
Egg Intake Is Associated with Lower Risks of Impaired Fasting Glucose and High Blood Pressure in Framingham Offspring Study Adults
 , and
, and
Abstract
1. Introduction
2. Materials and Methods
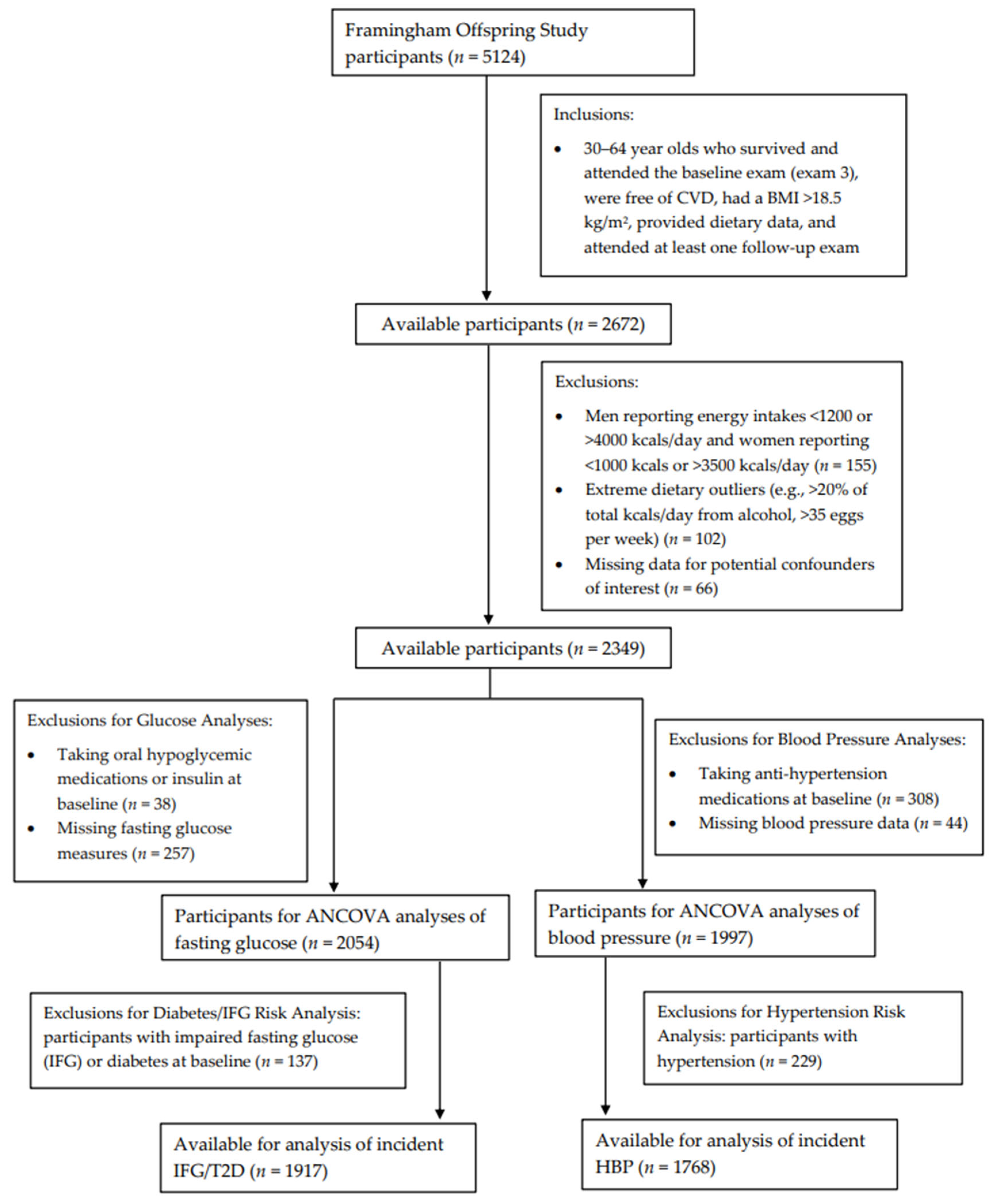
2.1. Study Population
2.2. Dietary Assessment
2.3. Main Outcome Measures
2.4. Potential Confounders
2.5. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Center for Health Statistics; Heron, M. Deaths: Leading Causes for 2018; National Center for Health Statistics: Hyattsville, MD, USA, 2021; Volume 70, pp. 1–114.
