
Associations between School Lunch and Obesity in Korean Children and Adolescents Based on the Korea National Health and Nutrition Examination Survey 2017–2019 Data: A Cross-Sectional Study

Abstract
1. Introduction
2. Materials and Methods
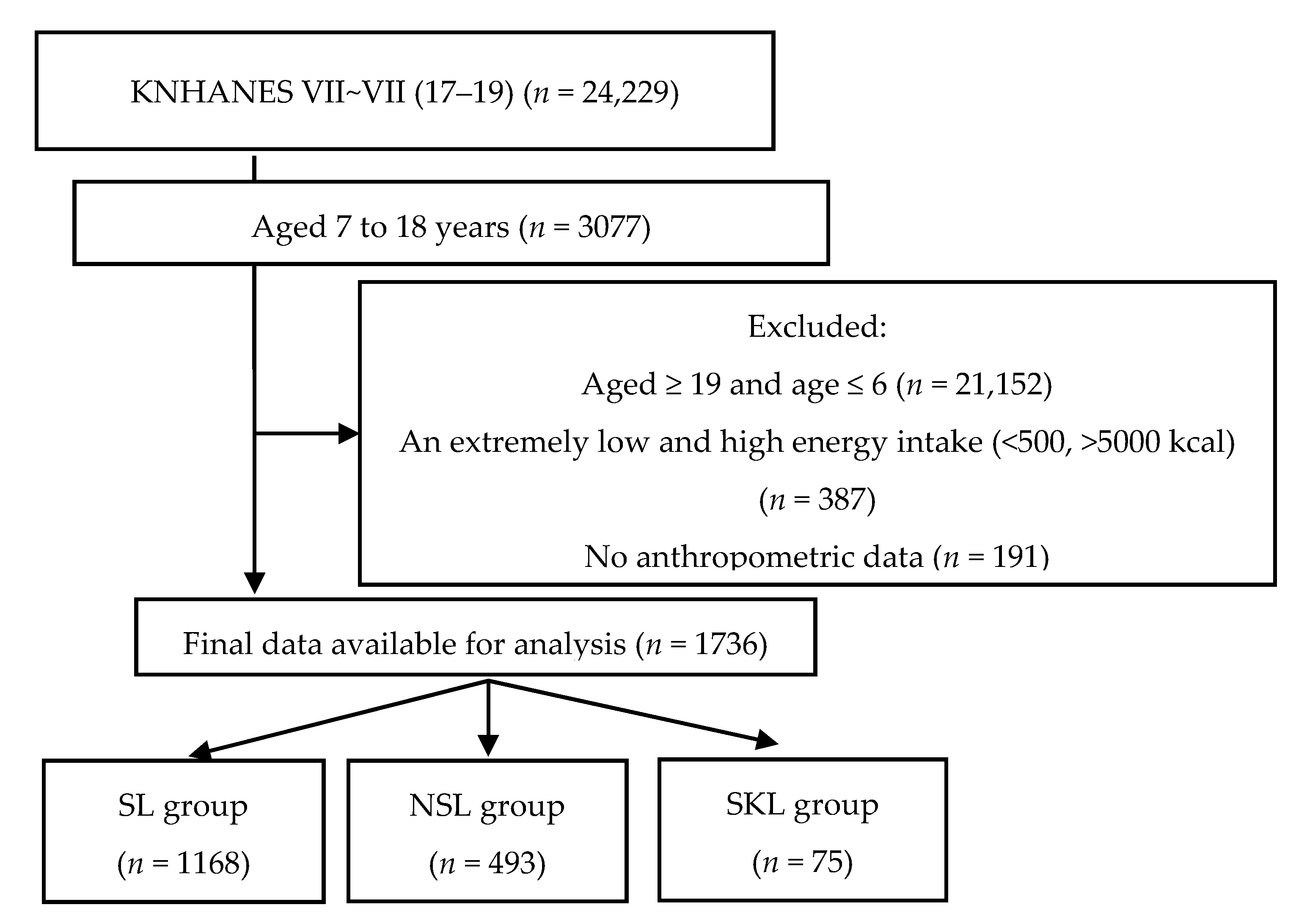
2.1. Data Source and Study Population
2.2. Assessment of Sociodemographic Data
2.3. Anthropometric Measurement
2.4. Dietary Intake and Lunch Type
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| BMI | Body Mass Index |
| KDRIs | Dietary Reference Intakes for Koreans |
| KNHANES | Korea National Health and Nutrition Examination Survey |
| NSL | Non-School Lunch |
| SFA | Saturated Fatty Acids |
| SL | School Lunch |
| SKL | Skipping Lunch |
| WC | Waist Circumference |
References
- World Health Organization. World Obesity Day 2022—Accelerating Action to Stop Obesity. Available online: https://www.who.int/news/item/04-03-2022-world-obesity-day-2022-accelerating-action-to-stop-obesity (accessed on 6 January 2023).
