. [Google Scholar] [CrossRef]
- Triantafillidis, J.K.; Nasioulas, G.; Kosmidis, P.A. Colorectal Cancer and Inflammatory Bowel Disease: Epidemiology, Risk Factors, Mechanisms of Carcinogenesis and Prevention Strategies. Anticancer Res. 2009, 29, 2727–2737. [Google Scholar]
- Chan, A.T.; Giovannucci, E.L. Primary Prevention of Colorectal Cancer. Gastroenterology 2010, 138, 2029–2043. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Boakye, D.; Chen, X.; Hoffmeister, M.; Brenner, H. Association of Body Mass Index with Risk of Early-Onset Colorectal Cancer: Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2021, 116, 2173–2183. [Google Scholar] [CrossRef]
- Guffey, C.R.; Fan, D.; Singh, U.P.; Murphy, E.A. Linking Obesity to Colorectal Cancer: Recent Insights into Plausible Biological Mechanisms. Curr. Opin. Clin. Nutr. Metab. Care 2013, 16, 595–600. [Google Scholar] [CrossRef] [PubMed]
- Veettil, S.K.; Lim, K.G.; Chaiyakunapruk, N.; Ching, S.M.; Abu Hassan, M.R. Colorectal Cancer in Malaysia: Its Burden and Implications for a Multiethnic Country. Asian J. Surg. 2017, 40, 481–489. [Google Scholar] [CrossRef] [PubMed]
- Shiels, M.S.; Katki, H.A.; Freedman, N.D.; Purdue, M.P.; Wentzensen, N.; Trabert, B.; Kitahara, C.M.; Furr, M.; Li, Y.; Kemp, T.J.; et al. Cigarette Smoking and Variations in Systemic Immune and Inflammation Markers. J. Natl. Cancer Inst. 2014, 106, dju294. [Google Scholar] [CrossRef] [PubMed]
- Li, L.F.; Chan, R.L.; Lu, L.; Shen, J.; Zhang, L.; Wu, W.K.; Wang, L.; Hu, T.; Li, M.X.; Cho, C.H. Cigarette Smoking and Gastrointestinal Diseases: The Causal Relationship and Underlying Molecular Mechanisms (Review). Int. J. Mol. Med. 2014, 34, 372–380. [Google Scholar] [CrossRef] [PubMed]
- George, S.; Abrahamse, H. Redox Potential of Antioxidants in Cancer Progression and Prevention. Antioxidants 2020, 9, 1156. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Quartiles of E-DII | p for Trend a | |||
|---|---|---|---|---|---|
| Q1 (≤−0.04) Mean ± SD (−0.75 ± 0.65) n = 78 | Q2 (−0.04–1.15) Mean ± SD (0.51 ± 0.39) n = 79 | Q3 (1.15–2.54) Mean ± SD (1.82 ± 0.43) n = 79 | Q4 (≥2.54) Mean ± SD (3.20 ± 0.48) n = 77 | ||
| Subjects | 0.004 ** | ||||
| CRC | 18 (23.1) | 25 (31.6) | 24 (30.4) | 32 (41.6) | |
| Colonic Polyps | 11 (14.1) | 24 (30.4) | 22 (27.8) | 16 (20.8) | |
| Healthy Control | 49 (62.8) | 30 (38.0) | 33 (41.8) | 29 (37.7) | |
| Sex | 0.071 | ||||
| Female | 42 (53.8) | 41 (51.9) | 34 (43.0) | 32 (41.6) | |
| Male | 36 (46.2) | 38 (48.1) | 45 (57.0) | 45 (58.4) | |
| Age (yr) b | 49.76 ± 15.2 | 51.59 ± 14.5 | 54.27 ± 14.8 | 58.74 ± 15.3 | <0.001 |
| Age groups (yr) | <0.001 | ||||
| <50 | 40 (51.3) | 36 (45.6) | 26 (32.9) | 18 (23.4) | |
| ≥50 | 38 (48.7) | 43 (54.4) | 53 (67.1) | 59 (76.6) | |
| Dietary energy intake (kcal) b | 1534 ± 453 | 1958 ± 309 | 2085 ± 301 | 2185 ± 346 | <0.001 |
