.png)

Glucose Metabolism and Metabolomic Changes in Response to Prolonged Fasting in Individuals with Obesity, Type 2 Diabetes and Non-Obese People—A Cohort Trial


 ,
,  ,
,  , , ,
, , ,  ,
,  add
Show full author list
add
Show full author list
Abstract

1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Study Design
2.3. Oral Glucose Tolerance Test (OGTT)
2.3.1. Homeostasis Model Assessment-Insulin Resistance
2.3.2. Quantitative Insulin Sensitivity Check Index
2.3.3. Matsuda Index
2.3.4. Indices of Insulin Secretion
2.4. Intravenous Glucose Tolerance Test (IVGTT)
2.5. Biochemical Measurements
2.6. Serum Sample Preparation for Metabolomics
2.7. Sample Size Calculation
2.8. Statistical Analysis
2.9. Metabolomics Data Analysis
2.10. Primary and Secondary Outcomes
3. Results
3.1. Baseline Characteristics
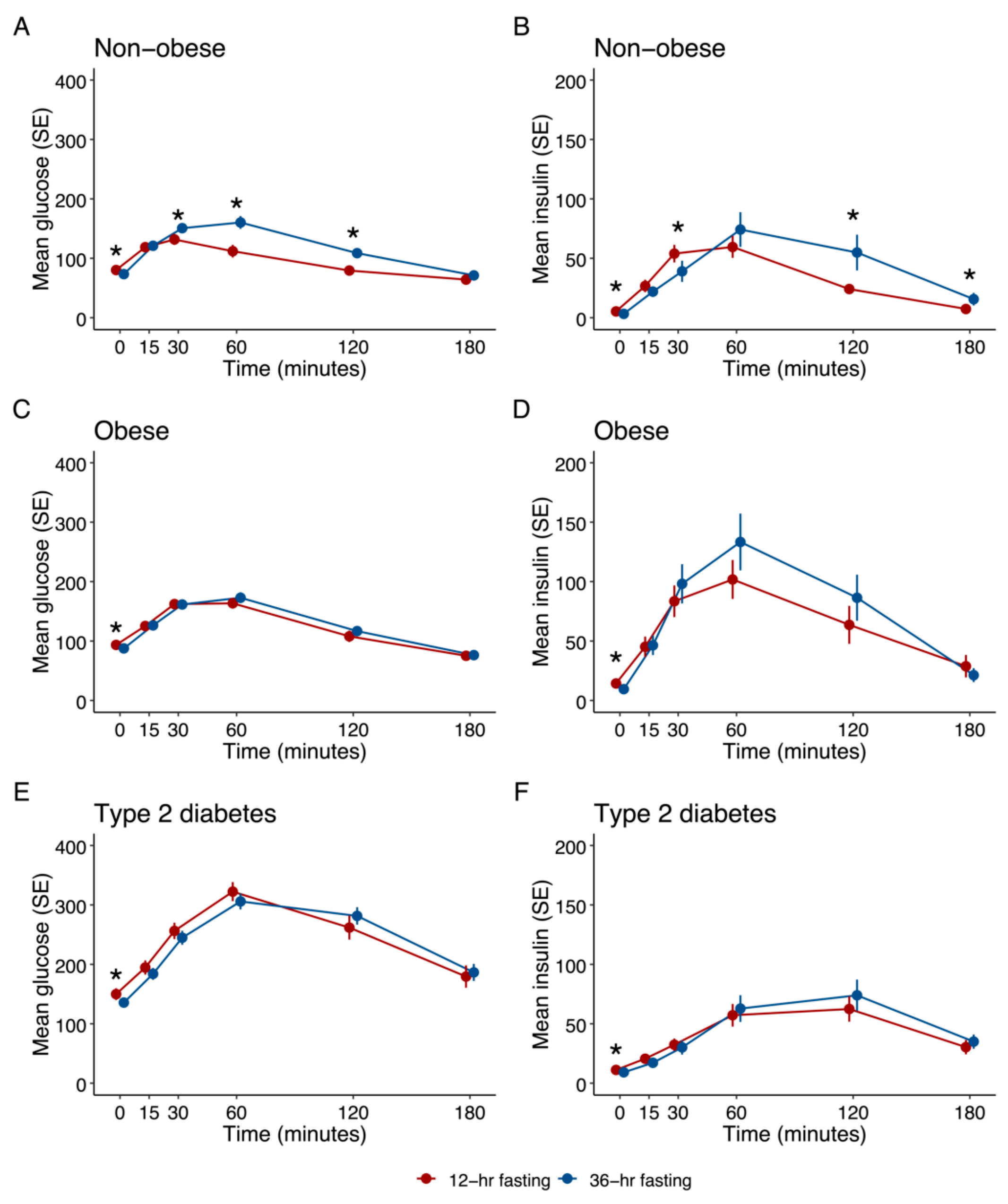
3.2. Glycaemic Parameters
3.2.1. Non-Obese Healthy Subjects
3.2.2. Obese Subjects
3.2.3. Subjects with Type 2 Diabetes (T2D)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-Obese Cohort (n = 20) | Obese Cohort (n = 20) | Type 2 Diabetes Cohort (n = 20) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| after 12 h Fasting | after 36 h Fasting | p-Value | after 12 h Fasting | after 36 h Fasting | p-Value | after 12 h Fasting | after 36 h Fasting | p-Value | |
| Fasting glucose (mg/dL) | 80 ± 7 | 73 ± 11 | 0.003 | 94 ± 10 | 88 ± 13 | 0.002 | 150 ± 37 | 136 ± 26 | 0.017 |
| Plasma glucose 120 min (mg/dL) | 79 ± 18 | 109 ± 31 | 0.001 | 108 ± 36 | 117 ± 29 | 0.067 | 262 ± 83 | 282 ± 59 | 0.121 |
| Fasting insulin (mU/L) | 4.3 (4.0–7.1) | 2.5 (1.8–4.1) | 0.002 | 11.4 (6.7–15.9) | 7.2 (5.0–14.5) | 0.020 | 11.2 ± 4.4 | 9.2 ± 5.8 | 0.007 |
| Fasting C-peptide (ng/mL) | 0.94 (0.83–1.13) | 0.61 (0.43–0.82) | 0.001 | 2.00 (1.55–2.46) | 1.65 (0.95–2.24) | 0.036 | 2.31 ± 0.75 | 1.94 ± 1.02 | 0.002 |
| Glucose (mg/dL) AUC (in minutes) | 17,070 ± 3128 | 21,627 ± 4002 | 0.000 | 22,638 ± 3872 | 23,315 ± 3622 | 0.197 | 46,771 ± 11532 | 46,238 ± 7822 | 0.734 |
| Insulin (mU/L) AUC (in minutes) | 5592 ± 2679 | 7557 ± 5448 | 0.137 | 12,621 ± 8364 | 13,794 ± 9254 | 0.629 | 7695 ± 4427 | 8337 ± 4394 | 0.392 |
