
Carrot Intake and Risk of Developing Cancer: A Prospective Cohort Study


Abstract
1. Introduction
2. Materials and Methods
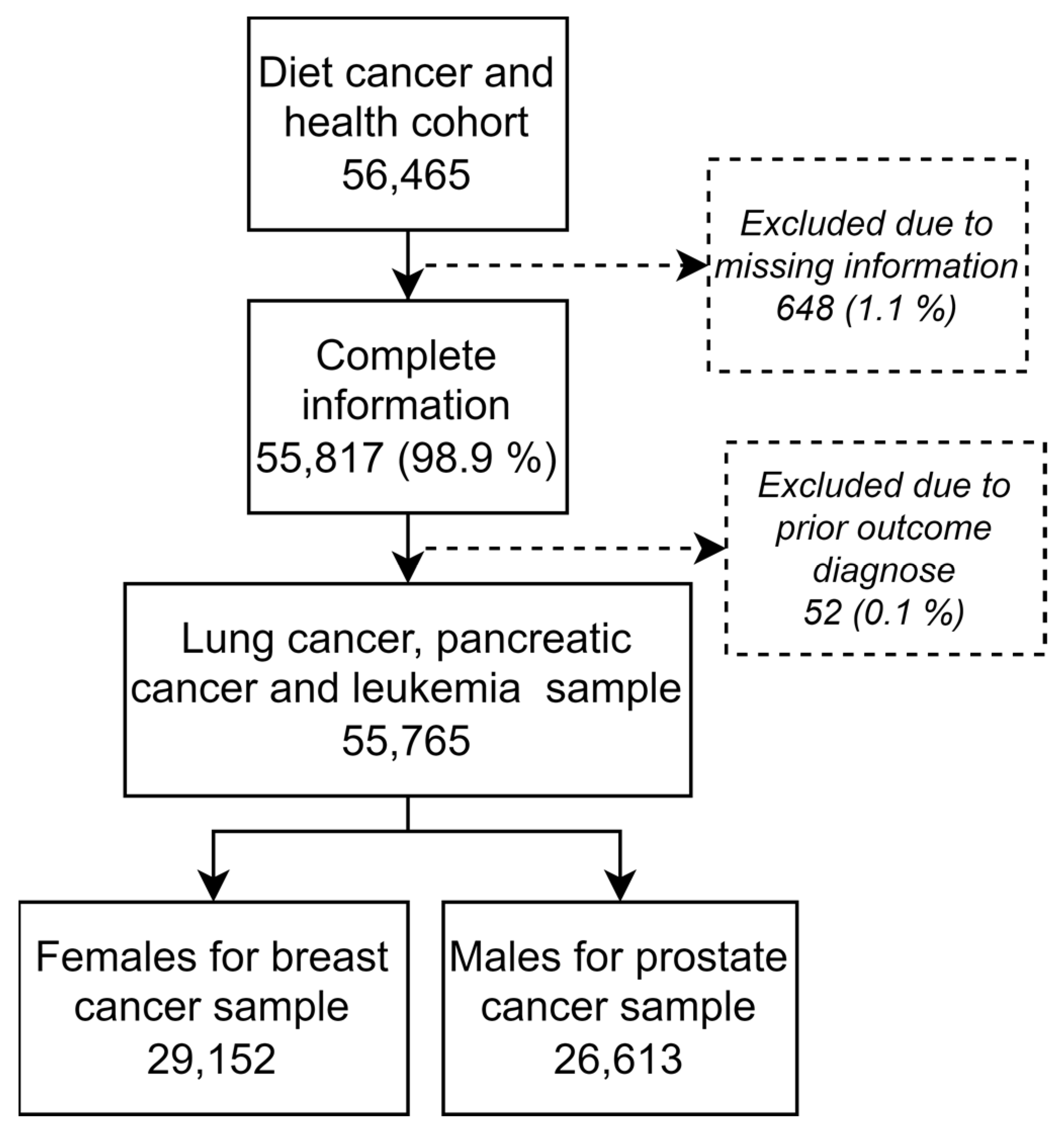
2.1. Population
2.2. Register Data
2.3. Exposure
2.4. Outcomes
2.5. Statistical Analysis
2.6. Covariates
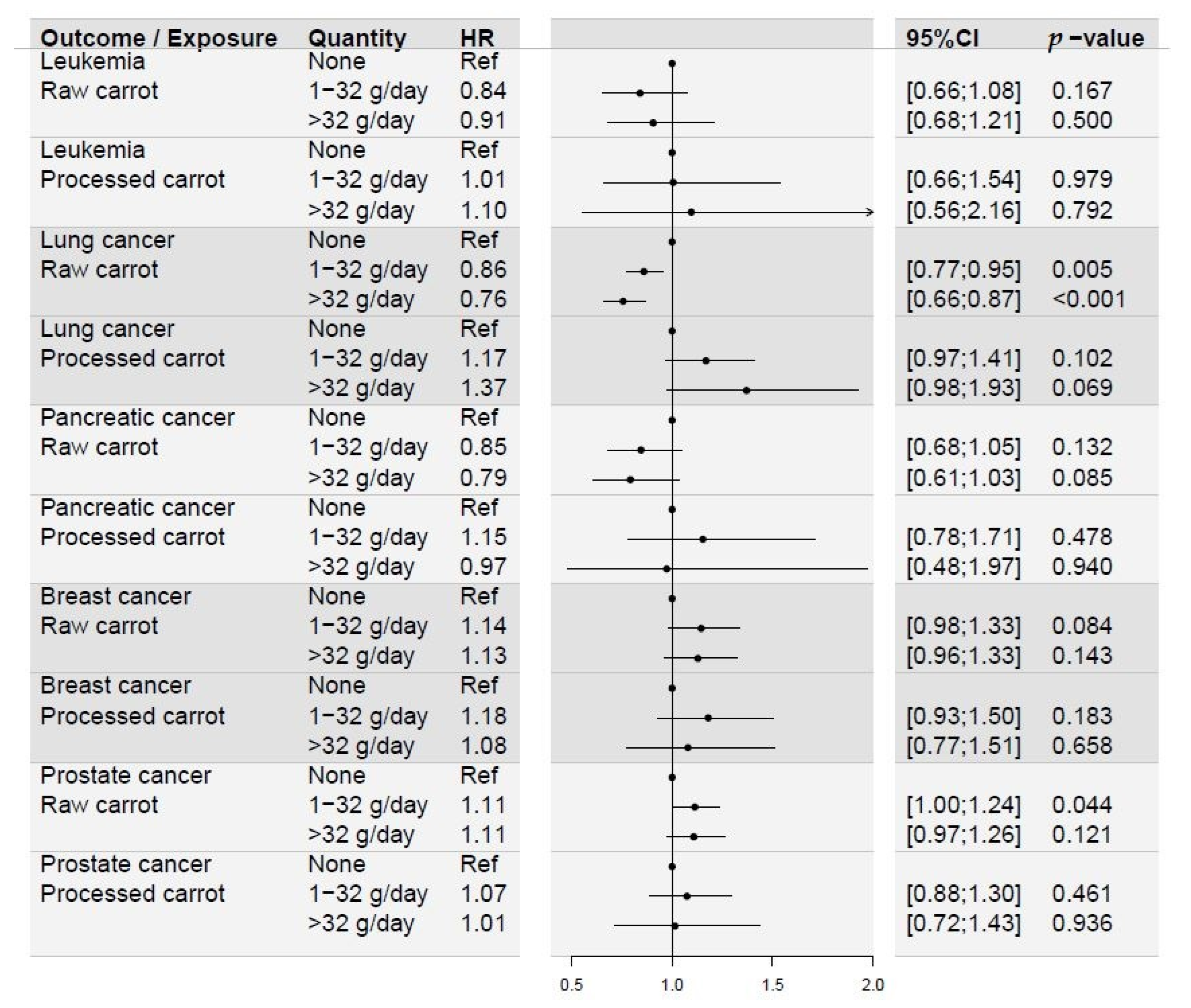
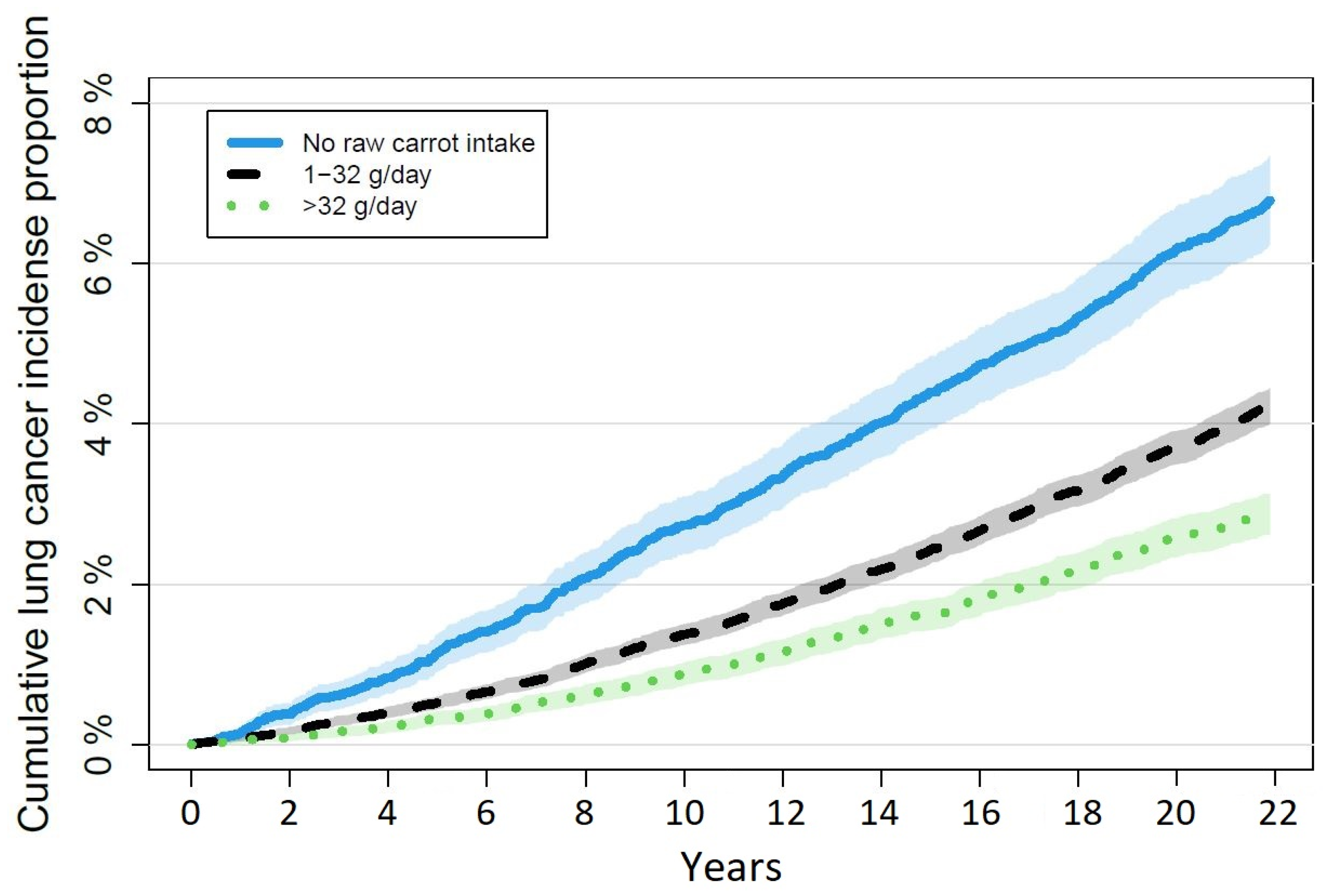
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Vainio, H.; Weiderpass, E. Fruit and vegetables in cancer prevention. Nutr. Cancer 2006, 54, 111–142. [Google Scholar] [CrossRef] [PubMed]
- Block, G.; Patterson, B.; Subar, A. Fruit, vegetables, and cancer prevention: A review of the epidemiological evidence. Nutr. Cancer 1992, 18, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Steinmetz, K.A.; Potter, J.D. Vegetables, fruit, and cancer prevention: A review. J. Am. Diet. Assoc. 1996, 96, 1027–1039. [Google Scholar] [CrossRef]
- Deding, U.; Baatrup, G.; Christensen, L.P.; Kobaek-Larsen, M. Carrot Intake and Risk of Colorectal Cancer: A Prospective Cohort Study of 57,053 Danes. Nutrients 2020, 12, 332. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Z.; Chen, H.; Li, M.; Wang, W.; Fan, C.; Long, F. Association of Dietary Carrot/Carotene Intakes with Colorectal Cancer Incidence and Mortality in the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial. Front. Nutr. 2022, 9, 888898. [Google Scholar] [CrossRef]
- O’Neill, M.E.; Carroll, Y.; Corridan, B.; Olmedilla, B.; Granado, F.; Blanco, I.; Van der Berg, H.; Hininger, I.; Rousell, A.-M.; Chopra, M.; et al. A European carotenoid database to assess carotenoid intakes and its use in a five-country comparative study. Br. J. Nutr. 2001, 85, 499–507. [Google Scholar] [CrossRef]