- The Ministry of Education. School Health Examination Data; The Ministry of Education: Sejong, Republic of Korea, 2021. [Google Scholar]
- Lee, H.A.; Lee, W.K.; Kong, K.-A.; Chang, N.; Ha, E.-H.; Hong, Y.S.; Park, H. The effect of eating behavior on being overweight or obese during preadolescence. J. Prev. Med. Public Health 2011, 44, 226. [Google Scholar] [CrossRef] [PubMed]
- Ha, S.A.; Lee, S.Y.; Kim, K.A.; Seo, J.S.; Sohn, C.M.; Park, H.R.; Kim, K.W. Eating habits, physical activity, nutrition knowledge, and self-efficacy by obesity status in upper-grade elementary school students. Nutr. Res. Pract. 2016, 10, 597–605. [Google Scholar] [CrossRef] [PubMed]
- Seo, J.W. Obesity in children and adolescents. Clin. Exp. Pediatr. 2009, 52, 1311–1320. [Google Scholar] [CrossRef]
- Tanaka, N.; Miyoshi, M. School lunch program for health promotion among children in Japan. Asia Pac. J. Clin. Nutr. 2012, 21, 155–158. [Google Scholar] [PubMed]
- Harper, C.; Wells, L. School Meal Provision in England and Other Western Countries: A Review; School Food Trust: Sheffield, UK, 2007. [Google Scholar]
- Caine-Bish, N.; Scheule, B. Food preferences of school age children and adolescents in an Ohio school district. J. Child Nutr. Manag. 2007, 31, 1559–5676. [Google Scholar]
- Miyawaki, A.; Lee, J.; Kobayashi, Y. Impact of the school lunch program on overweight and obesity among junior high school students: A nationwide study in Japan. J. Public Health 2019, 41, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Taber, D.R.; Chriqui, J.F.; Powell, L.; Chaloupka, F.J. Association between state laws governing school meal nutrition content and student weight status: Implications for new USDA school meal standards. JAMA Pediatr. 2013, 167, 513–519. [Google Scholar] [CrossRef]
- Holford, A.; Rabe, B. Going universal. The impact of free school lunches on child body weight outcomes. J. Public Econ. Plus 2022, 3, 100016. [Google Scholar] [CrossRef]
- Bethmann, D.; Cho, J.I. The impacts of free school lunch policies on adolescent BMI and mental health: Evidence from a natural experiment in South Korea. SSM-Popul. Health 2022, 18, 101072. [Google Scholar] [CrossRef]
- Gundersen, C.; Kreider, B.; Pepper, J. The impact of the National School Lunch Program on child health: A nonparametric bounds analysis. J. Econom. 2012, 166, 79–91. [Google Scholar] [CrossRef]
- Lundborg, P.; Rooth, D.-O.; Alex-Petersen, J. Long-term effects of childhood nutrition: Evidence from a school lunch reform. Rev. Econ. Stud. 2022, 89, 876–908. [Google Scholar] [CrossRef]
- Mirtcheva, D.M.; Powell, L.M. National school lunch program participation and child body weight. East. Econ. J. 2013, 39, 328–345. [Google Scholar] [CrossRef]
- Schanzenbach, D.W. Do school lunches contribute to childhood obesity? J. Hum. Resour. 2009, 44, 684–709. [Google Scholar]
- Clark, M.A.; Fox, M.K. Nutritional quality of the diets of US public school children and the role of the school meal programs. J. Am. Diet. Assoc. 2009, 109, S44–S56. [Google Scholar] [CrossRef]
- The Ministry of Education. The Current Status of School Lunch in 2020. Available online: https://www.moe.go.kr/boardCnts/viewRenew.do?boardID=316&lev=0&statusYN=W&s=moe&m=0302&opType=N&boardSeq=84684 (accessed on 12 December 2022).
