
Fecal Calprotectin in Self-Reported Milk Intolerance: Not Only Lactose Intolerance

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
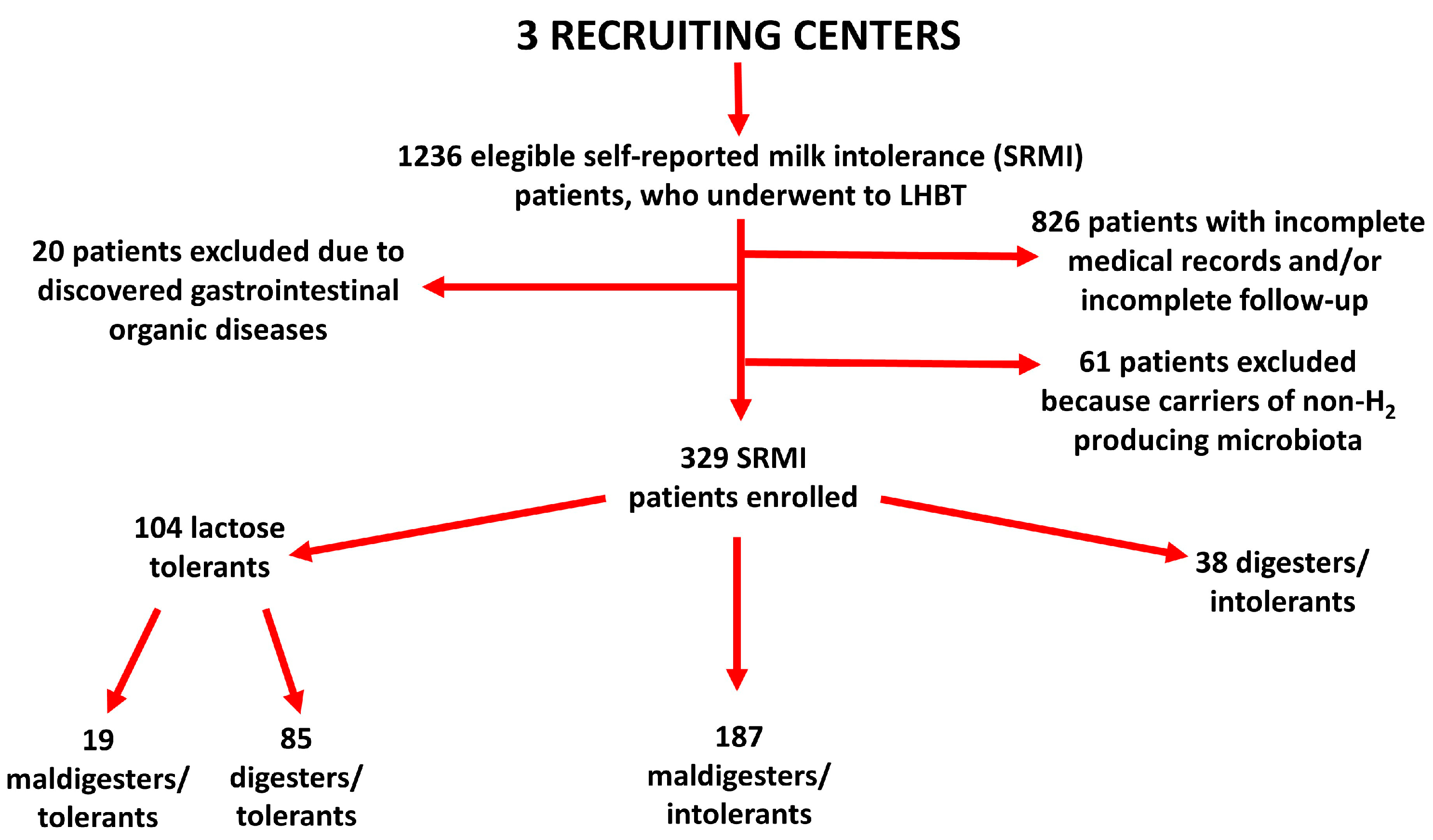
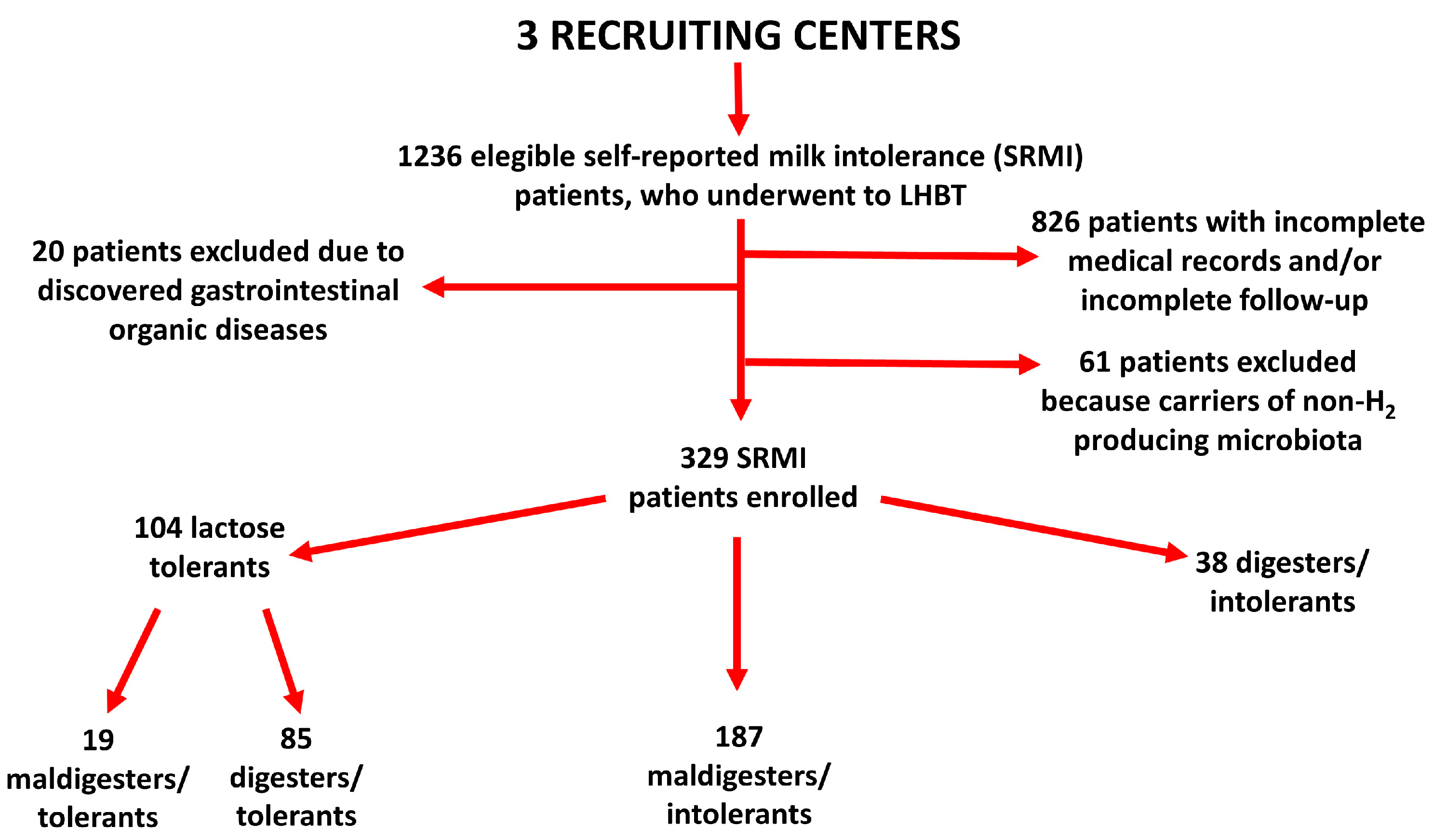
2.1. Inclusion Criteria of SRMI Patients
2.2. Exclusion Criteria of SRMI Patients
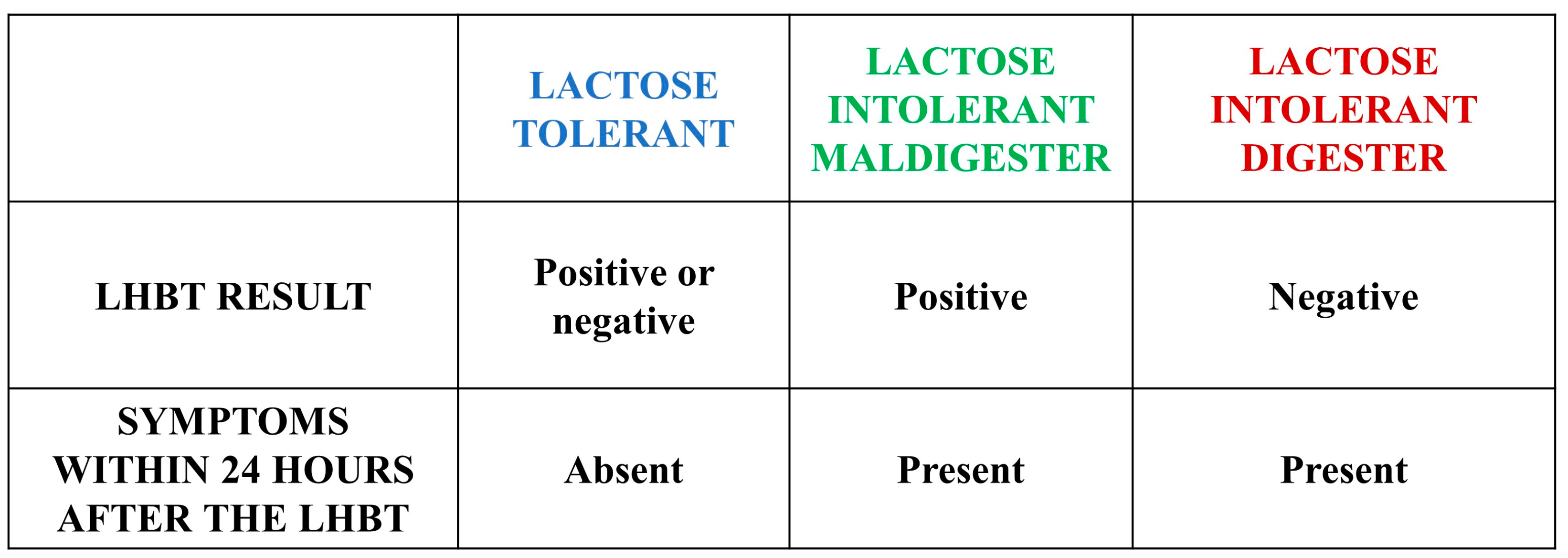
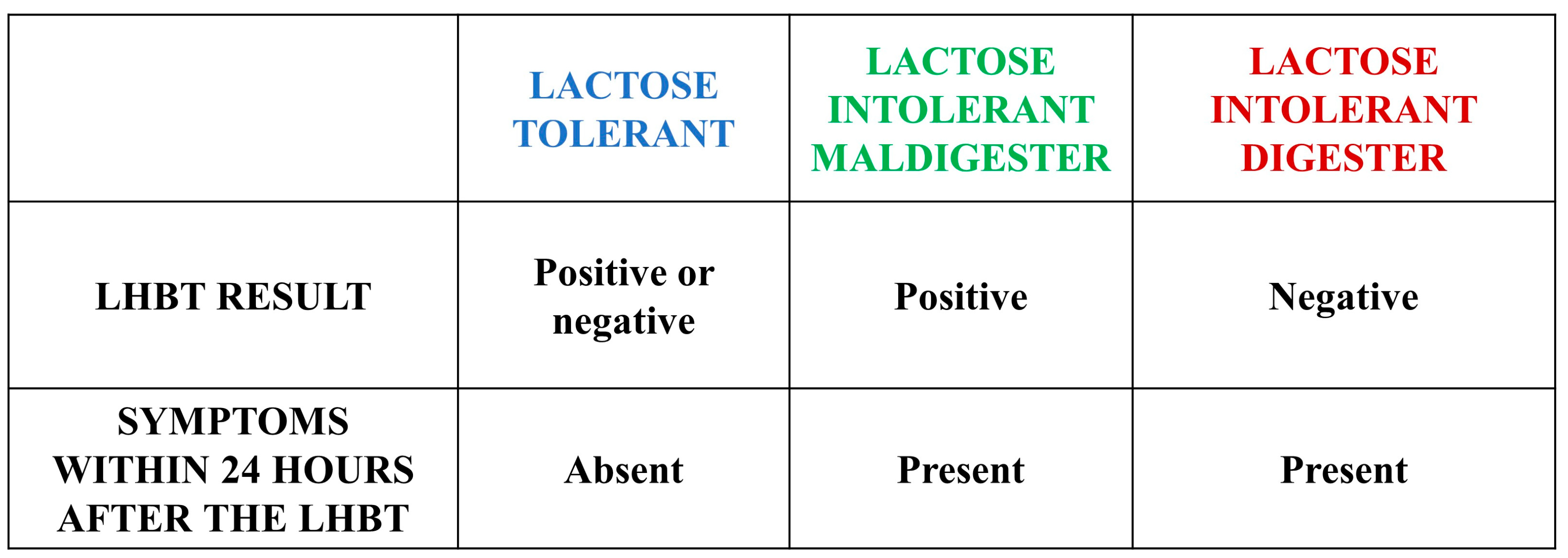
2.3. LHBT
- -
- ‘lactose tolerants’ (maldigesters/tolerants plus digesters/tolerants);
- -
- ‘maldigesters/intolerants’;
- -
- ‘digesters/intolerants’.
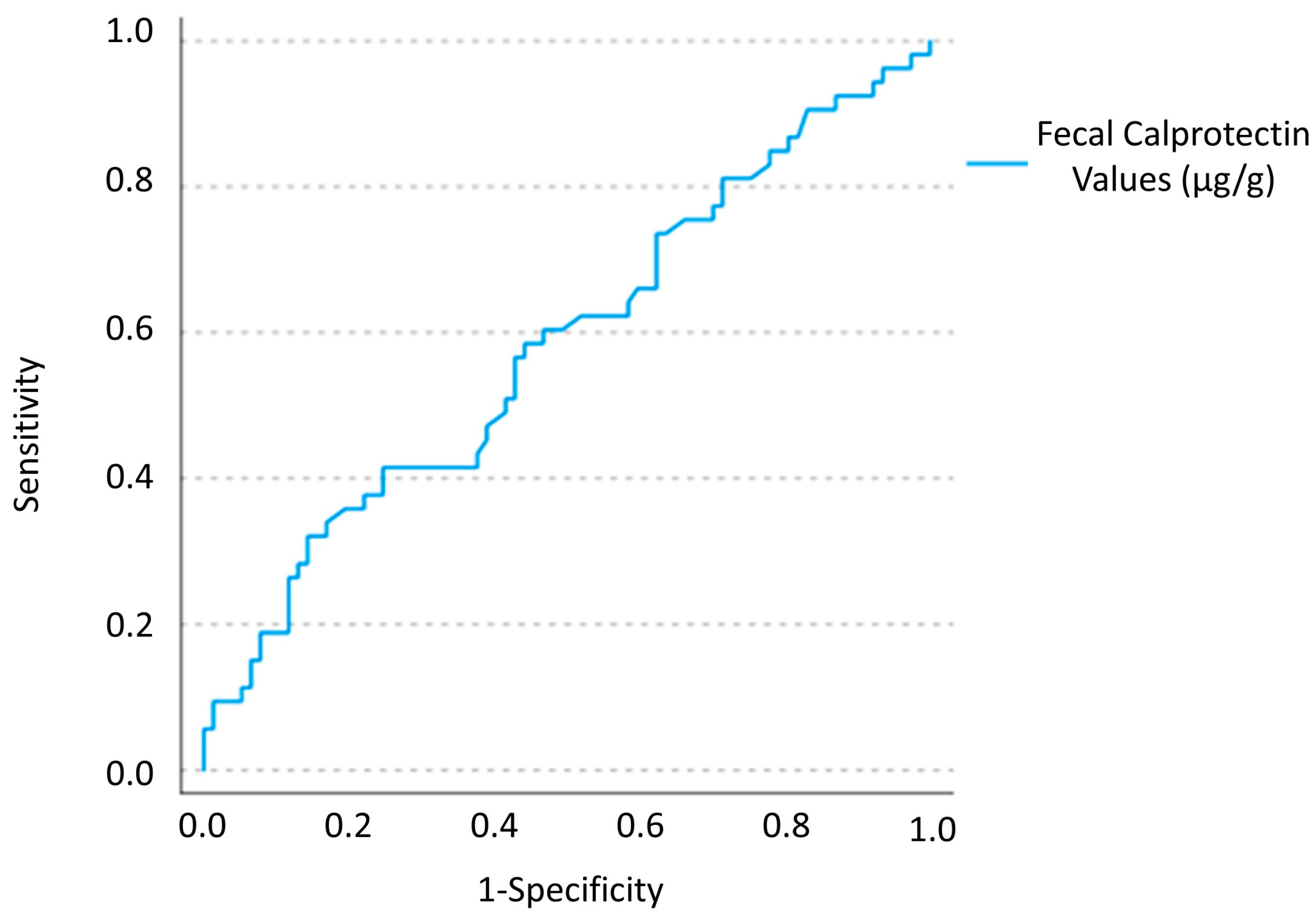
2.4. Fecal Calprotectin
2.4.1. Collection of the Fecal Samples
2.4.2. FCP Measurement
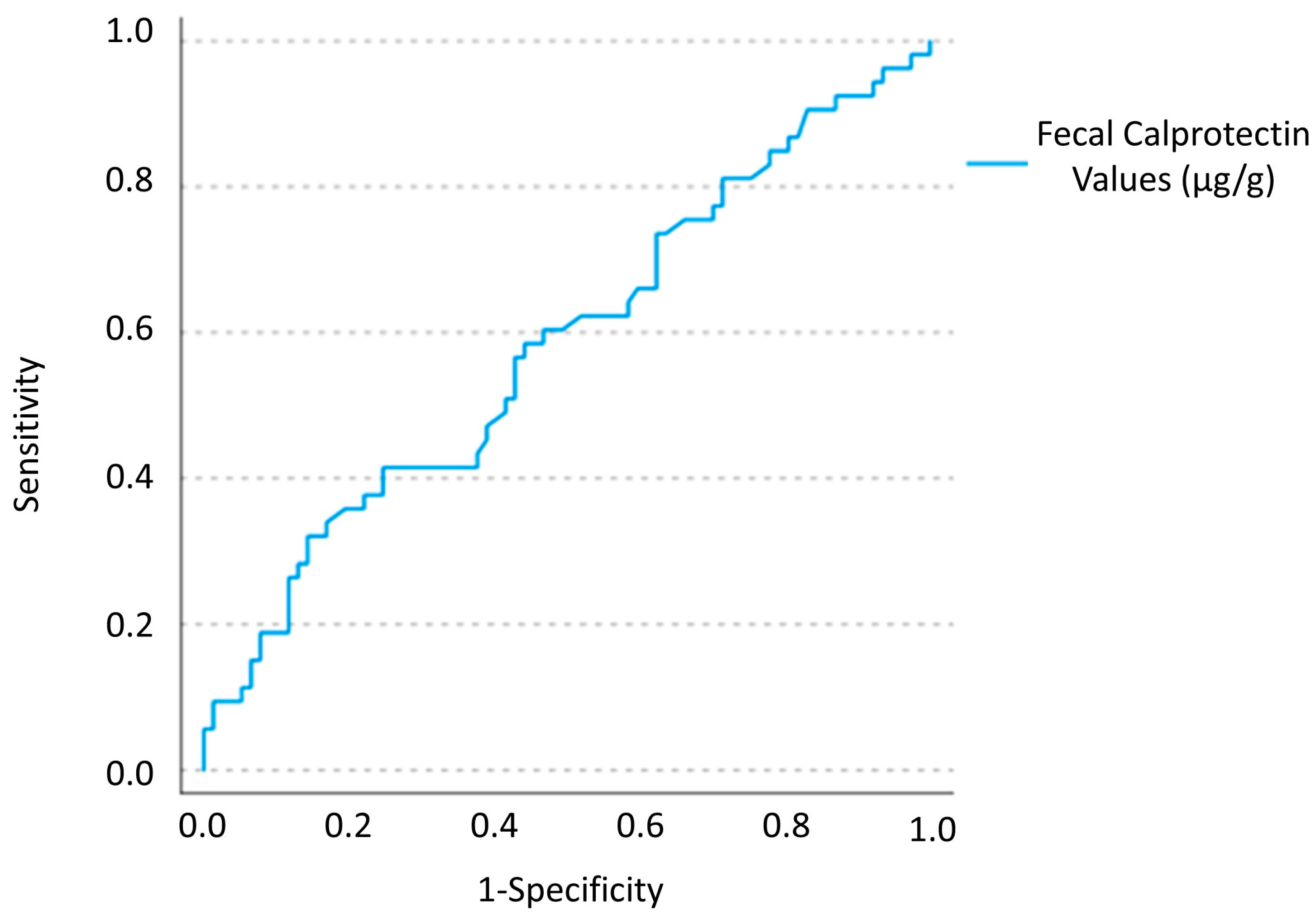
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Catanzaro, R.; Sciuto, M.; Marotta, F. Lactose intolerance: An update on its pathogenesis, diagnosis, and treatment. Nutr. Res. 2021, 89, 23–34. [Google Scholar] [CrossRef]
- Matthews, S.B.; Waud, J.P.; Roberts, A.G.; Campbell, A.K. Systemic lactose intolerance: A new perspective on an old problem. Postgrad. Med. J. 2005, 81, 167–173. [Google Scholar] [CrossRef] [Green Version]
- Ugidos-Rodríguez, S.; Matallana-González, M.C.; Sánchez-Mata, M.C. Lactose malabsorption and intolerance: A review. Food Funct. 2018, 9, 4056–4068. [Google Scholar] [CrossRef]
- Franzè, A.; Bertelè, A. Intolleranza al lattosio nella pratica clinica. Riv. Della Soc. Ital. Med. Gen. 2010, 3, 36–40. [Google Scholar]
- DiPalma, J.A.; Narvaez, R.M. Prediction of lactose malabsorption in referral patients. Dig. Dis. Sci. 1988, 33, 303–307. [Google Scholar] [CrossRef]
- Luyt, D.; Ball, H.; Makwana, N.; Green, M.R.; Bravin, K.; Nasser, S.M.; Clark, A.T. BSACI guideline for the diagnosis and management of cow’s milk allergy. Clin. Exp. Allergy 2014, 44, 642–672. [Google Scholar] [CrossRef]
- Mousan, G.; Kamat, D. Cow’s Milk Protein Allergy. Clin. Pediatr. 2016, 55, 1054–1063. [Google Scholar] [CrossRef]
- Carroccio, A.; Soresi, M.; Mantia, B.; Fayer, F.; La Blasca, F.; Seidita, A.; D’Alcamo, A.; Florena, A.M.; Tinè, C.; Garlisi, C.; et al. Whole Cow’s Milk but Not Lactose Can Induce Symptoms in Patients with Self-Reported Milk Intolerance: Evidence of Cow’s Milk Sensitivity in Adults. Nutrients 2021, 13, 3833. [Google Scholar] [CrossRef]
