
Association between Coffee Consumption and Brain MRI Parameters in the Hamburg City Health Study

 , , , , and
, , , , and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Clinical Data Assessment
2.3. MRI Acquisition and Processing
2.4. Statistical Analyses
3. Results
3.1. Study Sample Characteristics
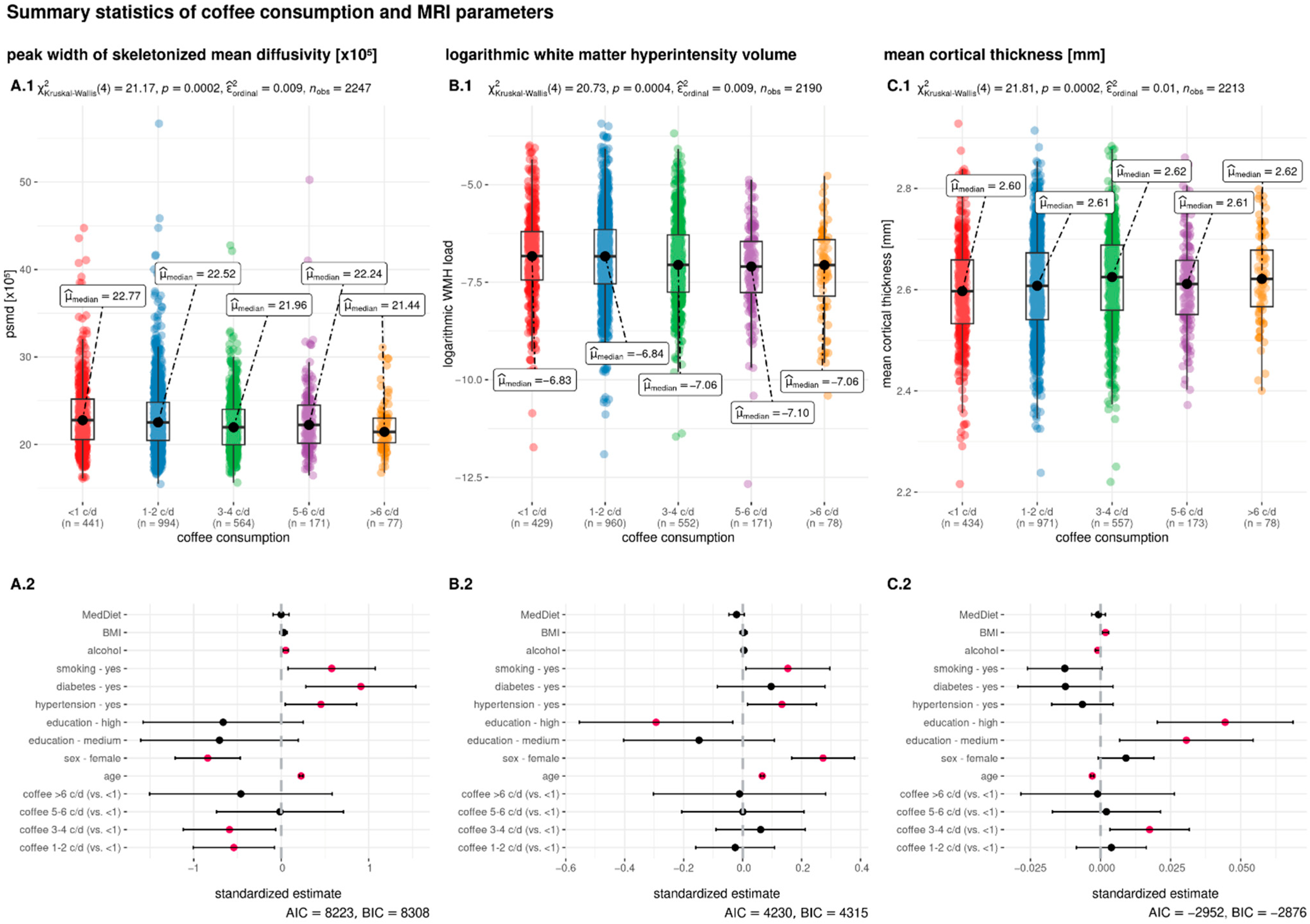
3.2. Association of Coffee Consumption with MRI Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Poole, R.; Kennedy, O.J.; Roderick, P.; Fallowfield, J.A.; Hayes, P.C.; Parkes, J. Coffee consumption and health: Umbrella review of meta-analyses of multiple health outcomes. BMJ 2017, 359, j5024. [Google Scholar] [CrossRef] [PubMed]
- Fredholm, B.B.; Bättig, K.; Holmén, J.; Nehlig, A.; Zvartau, E.E. Actions of caffeine in the brain with special reference to factors that contribute to its widespread use. Pharmacol. Rev. 1999, 51, 83–133. [Google Scholar] [PubMed]
- Eskelinen, M.H.; Ngandu, T.; Tuomilehto, J.; Soininen, H.; Kivipelto, M. Midlife Coffee and Tea Drinking and the Risk of Late-Life Dementia: A Population-Based CAIDE Study. J. Alzheimer’s Dis. 2009, 16, 85–91. [Google Scholar] [CrossRef] [PubMed]
- Driscoll, I.; Shumaker, S.A.; Snively, B.M.; Margolis, K.L.; Manson, J.E.; Vitolins, M.Z.; Rossom, R.C.; Espeland, M.A. Relationships Between Caffeine Intake and Risk for Probable Dementia or Global Cognitive Impairment: The Women’s Health Initiative Memory Study. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2016, 71, 1596–1602. [Google Scholar] [CrossRef] [PubMed]
- Larsson, S.C.; Virtamo, J.; Wolk, A. Coffee Consumption and Risk of Stroke in Women. Stroke 2011, 42, 908–912. [Google Scholar] [CrossRef]
- Lee, J.; Lee, J.-E.; Kim, Y. Relationship between coffee consumption and stroke risk in Korean population: The Health Examinees (HEXA) Study. Nutr. J. 2017, 16, 7. [Google Scholar] [CrossRef]
- Araújo, L.F.; Mirza, S.S.; Bos, D.; Niessen, W.J.; Barreto, S.M.; van der Lugt, A.; Vernooij, M.W.; Hofman, A.; Tiemeier, H.; Ikram, M.A. Association of Coffee Consumption with MRI Markers and Cognitive Function: A Population-Based Study. J. Alzheimer’s Dis. 2016, 53, 451–461. [Google Scholar] [CrossRef]
- Qi, H.; Li, S. Dose-response meta-analysis on coffee, tea and caffeine consumption with risk of Parkinson’s disease. Geriatr. Gerontol. Int. 2013, 14, 430–439. [Google Scholar] [CrossRef]
- Osama, H.; Abdelrahman, M.A.; Madney, Y.M.; Harb, H.S.; Saeed, H.; Abdelrahim, M.E.A. Coffee and type 2 diabetes risk: Is the association mediated by adiponectin, leptin, c-reactive protein or Interleukin-6? A systematic review and meta-analysis. Int. J. Clin. Pract. 2021, 75, e13983. [Google Scholar] [CrossRef]