| Ethnicity | <0.001 | ||||
| Malay | 40 (51.3) | 50 (63.3) | 50 (63.3) | 64 (83.1) | |
| Chinese | 20 (25.6) | 15 (19.0) | 22 (27.8) | 12 (15.6) | |
| Indian | 18 (23.1) | 14 (17.7) | 7 (8.9) | 1 (1.3) | |
| Educational Level | <0.001 | ||||
| Middle school or less | 9 (11.5) | 5 (6.3) | 8 (10.1) | 15 (19.5) | |
| High school | 22 (28.2) | 34 (43.0) | 39 (49.4) | 41 (53.2) | |
| College/University | 47 (60.3) | 40 (50.6) | 32 (40.5) | 21 (27.3) | |
| Residence | <0.001 | ||||
| Urban | 18 (23.1) | 30 (38.0) | 43 (54.4) | 72 (93.5) | |
| Suburban | 60 (76.9) | 49 (62.0) | 36 (45.6) | 5 (6.5) | |
| Family history of CRC | 26 (33.3) | 26 (32.9) | 28 (35.4) | 20 (26.3) | 0.443 |
| Previous history of polyps | 9 (11.5) | 9 (11.4) | 7 (8.9) | 4 (5.2) | 0.144 |
| BMI (kg/m2) b | 22.20 ± 3.0 | 24.66 ± 4.7 | 25.24 ± 4.7 | 28.53 ± 4.9 | <0.001 |
| BMI categories | <0.001 | ||||
| Non-obese (<25 kg/m2) | 50 (64.1) | 44 (55.7) | 34 (43.0) | 29 (37.7) | |
| Obese (≥25 kg/m2) | 28 (35.9) | 35 (44.3) | 45 (57.0) | 48 (62.3) | |
| Waist circumference (cm), males b | 88.99 ± 6.1 | 92.95 ± 11.3 | 96.06 ± 11.4 | 105.76 ± 11.9 | 0.002 ** |
| Waist circumference (cm), females b | 77.55 ± 7.8 | 89.54 ± 16.8 | 89.33 ± 15.4 | 93.91 ± 17.3 | 0.005 ** |
| Waist–hip ratio, males b | 0.91 ± 0.1 | 0.92 ± 0.1 | 0.94 ± 0.1 | 1.01 ± 0.1 | <0.001 |
| Waist–hip ratio, females b | 0.78 ± 0.1 | 0.83 ± 0.1 | 0.87 ± 0.1 | 0.92 ± 0.1 | <0.001 |
| Body fat (%), males b | 22.99 ± 8.3 | 25.16 ± 6.8 | 27.60 ± 5.8 | 31.76 ± 7.1 | <0.001 |
| Body fat (%), females b | 28.25 ± 5.9 | 34.12 ± 8.2 | 34.60 ± 8.2 | 35.21 ± 9.2 | 0.030 ** |
| Employment status | <0.001 | ||||
| Employed | 60 (76.9) | 55 (69.6) | 42 (53.2) | 39 (50.6) | |
| Unemployed | 18 (23.1) | 24 (30.4) | 37 (46.8) | 38 (49.4) | |
| Monthly household income (MYR) c | 0.485 | ||||
| <3860 | 43 (55.8) | 37 (47.4) | 51 (64.6) | 48 (63.2) | |
| 3860–8319 | 31 (40.3) | 37 (47.4) | 20 (25.3) | 22 (28.9) | |
| ≥8320 | 3 (3.9) | 5 (5.2) | 8 (10.1) | 7 (7.9) | |
| Marital Status | 0.291 | ||||
| Married | 48 (61.5) | 49 (62.0) | 52 (65.8) | 53 (68.8) | |
| Single/Divorced/Widowed | 30 (38.5) | 30 (38.0) | 27 (34.2) | 24 (31.2) | |
| Smoking Status | 0.449 | ||||
| Non-smoker | 45 (57.7) | 45 (57.0) | 47 (59.5) | 44 (57.1) | |
| Former smoker | 15 (19.2) | 19 (24.1) | 19 (24.1) | 22 (28.6) | |
| Current smoker | 18 (23.1) | 15 (19.0) | 13 (16.5) | 11 (14.3) | |
| Quartile of E-DII Score | All Subjects | BMI < 25 kg/m2 | BMI ≥ 25 kg/m2 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| No. Controls/CRC Cases | Crude OR (95% CI) | Adjusted OR (95% CI) d | No. Controls/ CRC Cases | Crude OR (95% CI) | Adjusted OR (95% CI) d | No. Controls/ CRC Cases | Crude OR (95% CI) | Adjusted OR (95% CI) d | |
| Q1 | 49/18 | 1.0 (ref.) | 1.0 (ref.) | 28/12 | 1.0 (ref.) | 1.0 (ref.) | 21/6 | 1.0 (ref.) | 1.0 (ref.) |