- Berni Canani, R.; Rapacciuolo, L.; Romano, M.T.; Tanturri de Horatio, L.; Terrin, G.; Manguso, F.; Cirillo, P.; Paparo, F.; Troncone, R. Diagnostic value of faecal calprotectin in paediatric gastroenterology clinical practice. Dig. Liver Dis. 2004, 36, 467–470. [Google Scholar] [CrossRef]
- Carroccio, A.; Iacono, G.; Cottone, M.; Di Prima, L.; Cartabellotta, F.; Cavataio, F.; Scalici, C.; Montalto, G.; Di Fede, G.; Rini, G.; et al. Diagnostic accuracy of fecal calprotectin assay in distinguishing organic causes of chronic diarrhea from irritable bowel syndrome: A prospective study in adults and children. Clin. Chem. 2003, 49, 861–867. [Google Scholar] [CrossRef]
- Merras-Salmio, L.; Kolho, K.L.; Pelkonen, A.S.; Kuitunen, M.; Mäkelä, M.J.; Savilahti, E. Markers of gut mucosal inflammation and cow’s milk specific immunoglobulins in non-IgE cow’s milk allergy. Clin. Transl. Allergy 2014, 4, 8. [Google Scholar] [CrossRef] [Green Version]
- Marsh, M.N. Gluten, major histocompatibility complex, and the small intestine. A molecular and immunobiologic approach to the spectrum of gluten sensitivity (‘celiac sprue’). Gastroenterology 1992, 102, 330–354. [Google Scholar] [CrossRef]
- Oberhuber, G.; Granditsch, G.; Vogelsang, H. The histopathology of coeliac disease: Time for a standardized report scheme for pathologists. Eur. J. Gastroenterol. Hepatol. 1999, 11, 1185–1194. [Google Scholar] [CrossRef]
- Misselwitz, B.; Butter, M.; Verbeke, K.; Fox, M.R. Update on lactose malabsorption and intolerance: Pathogenesis, diagnosis and clinical management. Gut 2019, 68, 2080–2091. [Google Scholar] [CrossRef] [Green Version]
- Storhaug, C.L.; Fosse, S.K.; Fadnes, L.T. Country, regional, and global estimates for lactose malabsorption in adults: A systematic review and meta-analysis. Gastroenterol. Hepatol. 2017, 2, 738–746. [Google Scholar] [CrossRef] [Green Version]