- Drouin-Chartier, J.-P.; Chen, S.; Li, Y.; Schwab, A.L.; Stampfer, M.J.; Sacks, F.M.; Rosner, B.; Willett, W.C.; Hu, F.B.; Bhupathiraju, S.N. Egg Consumption and Risk of Cardiovascular Disease: Three Large Prospective US Cohort Studies, Systematic Review, and Updated Meta-Analysis. BMJ 2020, 368, m513. [Google Scholar] [CrossRef]
- Kanter, M.M.; Kris-Etherton, P.M.; Fernandez, M.L.; Vickers, K.C.; Katz, D.L. Exploring the Factors That Affect Blood Cholesterol and Heart Disease Risk: Is Dietary Cholesterol as Bad for You as History Leads Us to Believe? Adv. Nutr. 2012, 3, 711–717. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services and U.S. Department of Agriculture. 2015–2020 Dietary Guidelines for Americans, 8th ed.; U.S. Department of Health and Human Services and U.S. Department of Agriculture: Washington, DC, USA, 2015.
- Zhong, V.W.; Van Horn, L.; Cornelis, M.C.; Wilkins, J.T.; Ning, H.; Carnethon, M.R.; Greenland, P.; Mentz, R.J.; Tucker, K.L.; Zhao, L.; et al. Associations of Dietary Cholesterol or Egg Consumption With Incident Cardiovascular Disease and Mortality. JAMA 2019, 321, 1081–1095. [Google Scholar] [CrossRef]
- Berger, S.; Raman, G.; Vishwanathan, R.; Jacques, P.F.; Johnson, E.J. Dietary Cholesterol and Cardiovascular Disease: A Systematic Review and Meta-Analysis. Am. J. Clin. Nutr. 2015, 102, 276–294. [Google Scholar] [CrossRef]
- Chen, G.-C.; Chen, L.-H.; Mossavar-Rahmani, Y.; Kamensky, V.; Shadyab, A.H.; Haring, B.; Wild, R.A.; Silver, B.; Kuller, L.H.; Sun, Y.; et al. Dietary Cholesterol and Egg Intake in Relation to Incident Cardiovascular Disease and All-Cause and Cause-Specific Mortality in Postmenopausal Women. Am. J. Clin. Nutr. 2021, 113, 948–959. [Google Scholar] [CrossRef]
- Liu, X.; Shao, Y.; Sun, J.; Tu, J.; Wang, Z.; Tao, J.; Chen, J. Egg Consumption Improves Vascular and Gut Microbiota Function without Increasing Inflammatory, Metabolic, and Oxidative Stress Markers. Food Sci. Nutr. 2022, 10, 295–304. [Google Scholar] [CrossRef]
- Go, A.S.; Mozaffarian, D.; Roger, V.L.; Benjamin, E.J.; Berry, J.D.; Borden, W.B.; Bravata, D.M.; Dai, S.; Ford, E.S.; Fox, C.S.; et al. Heart Disease and Stroke Statistics—2013 Update: A Report From the American Heart Association. Circulation 2013, 127, e6–e245. [Google Scholar] [CrossRef] [PubMed]
- Tamez, M.; Virtanen, J.K.; Lajous, M. Egg Consumption and Risk of Incident Type 2 Diabetes: A Dose–Response Meta-Analysis of Prospective Cohort Studies. Br. J. Nutr. 2016, 115, 2212–2218. [Google Scholar] [CrossRef] [PubMed]
- Drouin-Chartier, J.-P.; Schwab, A.L.; Chen, S.; Li, Y.; Sacks, F.M.; Rosner, B.; Manson, J.E.; Willett, W.C.; Stampfer, M.J.; Hu, F.B.; et al. Egg Consumption and Risk of Type 2 Diabetes: Findings from 3 Large US Cohort Studies of Men and Women and a Systematic Review and Meta-Analysis of Prospective Cohort Studies. Am. J. Clin. Nutr. 2020, 112, 619–630. [Google Scholar] [CrossRef]
- Wallin, A.; Forouhi, N.G.; Wolk, A.; Larsson, S.C. Egg Consumption and Risk of Type 2 Diabetes: A Prospective Study and Dose–Response Meta-Analysis. Diabetologia 2016, 59, 1204–1213. [Google Scholar] [CrossRef] [PubMed]