- Dall’Lgna, O.P.; Porciúncula, L.O.; Souza, D.O.; Cunha, R.A.; Lara, D.R. Neuroprotection by caffeine and adenosine A2A receptor blockade of β -amyloid neurotoxicity. Br. J. Pharmacol. 2003, 138, 1207–1209. [Google Scholar] [CrossRef]
- Shang, F.; Li, X.; Jiang, X. Coffee consumption and risk of the metabolic syndrome: A meta-analysis. Diabetes Metab. 2015, 42, 80–87. [Google Scholar] [CrossRef]
- Ding, M.; Bhupathiraju, S.N.; Chen, M.; van Dam, R.M.; Hu, F.B. Caffeinated and Decaffeinated Coffee Consumption and Risk of Type 2 Diabetes: A Systematic Review and a Dose-Response Meta-analysis. Diabetes Care 2014, 37, 569–586. [Google Scholar] [CrossRef]
- Debette, S.; Markus, H.S. The clinical importance of white matter hyperintensities on brain magnetic resonance imaging: Systematic review and meta-analysis. BMJ 2010, 341, c3666. [Google Scholar] [CrossRef]
- Georgakis, M.K.; Duering, M.; Wardlaw, J.M.; Dichgans, M. WMH and long-term outcomes in ischemic stroke: A Systematic Review and Meta-Analysis. Neurology 2019, 92, e1298–e1308. [Google Scholar] [CrossRef]
- Wardlaw, J.M.; Smith, E.E.; Biessels, G.J.; Cordonnier, C.; Fazekas, F.; Frayne, R.; Lindley, R.I.; O’Brien, J.T.; Barkhof, F.; Benavente, O.R.; et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. Lancet Neurol. 2013, 12, 822–838. [Google Scholar] [CrossRef]
- Dufouil, C.; de Kersaint–Gilly, A.; Besançon, V.; Levy, C.; Auffray, E.; Brunnereau, L.; Alpérovitch, A.; Tzourio, C. Longitudinal study of blood pressure and white matter hyperintensities: The EVA MRI Cohort. Neurology 2001, 56, 921–926. [Google Scholar] [CrossRef]
- Power, M.C.; Deal, J.A.; Sharrett, A.R.; Jack, C.R.; Knopman, D.; Mosley, T.H.; Gottesman, R.F. Smoking and white matter hyperintensity progression: The ARIC-MRI Study. Neurology 2015, 84, 841–848. [Google Scholar] [CrossRef]
- Frey, B.M.; Petersen, M.; Mayer, C.; Schulz, M.; Cheng, B.; Thomalla, G.; Frey, B.M.; Petersen, M.; Mayer, C.; Schulz, M.; et al. Characterization of White Matter Hyperintensities in Large-Scale MRI-Studies. Front. Neurol. 2019, 10, 238. [Google Scholar] [CrossRef]
- Ritchie, K.; Artero, S.; Portet, F.; Brickman, A.; Muraskin, J.; Beanino, E.; Ancelin, M.-L.; Carrière, I. Caffeine, Cognitive Functioning, and White Matter Lesions in the Elderly: Establishing Causality from Epidemiological Evidence. J. Alzheimer’s Dis. 2010, 20, S161–S166. [Google Scholar] [CrossRef]
- Park, J.; Han, J.W.; Lee, J.R.; Byun, S.; Suh, S.W.; Kim, J.H.; Kim, K.W. Association between lifetime coffee consumption and late life cerebral white matter hyperintensities in cognitively normal elderly individuals. Sci. Rep. 2020, 10, 421. [Google Scholar] [CrossRef]