- The Alpha-Tocopherol Beta Carotene Cancer Prevention Study Group. The effect of vitamin E and beta carotene on the incidence of lung cancer and other cancers in male smokers. N. Engl. J. Med. 1994, 330, 1029–1035. [Google Scholar] [CrossRef]
- Astorg, P. Food carotenoids and cancer prevention: An overview of current research. Trends Food Sci. Technol. 1997, 8, 406–413. [Google Scholar] [CrossRef]
- Omenn, G.S.; Goodman, G.E.; Thornquist, M.D.; Balmes, J.; Cullen, M.R.; Glass, A.; Keogh, J.P.; Meyskens, F.L., Jr.; Valanis, B.; Williams, J.H., Jr.; et al. Effects of a combination of beta carotene and vitamin A on lung cancer and cardiovascular disease. N. Engl. J. Med. 1996, 334, 1150–1155. [Google Scholar] [CrossRef]
- Greenberg, E.R.; Baron, J.A.; Karagas, M.R.; Stukel, T.A.; Nierenberg, D.W.; Stevens, M.M.; Mandel, J.S.; Haile, R.W. Mortality associated with low plasma concentration of beta carotene and the effect of oral supplementation. JAMA 1996, 275, 699–703. [Google Scholar] [CrossRef]
- Albanes, D.; Heinonen, O.P.; Taylor, P.R.; Virtamo, J.; Edwards, B.K.; Rautalahti, M.; Hartman, A.M.; Palmgren, J.; Freedman, L.S.; Haapakoski, J.; et al. Alpha-Tocopherol and beta-carotene supplements and lung cancer incidence in the alpha-tocopherol, beta-carotene cancer prevention study: Effects of base-line characteristics and study compliance. J. Natl. Cancer Inst. 1996, 88, 1560–1570. [Google Scholar] [CrossRef] [PubMed]
- Middha, P.; Weinstein, S.J.; Männistö, S.; Albanes, D.; Mondul, A.M. β-Carotene Supplementation and Lung Cancer Incidence in the Alpha-Tocopherol, Beta-Carotene Cancer Prevention Study: The Role of Tar and Nicotine. Nicotine Tob. Res. 2018, 21, 1045–1050. [Google Scholar] [CrossRef] [PubMed]
- Kordiak, J.; Bielec, F.; Jabłoński, S.; Pastuszak-Lewandoska, D. Role of Beta-Carotene in Lung Cancer Primary Chemoprevention: A Systematic Review with Meta-Analysis and Meta-Regression. Nutrients 2022, 14, 1361. [Google Scholar] [CrossRef] [PubMed]