- Zheng, X.; Chu, H.; Cong, Y.; Deng, Y.; Long, Y.; Zhu, Y.; Pohl, D.; Fried, M.; Dai, N.; Fox, M. Self-reported lactose intolerance in clinic patients with functional gastrointestinal symptoms: Prevalence, risk factors, and impact on food choices. Neurogastroenterol. Motil. 2015, 27, 1138–1146. [Google Scholar] [CrossRef]
- Bozzani, A.; Penagini, R.; Velio, P.; Camboni, G.; Corbellini, A.; Quatrini, M.; Conte, D.; Bianchi, P.A. Lactose malabsorption and intolerance in Italians. Clinical implications. Dig. Dis. Sci. 1986, 31, 1313–1316. [Google Scholar] [CrossRef]
- Farup, P.G.; Monsbakken, K.W.; Vandvik, P.O. Lactose malabsorption in a population with irritable bowel syndrome: Prevalence and symptoms. A case-control study. Scand. J. Gastroenterol. 2004, 39, 645–649. [Google Scholar] [CrossRef]
- Bianchi Porro, G.; Parente, F.; Sangaletti, O. Lactose intolerance in adults with chronic unspecific abdominal complaints. Hepatogastroenterol. 1983, 30, 254–257. [Google Scholar]
- Gupta, D.; Ghoshal, U.C.; Misra, A.; Choudhuri, G.; Singh, K. Lactose intolerance in patients with irritable bowel syndrome from northern India: A case-control study. J. Gastroenterol. Hepatol. 2007, 22, 2261–2265. [Google Scholar] [CrossRef]
- Sciarretta, G.; Giacobazzi, G.; Verri, A.; Zanirato, P.; Garuti, G.; Malaguti, P. Hydrogen breath test quantification and clinical correlation of lactose malabsorption in adult irritable bowel syndrome and ulcerative colitis. Dig. Dis. Sci. 1984, 29, 1098–1104. [Google Scholar] [CrossRef] [PubMed]
- Jellema, P.; Schellevis, F.G.; van der Windt, D.A.; Kneepkens, C.M.; van der Horst, H.E. Lactose malabsorption and intolerance: A systematic review on the diagnostic value of gastrointestinal symptoms and self-reported milk intolerance. QJM 2010, 103, 555–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ertekin, V.; Selimoğlu, M.A.; Turgut, A.; Bakan, N. Fecal calprotectin concentration in celiac disease. J. Clin. Gastroenterol. 2010, 44, 544–546. [Google Scholar] [CrossRef]
- Røseth, A.G.; Fagerhol, M.K.; Aadland, E.; Schjønsby, H. Assessment of the neutrophil dominating protein calprotectin in feces. A methodologic study. Scand. J. Gastroenterol. 1992, 27, 793–798. [Google Scholar] [CrossRef]
