
Association of Protein Intake with Handgrip Strength and Its Relation to Strength Exercise in Korean Adults Aged over 60 Years in the KNHANES (2014-18)

Abstract
1. Introduction
2. Methods
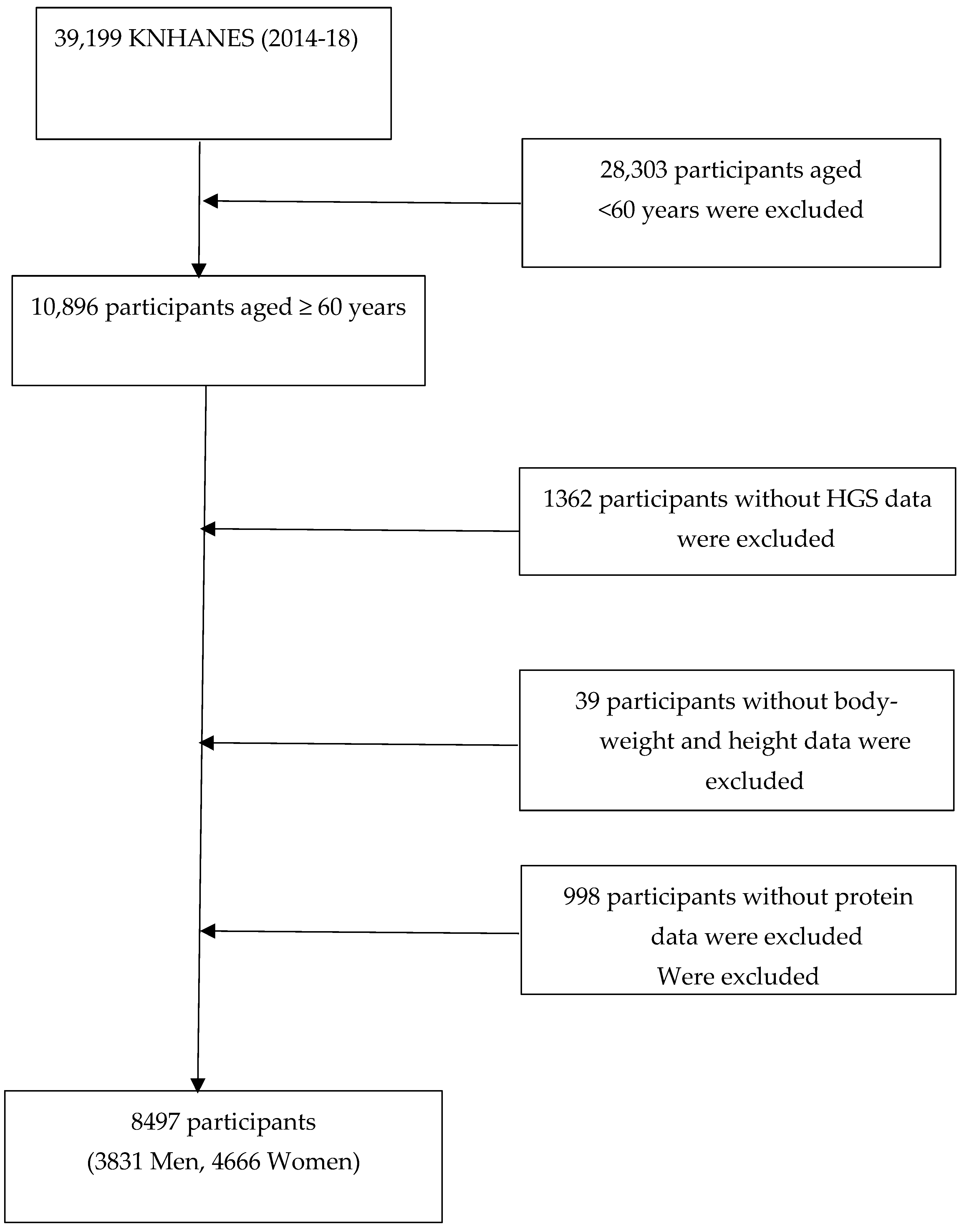
2.1. Study Subjects
2.2. Anthropometry and HGS Measurements
2.3. Protein Intake Assessment
2.4. Physical Activity Assessment
2.5. Assessment of Covariates
2.6. Statistical Analysis
3. Results
4. Discussion
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lawman, H.G.; Troiano, R.P.; Perna, F.M.; Wang, C.Y.; Fryar, C.D.; Ogden, C.L. Associations of Relative Handgrip Strength and Cardiovascular Disease Biomarkers in U.S. Adults, 2011–2012. Am. J. Prev. Med. 2016, 50, 677–683. [Google Scholar] [CrossRef] [PubMed]
- McGrath, R.P.; Kraemer, W.J.; Snih, S.A.; Peterson, M.D. Handgrip Strength and Health in Aging Adults. Sports Med. 2018, 48, 1993–2000. [Google Scholar] [CrossRef] [PubMed]
- Labott, B.K.; Bucht, H.; Morat, M.; Morat, T.; Donath, L. Effects of Exercise Training on Handgrip Strength in Older Adults: A Meta-Analytical Review. Gerontology 2019, 65, 686–698. [Google Scholar] [CrossRef] [PubMed]
- Cermak, N.M.; Res, P.T.; de Groot, L.C.; Saris, W.H.; van Loon, L.J. Protein supplementation augments the adaptive response of skeletal muscle to resistance-type exercise training: A meta-analysis. Am. J. Clin. Nutr. 2012, 96, 1454–1464. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Calvani, R.; Tosato, M.; Martone, A.M.; Ortolani, E.; Savera, G.; D’Angelo, E.; Sisto, A.; Marzetti, E. Protein Intake and Muscle Health in Old Age: From Biological Plausibility to Clinical Evidence. Nutrients 2016, 8, 295. [Google Scholar] [CrossRef] [PubMed]
- Atherton, P.J.; Smith, K. Muscle protein synthesis in response to nutrition and exercise. J. Physiol. 2012, 590, 1049–1057. [Google Scholar] [CrossRef]
- Morais, J.A.; Chevalier, S.; Gougeon, R. Protein turnover and requirements in the healthy and frail elderly. J. Nutr. Health Aging 2006, 10, 272–283. [Google Scholar]
- Bauer, J.; Biolo, G.; Cederholm, T.; Cesari, M.; Cruz-Jentoft, A.J.; Morley, J.E.; Phillips, S.; Sieber, C.; Stehle, P.; Teta, D.; et al. Evidence-based recommendations for optimal dietary protein intake in older people: A position paper from the PROT-AGE Study Group. J. Am. Med. Dir. Assoc. 2013, 14, 542–559. [Google Scholar] [CrossRef]