- Pham, K.; Mulugeta, A.; Zhou, A.; O’Brien, J.T.; Llewellyn, D.J.; Hyppönen, E. High coffee consumption, brain volume and risk of dementia and stroke. Nutr. Neurosci. 2021, 25, 2111–2122. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Byun, M.S.; Yi, D.; Lee, J.-Y.; Jeon, S.Y.; Jung, G.; Lee, H.N.; Sohn, B.K.; Lee, J.Y.; KBASE Research Group; et al. Coffee intake and decreased amyloid pathology in human brain. Transl. Psychiatry 2019, 9, 27. [Google Scholar] [CrossRef] [PubMed]
- Baykara, E.; Gesierich, B.; Adam, R.; Tuladhar, A.M.; Biesbroek, J.M.; Koek, H.L.; Ropele, S.; Jouvent, E.; Alzheimer’s Disease Neuroimaging Initiative; Chabriat, H.; et al. A Novel Imaging Marker for Small Vessel Disease Based on Skeletonization of White Matter Tracts and Diffusion Histograms: Novel SVD Imaging Marker. Ann. Neurol. 2016, 80, 581–592. [Google Scholar] [CrossRef]
- Haller, S.; Montandon, M.-L.; Rodriguez, C.; Herrmann, F.R.; Giannakopoulos, P. Impact of Coffee, Wine, and Chocolate Consumption on Cognitive Outcome and MRI Parameters in Old Age. Nutrients 2018, 10, 1391. [Google Scholar] [CrossRef] [PubMed]
- West, R.K.; Ravona-Springer, R.; Livny, A.; Heymann, A.; Shahar, D.; Leroith, D.; Preiss, R.; Zukran, R.; Silverman, J.M.; Schnaider-Beeri, M. Age Modulates the Association of Caffeine Intake with Cognition and with Gray Matter in Elderly Diabetics. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2019, 74, 683–688. [Google Scholar] [CrossRef]
- Perlaki, G.; Orsi, G.; Kovács, N.; Schwarcz, A.; Pap, Z.; Kalmár, Z.; Plozer, E.; Csathó, A.; Gábriel, R.; Komoly, S.; et al. Coffee consumption may influence hippocampal volume in young women. Brain Imaging Behav. 2011, 5, 274–284. [Google Scholar] [CrossRef]
- Jagodzinski, A.; Johansen, C.; Koch-Gromus, U.; Aarabi, G.; Adam, G.; Anders, S.; Augustin, M.; der Kellen, R.B.; Beikler, T.; Behrendt, C.-A.; et al. Rationale and Design of the Hamburg City Health Study. Eur. J. Epidemiol. 2020, 35, 169–181. [Google Scholar] [CrossRef]
- D’Agostino, R.B., Sr.; Vasan, R.S.; Pencina, M.J.; Wolf, P.A.; Cobain, M.; Massaro, J.M.; Kannel, W.B. General Cardiovascular Risk Profile for Use in Primary Care. Circulation 2008, 117, 743–753. [Google Scholar] [CrossRef]
- Nöthlings, U.; Hoffmann, K.; Bergmann, M.M.; Boeing, H. Fitting Portion Sizes in a Self-Administered Food Frequency Questionnaire. J. Nutr. 2007, 137, 2781–2786. [Google Scholar] [CrossRef]
- UNESCO Institute for Statistics. International Standard Classification of Education (ISCED) 2011; UNESCO Institute for Statistics: Montreal, QC, Canada, 2012; ISBN 978-92-9189-123-8. [Google Scholar]
- Hebestreit, K.; Yahiaoui-Doktor, M.; Engel, C.; Vetter, W.; Siniatchkin, M.; Erickson, N.; Halle, M.; Kiechle, M.; Bischoff, S.C. Validation of the German version of the Mediterranean Diet Adherence Screener (MEDAS) questionnaire. BMC Cancer 2017, 17, 341. [Google Scholar] [CrossRef]