- Kweon, S.; Kim, Y.; Jang, M.-j.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.-H.; Oh, K. Data resource profile: The Korea national health and nutrition examination survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef]
- Kim, J.H.; Yun, S.; Hwang, S.-s.; Shim, J.O.; Chae, H.W.; Lee, Y.J.; Lee, J.H.; Kim, S.C.; Lim, D.; Yang, S.W. The 2017 Korean National Growth Charts for children and adolescents: Development, improvement, and prospects. Korean J. Pediatr. 2018, 61, 135. [Google Scholar] [CrossRef] [PubMed]
- Korea Center for Disease Control & Prevention. The 2007 Growth Chart for Korean Children. Korea Center for Disease Control & Prevention. Available online: https://www.kdca.go.kr/filepath/boardDownload.es?bid=0019&list_no=138467&seq=644 (accessed on 26 May 2022).
- United States. Government Accountability Office. School Nutrition, USDA Has Efforts Underway to Help Address Ongoing Challenges Implementing Changes in Nutrition Standards; United States Government Accountability Office: Washington, DC, USA, 2015. [Google Scholar]
- Haskins, R. The school lunch lobby: A charmed federal food program that no longer just feeds the hungry. Educ. Next 2005, 5, 10–18. [Google Scholar]
- Physicians Committee for Responsible Medicine. Available online: https://atkinsfacts.org/opinions/pcrm/ (accessed on 26 May 2022).
- Gordon, A.; Hall, J.; Zeidman, E.; Crepinsek, M.K.; Clark, M.; Condon, E. School Nutrition Dietary Assessment Study-III: Volume III: Sampling and Data Collection; Mathematica Policy Research: Princeton, NJ, USA, 2007. [Google Scholar]
- Gould, R.; Russell, J.; Barker, M.E. School lunch menus and 11 to 12 year old children’s food choice in three secondary schools in England—Are the nutritional standards being met? Appetite 2006, 46, 86–92. [Google Scholar] [CrossRef]
- The Ministry of Health and Welfare. Dietary Reference Intakes for Koreans 2020; Ministry of Health and Welfare, The Korean Nutrition Society: Sejong, Republic of Korea, 2020. [Google Scholar]
- Gleason, P.M.; Suitor, C.W. Eating at school: How the National School Lunch Program affects children’s diets. Am. J. Agric. Econ. 2003, 85, 1047–1061. [Google Scholar] [CrossRef]
- Kim, M.-H.; Lee, K.-A. A comparison of the perceptions of children and their mothers of the effects of school lunch programs on children’s dietary behaviors. J. Korean Soc. Food Sci. Nutr. 2003, 32, 636–644. [Google Scholar]
- Bardin, S.; Gola, A.A. Analyzing the association between student weight status and school meal participation: Evidence from the school nutrition and meal cost study. Nutrients 2020, 13, 17. [Google Scholar] [CrossRef]
- Perelló, M.; Zigman, J.M. The role of ghrelin in reward-based eating. Biol. Psychiatry 2012, 72, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.-Y.; Lee, N.-R.; Lee, J.-S.; Choi, Y.-S.; Kwak, T.-K.; Chung, H.R.; Kwon, S.; Choi, Y.-J.; Lee, S.-K.; Kang, M.-H. Meal skipping relates to food choice, understanding of nutrition labeling, and prevalence of obesity in Korean fifth grade children. Nutr. Res. Pract. 2012, 6, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Isganaitis, E.; Lustig, R.H. Fast food, central nervous system insulin resistance, and obesity. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 2451–2462. [Google Scholar] [CrossRef] [PubMed]