| Q2 | 30/25 | 1.03 (0.95–1.40) | 1.05 (0.97–1.43) | 12/15 | 1.08 (0.98–1.45) | 1.16 (0.92–1.51) | 18/10 | 1.10 (1.02–1.49) | 1.06 (1.02–1.41) |
| Q3 | 33/24 | 1.26 (1.16–1.63) | 1.30 (1.23–1.72) | 9/17 | 1.39 (0.96–1.66) | 1.37 (0.96–1.55) | 24/7 | 1.20 (1.10–1.55) | 1.10 (1.08–1.46) |
| Q4 | 29/32 | 1.39 (1.27–1.74) | 1.46 (1.32–1.80) | 13/10 | 1.34 (0.99–1.63) | 1.32 (0.87–1.46) | 16/22 | 1.36 (1.25–1.77) | 1.45 (1.30–1.77) |
| p for trend | <0.001 | <0.001 | 0.130 | 0.182 | <0.001 | <0.001 | |||
| Quartile of E-DII Score | All subjects | BMI < 25 kg/m2 | BMI ≥ 25 kg/m2 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| No. Controls/ Colonic Polyps Cases | Crude OR (95% CI) | Adjusted OR (95% CI) d | No. Controls/ Colonic Polyps Cases | Crude OR (95% CI) | Adjusted OR (95% CI) d | No. Controls/ Colonic Polyps Cases | Crude OR (95% CI) | Adjusted OR (95% CI) d | |
| Q1 | 48/11 | 1.0 (ref.) | 1.0 (ref.) | 28/10 | 1.0 (ref.) | 1.0 (ref.) | 20/1 | 1.0 (ref.) | 1.0 (ref.) |
| Q2 | 30/25 | 0.93 (0.83–1.43) | 0.86 (0.76–1.35) | 12/17 | 0.99 (0.89–1.45) | 1.82 (0.73–1.32) | 18/8 | 1.12 (0.89–1.50) | 1.09 (0.79–1.39) |
| Q3 | 33/22 | 1.05 (0.96–1.53) | 0.79 (0.65–1.23) | 9/8 | 1.09 (0.99–1.56) | 1.07 (0.97–1.57) | 24/14 | 1.23 (0.93–1.53) | 1.24 (0.74–1.36) |
| Q4 | 29/16 | 1.11 (0.99–1.64) | 0.65 (0.56–1.15) | 13/6 | 1.14 (0.87–1.62) | 1.12 (0.99–1.59) | 16/10 | 1.19 (0.95–1.57) | 1.10 (0.86–1.47) |
| p for trend | 0.150 | 0.230 | 0.130 | 0.180 | 0.145 | 0.160 | |||
| Quartile of E-DII Score | p for Interaction | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | ||||||
| No. Controls/CRC Cases | OR (95% CI) e | No. Controls/CRC Cases | OR (95% CI) e | No. Controls/CRC Cases | OR (95% CI) e | No. Controls/CRC Cases | OR (95% CI) e | ||
| Sex | 0.272 | ||||||||
| Female | 30/7 | 1.0 (ref.) | 20/12 | 1.05 (0.92–1.37) | 12/13 | 1.08 (0.95–1.40) | 10/13 | 1.12 (0.99–1.44) | |
| Male | 19/11 | 1.0 (ref.) | 10/13 | 1.19 (0.96–1.41) | 21/11 | 1.15 (0.93–1.38) | 19/19 | 1.18 (0.95–1.40) | |
| Age group | 0.030 ** | ||||||||
| <50 years old | 24/8 | 1.0 (ref.) | 17/9 | 1.04 (1.02–1.50) | 15/3 | 1.12 (1.00–1.45) | 10/1 | 1.27 (1.15–1.65) | |
| ≥50 years old | 25/10 | 1.0 (ref.) | 13/16 | 1.29 (1.01–1.43) | 18/21 | 1.49 (1.35–1.80) | 19/31 | 2.09 (1.40–1.85) | |
| Smoking status | 0.043 ** | ||||||||
| Non-smokers | 30/11 | 1.0 (ref.) | 19/17 | 1.06 (0.93–1.40) | 20/13 | 1.12 (1.00–1.47) | 15/18 | 1.25 (1.13–1.60) | |
| Ever smokers | 19/7 | 1.0 (ref.) | 11/8 | 1.23 (1.13–1.58) | 13/11 | 1.45 (1.30–1.78) | 14/14 | 1.98 (1.55–2.03) | |
| Waist circumference (cm), males | <0.001 | ||||||||
| WC < 90 | 4/9 | 1.0 (ref.) | 2/7 | 1.05 (0.92–1.37) | 11/2 | 1.02 (0.89–1.35) | 15/6 | 1.15 (1.02–1.47) | |
| WC ≥ 90 | 15/2 | 1.0 (ref.) | 8/6 | 1.26 (1.17–1.64) | 10/9 | 1.95 (1.50–1.97) | 4/13 | 2.28 (1.96–2.43) | |
| Waist circumference (cm), females | <0.001 | ||||||||