- Christensen, L.P. Bioactive C(17) and C(18) Acetylenic Oxylipins from Terrestrial Plants as Potential Lead Compounds for Anticancer Drug Development. Molecules 2020, 25, 2568. [Google Scholar] [CrossRef]
- Matsunaga, H.; Katano, M.; Yamamoto, H.; Fujito, H.; Mori, M.; Takata, K. Cytotoxic activity of polyacetylene compounds in Panax ginseng C. A. Meyer. Chem. Pharm. Bull. 1990, 38, 3480–3482. [Google Scholar] [CrossRef]
- Bernart, M.W.; Cardellina, J.H., II; Balaschak, M.S.; Alexander, M.R.; Shoemaker, R.H.; Boyd, M.R. Cytotoxic falcarinol oxylipins from Dendropanax arboreus. J. Nat. Prod. 1996, 59, 748–753. [Google Scholar] [CrossRef]
- Kuo, Y.C.; Lin, Y.L.; Huang, C.P.; Shu, J.W.; Tsai, W.J. A tumor cell growth inhibitor from Saposhnikovae divaricata. Cancer Investig. 2002, 20, 955–964. [Google Scholar] [CrossRef]
- Young, J.F.; Duthie, S.J.; Milne, L.; Christensen, L.P.; Duthie, G.G.; Bestwick, C.S. Biphasic effect of falcarinol on caco-2 cell proliferation, DNA damage, and apoptosis. J. Agric. Food Chem. 2007, 55, 618–623. [Google Scholar] [CrossRef]
- Purup, S.; Larsen, E.; Christensen, L.P. Differential effects of falcarinol and related aliphatic C(17)-polyacetylenes on intestinal cell proliferation. J. Agric. Food Chem. 2009, 57, 8290–8296. [Google Scholar] [CrossRef]
- Kobaek-Larsen, M.; El-Houri, R.B.; Christensen, L.P.; Al-Najami, I.; Fretté, X.; Baatrup, G. Dietary polyacetylenes, falcarinol and falcarindiol, isolated from carrots prevents the formation of neoplastic lesions in the colon of azoxymethane-induced rats. Food Funct. 2017, 8, 964–974. [Google Scholar] [CrossRef]