- Costa, F.; Mumolo, M.G.; Bellini, M.; Romano, M.R.; Ceccarelli, L.; Arpe, P.; Sterpi, C.; Marchi, S.; Maltinti, G. Role of faecal calprotectin as non-invasive marker of intestinal inflammation. Dig. Liver Dis. 2003, 35, 642–647. [Google Scholar] [CrossRef]
- Bertani, L.; Mumolo, M.G.; Tapete, G.; Albano, E.; Baiano Svizzero, G.; Zanzi, F.; Ceccarelli, L.; Bellini, M.; Marchi, S.; Costa, F. Fecal calprotectin: Current and future perspectives for inflammatory bowel disease treatment. Eur. J. Gastroenterol. Hepatol. 2020, 32, 1091–1098. [Google Scholar] [CrossRef]
- Drossman, D.A. Functional Gastrointestinal Disorders: History, Pathophysiology, Clinical Features and Rome IV. Gastroenterol. 2016, 150, 1262–1279. [Google Scholar] [CrossRef] [Green Version]
- Maaser, C.; Sturm, A.; Vavricka, S.R.; Kucharzik, T.; Fiorino, G.; Annese, V.; Calabrese, E.; Baumgart, D.C.; Bettenworth, D.; Borralho Nunes, P.; et al. European Crohn’s and Colitis Organisation [ECCO] and the European Society of Gastrointestinal and Abdominal Radiology [ESGAR]. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial diagnosis, monitoring of known IBD, detection of complications. J. Crohns Colitis 2019, 1, 144–164. [Google Scholar]
- Mari, A.; Baker, F.A.; Mahamid, M.; Yacoob, A.; Sbeit, W.; Khoury, T. Clinical utility of fecal calprotectin: Potential applications beyond inflammatory bowel disease for the primary care physician. Ann. Gastroenterol. 2019, 32, 425–430. [Google Scholar] [CrossRef]
- Wildt, S.; Nordgaard-Lassen, I.; Bendtsen, F.; Rumessen, J.J. Metabolic and inflammatory faecal markers in collagenous colitis. Eur. J. Gastroenterol. Hepatol. 2007, 19, 567–574. [Google Scholar] [CrossRef]
- Von Arnim, U.; Wex, T.; Ganzert, C.; Schulz, C.; Malfertheiner, P. Fecal calprotectin: A marker for clinical differentiation of microscopic colitis and irritable bowel syndrome. Clin. Exp. Gastroenterol. 2016, 9, 97–103. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, S. Testing for Fecal Calprotectin in Food Protein-Induced Enterocolitis Syndrome. J. Investig. Allergol. Clin. Immunol. 2018, 28, 287–288. [Google Scholar] [CrossRef] [PubMed]