- Fuller, N.R.; Caterson, I.D.; Sainsbury, A.; Denyer, G.; Fong, M.; Gerofi, J.; Baqleh, K.; Williams, K.H.; Lau, N.S.; Markovic, T.P. The Effect of a High-Egg Diet on Cardiovascular Risk Factors in People with Type 2 Diabetes: The Diabetes and Egg (DIABEGG) Study—A 3-Mo Randomized Controlled Trial. Am. J. Clin. Nutr. 2015, 101, 705–713. [Google Scholar] [CrossRef]
- Mutungi, G.; Ratliff, J.; Puglisi, M.; Torres-Gonzalez, M.; Vaishnav, U.; Leite, J.O.; Quann, E.; Volek, J.S.; Fernandez, M.L. Dietary Cholesterol from Eggs Increases Plasma HDL Cholesterol in Overweight Men Consuming a Carbohydrate-Restricted Diet. J. Nutr. 2008, 138, 272–276. [Google Scholar] [CrossRef]
- Pearce, K.L.; Clifton, P.M.; Noakes, M. Egg Consumption as Part of an Energy-Restricted High-Protein Diet Improves Blood Lipid and Blood Glucose Profiles in Individuals with Type 2 Diabetes. Br. J. Nutr. 2011, 105, 584–592. [Google Scholar] [CrossRef]
- Tran, N.L.; Barraj, L.; Heilman, J.; Scrafford, C. Egg Consumption and Cardiovascular Disease among Diabetic Individuals: A Systematic Review of the Literature. Diabetes Metab. Syndr. Obes. Targets Ther. 2014, 7, 121–137. [Google Scholar] [CrossRef] [PubMed]
- Fuller, N.; Sainsbury, A.; Caterson, I.; Markovic, T. Egg Consumption and Human Cardio-Metabolic Health in People with and without Diabetes. Nutrients 2015, 7, 7399–7420. [Google Scholar] [CrossRef]
- Nicklas, T.A.; O’Neil, C.E.; Fulgoni, V.L. Differing Statistical Approaches Affect the Relation between Egg Consumption, Adiposity, and Cardiovascular Risk Factors in Adults. J. Nutr. 2015, 145, 170S–176S. [Google Scholar] [CrossRef]
- Kolahdouz-Mohammadi, R.; Malekahmadi, M.; Clayton, Z.S.; Sadat, S.Z.; Pahlavani, N.; Sikaroudi, M.K.; Soltani, S. Effect of Egg Consumption on Blood Pressure: A Systematic Review and Meta-Analysis of Randomized Clinical Trials. Curr. Hypertens. Rep. 2020, 22, 24. [Google Scholar] [CrossRef] [PubMed]
- Katz, D.L.; Evans, M.A.; Nawaz, H.; Njike, V.Y.; Chan, W.; Comerford, B.P.; Hoxley, M.L. Egg Consumption and Endothelial Function: A Randomized Controlled Crossover Trial. Int. J. Cardiol. 2005, 99, 65–70. [Google Scholar] [CrossRef]
- Katz, D.L.; Gnanaraj, J.; Treu, J.A.; Ma, Y.; Kavak, Y.; Njike, V.Y. Effects of Egg Ingestion on Endothelial Function in Adults with Coronary Artery Disease: A Randomized, Controlled, Crossover Trial. Am. Heart J. 2015, 169, 162–169. [Google Scholar] [CrossRef]
- Zhou, C.; Wu, Q.; Ye, Z.; Liu, M.; Zhang, Z.; Zhang, Y.; Li, H.; He, P.; Li, Q.; Liu, C.; et al. Inverse Association Between Variety of Proteins with Appropriate Quantity From Different Food Sources and New-Onset Hypertension. Hypertension 2022, 79, 1017–1027. [Google Scholar] [CrossRef]
- Kritchevsky, S.B. A Review of Scientific Research and Recommendations Regarding Eggs. J. Am. Coll. Nutr. 2004, 23, 596S–600S. [Google Scholar] [CrossRef] [PubMed]