- Petersen, M.; Naegele, F.L.; Mayer, C.; Schell, M.; Petersen, E.; Kuehn, S.; Gallinat, J.; Fiehler, J.; Pasternak, O.; Matschke, J.; et al. Brain Imaging and Neuropsychological Assessment of Individuals Recovered from Mild COVID-19. BioRxiv, 2022; preprint. [Google Scholar] [CrossRef]
- Gorgolewski, K.; Burns, C.D.; Madison, C.; Clark, D.; Halchenko, Y.O.; Waskom, M.L.; Ghosh, S.S. Nipype: A Flexible, Lightweight and Extensible Neuroimaging Data Processing Framework in Python. Front. Neuroinform. 2011, 5, 13. [Google Scholar] [CrossRef]
- Cieslak, M.; Cook, P.A.; He, X.; Yeh, F.-C.; Dhollander, T.; Adebimpe, A.; Aguirre, G.K.; Bassett, D.S.; Betzel, R.F.; Bourque, J.; et al. QSIPrep: An integrative platform for preprocessing and reconstructing diffusion MRI data. Nat. Methods 2021, 18, 775–778. [Google Scholar] [CrossRef]
- Fischl, B.; Salat, D.H.; Busa, E.; Albert, M.; Dieterich, M.; Haselgrove, C.; van der Kouwe, A.; Killiany, R.; Kennedy, D.; Klaveness, S.; et al. Whole Brain Segmentation: Automated Labeling of Neuroanatomical Structures in the Human Brain. Neuron 2002, 33, 341–355. [Google Scholar] [CrossRef]
- Fischl, B.; Dale, A.M. Measuring the thickness of the human cerebral cortex from magnetic resonance images. Proc. Natl. Acad. Sci. USA 2000, 97, 11050–11055. [Google Scholar] [CrossRef]
- Sundaresan, V.; Zamboni, G.; Le Heron, C.; Rothwell, P.M.; Husain, M.; Battaglini, M.; De Stefano, N.; Jenkinson, M.; Griffanti, L. Automated lesion segmentation with BIANCA: Impact of population-level features, classification algorithm and locally adaptive thresholding. Neuroimage 2019, 202, 116056. [Google Scholar] [CrossRef]
- Griffanti, L.; Zamboni, G.; Khan, A.; Li, L.; Bonifacio, G.; Sundaresan, V.; Schulz, U.G.; Kuker, W.; Battaglini, M.; Rothwell, P.M.; et al. BIANCA (Brain Intensity AbNormality Classification Algorithm): A new tool for automated segmentation of white matter hyperintensities. Neuroimage 2016, 141, 191–205. [Google Scholar] [CrossRef]
- Avants, B.; Epstein, C.; Grossman, M.; Gee, J. Symmetric diffeomorphic image registration with cross-correlation: Evaluating automated labeling of elderly and neurodegenerative brain. Med. Image Anal. 2008, 12, 26–41. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018. [Google Scholar]
- Andersen, L.F.; Jacobs, D.R.; Carlsen, M.H.; Blomhoff, R. Consumption of coffee is associated with reduced risk of death attributed to inflammatory and cardiovascular diseases in the Iowa Women’s Health Study. Am. J. Clin. Nutr. 2006, 83, 1039–1046. [Google Scholar] [CrossRef]
- Jeszka-Skowron, M.; Zgoła-Grześkowiak, A.; Grześkowiak, T. Analytical methods applied for the characterization and the determination of bioactive compounds in coffee. Eur. Food Res. Technol. 2014, 240, 19–31. [Google Scholar] [CrossRef]