- Beşer, O.F.; Sancak, S.; Erkan, T.; Kutlu, T.; Cokuğraş, H.; Cokuğraş, F.Ç. Can Fecal Calprotectin Level Be Used as a Markers of Inflammation in the Diagnosis and Follow-Up of Cow’s Milk Protein Allergy? Allergy Asthma Immunol. Res. 2014, 6, 33–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, L.; Wang, J.; Ren, F.; Shen, L.; Li, F. Can fecal calprotectin levels be used to monitor infant milk protein allergies? Allergy Asthma Clin. Immunol. 2021, 17, 132. [Google Scholar] [CrossRef]
- Lendvai-Emmert, D.; Emmert, V.; Makai, A.; Fusz, K.; Prémusz, V.; Eklics, K.; Sarlós, P.; Tóth, P.; Amrein, K.; Tóth, G. Fecal calprotectin levels in pediatric cow’s milk protein allergy. Front. Pediatr. 2022, 9, 945212. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.H.; Wang, W.; Zhang, X.H.; Pan, J.; Chen, X. Fecal Calprotectin in Children with Cow’s Milk Protein Allergy: A Systematic Review and Meta-Analysis. Int. Arch. Allergy Immunol. 2022, 183, 1189–1197. [Google Scholar] [CrossRef]
- Chin, K.C.; Tarlow, M.J.; Allfree, A.J. Allergy to cows’ milk presenting as chronic constipation. Br. Med. J. (Clin. Res. Ed.) 1983, 287, 1593. [Google Scholar] [CrossRef] [Green Version]
- Iacono, G.; Cavataio, F.; Montalto, G.; Florena, A.; Tumminello, M.; Soresi, M.; Notarbartolo, A.; Carroccio, A. Intolerance of cow’s milk and chronic constipation in children. N. Engl. J. Med. 1998, 339, 1100–1104. [Google Scholar] [CrossRef]
- Iacono, G.; Carroccio, A.; Cavataio, F.; Montalto, G.; Cantarero, M.D.; Notarbartolo, A. Chronic constipation as a symptom of cow milk allergy. J. Pediatr. 1995, 126, 34–39. [Google Scholar] [CrossRef]
- Shah, N.; Lindley, K.; Milla, P. Cow’s milk and chronic constipation in children. N. Engl. J. Med. 1999, 340, 891–892. [Google Scholar]
- Carroccio, A.; Iacono, G. Review article: Chronic constipation and food hypersensitivity--an intriguing relationship. Aliment. Pharmacol. Ther. 2006, 24, 1295–1304. [Google Scholar] [CrossRef] [PubMed]