| QUICKI | 0.39 (0.37–0.40) | 0.45 (0.41–0.49) | 0.000 | 0.33 (0.31–0.35) | 0.36 (0.32–0.39) | 0.021 | 0.31 (0.30–0.33) | 0.32 (0.31–0.37) | 0.001 |
| HOMAIR | 0.86 (0.75–1.41) | 0.43 (0.27–0.67) | 0.001 | 2.52 (1.72–4.27) | 1.37 (0.90–3.07) | 0.001 | 4.26 ± 2.06 | 3.17 ± 2.17 | 0.012 |
| ISI | 1.28 ± 0.95 | 1.88 ± 1.34 | 0.004 | 0.40 (0.32–0.53) | 0.54 (0.27–0.72) | 0.078 | 0.26 (0.22–0.48) | 0.30 (0.20–0.68) | 0.014 |
| Proinsulin (pmol/L) | 3.9 (3.4–5.0) | 3.6 (2.7–4.6) | 0.111 | 9.9 (7.0–25.9) | 11.1 (6.6–16.6) | 0.151 | 23.6 (15.3–37.1) | 20.7 (10.6–33.0) | 0.019 |
| 1st phase insulin secretion | 1138 ± 496 | 742 ± 471 | 0.001 | 1400 ± 956 | 1408 ± 759 | 0.972 | −68 ± 635 | −17 ± 585 | 0.536 |
| 2nd phase insulin secretion | 295 ± 108 | 211 ± 104 | 0.001 | 370 ± 224 | 370 ± 176 | 0.994 | 68 ± 130 | 73 ± 125 | 0.740 |
| HOMA-β | 105.4 (75.9–161.7) | 63.6 (18.4–175.9) | 0.202 | 140.3 (89.1–240.0) | 149.1 (82.3–252.9) | 0.963 | 53.2 ± 31.8 | 47.1 ± 32.4 | 0.102 |
| ΔIns30/ΔGlc30 | 1.14 (0.95–1.50) | 0.49 (0.13–0.86) | 0.001 | 0.83 (0.50–1.91) | 0.92 (0.47–2.11) | 0.762 | 0.23 ± 0.23 | 0.21 ± 0.22 | 0.157 |
3.2.4. Comparison between Groups
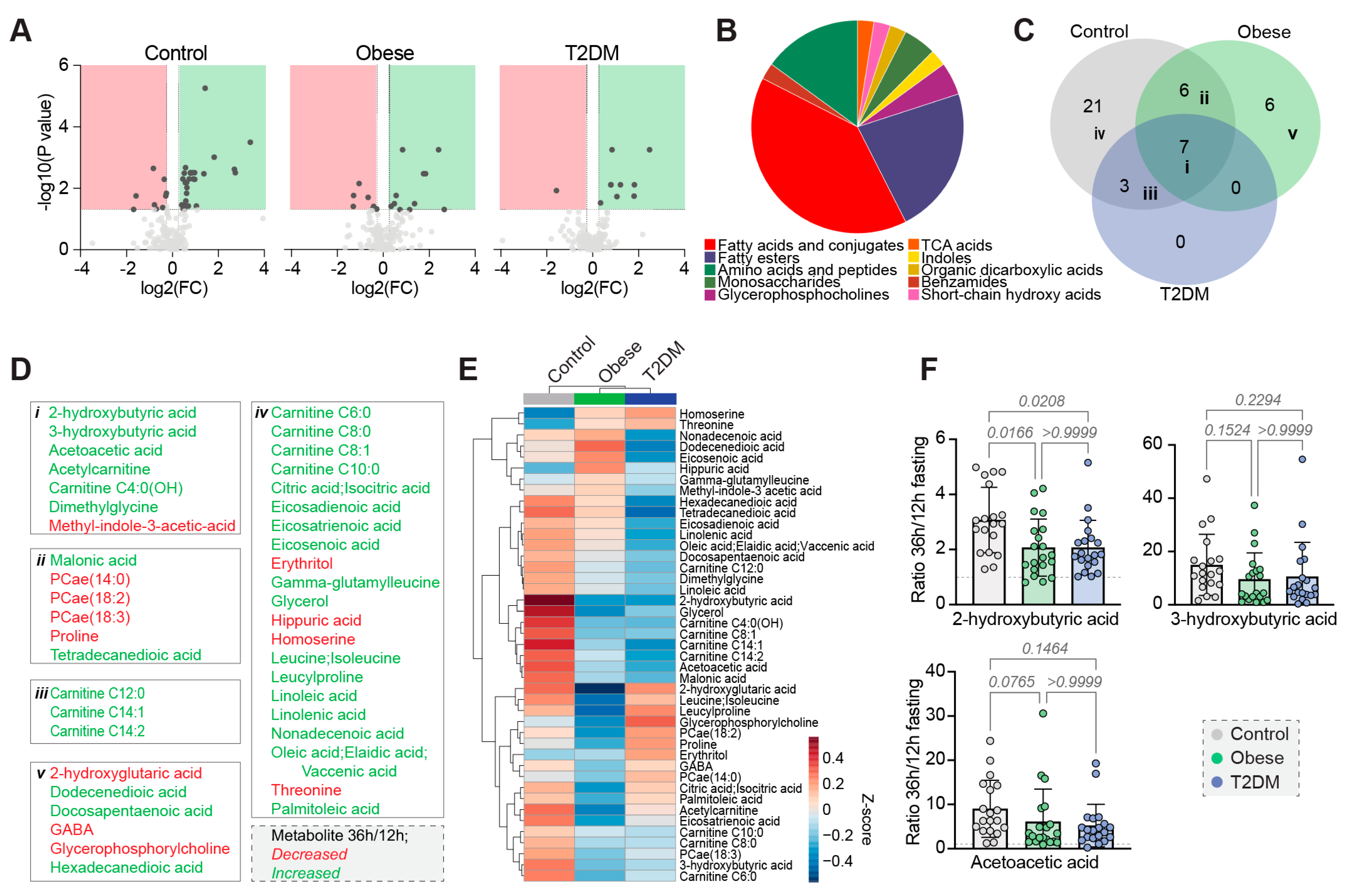
3.3. Metabolomics Results
3.3.1. Twelve Hours Fasting Period
3.3.2. Thirty-Six Hours Fasting Period
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Soeters, M.R.; Soeters, P.B.; Schooneman, M.G.; Houten, S.M.; Romijn, J.A. Adaptive reciprocity of lipid and glucose metabolism in human short-term starvation. Am. J. Physiol. Endocrinol. Metab. 2012, 303, E1397–E1407. [Google Scholar] [CrossRef]
- Goodpaster, B.H.; Sparks, L.M. Metabolic Flexibility in Health and Disease. Cell Metab. 2017, 25, 1027–1036. [Google Scholar] [CrossRef]
- Hofer, S.J.; Carmona-Gutierrez, D.; Mueller, M.I.; Madeo, F. The ups and downs of caloric restriction and fasting: From molecular effects to clinical application. EMBO Mol. Med. 2022, 14, e14418. [Google Scholar] [CrossRef]
- De Cabo, R.; Mattson, M.P. Effects of Intermittent Fasting on Health, Aging, and Disease. N. Engl. J. Med. 2019, 381, 2541–2551. [Google Scholar] [CrossRef]
