


Plant-Based Diet Indices and Their Association with Frailty in Older Adults: A CLHLS-Based Cohort Study


Abstract
:1. Introduction
2. Objects and Methods
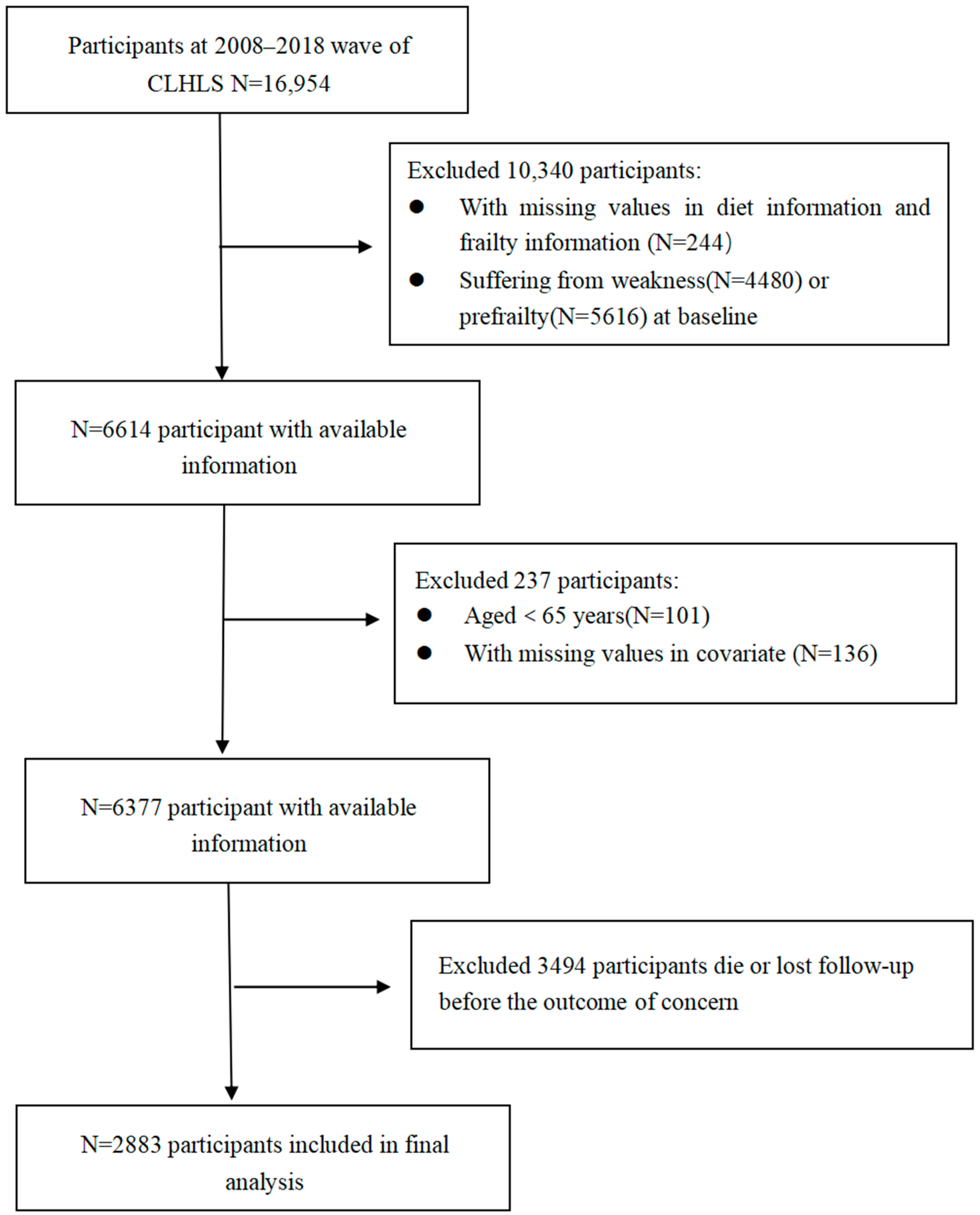
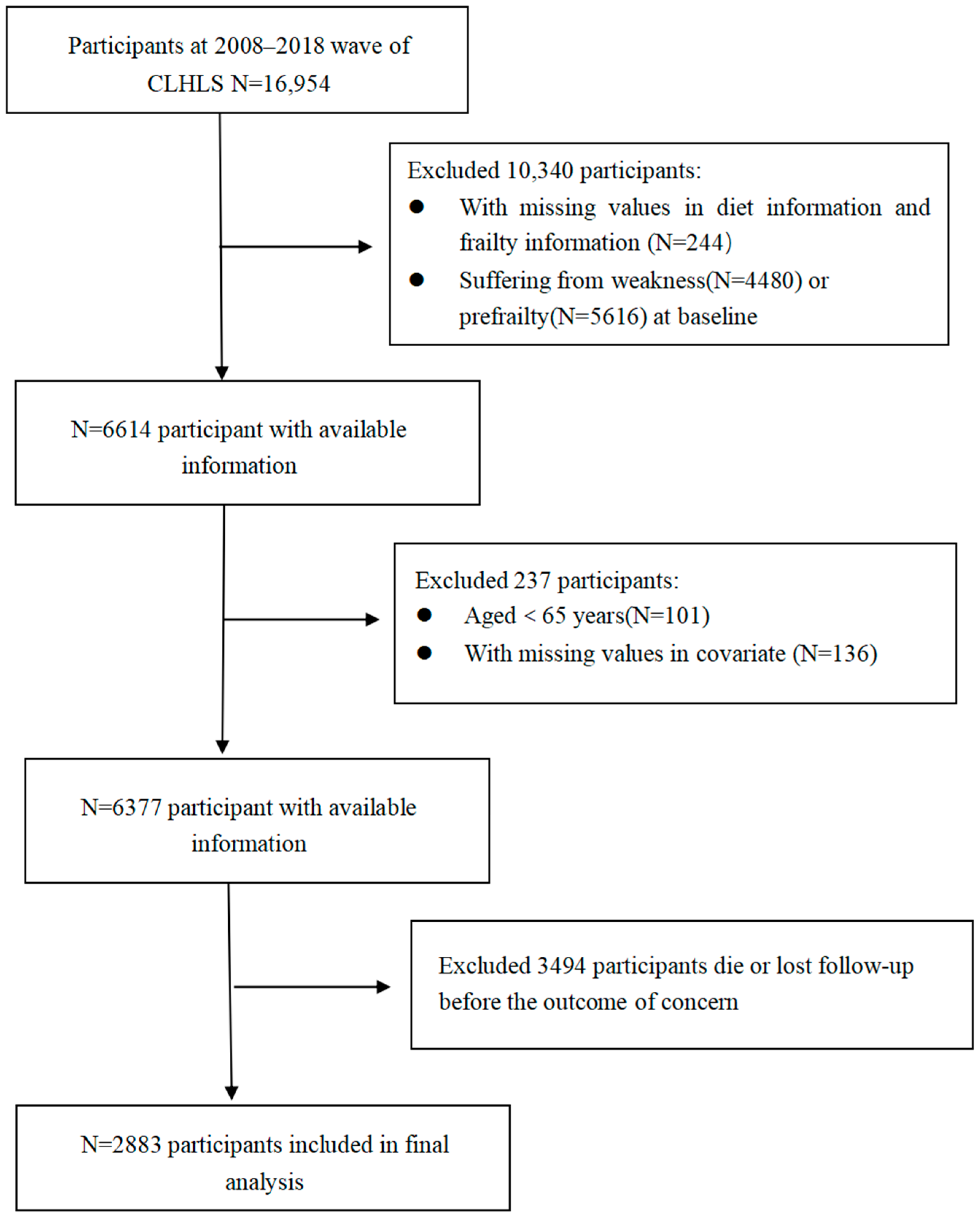
2.1. Study Population
2.2. Calculation of Plant-Based Diet Indices
2.3. Assessment of Frailty
2.4. Assessment of Covariates
2.5. Statistical Analysis
3. Results
3.1. Basic Information
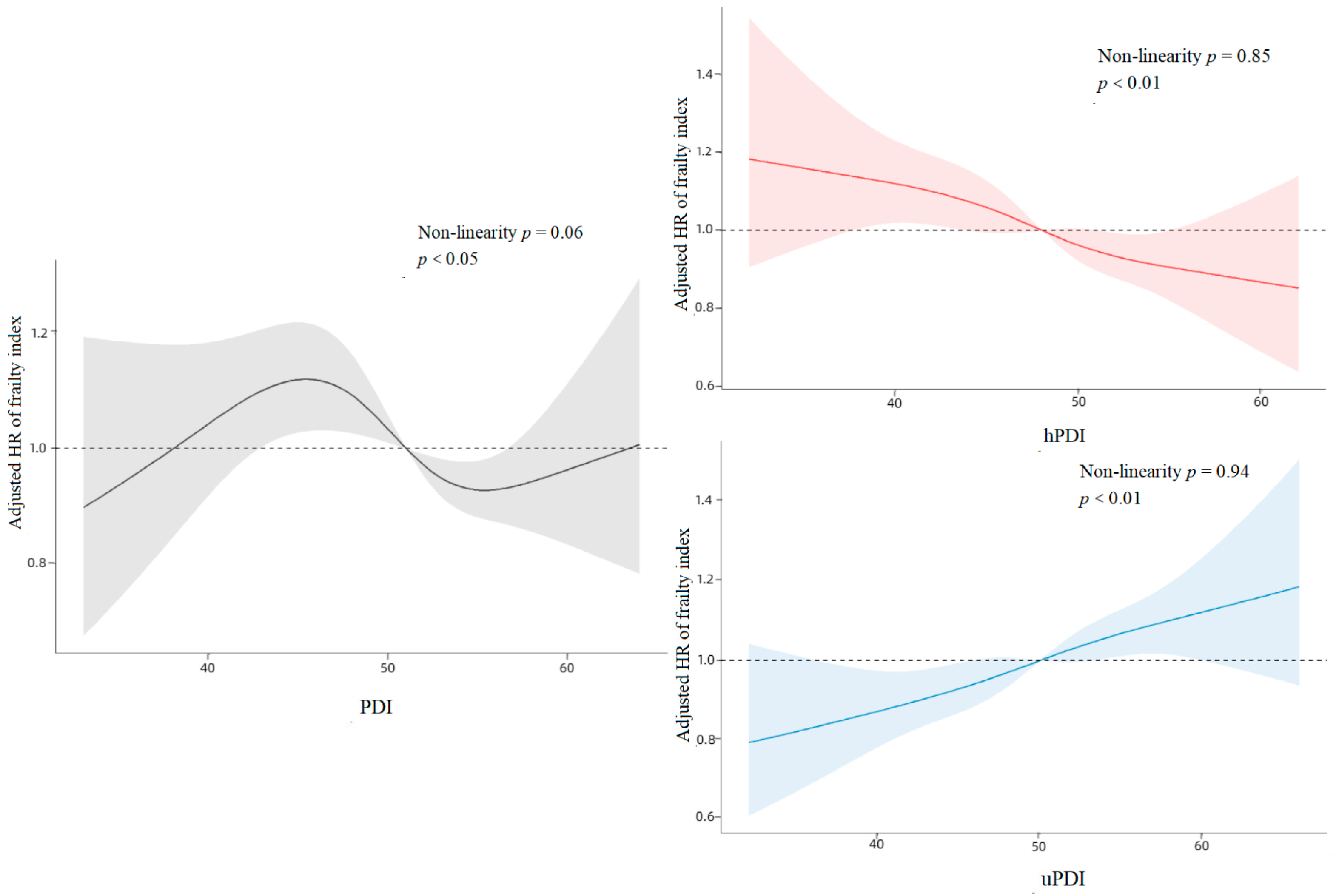
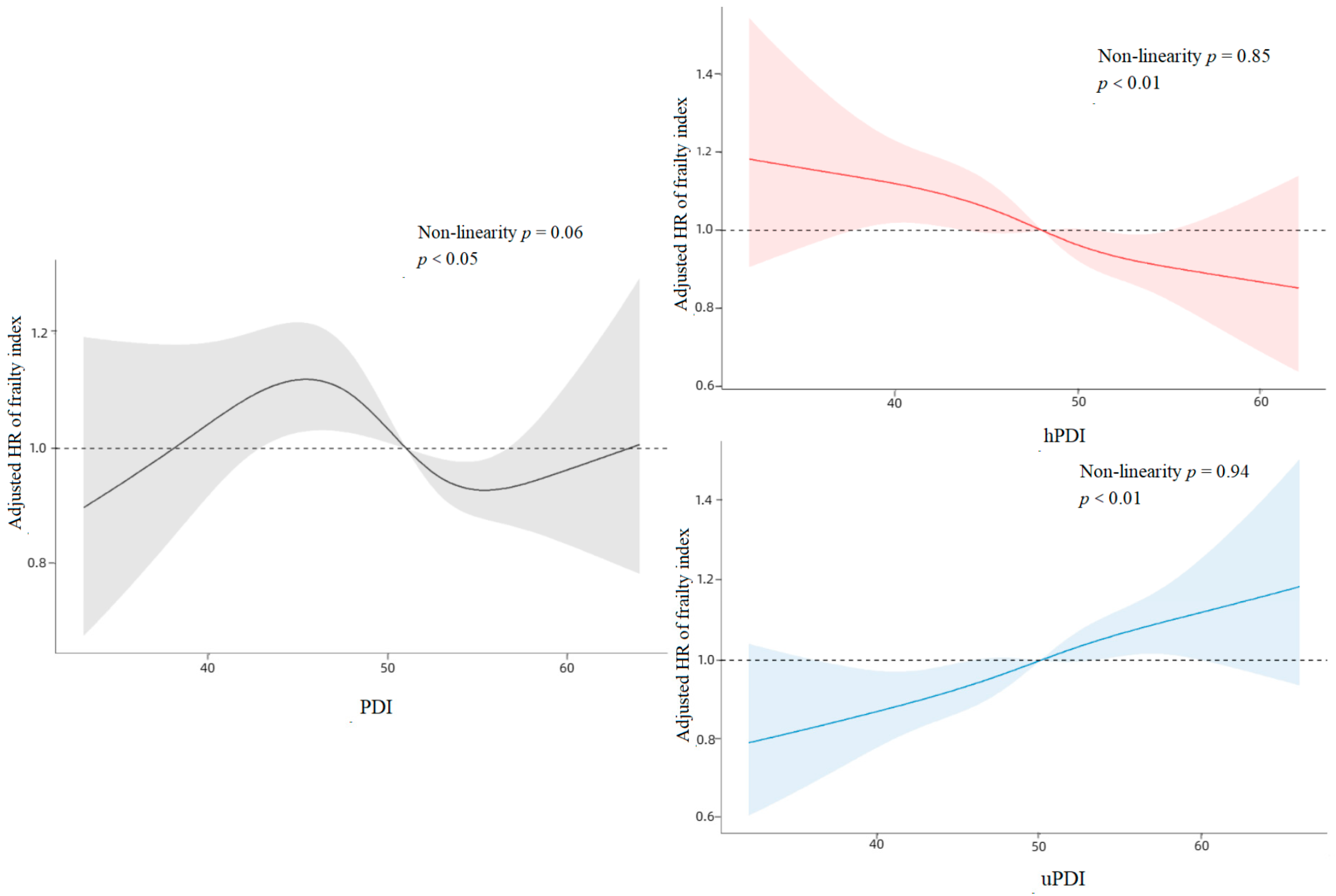
3.2. Association between Baseline Plant-Based Diet Index and Frailty Index
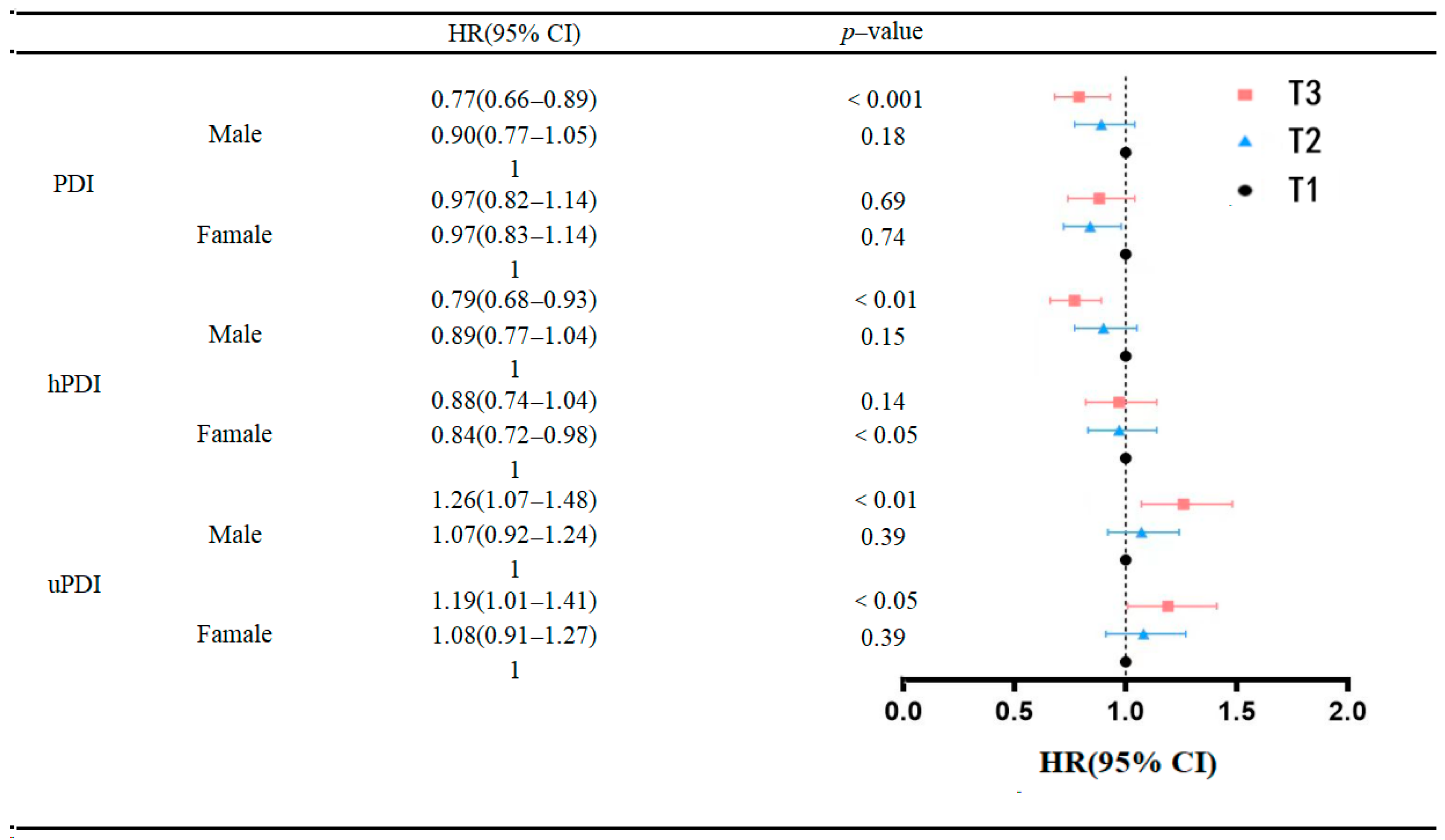
3.3. Gender Differences in the Association between Plant-Based Diet Index and Frailty Index
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in elderly people. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef]