- Kobaek-Larsen, M.; Baatrup, G.; Notabi, M.K.; El-Houri, R.B.; Pipó-Ollé, E.; Christensen Arnspang, E.; Christensen, L.P. Dietary Polyacetylenic Oxylipins Falcarinol and Falcarindiol Prevent Inflammation and Colorectal Neoplastic Transformation: A Mechanistic and Dose-Response Study in A Rat Model. Nutrients 2019, 11, 2223. [Google Scholar] [CrossRef] [PubMed]
- Kobaek-Larsen, M.; Christensen, L.P.; Vach, W.; Ritskes-Hoitinga, J.; Brandt, K. Inhibitory effects of feeding with carrots or (−)-falcarinol on development of azoxymethane-induced preneoplastic lesions in the rat colon. J. Agric. Food Chem. 2005, 53, 1823–1827. [Google Scholar] [CrossRef] [PubMed]
- Metzger, B.T.; Barnes, D.M.; Reed, J.D. Purple carrot (Daucus carota L.) polyacetylenes decrease lipopolysaccharide-induced expression of inflammatory proteins in macrophage and endothelial cells. J. Agric. Food Chem. 2008, 56, 3554–3560. [Google Scholar] [CrossRef]
- Alanko, J.; Kurahashi, Y.; Yoshimoto, T.; Yamamoto, S.; Baba, K. Panaxynol, a polyacetylene compound isolated from oriental medicines, inhibits mammalian lipoxygenases. Biochem. Pharmacol. 1994, 48, 1979–1981. [Google Scholar] [CrossRef]
- Tjønneland, A.; Olsen, A.; Boll, K.; Stripp, C.; Christensen, J.; Engholm, G.; Overvad, K. Study design, exposure variables, and socioeconomic determinants of participation in Diet, Cancer and Health: A population-based prospective cohort study of 57,053 men and women in Denmark. Scand. J. Public Health 2007, 35, 432–441. [Google Scholar] [CrossRef] [PubMed]
- Overvad, K.I.M.; JØNneland, A.T.; HaraldsdÓTtir, J.; Ewertz, M.; Jensen, O.M. Development of a Semiquantitative Food Frequency Questionnaire to Assess Food, Energy and Nutrient Intake in Denmark. Int. J. Epidemiol. 1991, 20, 900–905. [Google Scholar] [CrossRef] [PubMed]