- Kannel, W.B.; Feinleib, M.; McNAMARA, P.M.; Garrison, R.J.; Castelli, W.P. An Investigation of Coronary Heart Disease in Families. The Framingham Offspring Study. Am. J. Epidemiol. 1979, 110, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Schakel, S.F. Sources of Data for Developing and Maintaining a Nutrient Database. J. Am. Diet. Assoc. 1988, 88, 1268–1271. [Google Scholar] [CrossRef] [PubMed]
- Moore, L.L.; Singer, M.R.; Bradlee, M.L.; Djouss, L.; Proctor, M.H.; Cupples, L.A.; Ellison, R.C. Intake of Fruits, Vegetables, and Dairy Products in Early Childhood and Subsequent Blood Pressure Change. Epidemiology 2005, 16, 4–11. [Google Scholar] [CrossRef]
- Guenther, P.M.; Reedy, J.; Krebs-Smith, S.M. Development of the Healthy Eating Index-2005. J. Am. Diet. Assoc. 2008, 108, 1896–1901. [Google Scholar] [CrossRef]
- Meigs, J.B.; Mittleman, M.A.; Nathan, D.M.; Tofler, G.H.; Singer, D.E.; Murphy-Sheehy, P.M.; Lipinska, I.; D’Agostino, R.B.; Wilson, P.W.F. Hyperinsulinemia, Hyperglycemia, and Impaired Hemostasis: The Framingham Offspring Study. JAMA 2000, 283, 221–228. [Google Scholar] [CrossRef]
- The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Diabetes Care 1997, 20, 1183–1197. [Google Scholar] [CrossRef]
- The Sixth Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Arch. Intern. Med. 1997, 157, 2413–2446. [CrossRef]
- Phillips, L.S.; Weintraub, W.S.; Ziemer, D.C.; Kolm, P.; Foster, J.K.; Vaccarino, V.; Rhee, M.K.; Budhwani, R.K.; Caudle, J.M. All Pre-Diabetes Is Not the Same: Metabolic and Vascular Risks of Impaired Fasting Glucose at 100 Versus 110 Mg/Dl. Diabetes Care 2006, 29, 1405–1407. [Google Scholar] [CrossRef] [PubMed]
- Kannel, W.B. Some Health Benefits of Physical Activity: The Framingham Study. Arch. Intern. Med. 1979, 139, 857–861. [Google Scholar] [CrossRef]
- Kouvari, M.; Damigou, E.; Florentin, M.; Kosti, R.I.; Chrysohoou, C.; Pitsavos, C.S.; Panagiotakos, D.B. Egg Consumption, Cardiovascular Disease and Cardiometabolic Risk Factors: The Interaction with Saturated Fatty Acids. Results from the ATTICA Cohort Study (2002–2012). Nutrients 2022, 14, 5291. [Google Scholar] [CrossRef]
- Virtanen, J.K.; Mursu, J.; Tuomainen, T.-P.; Virtanen, H.E.; Voutilainen, S. Egg Consumption and Risk of Incident Type 2 Diabetes in Men: The Kuopio Ischaemic Heart Disease Risk Factor Study. Am. J. Clin. Nutr. 2015, 101, 1088–1096. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Kim, J. Egg Consumption Is Associated with a Lower Risk of Type 2 Diabetes in Middle-Aged and Older Men. Nutr. Res. Pract. 2018, 12, 396–405. [Google Scholar] [CrossRef] [PubMed]
- Geiker, N.R.W.; Larsen, M.L.; Dyerberg, J.; Stender, S.; Astrup, A. Egg Consumption, Cardiovascular Diseases and Type 2 Diabetes. Eur. J. Clin. Nutr. 2018, 72, 44–56. [Google Scholar] [CrossRef]
- Ho, C.P.; Yu, J.H.; Lee, T.J.F. Ovo-Vegetarian Diet Is Associated with Lower Systemic Blood Pressure in Taiwanese Women. Public Health 2017, 153, 70–77. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B. A Prospective Study of Egg Consumption and Risk of Cardiovascular Disease in Men and Women. JAMA 1999, 281, 1387–1394. [Google Scholar] [CrossRef]