- Carroccio, A.; Di Prima, L.; Iacono, G.; Florena, A.M.; D’Arpa, F.; Sciumè, C.; Cefalù, A.B.; Noto, D.; Averna, M.R. Multiple food hypersensitivity as a cause of refractory chronic constipation in adults. Scand. J. Gastroenterol. 2006, 41, 498–504. [Google Scholar] [CrossRef] [Green Version]
- Zingone, F.; Maimaris, S.; Auricchio, R.; Caio, G.P.I.; Carroccio, A.; Elli, L.; Galliani, E.; Montagnani, M.; Valiante, F.; Biagi, F. Guidelines of the Italian societies of gastroenterology on the diagnosis and management of coeliac disease and dermatitis herpetiformis. Dig. Liver Dis. 2022, 54, 1304–1319. [Google Scholar] [CrossRef] [PubMed]
- Carroccio, A.; Mansueto, P.; D’Alcamo, A.; Iacono, G. Non-celiac wheat sensitivity as an allergic condition: Personal experience and narrative review. Am. J. Gastroenterol. 2013, 108, 1845–1852. [Google Scholar] [CrossRef] [PubMed]
- Fritscher-Ravens, A.; Pflaum, T.; Mösinger, M.; Ruchay, Z.; Röcken, C.; Milla, P.J.; Das, M.; Böttner, M.; Wedel, T.; Schuppan, D. Many Patients With Irritable Bowel Syndrome Have Atypical Food Allergies Not Associated With Immunoglobulin E. Gastroenterology 2019, 157, 109–118.e5. [Google Scholar] [CrossRef] [Green Version]
- Carroccio, A.; Brusca, I.; Mansueto, P.; Pirrone, G.; Barrale, M.; Di Prima, L.; Ambrosiano, G.; Iacono, G.; Lospalluti, M.L.; La Chiusa, S.M.; et al. A cytologic assay for diagnosis of food hypersensitivity in patients with irritable bowel syndrome. Clin. Gastroenterol. Hepatol. 2010, 8, 254–260. [Google Scholar] [CrossRef]
- Carroccio, A.; Mansueto, P.; Iacono, G.; Soresi, M.; D’Alcamo, A.; Cavataio, F.; Brusca, I.; Florena, A.M.; Ambrosiano, G.; Seidita, A.; et al. Non-celiac wheat sensitivity diagnosed by double-blind placebo-controlled challenge: Exploring a new clinical entity. Am. J. Gastroenterol. 2012, 107, 1898–1906. [Google Scholar] [CrossRef] [Green Version]
- Fritscher-Ravens, A.; Schuppan, D.; Ellrichmann, M.; Schoch, S.; Röcken, C.; Brasch, J.; Bethge, J.; Böttner, M.; Klose, J.; Milla, P.J. Confocal endomicroscopy shows food-associated changes in the intestinal mucosa of patients with irritable bowel syndrome. Gastroenterology 2014, 147, 1012–1020.e4. [Google Scholar] [CrossRef]