- Tjønneland, A.; Overvad, K.I.M.; Haraldsdottir, J.; Bang, S.; Ewertz, M.; Jensen, O.M. Validation of a Semiquantitative Food Frequency Questionnaire Developed in Denmark. Int. J. Epidemiol. 1991, 20, 906–912. [Google Scholar] [CrossRef]
- Lynge, E.; Sandegaard, J.L.; Rebolj, M. The Danish National Patient Register. Scand. J. Public Health 2011, 39, 30–33. [Google Scholar] [CrossRef]
- Helweg-Larsen, K. The Danish Register of Causes of Death. Scand. J. Public Health 2011, 39, 26–29. [Google Scholar] [CrossRef]
- Rawson, A.; Brunton, N.P.; Rai, D.K.; McLoughlin, P.; Tiwari, B.K.; Tuohy, M.G. Stability of falcarinol type polyacetylenes during processing of Apiaceae vegetables. Trends Food Sci. Technol. 2013, 30, 133–141. [Google Scholar] [CrossRef]
- Hansen, S.L.; Purup, S.; Christensen, L.P. Bioactivity of falcarinol and the influenceof processing and storage on its content in carrots (Daucus carota L). J. Sci. Food Agric. 2003, 83, 1010–1017. [Google Scholar] [CrossRef]
- Team, R.C. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2019. [Google Scholar]
- Gerds, T.A.; Ozenne, B. Publish: Format Output of Various Routines in a Suitable Way for Reports and Publication. R Package Version. 2019. Available online: https://cran.r-project.org/web/packages/Publish/index.html (accessed on 15 November 2022).
- Therneau, T. _A Package for Survival Analysis in S_. Version 2.38. 2019. Available online: https://cranr-project.org/package=survival (accessed on 15 November 2022).
- Tawil, M.; Bekdash, A.; Mroueh, M.; Daher, C.F.; Abi-Habib, R.J. Wild carrot oil extract is selectively cytotoxic to human acute myeloid leukemia cells. Asian Pac. J. Cancer Prev. APJCP 2015, 16, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Shao, F.; Zhang, F.; Miao, Q. Association between dietary carrot intake and breast cancer: A meta-analysis. Medicine 2018, 97, e12164. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Disease | ICD-8 | ICD-10 |