- Azzout-Marniche, D.; Gaudichon, C.; Tomé, D. Dietary Protein and Blood Glucose Control. Curr. Opin. Clin. Nutr. Metab. Care 2014, 17, 349–354. [Google Scholar] [CrossRef]
- Ribaya-Mercado, J.D.; Blumberg, J.B. Lutein and Zeaxanthin and Their Potential Roles in Disease Prevention. J. Am. Coll. Nutr. 2004, 23, 567S–587S. [Google Scholar] [CrossRef]
- Coyne, T.; Ibiebele, T.I.; Baade, P.D.; Dobson, A.; McClintock, C.; Dunn, S.; Leonard, D.; Shaw, J. Diabetes Mellitus and Serum Carotenoids: Findings of a Population-Based Study in Queensland, Australia. Am. J. Clin. Nutr. 2005, 82, 685–693. [Google Scholar] [CrossRef]
- Kaulmann, A.; Bohn, T. Carotenoids, Inflammation, and Oxidative Stress—Implications of Cellular Signaling Pathways and Relation to Chronic Disease Prevention. Nutr. Res. 2014, 34, 907–929. [Google Scholar] [CrossRef]
- Applegate, E. Introduction: Nutritional and Functional Roles of Eggs in the Diet. J. Am. Coll. Nutr. 2000, 19, 495S–498S. [Google Scholar] [CrossRef] [PubMed]
- Pittas, A.G.; Lau, J.; Hu, F.B.; Dawson-Hughes, B. The Role of Vitamin D and Calcium in Type 2 Diabetes. A Systematic Review and Meta-Analysis. J. Clin. Endocrinol. Metab. 2007, 92, 2017–2029. [Google Scholar] [CrossRef] [PubMed]
- Chelliah, R.; Wei, S.; Daliri, E.B.-M.; Elahi, F.; Yeon, S.-J.; Tyagi, A.; Liu, S.; Madar, I.H.; Sultan, G.; Oh, D.-H. The Role of Bioactive Peptides in Diabetes and Obesity. Foods 2021, 10, 2220. [Google Scholar] [CrossRef] [PubMed]
- Bhat, Z.F.; Kumar, S.; Bhat, H.F. Antihypertensive Peptides of Animal Origin: A Review. Crit. Rev. Food Sci. Nutr. 2017, 57, 566–578. [Google Scholar] [CrossRef]
- Martynowicz, H.; Nowacki, D.; Mazur, G.; Trziszka, T.; Szuba, A. The Phospholipid Fraction Obtained from Egg Yolk Reduces Blood Pressure Increase Induced by Acute Stress in Spontaneously Hypertensive Rats. Adv. Clin. Exp. Med. 2018, 27, 1745–1749. [Google Scholar] [CrossRef]
- Jahandideh, F.; Majumder, K.; Chakrabarti, S.; Morton, J.S.; Panahi, S.; Kaufman, S.; Davidge, S.T.; Wu, J. Beneficial Effects of Simulated Gastro-Intestinal Digests of Fried Egg and Its Fractions on Blood Pressure, Plasma Lipids and Oxidative Stress in Spontaneously Hypertensive Rats. PLoS ONE 2014, 9, e115006. [Google Scholar] [CrossRef]
- Teunissen-Beekman, K.F.M.; van Baak, M.A. The Role of Dietary Protein in Blood Pressure Regulation. Curr. Opin. Lipidol. 2013, 24, 65–70. [Google Scholar] [CrossRef]


{kind=link}
| Weekly Number of Eggs Consumed | ||||
|---|---|---|---|---|
| 0 to 0.5 | 0.5 to <5 | ≥5 | p-Trend | |
| Subjects, n | 353 | 1329 | 372 | |
| Male, n (%) | 133 (37.7%) | 568 (42.7%) | 223 (60.0%) | <0.0001 |
| Smoker, n (% current) | 79 (22.4%) | 285 (21.4%) | 98 (26.3%) | 0.14 |
| More than high school 2, n (%) | 178 (57.2%) | 754 (63.2%) | 201 (61.1%) | 0.15 |
| Age, years | 49.6 ± 0.47 | 48.6 ± 0.24 | 48.1 ± 0.46 | 0.07 |
| Height, cm | 168.5 ± 0.33 | 168.5 ± 0.18 | 169.2 ± 0.33 | 0.18 |