- Van Dijk, E.J.; Prins, N.D.; Vermeer, S.E.; Vrooman, H.A.; Hofman, A.; Koudstaal, P.J.; Breteler, M.M. C-Reactive Protein and Cerebral Small-Vessel Disease: The Rotterdam Scan Study. Circulation 2005, 112, 900–905. [Google Scholar] [CrossRef]
- Satizabal, C.L.; Zhu, Y.C.; Mazoyer, B.; Dufouil, C.; Tzourio, C. Circulating IL-6 and CRP are associated with MRI findings in the elderly: The 3C-Dijon Study. Neurology 2012, 78, 720–727. [Google Scholar] [CrossRef] [PubMed]
- Walker, K.A.; Power, M.C.; Hoogeveen, R.C.; Folsom, A.R.; Ballantyne, C.M.; Knopman, D.S.; Windham, B.G.; Selvin, E.; Jack, C.R., Jr.; Gottesman, R.F. Midlife Systemic Inflammation, Late-Life White Matter Integrity, and Cerebral Small Vessel Disease—The Atherosclerosis Risk in Communities Study. Stroke 2017, 48, 3196–3202. [Google Scholar] [CrossRef]
- Engelhart, M.J.; Geerlings, M.I.; Meijer, J.; Kiliaan, A.; Ruitenberg, A.; van Swieten, J.C.; Stijnen, T.; Hofman, A.; Witteman, J.C.M.; Breteler, M.M.B. Inflammatory Proteins in Plasma and the Risk of Dementia: The Rotterdam Study. Arch. Neurol. 2004, 61, 668–672. [Google Scholar] [CrossRef] [PubMed]
- Cesari, M.; Penninx, B.W.; Newman, A.B.; Kritchevsky, S.B.; Nicklas, B.J.; Sutton-Tyrrell, K.; Rubin, S.M.; Ding, J.; Simonsick, E.M.; Harris, T.B.; et al. Inflammatory Markers and Onset of Cardiovascular Events: Results From the Health ABC Study. Circulation 2003, 108, 2317–2322. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.; Jia, T.; Jiao, Z.; Shen, C.; Xie, C.; Cheng, W.; Sahakian, B.J.; Waxman, D.; Feng, J. Increased brain volume from higher cereal and lower coffee intake: Shared genetic determinants and impacts on cognition and metabolism. Cereb. Cortex 2022, 32, 5163–5174. [Google Scholar] [CrossRef] [PubMed]
- Behan, W.M.H.; Stone, T.W. Enhanced neuronal damage by co-administration of quinolinic acid and free radicals, and protection by adenosine A2A receptor antagonists: Quinolinate and Free Radicals. Br. J. Pharmacol. 2002, 135, 1435–1442. [Google Scholar] [CrossRef] [PubMed]
- Monopoli, A.; Lozza, G.; Forlani, A.; Mattavelli, A.; Ongini, E. Blockade of adenosine A2A receptors by SCH 58261 results in neuroprotective effects in cerebral ischaemia in rats. Neuroreport 1998, 9, 3955–3958. [Google Scholar] [CrossRef]
- Chen, J.-F.; Xu, K.; Petzer, J.P.; Staal, R.; Xu, Y.-H.; Beilstein, M.; Sonsalla, P.K.; Castagnoli, K.; Castagnoli, N.; Schwarzschild, M.A. Neuroprotection by Caffeine and A2A Adenosine Receptor Inactivation in a Model of Parkinson’s Disease. J. Neurosci. 2001, 21, RC143. [Google Scholar] [CrossRef]
- Ding, M.; Bhupathiraju, S.N.; Satija, A.; van Dam, R.; Hu, F.B. Long-Term Coffee Consumption and Risk of Cardiovascular Disease: A systematic review and a dose-response meta-analysis of prospective cohort studies. Circulation 2014, 129, 643–659. [Google Scholar] [CrossRef]