- Anson, R.M.; Guo, Z.; de Cabo, R.; Iyun, T.; Rios, M.; Hagepanos, A.; Ingram, D.K.; Lane, M.A.; Mattson, M.P. Intermittent fasting dissociates beneficial effects of dietary restriction on glucose metabolism and neuronal resistance to injury from calorie intake. Proc. Natl. Acad. Sci. USA 2003, 100, 6216–6220. [Google Scholar] [CrossRef]
- Li, L.; Wang, Z.; Zuo, Z. Chronic intermittent fasting improves cognitive functions and brain structures in mice. PLoS ONE 2013, 8, e66069. [Google Scholar] [CrossRef]
- Anderson, J.W.; Herman, R.H. Effects of carbohydrate restriction on glucose tolerance of normal men and reactive hypoglycemic patients. Am. J. Clin. Nutr. 1975, 28, 748–755. [Google Scholar] [CrossRef]
- Pehleman, T.L.; Peters, S.J.; Heigenhauser, G.J.; Spriet, L.L. Enzymatic regulation of glucose disposal in human skeletal muscle after a high-fat, low-carbohydrate diet. J. Appl. Physiol. (1985) 2005, 98, 100–107. [Google Scholar] [CrossRef]
- Unger, R.H.; Eisentraut, A.M.; Madison, L.L. The effects of total starvation upon the levels of circulating glucagon and insulin in man. J. Clin. Investig. 1963, 42, 1031–1039. [Google Scholar] [CrossRef]
- Allison, S.P. Effect of insulin on metabolic response to injury. JPEN J. Parenter. Enter. Nutr. 1980, 4, 175–179. [Google Scholar] [CrossRef]
- Best, C.H.; Haist, R.E.; Ridout, J.H. Diet and the insulin content of pancreas. J. Physiol. 1939, 97, 107–119. [Google Scholar] [CrossRef]
- American Diabetes Association Professional Practice Committee. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022, 45, S17–S38. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Chen, H.; Sullivan, G.; Yue, L.Q.; Katz, A.; Quon, M.J. QUICKI is a useful index of insulin sensitivity in subjects with hypertension. Am. J. Physiol. Endocrinol. Metab. 2003, 284, E804–E812. [Google Scholar] [CrossRef]
- Matsuda, M.; DeFronzo, R.A. Insulin sensitivity indices obtained from oral glucose tolerance testing: Comparison with the euglycemic insulin clamp. Diabetes Care 1999, 22, 1462–1470. [Google Scholar] [CrossRef]
- Stumvoll, M.; Van Haeften, T.; Fritsche, A.; Gerich, J. Oral glucose tolerance test indexes for insulin sensitivity and secretion based on various availabilities of sampling times. Diabetes Care 2001, 24, 796–797. [Google Scholar] [CrossRef]