- Kirwan, R.P.; Mazidi, M.; Rodriguez Garcia, C.; Lane, K.E.; Jafari, A.; Butler, T.; Perez de Heredia, F.; Davies, I.G. Protein interventions augment the effect of resistance exercise on appendicular lean mass and handgrip strength in older adults: A systematic review and meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2022, 115, 897–913. [Google Scholar] [CrossRef]
- Kim, H.N.; Kim, S.H.; Eun, Y.M.; Song, S.W. Impact of dietary protein intake on the incidence of low muscle strength in middle-aged and older adults. Clin. Nutr. 2021, 40, 1467–1474. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.R.; Jeon, Y.J.; Jeong, T. Risk factors associated with low handgrip strength in the older Korean population. PLoS ONE 2019, 14, e0214612. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.K.; Woo, J.; Assantachai, P.; Auyeung, T.W.; Chou, M.Y.; Iijima, K.; Jang, H.C.; Kang, L.; Kim, M.; Kim, S.; et al. Asian Working Group for Sarcopenia: 2019 Consensus Update on Sarcopenia Diagnosis and Treatment. J. Am. Med. Dir. Assoc. 2020, 21, 300–307.e302. [Google Scholar] [CrossRef] [PubMed]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [PubMed]
- National Academy of Agricultural Sciences. Korean Standard Food Composition Table; National Academy of Agricultural Sciences: Suwon, Republic of Korea, 2016; pp. 1–570. [Google Scholar]
- Park, S.H.; Kim, S.N.; Lee, S.H.; Choe, J.S.; Choi, Y. Development of 9th Revision Korean Food Composition Table and Its Major Changes. Korean J. Community Nutr. 2018, 23, 352–365. [Google Scholar] [CrossRef]
- Lee, J.; Lee, C.; Min, J.; Kang, D.W.; Kim, J.Y.; Yang, H.I.; Park, J.; Lee, M.K.; Lee, M.Y.; Park, I.; et al. Development of the Korean Global Physical Activity Questionnaire: Reliability and validity study. Glob. Health Promot. 2020, 27, 44–55. [Google Scholar] [CrossRef]
- Gregorio, L.; Brindisi, J.; Kleppinger, A.; Sullivan, R.; Mangano, K.M.; Bihuniak, J.D.; Kenny, A.M.; Kerstetter, J.E.; Insogna, K.L. Adequate dietary protein is associated with better physical performance among post-menopausal women 60-90 years. J. Nutr. Health Aging 2014, 18, 155–160. [Google Scholar] [CrossRef]
- Isanejad, M.; Mursu, J.; Sirola, J.; Kroger, H.; Rikkonen, T.; Tuppurainen, M.; Erkkila, A.T. Dietary protein intake is associated with better physical function and muscle strength among elderly women. Br. J. Nutr. 2016, 115, 1281–1291. [Google Scholar] [CrossRef]