- Liebeskind, D.S.; Sanossian, N.; Fu, K.A.; Wang, H.-J.; Arab, L. The coffee paradox in stroke: Increased consumption linked with fewer strokes. Nutr. Neurosci. 2015, 19, 406–413. [Google Scholar] [CrossRef]
- Taylor-Bateman, V.; Gill, D.; Georgakis, M.K.; Malik, R.; Munroe, P.; Traylor, M.; on behalf of the International Consortium of Blood Pressure (ICBP). Cardiovascular Risk Factors and MRI Markers of Cerebral Small Vessel Disease: A Mendelian Ran-domization Study. Neurology 2021, 98, e343–e351. [Google Scholar] [CrossRef]
- Barbaresko, J.; Lellmann, A.W.; Schmidt, A.; Lehmann, A.; Amini, A.M.; Egert, S.; Schlesinger, S.; Nöthlings, U. Dietary Factors and Neurodegenerative Disorders: An Umbrella Review of Meta-Analyses of Prospective Studies. Adv. Nutr. 2020, 11, 1161–1173. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Coffee Consumption | p-Value * | |||||
|---|---|---|---|---|---|---|---|
| Overall Cohort | <1 c/d | 1–2 c/d | 3–4 c/d | 5–6 c/d | >6 c/d | ||
| Group size | 2316 | 459 | 1020 | 581 | 176 | 80 | |
| Sociodemographic characteristics | |||||||
| Age, median (IQR) | 65 (14) | 67 (13) | 67 (13) | 62 (14) | 61 (13) | 60 (9) | <0.001 |
| Female sex, n (%) | 1026 (44.3) | 191 (41.61) | 501 (49.12) | 254 (43.72) | 55 (31.25) | 25 (31.25) | <0.001 |
| Education 1 | <0.001 | ||||||
| Low, n (%) | 98 (4.23) | 25 (5.75) | 47 (4.78) | 18 (3.2) | 6 (3.49) | 2 (2.53) | |
| Medium, n (%) | 1087 (46.93) | 219 (50.34) | 472 (47.97) | 275 (48.85) | 80 (46.51) | 41 (51.9) | |
| High, n (%) | 1048 (45.25) | 191 (43.91) | 465 (47.26) | 270 (47.96) | 86 (50) | 36 (45.57) | |
| Cardiovascular risk factors | |||||||
| Smoking, n (%) | 320 (13.82) | 37 (9.3) | 113 (12.58) | 110 (21.07) | 39 (24.68) | 21 (28.77) | <0.001 |
| Diabetes mellitus, n (%) 2 | 210 (9.07) | 61 (13.96) | 88 (9.23) | 45 (8.43) | 12 (7.14) | 4 (5.33) | 0.01 |
| Hypertension, n (%) 3 | 1611 (69.56) | 330 (73.99) | 734 (74.37) | 380 (68.1) | 121 (69.94) | 46 (61.33) | 0.015 |
| BMI, median (IQR) | 26.15 (9.45) | 26.18 (5.59) | 25.96 (5.44) | 26.11 (5.43) | 26.49 (4.59) | 28 (4.9) | 0.02 |
| Alcohol consumption [monthly frequency], median (IQR) | 3 (9) | 3 (9) | 3 (7) | 10 (13) | 10 (14) | 3 (9) | 0.001 |
| Adherence to the Mediterranean diet, median (IQR) | 4 (3) | 4 (3) | 4 (3) | 4 (3) | 5 (3) | 4 (2) | 0.945 |
| MRI parameters | |||||||
| Brain volume [mL], median (IQR) | 1210.3 (166.6) | 1204.38 (157.79) | 1195.82 (168.59) | 1226.89 (162.09) | 1238.15 (162.73) | 1240.43 (150.83) | <0.001 |
| Mean cortical thickness [mm], median (IQR) | 2.61 (0.13) | 2.6 (0.13) | 2.61 (0.13) | 2.62 (0.13) | 2.61 (0.11) | 2.62 (0.11) | <0.001 |