- Seltzer, H.S.; Allen, E.W.; Herron, A.L., Jr.; Brennan, M.T. Insulin secretion in response to glycemic stimulus: Relation of delayed initial release to carbohydrate intolerance in mild diabetes mellitus. J. Clin. Investig. 1967, 46, 323–335. [Google Scholar] [CrossRef]
- Grajeda-Iglesias, C.; Durand, S.; Daillere, R.; Iribarren, K.; Lemaitre, F.; Derosa, L.; Aprahamian, F.; Bossut, N.; Nirmalathasan, N.; Madeo, F.; et al. Oral administration of Akkermansia muciniphila elevates systemic antiaging and anticancer metabolites. Aging 2021, 13, 6375–6405. [Google Scholar] [CrossRef]
- Durand, S.; Grajeda-Iglesias, C.; Aprahamian, F.; Nirmalathasan, N.; Kepp, O.; Kroemer, G. The intracellular metabolome of starving cells. Methods Cell Biol. 2021, 164, 137–156. [Google Scholar] [CrossRef]
- Stekovic, S.; Hofer, S.J.; Tripolt, N.; Aon, M.A.; Royer, P.; Pein, L.; Stadler, J.T.; Pendl, T.; Prietl, B.; Url, J.; et al. Alternate Day Fasting Improves Physiological and Molecular Markers of Aging in Healthy, Non-obese Humans. Cell Metab. 2019, 30, 462–476.e6. [Google Scholar] [CrossRef]
- Pang, Z.; Chong, J.; Zhou, G.; de Lima Morais, D.A.; Chang, L.; Barrette, M.; Gauthier, C.; Jacques, P.E.; Li, S.; Xia, J. MetaboAnalyst 5.0: Narrowing the gap between raw spectra and functional insights. Nucleic Acids Res. 2021, 49, W388–W396. [Google Scholar] [CrossRef] [PubMed]
- Jorgensen, S.W.; Hjort, L.; Gillberg, L.; Justesen, L.; Madsbad, S.; Brons, C.; Vaag, A.A. Impact of prolonged fasting on insulin secretion, insulin action, and hepatic versus whole body insulin secretion disposition indices in healthy young males. Am. J. Physiol. Endocrinol. Metab. 2021, 320, E281–E290. [Google Scholar] [CrossRef] [PubMed]
- Salgin, B.; Marcovecchio, M.L.; Humphreys, S.M.; Hill, N.; Chassin, L.J.; Lunn, D.J.; Hovorka, R.; Dunger, D.B. Effects of prolonged fasting and sustained lipolysis on insulin secretion and insulin sensitivity in normal subjects. Am. J. Physiol. Endocrinol. Metab. 2009, 296, E454–E461. [Google Scholar] [CrossRef] [PubMed]
- Rorsman, P.; Braun, M. Regulation of insulin secretion in human pancreatic islets. Annu. Rev. Physiol. 2013, 75, 155–179. [Google Scholar] [CrossRef]