- Karatzi, K.; Moschonis, G.; Choupi, E.; Manios, Y.; Skenderi, K.P.; Grammatikaki, E.; Androutsos, O.; Tanagra, S.; Koumpitski, A.; Siatitsa, P.-E. Late-night overeating is associated with smaller breakfast, breakfast skipping, and obesity in children: The Healthy Growth Study. Nutrition 2017, 33, 141–144. [Google Scholar] [CrossRef]
- Zeballos, E.; Todd, J.E. The effects of skipping a meal on daily energy intake and diet quality. Public Health Nutr. 2020, 23, 3346–3355. [Google Scholar] [CrossRef]
- Youn, H.-S. New nutritional concepts of vitamins and minerals. Clin. Exp. Pediatr. 2005, 48, 1295–1309. [Google Scholar]
- Ekmekcioglu, C.; Touitou, Y. Chronobiological aspects of food intake and metabolism and their relevance on energy balance and weight regulation. Obes. Rev. 2011, 12, 14–25. [Google Scholar] [CrossRef]
- Monnard, C.; Fleith, M. Total Fat and Fatty Acid Intake among 1–7-Year-Old Children from 33 Countries: Comparison with International Recommendations. Nutrients 2021, 13, 3547. [Google Scholar] [CrossRef]
- Bowman, S.A.; Vinyard, B.T. Fast food consumption of US adults: Impact on energy and nutrient intakes and overweight status. J. Am. Coll. Nutr. 2004, 23, 163–168. [Google Scholar] [CrossRef]
- Bryant, E.J.; King, N.; Blundell, J.E. Disinhibition: Its effects on appetite and weight regulation. Obes. Rev. 2008, 9, 409–419. [Google Scholar] [CrossRef] [PubMed]
- Polivy, J.; Herman, C.P.; Deo, R. Getting a bigger slice of the pie. Effects on eating and emotion in restrained and unrestrained eaters. Appetite 2010, 55, 426–430. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health and Welfare. A Study on the Prevention of Obesity among Children and Adolescents. Available online: https://scienceon.kisti.re.kr/srch/selectPORSrchReport.do?cn=TRKO201500019390 (accessed on 21 December 2022).


{kind=link}
| Variables | Total (n = 1736, N = 12,161,556) | SL Group (n = 1168, N = 7,685,180) | NSL Group (n = 493, N = 3,834,876) | SKL Group (n = 75, N = 641,501) | p-Value 3 |
|---|---|---|---|---|---|
| Age 1 | |||||
| 12.6 ± 0.1 | 11.8 ± 0.1 c | 13.8 ± 0.2 ab | 14.5 ± 0.5 a | <0.0001 | |
| Sex 2 | |||||
| Boys | 896 (51.6) | 599 (50.8) | 259 (52.5) | 38 (55.2) | 0.747 |
| Girls | 840 (48.4) | 569 (49.2) | 234 (47.5) | 37 (44.8) | |
| School level 2 | |||||
| Elementary | 1067 (50.3) | 798 (59.5) | 244 (36.1) | 25 (26.2) | <0.0001 |
| Middle | 361 (22.4) | 237 (22.4) | 102 (22.2) | 22 (23.5) | |
| High | 308 (27.2) | 133 (18.1) | 147 (41.7) | 28 (50.3) | |
| Residential area 2 | |||||
| Urban | 1482 (87.6) | 993 (87.2) | 424 (88.4) | 65 (88.4) | 0.882 |
| Rural | 254 (12.4) | 175 (12.8) | 69 (11.6) | 10 (11.6) | |