- Lapides, R.A.; Savaiano, D.A. Gender, Age, Race and Lactose Intolerance: Is There Evidence to Support a Differential Symptom Response? A Scoping Review. Nutrients 2018, 11, 1956. [Google Scholar] [CrossRef] [Green Version]
- Toro-Monjaraz, E.M.; Fonseca-Camarillo, G.; Zárate-Mondragón, F.; Montijo-Barrios, E.; Cadena-León, J.; Avelar-Rodríguez, D.; Ramírez-Mayans, J.; Cervantes-Bustamante, R.; Yamamoto-Furusho, J.K. Differential Cytokine Expression in the Duodenum and Rectum of Children with Non-Immunoglobulin E-Mediated Cow’s Milk Protein Allergy. Dig. Dis. Sci. 2021, 66, 3769–3775. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| SRMI 1 (n = 329) (%) (A + B + C) | SRMI 1 Lactose Tolerants 2 (n = 104) (%) (A) | SRMI 1 Maldigesters/ Intolerants 3 (n = 187) (%) (B) | SRMI 1 Digesters/ Intolerants 4 (n = 38) (%) (C) | p | |
|---|---|---|---|---|---|
| Gender | A vs. B 0.02 | ||||
| Female | 271 (82.4) | 78 (75.0) | 162 (86.6) | 31 (81.6) | |
| Male | 58 (17.6) | 26 (25.0) | 25 (13.4) | 7 (18.4) | |
| Age at symptoms onset (years) (mean ± SD 10) | 28.8 ± 13.9 | 29.5 ± 14.1 | 29.4 ± 14.0 | 22.5 ± 10.6 | A vs. C 0.03 B vs. C < 0.02 |
| IBS 5-like symptoms | |||||
| None | 106 (32.2) | 30 (28.8) | 67 (35.8) | 9 (23.7) | NS 11 |
| Diarrhea | 168 (51.1) | 55 (52.9) | 92 (49.2) | 21 (55.3) | NS 11 |
| Constipation | 13 (4.0) | 6 (5.8) | 5 (2.7) | 2 (5.3) | NS 11 |
| Mixed bowel habits | 42 (12.8) | 13 (12.5) | 22 (12.3) | 6 (15.8) | NS 11 |
| Dyspepsia-like | 244 (74.2) | 74 (71.2) | 143 (76.5) | 27 (71.1) | NS 11 |
| Extraintestinal symptoms | 75 (22.8) | 31 (29.8) | 38 (20.3) | 6 (15.8) | NS 11 |
| Anemia | 62 (18.8) | 28 (26.9) | 28 (15.0) | 6 (15.8) | A vs. B 0.02 |
| Weight loss | 65 (19.8) | 25 (24.0) | 34 (18.2) | 6 (15.8) | NS 11 |
| Autoimmune diseases | 48 (14.6) | 16 (15.4) | 28 (15.0) | 4 (10.5) | NS 11 |
| Hashimoto thyroiditis | 35 (10.6) | 12 (11.5) | 21 (11.2) | 2 (5.3) | NS 11 |
| Celiac disease | 32 (9.7) | 12 (11.5) | 19 (10.2) | 1 (2.6) | NS 11 |
| NCWS 6 | 105 (31.9) | 32 (30.8) | 61 (32.6) | 12 (31.6) | NS 11 |
| SNAS 7 | 41 (12.5) | 14 (13.5) | 26 (13.9) | 1 (2.6) | NS 11 |