- Goginashvili, A.; Zhang, Z.; Erbs, E.; Spiegelhalter, C.; Kessler, P.; Mihlan, M.; Pasquier, A.; Krupina, K.; Schieber, N.; Cinque, L.; et al. Insulin granules. Insulin secretory granules control autophagy in pancreatic beta cells. Science 2015, 347, 878–882. [Google Scholar] [CrossRef] [PubMed]
- Knop, F.K.; Aaboe, K.; Vilsboll, T.; Volund, A.; Holst, J.J.; Krarup, T.; Madsbad, S. Impaired incretin effect and fasting hyperglucagonaemia characterizing type 2 diabetic subjects are early signs of dysmetabolism in obesity. Diabetes Obes. Metab. 2012, 14, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Nauck, M.; Stockmann, F.; Ebert, R.; Creutzfeldt, W. Reduced incretin effect in type 2 (non-insulin-dependent) diabetes. Diabetologia 1986, 29, 46–52. [Google Scholar] [CrossRef]
- Sundfor, T.M.; Svendsen, M.; Tonstad, S. Effect of intermittent versus continuous energy restriction on weight loss, maintenance and cardiometabolic risk: A randomized 1-year trial. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 698–706. [Google Scholar] [CrossRef]
- Beaulieu, K.; Casanova, N.; Oustric, P.; Turicchi, J.; Gibbons, C.; Hopkins, M.; Varady, K.; Blundell, J.; Finlayson, G. Matched Weight Loss Through Intermittent or Continuous Energy Restriction Does Not Lead To Compensatory Increases in Appetite and Eating Behavior in a Randomized Controlled Trial in Women with Overweight and Obesity. J. Nutr. 2020, 150, 623–633. [Google Scholar] [CrossRef]
- Harvie, M.; Wright, C.; Pegington, M.; McMullan, D.; Mitchell, E.; Martin, B.; Cutler, R.G.; Evans, G.; Whiteside, S.; Maudsley, S.; et al. The effect of intermittent energy and carbohydrate restriction v. daily energy restriction on weight loss and metabolic disease risk markers in overweight women. Br. J. Nutr. 2013, 110, 1534–1547. [Google Scholar] [CrossRef]
- Martin, C.K.; Heilbronn, L.K.; de Jonge, L.; DeLany, J.P.; Volaufova, J.; Anton, S.D.; Redman, L.M.; Smith, S.R.; Ravussin, E. Effect of calorie restriction on resting metabolic rate and spontaneous physical activity. Obesity 2007, 15, 2964–2973. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, A.; Doucet, E. Relative changes in resting energy expenditure during weight loss: A systematic review. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2010, 11, 531–547. [Google Scholar] [CrossRef] [PubMed]