| BMI, kg/m2 | 26.2 ± 0.23 | 26.0 ± 0.12 | 26.8 ± 0.23 | 0.003 |
| Systolic blood pressure, mmHg | 124.1 ± 0.84 | 122.4 ± 0.43 | 122.1 ± 0.82 | 0.15 |
| Diastolic blood pressure, mmHg | 78.4 ± 0.49 | 77.8 ± 0.25 | 77.8 ± 0.48 | 0.53 |
| Fasting glucose, mg/dL | 95.4 ± 0.71 | 92.5 ± 0.36 | 92.7 ± 0.69 | 0.001 |
| Physical activity index | 12.7 ± 0.42 | 12.4 ± 0.22 | 13.0 ± 0.41 | 0.30 |
| Energy intake, kcals/day | 1722 ± 24.1 | 1919 ± 12.4 | 2074 ± 23.6 | <0.0001 |
| Dietary cholesterol, mg/day | 173 ± 4.19 | 242 ± 2.16 | 402 ± 4.11 | <0.0001 |
| Protein, % of energy | 17.7 ± 0.17 | 16.8 ± 0.09 | 16.4 ± 0.17 | <0.0001 |
| Carbohydrate, % of energy | 47.4 ± 0.42 | 46.2 ± 0.22 | 43.9 ± 0.41 | <0.0001 |
| Fat, % of energy | 32.9 ± 0.34 | 35.1 ± 0.18 | 38.0 ± 0.33 | <0.0001 |
| Saturated fat, % of energy | 10.9 ± 0.15 | 12.0 ± 0.08 | 13.3 ± 0.15 | <0.0001 |
| SoFAAs, % energy | 12.5 ± 0.28 | 10.3 ± 0.14 | 8.7 ± 0.27 | <0.0001 |
| FNSV, cup equivalents/day | 2.6 ± 0.07 | 2.6 ± 0.04 | 2.3 ± 0.07 | 0.006 |
| Whole grains, ounce equivalents/day | 0.6 ± 0.04 | 0.6 ± 0.02 | 0.5 ± 0.04 | 0.17 |
| Dairy, cup equivalents/day | 1.3 ± 0.05 | 1.4 ± 0.02 | 1.4 ± 0.05 | 0.16 |
| Dietary fiber, grams/day | 16.1 ± 0.32 | 16.1 ± 0.16 | 15.5 ± 0.31 | 0.16 |
| All Subjects | BMI < 25 kg/m2 | BMI ≥ 25 kg/m2 | Females | Males | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Egg Intake/Week | n | Mean ± SE | n | Mean ± SE | n | Mean ± SE | n | Mean ± SE | n | Mean ± SE |
| Fasting glucose (mg/dL) | ||||||||||
| <0.5 | 353 | 96.6 ± 0.73 | 157 | 90.9 ± 0.72 | 196 | 101.0 ± 1.20 | 220 | 94.2 ± 0.90 | 133 | 99.5 ± 1.21 |
| 0.5 to <5 | 1329 | 93.2 ± 0.38 | 610 | 88.7 ± 0.37 | 719 | 96.4 ± 0.63 | 761 | 90.6 ± 0.49 | 568 | 96.4 ± 0.59 |
| ≥5 | 372 | 92.9 ± 0.72 | 132 | 89.3 ± 0.79 | 240 | 96.5 ± 1.09 | 149 | 90.4 ± 1.10 | 223 | 96.0 ± 0.94 |
| p-trend | 0.0004 | 0.0979 | 0.0098 | 0.0025 | 0.0450 | |||||
| Systolic blood pressure (mmHg) | ||||||||||
| <0.5 | 354 | 125.7 ± 0.78 | 164 | 119.4 ± 1.13 | 190 | 131.1 ± 1.09 | 223 | 122.7 ± 1.01 | 131 | 129.9 ± 1.20 |
| 0.5 to <5 | 1269 | 123.6 ± 0.41 | 618 | 118.6 ± 0.58 | 651 | 127.8 ± 0.59 | 743 | 121.6 ± 0.55 | 526 | 126.1 ± 0.60 |
| ≥5 | 374 | 123.3 ± 0.76 | 143 | 120.0 ± 1.21 | 231 | 127.0 ± 0.99 | 147 | 121.3 ± 1.25 | 227 | 125.8 ± 0.91 |
| p-trend | 0.0284 | 0.7581 | 0.0071 | 0.3419 | 0.0173 | |||||
| Diastolic blood pressure (mmHg) | ||||||||||
| <0.5 | 354 | 78.6 ± 0.47 | 164 | 74.3 ± 0.69 | 190 | 82.3 ± 0.65 | 223 | 75.8 ± 0.61 | 131 | 82.4 ± 0.75 |
| 0.5 to <5 | 1269 | 77.6 ± 0.25 | 618 | 74.5 ± 0.35 | 651 | 80.1 ± 0.35 | 743 | 75.4 ± 0.33 | 526 | 80.3 ± 0.37 |
| ≥5 | 374 | 77.6 ± 0.46 | 143 | 75.0 ± 0.74 | 231 | 80.2 ± 0.60 | 147 | 74.9 ± 0.75 | 227 | 80.7 ± 0.57 |
| p-trend | 0.1157 | 0.5064 | 0.0279 | 0.3783 | 0.1530 | |||||
| Fasting Glucose (mg/dL) | SBP (mmHg) | DBP (mmHg) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline Diet Pattern 2 | n | Mean ± SE | p-Value | n | Mean ± SE | p-Value | n | Mean ± SE | p-Value |
| Eggs/Dairy | |||||||||