- Granic, A.; Mendonca, N.; Sayer, A.A.; Hill, T.R.; Davies, K.; Adamson, A.; Siervo, M.; Mathers, J.C.; Jagger, C. Low protein intake, muscle strength and physical performance in the very old: The Newcastle 85+ Study. Clin. Nutr. 2018, 37, 2260–2270. [Google Scholar] [CrossRef]
- McLean, R.R.; Mangano, K.M.; Hannan, M.T.; Kiel, D.P.; Sahni, S. Dietary Protein Intake Is Protective Against Loss of Grip Strength Among Older Adults in the Framingham Offspring Cohort. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2016, 71, 356–361. [Google Scholar] [CrossRef]
- Tieland, M.; Franssen, R.; Dullemeijer, C.; van Dronkelaar, C.; Kyung Kim, H.; Ispoglou, T.; Zhu, K.; Prince, R.L.; van Loon, L.J.C.; de Groot, L. The Impact of Dietary Protein or Amino Acid Supplementation on Muscle Mass and Strength in Elderly People: Individual Participant Data and Meta-Analysis of RCT’s. J. Nutr. Health Aging 2017, 21, 994–1001. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Park, H.; Cho, Y.; Bong, A. Protein Intake by Korean Adults through Meals. Korean J. Health Promot. 2021, 21, 10. [Google Scholar] [CrossRef]
- Moore, D.R.; Churchward-Venne, T.A.; Witard, O.; Breen, L.; Burd, N.A.; Tipton, K.D.; Phillips, S.M. Protein ingestion to stimulate myofibrillar protein synthesis requires greater relative protein intakes in healthy older versus younger men. J. Gerontol. A Biol. Sci. Med. Sci. 2015, 70, 57–62. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Breen, L.; Burd, N.A.; Hector, A.J.; Churchward-Venne, T.A.; Josse, A.R.; Tarnopolsky, M.A.; Phillips, S.M. Resistance exercise enhances myofibrillar protein synthesis with graded intakes of whey protein in older men. Br. J. Nutr. 2012, 108, 1780–1788. [Google Scholar] [CrossRef]
- Berrazaga, I.; Micard, V.; Gueugneau, M.; Walrand, S. The Role of the Anabolic Properties of Plant- versus Animal-Based Protein Sources in Supporting Muscle Mass Maintenance: A Critical Review. Nutrients 2019, 11, 1825. [Google Scholar] [CrossRef]
- Rand, W.M.; Pellett, P.L.; Young, V.R. Meta-analysis of nitrogen balance studies for estimating protein requirements in healthy adults. Am. J. Clin. Nutr. 2003, 77, 109–127. [Google Scholar] [CrossRef]
- Courtney-Martin, G.; Ball, R.O.; Pencharz, P.B.; Elango, R. Protein Requirements during Aging. Nutrients 2016, 8, 492. [Google Scholar] [CrossRef]