- Obermayer, A.; Tripolt, N.J.; Pferschy, P.N.; Kojzar, H.; Aziz, F.; Muller, A.; Schauer, M.; Oulhaj, A.; Aberer, F.; Sourij, C.; et al. Efficacy and Safety of Intermittent Fasting in People With Insulin-Treated Type 2 Diabetes (INTERFAST-2)-A Randomized Controlled Trial. Diabetes Care 2022, dc221622. [Google Scholar] [CrossRef]
- Zhang, A.H.; Sun, H.; Yan, G.L.; Yuan, Y.; Han, Y.; Wang, X.J. Metabolomics study of type 2 diabetes using ultra-performance LC-ESI/quadrupole-TOF high-definition MS coupled with pattern recognition methods. J. Physiol. Biochem. 2014, 70, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Al-Sulaiti, H.; Diboun, I.; Agha, M.V.; Mohamed, F.F.S.; Atkin, S.; Domling, A.S.; Elrayess, M.A.; Mazloum, N.A. Metabolic signature of obesity-associated insulin resistance and type 2 diabetes. J. Transl. Med. 2019, 17, 348. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.; Jang, H.B.; Ra, M.; Choi, Y.; Lee, H.J.; Park, J.Y.; Kang, J.H.; Park, K.H.; Park, S.I.; Song, J. Prediction of future risk of insulin resistance and metabolic syndrome based on Korean boy’s metabolite profiling. Obes. Res. Clin. Pract. 2015, 9, 336–345. [Google Scholar] [CrossRef]
- LaBarre, J.L.; Hirschfeld, E.; Soni, T.; Kachman, M.; Wigginton, J.; Duren, W.; Fleischman, J.Y.; Karnovsky, A.; Burant, C.F.; Lee, J.M. Comparing the Fasting and Random-Fed Metabolome Response to an Oral Glucose Tolerance Test in Children and Adolescents: Implications of Sex, Obesity, and Insulin Resistance. Nutrients 2021, 13, 3365. [Google Scholar] [CrossRef]
- Gall, W.E.; Beebe, K.; Lawton, K.A.; Adam, K.P.; Mitchell, M.W.; Nakhle, P.J.; Ryals, J.A.; Milburn, M.V.; Nannipieri, M.; Camastra, S.; et al. alpha-hydroxybutyrate is an early biomarker of insulin resistance and glucose intolerance in a nondiabetic population. PLoS ONE 2010, 5, e10883. [Google Scholar] [CrossRef]
- Sousa, A.P.; Cunha, D.M.; Franco, C.; Teixeira, C.; Gojon, F.; Baylina, P.; Fernandes, R. Which Role Plays 2-Hydroxybutyric Acid on Insulin Resistance? Metabolites 2021, 11, 835. [Google Scholar] [CrossRef]