|---|---|---|
| Breast cancer | 174.00; 174.01; 174.02; 174.08; 174.09 | C50 |
| Lung cancer | 162.09-19 | C33; C34; C45 |
| Prostate cancer | 185.99 | C61 |
| Pancreatic cancer | 157.09; 157.80; 157.81; 157.89; 157.99 | C25 |
| Leukemia | 204.09–207.99 | C91–C95 |
| No Leukemia, n = 55,223 (%) | Leukemia During Follow-Up, n = 542 (%) | Total, n = 55,765 | p-Value | ||
| Raw carrot intake | None | 7800 (98.8) | 93 (1.2) | 7893 | |
| 1–32 g/day | 31,199 (99.1) | 294 (0.9) | 31,493 | ||
| >32 g/day | 16,224 (99.1) | 155 (0.9) | 16,379 | 0.130 | |
| Processed carrot intake | None | 2240 (98.9) | 24 (1.1) | 2264 | |
| 1–32 g/day | 51,699 (99.0) | 503 (1.0) | 52,202 | ||
| >32 g/day | 1284 (98.8) | 15 (1.2) | 1299 | 0.715 | |
| No Lung Cancer, n = 53,314 (%) | Lung Cancer During Follow-Up, n = 2451 (%) | Total, n = 55,765 | p-Value | ||
| Raw carrot intake | None | 7336 (92.9) | 557 (7.1) | 7893 | |
| 1–32 g/day | 30,097 (95.6) | 1396 (4.4) | 31,493 | ||
| >32 g/day | 15,881 (97.0) | 498 (3.0) | 16,379 | <0.001 | |
| Processed carrot intake | None | 2138 (94.4) | 126 (5.6) | 2264 | |
| 1–32 g/day | 49,930 (95.6) | 2272 (4.4) | 52,202 | ||
| >32 g/day | 1246 (95.9) | 53 (4.1) | 1299 | 0.019 | |
| No Pancreatic Cancer, n = 55,110 (%) | Pancreatic Cancer During Follow-Up, n = 655 (%) | Total, n = 55,765 | p-Value | ||
| Raw carrot intake | None | 7773 (98.5) | 120 (1.5) | 7893 | |
| 1–32 g/day | 31,123 (98.8) | 370 (1.2) | 31,493 | ||
| >32 g/day | 16,214 (99.0) | 165 (1.0) | 16,379 | 0.002 | |
| Processed carrot intake | None | 2236 (98.8) | 28 (1.2) | 2264 | |
| 1–32 g/day | 51,587 (98.8) | 615 (1.2) | 52,202 | ||
| >32 g/day | 1287 (99.1) | 12 (0.9) | 1299 | 0.675 | |