- Granic, A.; Jagger, C.; Davies, K.; Adamson, A.; Kirkwood, T.; Hill, T.R.; Siervo, M.; Mathers, J.C.; Sayer, A.A. Effect of Dietary Patterns on Muscle Strength and Physical Performance in the Very Old: Findings from the Newcastle 85+ Study. PLoS ONE 2016, 11, e0149699. [Google Scholar] [CrossRef]
- Mertz, K.H.; Reitelseder, S.; Bechshoeft, R.; Bulow, J.; Hojfeldt, G.; Jensen, M.; Schacht, S.R.; Lind, M.V.; Rasmussen, M.A.; Mikkelsen, U.R.; et al. The effect of daily protein supplementation, with or without resistance training for 1 year, on muscle size, strength, and function in healthy older adults: A randomized controlled trial. Am. J. Clin. Nutr. 2021, 113, 790–800. [Google Scholar] [CrossRef]
- Hou, L.; Lei, Y.; Li, X.; Huo, C.; Jia, X.; Yang, J.; Xu, R.; Wang, X. Effect of Protein Supplementation Combined with Resistance Training on Muscle Mass, Strength and Function in the Elderly: A Systematic Review and Meta-Analysis. J. Nutr. Health Aging 2019, 23, 451–458. [Google Scholar] [CrossRef]
- Liao, C.D.; Tsauo, J.Y.; Wu, Y.T.; Cheng, C.P.; Chen, H.C.; Huang, Y.C.; Chen, H.C.; Liou, T.H. Effects of protein supplementation combined with resistance exercise on body composition and physical function in older adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2017, 106, 1078–1091. [Google Scholar] [CrossRef] [PubMed]
- Timmons, J.F.; Hone, M.; Cogan, K.E.; Duffy, O.; Egan, B. Increased Leg Strength After Concurrent Aerobic and Resistance Exercise Training in Older Adults Is Augmented by a Whole Food-Based High Protein Diet Intervention. Front. Sports Act. Living 2021, 3, 653962. [Google Scholar] [CrossRef] [PubMed]
- Biolo, G.; Tipton, K.D.; Klein, S.; Wolfe, R.R. An abundant supply of amino acids enhances the metabolic effect of exercise on muscle protein. Am. J. Physiol. 1997, 273, E122–E129. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Men | Women | |||||||
|---|---|---|---|---|---|---|---|---|
| Protein Per kg BW | p | Protein Per kg BW | p | |||||
| <0.8 | ≥0.8 and <1.2 | ≥1.2 | <0.8 | ≥0.8 and <1.2 | ≥1.2 | |||
| Unweighted sample size | 1365 | 1364 | 1102 | 2306 | 1441 | 919 | ||
| Proportion (%) | 34.5 (1.0) | 36.5 (0.9) | 29.0 (0.9) | <0.001 | 49.2 (0.9) | 30.8 (0.8) | 20.0 (0.7) | <0.001 |
| Age, y | 70.2 (0.2) | 68.9 (0.2) | 67.7 (0.2) | <0.001 | 71.3 (0.2) | 69.6 (0.2) | 67.5 (0.2) | <0.001 |