- Zhang, H.; Zhao, Y.; Zhao, D.; Chen, X.; Khan, N.U.; Liu, X.; Zheng, Q.; Liang, Y.; Zhu, Y.; Iqbal, J.; et al. Potential biomarkers identified in plasma of patients with gestational diabetes mellitus. Metabolomics 2021, 17, 99. [Google Scholar] [CrossRef]
- DiNicolantonio, J.J.; McCarty, M.F.; JH, O.K. Role of dietary histidine in the prevention of obesity and metabolic syndrome. Open Heart 2018, 5, e000676. [Google Scholar] [CrossRef] [PubMed]
- Iaconelli, A.; Gastaldelli, A.; Chiellini, C.; Gniuli, D.; Favuzzi, A.; Binnert, C.; Mace, K.; Mingrone, G. Effect of oral sebacic Acid on postprandial glycemia, insulinemia, and glucose rate of appearance in type 2 diabetes. Diabetes Care 2010, 33, 2327–2332. [Google Scholar] [CrossRef] [PubMed]
- Hellmuth, C.; Kirchberg, F.F.; Lass, N.; Harder, U.; Peissner, W.; Koletzko, B.; Reinehr, T. Tyrosine Is Associated with Insulin Resistance in Longitudinal Metabolomic Profiling of Obese Children. J. Diabetes Res. 2016, 2016, 2108909. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.H.; Li, J.; Feng, X.F.; Sun, X.Y.; Li, J.; Yang, X.; Fang, Z.Z. Plasma phenylalanine and tyrosine and their interactions with diabetic nephropathy for risk of diabetic retinopathy in type 2 diabetes. BMJ Open Diabetes Res. Care 2020, 8, e000877. [Google Scholar] [CrossRef]
- Mohorko, N.; Petelin, A.; Jurdana, M.; Biolo, G.; Jenko-Praznikar, Z. Elevated serum levels of cysteine and tyrosine: Early biomarkers in asymptomatic adults at increased risk of developing metabolic syndrome. BioMed Res. Int. 2015, 2015, 418681. [Google Scholar] [CrossRef]
- Zhou, C.; Zhang, Q.; Lu, L.; Wang, J.; Liu, D.; Liu, Z. Metabolomic Profiling of Amino Acids in Human Plasma Distinguishes Diabetic Kidney Disease From Type 2 Diabetes Mellitus. Front. Med. 2021, 8, 765873. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.W. Metabolomic Approaches to Investigate the Effect of Metformin: An Overview. Int. J. Mol. Sci. 2021, 22, 10275. [Google Scholar] [CrossRef]



| Non-Obese Cohort (n = 20) | Obese Cohort (n = 20) | Type 2 Diabetes Cohort (n = 20) | |
|---|---|---|---|
| Age (years) | 32 ± 10 | 37 ± 10 | 60 ± 9 |
| Bodyweight (kg) | 67.5 ± 9.6 | 102.7 ± 14.1 | 64.9 ± 23.9 |
| Height (cm) | 173 ± 10 | 174 ± 8 | 176 ± 8 |