| Lower/Lower | 876 | 94.2 ± 0.47 | - | 841 | 124.3 ± 0.51 | - | 841 | 78.1 ± 0.31 | - |
| Lower/Higher | 294 | 94.1 ± 0.80 | 0.9154 | 287 | 124.5 ± 0.86 | 0.8574 | 287 | 77.2 ± 0.52 | 0.1427 |
| Higher/Lower | 621 | 93.7 ± 0.55 | 0.4693 | 608 | 123.7 ± 0.59 | 0.4646 | 608 | 77.8 ± 0.36 | 0.5196 |
| Higher/Higher | 263 | 91.9 ± 0.86 | 0.0203 | 261 | 122.5 ± 0.91 | 0.0793 | 261 | 77.0 ± 0.56 | 0.0784 |
| Eggs/Fish | |||||||||
| Lower/Lower | 592 | 94.6 ± 0.57 | - | 582 | 124.4 ± 0.61 | - | 582 | 77.9 ± 0.37 | - |
| Lower/Higher | 578 | 93.7 ± 0.57 | 0.2221 | 546 | 124.3 ± 0.62 | 0.9680 | 546 | 77.9 ± 0.38 | 0.9755 |
| Higher/Lower | 461 | 94.0 ± 0.64 | 0.4424 | 470 | 123.4 ± 0.67 | 0.3046 | 470 | 77.3 ± 0.41 | 0.2954 |
| Higher/Higher | 423 | 92.2 ± 0.67 | 0.0063 | 399 | 123.3 ± 0.73 | 0.2545 | 399 | 77.9 ± 0.45 | 0.9935 |
| Eggs/WG | |||||||||
| Lower/Lower | 656 | 94.7 ± 0.54 | - | 626 | 124.9 ± 0.58 | - | 626 | 78.2 ± 0.36 | - |
| Lower/Higher | 514 | 93.5 ± 0.61 | 0.1279 | 502 | 123.6 ± 0.65 | 0.1396 | 502 | 77.5 ± 0.40 | 0.2483 |
| Higher/Lower | 516 | 93.2 ± 0.61 | 0.0762 | 501 | 123.1 ± 0.65 | 0.0331 | 501 | 77.2 ± 0.40 | 0.0851 |
| Higher/Higher | 368 | 93.0 ± 0.72 | 0.0591 | 368 | 123.8 ± 0.76 | 0.2377 | 368 | 78.0 ± 0.47 | 0.8443 |
| Eggs/Fiber | |||||||||
| Lower/Lower | 765 | 94.9 ± 0.57 | - | 737 | 125.0 ± 0.54 | - | 737 | 78.5 ± 0.33 | - |
| Lower/Higher | 405 | 92.9 ± 0.58 | 0.0136 | 391 | 123.1 ± 0.74 | 0.0364 | 391 | 76.8 ± 0.45 | 0.0018 |
| Higher/Lower | 585 | 93.3 ± 0.67 | 0.0351 | 574 | 123.7 ± 0.61 | 0.1135 | 574 | 77.8 ± 0.37 | 0.1917 |
| Higher/Higher | 299 | 92.9 ± 0.65 | 0.0367 | 295 | 122.7 ± 0.85 | 0.0195 | 295 | 77.1 ± 0.52 | 0.0201 |
| Eggs/FNSV | |||||||||
| Lower/Lower | 786 | 94.4 ± 0.49 | - | 769 | 124.7 ± 0.53 | - | 769 | 78.1 ± 0.32 | - |
| Lower/Higher | 384 | 93.5 ± 0.70 | 0.2779 | 359 | 123.6 ± 0.77 | 0.2437 | 359 | 77.4 ± 0.47 | 0.2536 |
| Higher/Lower | 634 | 93.4 ± 0.55 | 0.1610 | 631 | 123.5 ± 0.58 | 0.1360 | 631 | 77.6 ± 0.36 | 0.3121 |
| Higher/Higher | 250 | 92.4 ± 0.87 | 0.0448 | 238 | 122.9 ± 0.95 | 0.1060 | 238 | 77.5 ± 0.58 | 0.3697 |
| Egg Intake/Week | n | PY | Cases | Incidence Rate/1000 PY | HR (95% CI) 1 |
|---|---|---|---|---|---|
| All Subjects | |||||
| IFG/T2D 2 | |||||
| <0.5 | 316 | 3364.7 | 60 | 17.83 | 1.00 |
| 0.5 to <5 | 1254 | 14,318.8 | 219 | 15.30 | 0.74 (0.55, 0.98) |
| ≥5 | 347 | 3779.4 | 74 | 19.58 | 0.72 (0.51, 1.03) |
| High blood pressure | |||||
| <0.5 | 303 | 3082.6 | 93 | 30.17 | 1.00 |
| 0.5 to <5 | 1142 | 12,629.0 | 337 | 26.69 | 0.90 (0.71, 1.14) |
| ≥5 | 323 | 3511.0 | 78 | 22.22 | 0.68 (0.50, 0.93) |
| Females | |||||
| IFG/T2D | |||||
| <0.5 | 204 | 2155.6 | 33 | 15.31 | 1.00 |
| 0.5 to <5 | 727 | 8478.0 | 81 | 9.55 | 0.56 (0.37, 0.84) |
| ≥5 | 143 | 1529.7 | 24 | 15.69 | 0.63 (0.36, 1.10) |
| High blood pressure | |||||
| <0.5 | 199 | 2096.1 | 51 | 24.33 | 1.00 |
| 0.5 to <5 | 685 | 7645.0 | 192 | 25.12 | 1.08 (0.79, 1.48) |
| ≥5 | 135 | 1500.7 | 28 | 18.66 | 0.68 (0.42, 1.09) |
| Males | |||||
| IFG/T2D | |||||