- O’caoimh, R.; Sezgin, D.; O’donovan, M.R.; Molloy, D.W.; Clegg, A.; Rockwood, K.; Liew, A. Prevalence of frailty in 62 countries across the world: A systematic review and meta-analysis of population-level studies. Age Ageing 2021, 50, 96–104. [Google Scholar] [CrossRef]
- Dent, E.; Martin, F.C.; Bergman, H.; Woo, J.; Romero-Ortuno, R.; Walston, J.D. Management of frailty: Opportunities, challenges, and future directions. Lancet 2019, 394, 1376–1386. [Google Scholar] [CrossRef]
- Greco, E.A.; Pietschmann, P.; Migliaccio, S. Osteoporosis and Sarcopenia Increase Frailty Syndrome in the Elderly. Front. Endocrinol. 2019, 10, 255. [Google Scholar] [CrossRef]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the concepts of disability, frailty, and comorbidity: Implications for improved targeting and care. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 255–263. [Google Scholar] [CrossRef]
- Lu, Z.; Er, Y.; Zhan, Y.; Deng, X.; Jin, Y.; Ye, P.; Duan, L. Association of Frailty Status with Risk of Fall among Middle-Aged and Older Adults in China: A Nationally Representative Cohort Study. J. Nutr. Health Aging 2021, 25, 985–992. [Google Scholar] [CrossRef]
- Kojima, G.; Iliffe, S.; Walters, K. Frailty index as a predictor of mortality: A systematic review and meta-analysis. Age Ageing 2018, 47, 193–200. [Google Scholar] [CrossRef]
- Ward, D.D.; Ranson, J.M.; Wallace, L.M.; Llewellyn, D.J.; Rockwood, K. Frailty, lifestyle, genetics and dementia risk. J. Neurol. Neurosurg. Psychiatry 2022, 93, 343–350. [Google Scholar] [CrossRef]