| BMI (kg/m2) 1 | 22.6 ± 1.7 | 34.6 ± 4.8 | 31.0 ± 7.1 |
| Blood pressure systolic (mmHg) | 117 ± 11 | 122 ± 10 | 123 ± 12 |
| Blood pressure diastolic (mmHg) | 76 ± 13 | 79 ± 11 | 74 ± 8 |
| Waist to hip ratio | 0.8 ± 0.1 | 0.9 ± 0.1 | 1.0 ± 0.1 |
| Fasting glucose (mg/dL) | 80.3 ± 7.3 | 93.5 ± 14.9 | 149.9 ± 36.9 |
| Fasting insulin (mU/L) | 5.3 ± 2.5 | 14.3 ± 14.9 | 11.1 ± 4.3 |
| HbA1c (mmol/mol) | 32 ± 2 | 35 ± 3 | 53 ± 8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tripolt, N.J.; Hofer, S.J.; Pferschy, P.N.; Aziz, F.; Durand, S.; Aprahamian, F.; Nirmalathasan, N.; Waltenstorfer, M.; Eisenberg, T.; Obermayer, A.M.A.; et al. Glucose Metabolism and Metabolomic Changes in Response to Prolonged Fasting in Individuals with Obesity, Type 2 Diabetes and Non-Obese People—A Cohort Trial. Nutrients 2023, 15, 511. https://doi.org/10.3390/nu15030511
Tripolt NJ, Hofer SJ, Pferschy PN, Aziz F, Durand S, Aprahamian F, Nirmalathasan N, Waltenstorfer M, Eisenberg T, Obermayer AMA, et al. Glucose Metabolism and Metabolomic Changes in Response to Prolonged Fasting in Individuals with Obesity, Type 2 Diabetes and Non-Obese People—A Cohort Trial. Nutrients. 2023; 15(3):511. https://doi.org/10.3390/nu15030511
Chicago/Turabian StyleTripolt, Norbert J., Sebastian J. Hofer, Peter N. Pferschy, Faisal Aziz, Sylvère Durand, Fanny Aprahamian, Nitharsshini Nirmalathasan, Mara Waltenstorfer, Tobias Eisenberg, Anna M. A. Obermayer, and et al. 2023. "Glucose Metabolism and Metabolomic Changes in Response to Prolonged Fasting in Individuals with Obesity, Type 2 Diabetes and Non-Obese People—A Cohort Trial" Nutrients 15, no. 3: 511. https://doi.org/10.3390/nu15030511
APA StyleTripolt, N. J., Hofer, S. J., Pferschy, P. N., Aziz, F., Durand, S., Aprahamian, F., Nirmalathasan, N., Waltenstorfer, M., Eisenberg, T., Obermayer, A. M. A., Riedl, R., Kojzar, H., Moser, O., Sourij, C., Bugger, H., Oulhaj, A., Pieber, T. R., Zanker, M., Kroemer, G., ... Sourij, H. (2023). Glucose Metabolism and Metabolomic Changes in Response to Prolonged Fasting in Individuals with Obesity, Type 2 Diabetes and Non-Obese People—A Cohort Trial. Nutrients, 15(3), 511. https://doi.org/10.3390/nu15030511