| Household income level 2 | |||||
| Low | 155 (9.5) | 116 (10.7) | 33 (7.2) | 6 (8.8) | 0.422 |
| Low-middle | 461 (26.3) | 308 (26.5) | 137 (26.8) | 16 (19.9) | |
| Middle-high | 590 (33.2) | 402 (32.7) | 158 (32.7) | 30 (41.8) | |
| High | 529 (31.1) | 342 (30.1) | 164 (33.3) | 23 (29.5) | |
| Physical activity | |||||
| ≥60 min of physical activity 2 | |||||
| <5 day/week | 750 (93.3) | 440 (94.8) | 260 (91.6) | 50 (90.8) | 0.262 |
| ≥5 day/week | 58 (6.7) | 30 (5.2) | 24 (8.4) | 4 (9.2) | |
| Muscular exercise 2 | |||||
| <3 day/week | 678 (82.4) | 402 (84.2) | 231 (79.6) | 45 (83.3) | 0.351 |
| ≥3 day/week | 130 (17.6) | 68 (15.8) | 53 (20.4) | 9 (16.7) | |
| Variables | Total (n = 1736, N = 12,161,556) | SL Group (n = 1168, N = 7,685,180) | NSL Group (n = 493, N = 3,834,876) | SKL Group (n = 75, N = 641,501) | p-Value |
|---|---|---|---|---|---|
| Height (cm) 1 | 153.8 ± 0.5 | 151.1 ± 0.6 b | 157.7 ± 0.9 a | 162.4 ± 2.1 ab | 0.012 |
| Weight (kg) | 49.3 ± 0.6 | 46.8 ± 0.6 | 52.8 ± 1.0 | 59.7 ± 2.7 | 0.041 |
| BMI (kg/m2) 1 | 20.2 ± 0.1 | 19.8 ± 0.2 | 20.6 ± 0.3 | 22.1 ± 0.7 | 0.113 |
| Underweight 2,3 | 154 (8.6) | 98 (8.5) | 50 (9.3) | 6 (6.9) | 0.021 |
| Normal weight | 1184 (68.5) | 800 (69.2) | 340 (69.1) | 44 (56.9) | |
| Overweight | 156 (8.4) | 109 (8.7) | 41 (8.2) | 6 (5.8) | |
| Obesity | 242 (14.5) | 161 (13.7) | 62 (13.5) | 19 (30.4) | |
| WC (cm) 1 | 68.0 ± 0.4 | 66.6 ± 0.4 | 69.8 ± 0.7 | 73.7 ± 1.9 | 0.264 |
| Normal 2,4 | 1526 (87.4) | 1031 (88.7) | 437 (87.3) | 58 (72.8) | 0.004 |
| Central obesity | 210 (12.6) | 137 (11.3) | 56 (12.7) | 17 (27.2) |
| Variables | SL Group (n = 1168, N = 7,685,180) | NSL Group (n = 493, N = 3,834,876) | SKL Group (n = 75, N = 641,501) | p-Value 2 |
|---|---|---|---|---|
| Energy (kcal/day) | 2015.0 ± 28.1 a,1 | 1943.6 ± 44.2 b,c | 1726.7 ± 113.5 c | 0.0001 |
| Carbohydrate (g/day) | 301.1 ± 4.3 | 287.8 ± 6.3 | 250.1 ± 16.4 | 0.384 |
| Fat (g/day) | 54.9 ± 1.1 | 54.5 ± 1.8 | 52.7 ± 5.6 | 0.022 |
| Protein (g/day) | 74.4 ± 1.2 a | 69.2 ± 1.9 b | 60.1 ± 4.2 a,b | 0.0003 |
| C:F:p (%) | 60.3:24.0:14.7 | 59.8:24.8:14.3 | 60.0:24.9:14.5 | |
| Fiber (g/day) | 19.1 ± 0.4 | 19.2 ± 0.5 | 16.6 ± 1.5 | 0.442 |
| Calcium (mg/day) | 560.3 ± 10.7 | 488.2 ± 17.5 | 476.6 ± 44.9 | 0.095 |
| Phosphorus (mg/day) | 1088.0 ± 16.5 a | 995.1 ± 24.1 b | 890.6 ± 64.0 a,b | 0.002 |
| Iron (mg/day) | 10.9 ± 0.2 | 10.3 ± 0.3 | 8.7 ± 0.6 | 0.037 |
| Sodium (mg/day) | 2940.8 ± 58.4 | 2887.4 ± 86.6 | 2448.7 ± 191.2 | 0.065 |
| Potassium (mg/day) | 2410.1 ± 38.7 a | 2165.9 ± 51.4 b | 1945.4 ± 133.7 a,b | 0.0002 |
| Vitamin A(μgRE/day) | 407.2 ± 12.7 a | 326.1 ± 14.3 b | 286.8 ± 27.9 a,b | 0.002 |
| Carotene (μg/day) | 1986.0 ± 59.4 a | 1653.2 ± 83.6 b,c | 1383.9 ± 172.5c | 0.002 |
| Retinol (μg/day) | 241.2 ± 11.5 | 187.8 ± 13.7 | 170.4 ± 20.9 | 0.102 |
| Vitamin B1 (mg/day) | 1.4 ± 0.0 a | 1.3 ± 0.0 b,c | 1.0 ± 0.1 c | <0.0001 |
| Vitamin B2 (mg/day) | 1.7 ± 0.0 | 1.6 ± 0.1 | 1.5 ± 0.1 | 0.951 |