| No Breast Cancer, n = 26,433 (%) | Breast Cancer During Follow-Up, n = 2719 (%) | Total, n = 29,152 | p-Value | ||
| Raw carrot intake | None | 2324 (92.1) | 198 (7.9) | 2522 | |
| 1–32 g/day | 13,825 (90.4) | 1472 (9.6) | 15,297 | ||
| >32 g/day | 10,284 (90.7) | 1049 (9.3) | 11,333 | 0.017 | |
| Processed carrot intake | None | 846 (92.4) | 70 (7.6) | 916 | |
| 1–32 g/day | 24,826 (90.6) | 2572 (9.4) | 27,398 | ||
| >32 g/day | 761 (90.8) | 77 (9.2) | 838 | 0.201 | |
| No Prostate Cancer, n = 23,792 (%) | Prostate Cancer During Follow-Up, 2821 (%) | Total, n = 26,613 | p-Value | ||
| Raw carrot intake | None | 4869 (90.7) | 502 (9.3) | 5371 | |
| 1–32 g/day | 14,433 (89.1) | 1763 (10.9) | 16,196 | ||
| >32 g/day | 4490 (89.0) | 556 (11.0) | 5046 | 0.004 | |
| Processed carrot intake | None | 1228 (91.1) | 120 (8.9) | 1348 | |
| 1–32 g/day | 22,152 (89.3) | 2652 (10.7) | 24,804 | ||
| >32 g/day | 412 (89.4) | 49 (10.6) | 461 | 0.115 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Deding, U.; Baatrup, G.; Kaalby, L.; Kobaek-Larsen, M. Carrot Intake and Risk of Developing Cancer: A Prospective Cohort Study. Nutrients 2023, 15, 678. https://doi.org/10.3390/nu15030678
Deding U, Baatrup G, Kaalby L, Kobaek-Larsen M. Carrot Intake and Risk of Developing Cancer: A Prospective Cohort Study. Nutrients. 2023; 15(3):678. https://doi.org/10.3390/nu15030678
Chicago/Turabian StyleDeding, Ulrik, Gunnar Baatrup, Lasse Kaalby, and Morten Kobaek-Larsen. 2023. "Carrot Intake and Risk of Developing Cancer: A Prospective Cohort Study" Nutrients 15, no. 3: 678. https://doi.org/10.3390/nu15030678
APA StyleDeding, U., Baatrup, G., Kaalby, L., & Kobaek-Larsen, M. (2023). Carrot Intake and Risk of Developing Cancer: A Prospective Cohort Study. Nutrients, 15(3), 678. https://doi.org/10.3390/nu15030678