| WC < 80 | 12/4 | 1.0 (ref.) | 8/4 | 1.09 (0.96–1.43) | 10/3 | 1.22 (1.10–1.57) | 7/2 | 1.48 (1.31–1.78) | |
| WC ≥ 80 | 18/3 | 1.0 (ref.) | 12/8 | 1.31 (1.21–1.67) | 2/10 | 1.67 (1.37–1.87) | 3/11 | 2.48 (2.16–2.67) | |
| Waist–hip ratio, males | |||||||||
| WHR < 1.0 | 6/3 | 1.0 (ref.) | 10/8 | 1.10 (0.98–1.47) | 18/10 | 1.12 (1.01–1.49) | 16/16 | 1.25 (1.16–1.63) | |
| WHR ≥ 1.0 | 13/8 | 1.0 (ref.) | 0/5 | 1.39 (1.28–1.75) | 3/1 | 1.95 (1.51–1.97) | 3/3 | 2.33 (2.06–2.53) | |
| Waist–hip ratio, females | <0.001 | ||||||||
| WHR < 0.85 | 11/4 | 1.0 (ref.) | 8/4 | 1.15 (1.05–1.57) | 9/3 | 1.19 (1.10–1.57) | 8/2 | 1.21 (1.19–1.67) | |
| WHR ≥ 0.85 | 19/3 | 1.0 (ref.) | 12/8 | 1.26 (1.17–1.67) | 3/10 | 1.65 (1.33–1.80) | 2/11 | 2.58 (2.26–2.73) | |
| Body fat (%), males | <0.001 | ||||||||
| BF < 25% | 4/3 | 1.0 (ref.) | 10/8 | 1.18 (1.08–1.57) | 12/9 | 1.21 (1.20–1.67) | 10/13 | 1.35 (1.26–1.73) | |
| BF ≥ 25% | 15/8 | 1.0 (ref.) | 0/5 | 1.35 (1.27–1.75) | 9/2 | 1.75 (1.42–1.87) | 9/6 | 2.52 (2.27–2.74) | |
| Body fat (%), females | <0.001 | ||||||||
| BF < 35% | 9/3 | 1.0 (ref.) | 6/3 | 1.20 (1.12–1.60) | 6/2 | 1.24 (1.22–1.69) | 8/0 | 1.39 (1.28–1.76) | |
| BF ≥ 35% | 21/4 | 1.0 (ref.) | 14/9 | 1.40 (1.34–1.87) | 6/11 | 1.99 (1.54–2.01) | 2/13 | 2.47 (2.13–2.61) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shafiee, N.H.; Razalli, N.H.; Shahril, M.R.; Muhammad Nawawi, K.N.; Mohd Mokhtar, N.; Abd Rashid, A.A.; Ashari, L.S.; Jan Mohamed, H.J.; Raja Ali, R.A. Dietary Inflammatory Index, Obesity, and the Incidence of Colorectal Cancer: Findings from a Hospital-Based Case-Control Study in Malaysia. Nutrients 2023, 15, 982. https://doi.org/10.3390/nu15040982
Shafiee NH, Razalli NH, Shahril MR, Muhammad Nawawi KN, Mohd Mokhtar N, Abd Rashid AA, Ashari LS, Jan Mohamed HJ, Raja Ali RA. Dietary Inflammatory Index, Obesity, and the Incidence of Colorectal Cancer: Findings from a Hospital-Based Case-Control Study in Malaysia. Nutrients. 2023; 15(4):982. https://doi.org/10.3390/nu15040982
Chicago/Turabian StyleShafiee, Nor Hamizah, Nurul Huda Razalli, Mohd Razif Shahril, Khairul Najmi Muhammad Nawawi, Norfilza Mohd Mokhtar, Ainaa Almardhiyah Abd Rashid, Lydiatul Shima Ashari, Hamid Jan Jan Mohamed, and Raja Affendi Raja Ali. 2023. "Dietary Inflammatory Index, Obesity, and the Incidence of Colorectal Cancer: Findings from a Hospital-Based Case-Control Study in Malaysia" Nutrients 15, no. 4: 982. https://doi.org/10.3390/nu15040982
APA StyleShafiee, N. H., Razalli, N. H., Shahril, M. R., Muhammad Nawawi, K. N., Mohd Mokhtar, N., Abd Rashid, A. A., Ashari, L. S., Jan Mohamed, H. J., & Raja Ali, R. A. (2023). Dietary Inflammatory Index, Obesity, and the Incidence of Colorectal Cancer: Findings from a Hospital-Based Case-Control Study in Malaysia. Nutrients, 15(4), 982. https://doi.org/10.3390/nu15040982