| Vitamin C (mg/day) | 61.4 ± 2.4 | 61.0 ± 4.0 | 52.6 ± 8.0 | 0.384 |
| Niacin (mg/day) | 12.5 ± 0.2 a | 11.8 ± 0.3 a,b | 9.7 ± 0.8 b | 0.029 |
| Cholesterol (mg/day) | 276.3 ± 6.5 | 277.2 ± 17.3 | 243.3 ± 30.1 | 0.822 |
| SFA (g/day) | 19.5 ± 0.4 b | 19.3 ± 0.7 a,b | 19.8 ± 2.2 a | 0.007 |
| MUFA (g/day) | 17.6 ± 0.4 | 18.0 ± 0.7 | 17.6 ± 2.1 | 0.017 |
| PUFA (g/day) | 12.6 ± 0.3 | 12.0 ± 0.4 | 10.6 ± 1.2 | 0.946 |
| w-3 FA (mg/day) | 1.6 ± 0.1 | 1.4 ± 0.1 | 1.2 ± 0.2 | 0.558 |
| w-6 FA (mg/day) | 11.0 ± 0.3 | 10.5 ± 0.4 | 9.3 ± 1.0 | 0.951 |
| Sugar (g/day) | 65.7 ± 1.4 | 66.8 ± 2.4 | 61.6 ± 5.1 | 0.016 |
| Variables | Model 1 1 | Model 2 2 | Model 3 3 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value 4 | OR | 95% CI | p-Value | OR | 95% CI | p-Value | ||
| Obesity | SL group | 1.000 (ref) | 1.000 (ref) | 1.000 (ref) | ||||||
| NSL group | 0.982 | (0.696–1.385) | 0.916 | 0.916 | (0.642–1.307) | 0.627 | 0.926 | (0.650–1.319) | 0.670 | |
| SKL group | 2.759 | (1.450–5.249) | 0.002 | 2.511 | (1.307–4.822) | 0.006 | 2.479 | (1.282–4.791) | 0.007 | |
| Overweight and obesity | SL group | 1.000 (ref) | 1.000 (ref) | 1.000 (ref) | ||||||
| NSL group | 0.958 | (0.707–1.298) | 0.781 | 0.921 | (0.680–1.247) | 0.593 | 0.944 | (0.699–1.273) | 0.704 | |
| SKL group | 1.967 | (1.087–3.559) | 0.025 | 1.861 | (1.027–3.372) | 0.041 | 1.861 | (1.011–3.426) | 0.046 | |
| Central obesity | SL group | 1.000 (ref) | 1.000 (ref) | 1.000 (ref) | ||||||
| NSL group | 1.148 | (0.762–1.730) | 0.508 | 1.019 | (0.678–1.532) | 0.929 | 1.028 | (0.685–1.542) | 0.893 | |
| SKL group | 2.944 | (1.497–5.788) | 0.002 | 2.513 | (1.283–4.920) | 0.007 | 2.456 | (1.251–4.824) | 0.009 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, Y.; Son, K.; Kim, J.; Lee, M.; Park, K.-H.; Lim, H. Associations between School Lunch and Obesity in Korean Children and Adolescents Based on the Korea National Health and Nutrition Examination Survey 2017–2019 Data: A Cross-Sectional Study. Nutrients 2023, 15, 698. https://doi.org/10.3390/nu15030698
Kim Y, Son K, Kim J, Lee M, Park K-H, Lim H. Associations between School Lunch and Obesity in Korean Children and Adolescents Based on the Korea National Health and Nutrition Examination Survey 2017–2019 Data: A Cross-Sectional Study. Nutrients. 2023; 15(3):698. https://doi.org/10.3390/nu15030698
Chicago/Turabian StyleKim, Yeji, Kumhee Son, Jieun Kim, Miji Lee, Kyung-Hee Park, and Hyunjung Lim. 2023. "Associations between School Lunch and Obesity in Korean Children and Adolescents Based on the Korea National Health and Nutrition Examination Survey 2017–2019 Data: A Cross-Sectional Study" Nutrients 15, no. 3: 698. https://doi.org/10.3390/nu15030698
APA StyleKim, Y., Son, K., Kim, J., Lee, M., Park, K.-H., & Lim, H. (2023). Associations between School Lunch and Obesity in Korean Children and Adolescents Based on the Korea National Health and Nutrition Examination Survey 2017–2019 Data: A Cross-Sectional Study. Nutrients, 15(3), 698. https://doi.org/10.3390/nu15030698