| 60–69 | 48.9 (1.6) | 57.0 (1.5) | 65.8 (1.7) | <0.001 | 41.7 (1.2) | 53.0 (1.6) | 66.4 (1.8) | <0.001 |
| 70–79 | 37.2 (1.5) | 33.5 (1.4) | 28.4 (1.5) | 40.4 (1.2) | 35.2 (1.5) | 26.2 (1.6) | ||
| ≥80 | 13.9 (1.0) | 9.5 (0.9) | 5.8 (0.8) | 17.9 (1.0) | 11.8 (1.0) | 7.4 (1.0) | ||
| BMI, kg/m2 | 24.5 (0.1) | 23.8 (0.1) | 23.3 (0.1) | <0.001 | 25.1 (0.1) | 24.1 (0.1) | 23.3 (0.1) | <0.001 |
| HGS (kg) | 33.3 (0.2) | 35.0 (0.2) | 35.7 (0.2) | <0.001 | 20.3 (0.2) | 20.8 (0.2) | 21.6 (0.2) | <0.001 |
| Protein intake (g/day) | 39.3 (0.3) | 65.5 (0.4) | 104.6 (1.1) | <0.001 | 32.5 (0.2) | 54.8 (0.3) | 87.0 (0.9) | <0.001 |
| Protein intake/kg (g/kg) | 0.6 (0.00) | 1.0 (0.00) | 1.6 (0.02) | <0.001 | 0.6 (0.00) | 1.0 (0.00) | 1.6 (0.02) | <0.001 |
| Currently smoking | 0.091 | 0.561 | ||||||
| no | 75.3 (1.5) | 79.3 (1.3) | 78.4 (1.4) | 97.4 (0.4) | 97.6 (0.5) | 98.2 (0.6) | ||
| yes | 24.7 (1.5) | 20.7 (1.3) | 21.6 (1.4) | 2.6 (0.4) | 2.4 (0.5) | 1.8 (0.6) | ||
| Heavy drinking | 0.014 | 0.001 | ||||||
| no | 89.0 (1.1) | 89.2 (1.1) | 84.8 (1.3) | 99.3 (0.2) | 98.8 (0.3) | 97.6 (0.6) | ||
| yes | 11.0 (1.1) | 10.8 (1.1) | 15.2 (1.3) | 1.7 (0.2) | 1.2 (0.3) | 2.4 (0.6) | ||
| Education | <0.001 | <0.001 | ||||||
| <university | 77.2 (1.4) | 66.8 (1.6) | 64.2 (1.7) | 96.8 (0.48) | 92.2 (0.8) | 86.5 (1.3) | ||
| ≥university | 22.8 (1.4) | 33.2 (1.6) | 35.8 (1.7) | 3.2 (0.4) | 7.8 (0.8) | 13.5 (1.3) | ||
| Aerobic PA | <0.001 | <0.001 | ||||||
| no | 64.6 (1.6) | 57.8 (1.7) | 53.3 (1.7) | 71.6 (1.2) | 65.8 (1.5) | 62.0 (1.9) | ||
| yes | 35.4 (1.6) | 42.2 (1.7) | 46.7 (1.7) | 28.4 (1.2) | 34.2 (1.5) | 38.0 (1.9) | ||
| Strength exercise | <0.001 | <0.001 | ||||||
| no | 77.2 (1.4) | 66.8 (1.6) | 64.2 (1.7) | 91.6 (0.7) | 86.4 (1.1) | 82.8 (1.5) | ||
| yes | 22.8 (1.4) | 33.2 (1.6) | 35.8 (1.7) | 8.4 (0.7) | 13.6 (1.1) | 17.2 (1.5) | ||
| Chronic disease | <0.001 | <0.001 | ||||||
| no | 61.3 (1.7) | 63.3 (1.6) | 70.9 (1.4) | 61.5 (1.3) | 68.7 (1.5) | 72.4 (1.8) | ||
| yes | 38.7 (1.7) | 36.7 (1.6) | 29.1 (1.4) | 38.5 (1.3) | 31.3 (1.5) | 27.6 (1.8) | ||
| Limitation | <0.001 | <0.001 | ||||||
| no | 83.6 (1.2) | 88.5 (1.0) | 91.7 (0.9) | 79.7 (1.1) | 85.5 (1.1) | 89.0 (1.3) | ||
| yes | 16.4 (1.2) | 11.5 (0.9) | 8.3 (0.9) | 20.3 (1.1) | 14.5 (1.1) | 11.0 (1.3) | ||
| Occupation | <0.001 | <0.001 | ||||||
| White collar worker | 37.8 (1.6) | 48.0 (1.9) | 49.4 (1.9) | 40.2 (1.4) | 48.5 (1.7) | 51.6 (2.2) | ||