| WMH volume [mL], median (IQR) | 1.48 (2.22) | 1.61 (2.18) | 1.59 (2.51) | 1.29 (2.09) | 1.32 (1.93) | 1.28 (1.71) | 0.002 |
| PSMD [×105], median (IQR) | 22.3 (4.31) | 22.77 (4.61) | 22.52 (4.36) | 21.96 (4.05) | 22.24 (4.37) | 21.44 (2.81) | <0.001 |
| Dependent Variable | PSMD [×105] | Mean Cortical Thickness [mm] | log WMH Load 4 | |||
|---|---|---|---|---|---|---|
| β | p | β | p | β | p | |
| Intercept | 23.96 | <0.001 | 2.571 | <0.001 | −6.967 | <0.001 |
| Age | 1.917 | <0.001 | −0.025 | 0.001 | 0.558 | <0.001 |
| Sex—female | −0.84 | <0.001 | 0.009 | 0.074 | 0.273 | <0.001 |
| Education—medium 1 | −0.705 | 0.125 | 0.031 | 0.012 | −0.148 | 0.257 |
| Education—high 1 | −0.663 | 0.155 | 0.044 | <0.001 | −0.294 | 0.027 |
| Hypertension—yes 2 | 0.455 | 0.029 | −0.006 | 0.245 | 0.133 | 0.026 |
| Diabetes—yes 3 | 0.911 | 0.005 | −0.013 | 0.147 | 0.097 | 0.299 |
| Smoking—yes | 0.577 | 0.023 | −0.013 | 0.06 | 0.153 | 0.035 |
| Alcohol consumption | 0.303 | 0.001 | −0.006 | 0.017 | 0.025 | 0.358 |
| BMI | 0.114 | 0.221 | 0.008 | 0.002 | 0.015 | 0.586 |
| Mediterranean diet | −0.002 | 0.986 | −0.001 | 0.569 | −0.039 | 0.123 |
| Coffee consumption—1–2 c/d | −0.542 | 0.022 | 0.004 | 0.544 | −0.025 | 0.71 |
| Coffee consumption—3–4 c/d | −0.591 | 0.028 | 0.018 | 0.015 | 0.061 | 0.429 |
| Coffee consumption—5–6 c/d | −0.014 | 0.97 | 0.002 | 0.831 | 0.001 | 0.994 |
| Coffee consumption—>6 c/d | −0.461 | 0.386 | −0.001 | 0.941 | −0.01 | 0.944 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mayer, C.; Nägele, F.L.; Petersen, M.; Schell, M.; Aarabi, G.; Beikler, T.; Borof, K.; Frey, B.M.; Nikorowitsch, J.; Senftinger, J.; et al. Association between Coffee Consumption and Brain MRI Parameters in the Hamburg City Health Study. Nutrients 2023, 15, 674. https://doi.org/10.3390/nu15030674
Mayer C, Nägele FL, Petersen M, Schell M, Aarabi G, Beikler T, Borof K, Frey BM, Nikorowitsch J, Senftinger J, et al. Association between Coffee Consumption and Brain MRI Parameters in the Hamburg City Health Study. Nutrients. 2023; 15(3):674. https://doi.org/10.3390/nu15030674
Chicago/Turabian StyleMayer, Carola, Felix L. Nägele, Marvin Petersen, Maximilian Schell, Ghazal Aarabi, Thomas Beikler, Katrin Borof, Benedikt M. Frey, Julius Nikorowitsch, Juliana Senftinger, and et al. 2023. "Association between Coffee Consumption and Brain MRI Parameters in the Hamburg City Health Study" Nutrients 15, no. 3: 674. https://doi.org/10.3390/nu15030674
APA StyleMayer, C., Nägele, F. L., Petersen, M., Schell, M., Aarabi, G., Beikler, T., Borof, K., Frey, B. M., Nikorowitsch, J., Senftinger, J., Walther, C., Wenzel, J.-P., Zyriax, B.-C., Cheng, B., & Thomalla, G. (2023). Association between Coffee Consumption and Brain MRI Parameters in the Hamburg City Health Study. Nutrients, 15(3), 674. https://doi.org/10.3390/nu15030674