| <0.5 | 112 | 1209.2 | 27 | 22.33 | 1.00 |
| 0.5 to <5 | 527 | 5840.7 | 138 | 23.63 | 0.97 (0.64, 1.48) |
| ≥5 | 204 | 2249.7 | 50 | 22.23 | 0.87 (0.54, 1.41) |
| High blood pressure | |||||
| <0.5 | 104 | 986.5 | 42 | 42.58 | 1.00 |
| 0.5 to <5 | 457 | 4984.0 | 145 | 29.09 | 0.71 (0.50, 1.00) |
| ≥5 | 188 | 2010.3 | 50 | 24.87 | 0.62 (0.40, 0.94) |
| IFG/Type 2 Diabetes 1 | High Blood Pressure 2 | |||
|---|---|---|---|---|
| Baseline Diet Pattern 3 | n | HR (95% CI) | n | HR (95% CI) |
| Eggs/Dairy | ||||
| Lower/Lower | 813 | 1.00 | 740 | 1.00 |
| Lower/Higher | 274 | 1.42 (1.04, 1.93) | 254 | 0.92 (0.70, 1.20) |
| Higher/Lower | 579 | 1.00 (0.78, 1.29) | 542 | 0.81 (0.66, 1.00) |
| Higher/Higher | 251 | 0.81 (0.57, 1.15) | 232 | 0.75 (0.56, 1.00) |
| Eggs/Fish | ||||
| Lower/Lower | 548 | 1.00 | 507 | 1.00 |
| Lower/Higher | 539 | 0.78 (0.59, 1.04) | 487 | 0.89 (0.71, 1.12) |
| Higher/Lower | 431 | 0.90 (0.67, 1.20) | 412 | 0.86 (0.67, 1.10) |
| Higher/Higher | 399 | 0.71 (0.52, 0.95) | 362 | 0.73 (0.56, 0.94) |
| Eggs/WG | ||||
| Lower/Lower | 604 | 1.00 | 552 | 1.00 |
| Lower/Higher | 483 | 0.93 (0.70, 1.24) | 442 | 0.88 (0.70, 1.11) |
| Higher/Lower | 479 | 1.01 (0.77, 1.32) | 444 | 0.72 (0.57, 0.92) |
| Higher/Higher | 351 | 0.71 (0.51, 0.98) | 330 | 0.88 (0.68, 1.13) |
| Eggs/Fiber | ||||
| Lower/Lower | 563 | 1.00 | 523 | 1.00 |
| Lower/Higher | 524 | 0.84 (0.63, 1.13) | 471 | 0.71 (0.56, 0.91) |
| Higher/Lower | 393 | 0.95 (0.70, 1.27) | 374 | 0.86 (0.68, 1.10) |
| Higher/Higher | 437 | 0.74 (0.55, 1.00) | 400 | 0.59 (0.46, 0.77) |
| Eggs/ FNSV | ||||
| Lower/Lower | 733 | 1.00 | 680 | 1.00 |
| Lower/Higher | 354 | 0.73 (0.53, 1.01) | 314 | 0.76 (0.59, 0.99) |
| Higher/Lower | 593 | 0.84 (0.66, 1.08) | 568 | 0.79 (0.64, 0.98) |
| Higher/Higher | 237 | 0.77 (0.55, 1.08) | 206 | 0.71 (0.52, 0.97) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mott, M.M.; Zhou, X.; Bradlee, M.L.; Singer, M.R.; Yiannakou, I.; Moore, L.L. Egg Intake Is Associated with Lower Risks of Impaired Fasting Glucose and High Blood Pressure in Framingham Offspring Study Adults. Nutrients 2023, 15, 507. https://doi.org/10.3390/nu15030507
Mott MM, Zhou X, Bradlee ML, Singer MR, Yiannakou I, Moore LL. Egg Intake Is Associated with Lower Risks of Impaired Fasting Glucose and High Blood Pressure in Framingham Offspring Study Adults. Nutrients. 2023; 15(3):507. https://doi.org/10.3390/nu15030507
Chicago/Turabian StyleMott, Melanie M., Xinyi Zhou, M. Loring Bradlee, Martha R. Singer, Ioanna Yiannakou, and Lynn L. Moore. 2023. "Egg Intake Is Associated with Lower Risks of Impaired Fasting Glucose and High Blood Pressure in Framingham Offspring Study Adults" Nutrients 15, no. 3: 507. https://doi.org/10.3390/nu15030507
APA StyleMott, M. M., Zhou, X., Bradlee, M. L., Singer, M. R., Yiannakou, I., & Moore, L. L. (2023). Egg Intake Is Associated with Lower Risks of Impaired Fasting Glucose and High Blood Pressure in Framingham Offspring Study Adults. Nutrients, 15(3), 507. https://doi.org/10.3390/nu15030507