| Blue collar worker | 62.2 (1.6) | 52.0 (1.9) | 50.6 (1.9) | 59.8 (1.4) | 51.5 (1.7) | 48.4 (2.2) | ||
| Weak HGS | <0.001 | <0.001 | ||||||
| no | 76.3 (1.3) | 83.3 (1.1) | 85.9 (1.2) | 66.4 (1.4) | 73.6 (1.4) | 79.5 (1.5) | ||
| yes | 23.7 (1.3) | 16.7 (1.1) | 14.1 (1.2) | 33.6 (1.4) | 26.4 (1.4) | 20.5 (15) | ||
| Protein Intake Per kg BW | |||||
|---|---|---|---|---|---|
| <0.8 | ≥0.8 and <1.2 | ≥1.2 | p | Ptrend | |
| Men | |||||
| Prevalence (%) | 23.7 (1.3) | 16.7 (1.1) | 14.1 (1.2) | <0.001 | <0.001 |
| Model I | 1.46 (1.16–1.84) | 1.00 | 0.93 (0.71–1.22) | 0.001 | 0.001 |
| Model II | 1.46 (1.16–1.83) | 1.00 | 1.01 (0.73–1.38) | 0.010 | 0.035 |
| Women | |||||
| Prevalence (%) | 33.6 (1.4) | 26.4 (1.4) | 20.5 (1.1) | <0.001 | <0.001 |
| Model I | 1.18 (0.97–1.44) | 1.00 | 0.94 (0.74–1.20) | 0.093 | 0.032 |
| Model II | 1.18 (0.93–1.50) | 1.00 | 0.96 (0.74–1.27) | 0.270 | 0.118 |
| Protein Intake Per kg BW | |||||
|---|---|---|---|---|---|
| < 0.8 | ≥0.8 and <1.2 | ≥1.2 | p | Ptrend | |
| Men | |||||
| Strength exercises | |||||
| No | 1.36 (1.01–1.82) | 1.00 | 1.14 (0.80–1.62) | 0.121 | 0.252 |
| Yes | 1.77 (0.88–3.54) | 1.00 | 0.67 (0.34–1.32) | 0.008 | <0.001 |
| Women | |||||
| Strength exercises | |||||
| No | 1.11 (0.87–1.43) | 1.00 | 0.96 (0.72–1.28) | 0561 | 0.288 |
| Yes | 2.46 (1.03–5.92) | 1.00 | 0.91 (0.35–2.37) | 0.050 | 0.025 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, E.Y. Association of Protein Intake with Handgrip Strength and Its Relation to Strength Exercise in Korean Adults Aged over 60 Years in the KNHANES (2014-18). Nutrients 2023, 15, 1014. https://doi.org/10.3390/nu15041014
Choi EY. Association of Protein Intake with Handgrip Strength and Its Relation to Strength Exercise in Korean Adults Aged over 60 Years in the KNHANES (2014-18). Nutrients. 2023; 15(4):1014. https://doi.org/10.3390/nu15041014
Chicago/Turabian StyleChoi, Eun Young. 2023. "Association of Protein Intake with Handgrip Strength and Its Relation to Strength Exercise in Korean Adults Aged over 60 Years in the KNHANES (2014-18)" Nutrients 15, no. 4: 1014. https://doi.org/10.3390/nu15041014
APA StyleChoi, E. Y. (2023). Association of Protein Intake with Handgrip Strength and Its Relation to Strength Exercise in Korean Adults Aged over 60 Years in the KNHANES (2014-18). Nutrients, 15(4), 1014. https://doi.org/10.3390/nu15041014