| MFH 8 | 25 (7.6) | 12 (11.5) | 7 (3.7) | 6 (15.8) | A vs. B < 0.04 B vs. C < 0.02 |
| HLA 9 DQ2-DQ8 positivity | 176 (53.5) | 63 (60.6) | 99 (52.9) | 14 (36.8) | NS 11 |
| Duodenal biopsy Marsh classification | |||||
| Stage 0 | 37/80 (46.3) | 12/22 (54.5) | 23/48 (47.9) | 2/10 (20.0) | NS 11 |
| Stage 1 | 41/80 (51.2) | 10/22 (45.5) | 24/48 (50.0) | 7/10 (70.0) | NS 11 |
| Stage 2 | 2/80 (2.5) | 0/22 (0.0) | 1/48 (2.1) | 1/10 (10.0) | NS 11 |
| SRMI 1 (n = 329) (A + B+C) | SRMI 1 Lactose Tolerants 2 (n = 104) (%) (A) | SRMI 1 Maldigesters/ Intolerants 3 (n = 187) (%) (B) | SRMI 1 Digesters/ Intolerants 4 (n = 38) (%) (C) | p | |
|---|---|---|---|---|---|
| Fecal calprotectin | A vs. C <0.0001 B vs. C <0.0001 A vs. C 0.04 | ||||
| Positive (r.v. 5 > 50 mg/g | 172 (52.3) | 60 (57.7) | 97 (51.9) | 15 (39.4) | |
| Median (IQR 6) | 106 | 130 | 100 | 98 | |
| (mg/g) > 50 | (75–171) | (94.75–220.5) | (69.6–164.25) | (100–349) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seidita, A.; Mansueto, P.; Giuliano, A.; Chiavetta, M.; Soresi, M.; Carroccio, A.; the Internal Medicine Study Group. Fecal Calprotectin in Self-Reported Milk Intolerance: Not Only Lactose Intolerance. Nutrients 2023, 15, 1048. https://doi.org/10.3390/nu15041048
Seidita A, Mansueto P, Giuliano A, Chiavetta M, Soresi M, Carroccio A, the Internal Medicine Study Group. Fecal Calprotectin in Self-Reported Milk Intolerance: Not Only Lactose Intolerance. Nutrients. 2023; 15(4):1048. https://doi.org/10.3390/nu15041048
Chicago/Turabian StyleSeidita, Aurelio, Pasquale Mansueto, Alessandra Giuliano, Marta Chiavetta, Maurizio Soresi, Antonio Carroccio, and the Internal Medicine Study Group. 2023. "Fecal Calprotectin in Self-Reported Milk Intolerance: Not Only Lactose Intolerance" Nutrients 15, no. 4: 1048. https://doi.org/10.3390/nu15041048
APA StyleSeidita, A., Mansueto, P., Giuliano, A., Chiavetta, M., Soresi, M., Carroccio, A., & the Internal Medicine Study Group. (2023). Fecal Calprotectin in Self-Reported Milk Intolerance: Not Only Lactose Intolerance. Nutrients, 15(4), 1048. https://doi.org/10.3390/nu15041048