- Hoogendijk, E.O.; Afilalo, J.; Ensrud, K.E.; Kowal, P.; Onder, G.; Fried, L.P. Frailty: Implications for clinical practice and public health. Lancet 2019, 394, 1365–1375. [Google Scholar] [CrossRef]
- Van Assen, M.; Helmink, J.H.M.; Gobbens, R.J.J. Associations between lifestyle factors and multidimensional frailty: A cross-sectional study among community-dwelling older people. BMC Geriatr. 2022, 22, 7. [Google Scholar] [CrossRef]
- Balomenos, V.; Ntanasi, E.; Anastasiou, C.A.; Charisis, S.; Velonakis, G.; Karavasilis, E.; Tsapanou, A.; Yannakoulia, M.; Kosmidis, A.H.; Dardiotis, E.; et al. Association Between Sleep Disturbances and Frailty: Evidence From a Population-Based Study. J. Am. Med. Dir. Assoc. 2021, 22, 551–558.e1. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.; Yan, L.; Wu, C.; Ji, J.S. Residential Greenness and Frailty Among Older Adults: A Longitudinal Cohort in China. J. Am. Med. Dir. Assoc 2020, 21, 759–765.e2. [Google Scholar] [CrossRef] [PubMed]
- Larsen, R.T.; Turcotte, L.A.; Westendorp, R.; Langberg, H.; Hirdes, J.P. Frailty Index Status of Canadian Home Care Clients Improves With Exercise Therapy and Declines in the Presence of Polypharmacy. J. Am. Med. Dir. Assoc. 2020, 21, 766–771.e1. [Google Scholar] [CrossRef] [PubMed]
- Gao, T.; Han, S.; Mo, G.; Sun, Q.; Zhang, M.; Liu, H. Long-term tea consumption reduces the risk of frailty in older Chinese people: Result from a 6-year longitudinal study. Front. Nutr. 2022, 9, 916791. [Google Scholar] [CrossRef] [PubMed]
- Kojima, G.; Taniguchi, Y.; Urano, T. Fruit and Vegetable Consumption and Incident Frailty in Older Adults: A Systematic Review and Meta-Analysis. J. Frailty Aging 2022, 11, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Gao, J.; Jia, Y.; Dai, J.; Fu, H.; Wang, Y.; Yan, H.; Zhu, Y.; Nie, X. Association of Fruit and Vegetable Intake and Frailty among Chinese Elders: A Cross-Sectional Study in Three Cities. J. Nutr. Health Aging 2019, 23, 890–895. [Google Scholar] [CrossRef] [PubMed]
- Struijk, E.A.; Fung, T.T.; Sotos-Prieto, M.; Rodriguez-Artalejo, F.; Willett, W.C.; Hu, F.B.; Lopez-Garcia, E. Red meat consumption and risk of frailty in older women. J. Cachexia Sarcopenia Muscle 2022, 13, 210–219. [Google Scholar] [CrossRef]
- Liang, F.; Fu, J.; Turner-McGrievy, G.; Wang, Y.; Qiu, N.; Ding, K.; Zeng, J.; Moore, J.B.; Li, R. Association of Body Mass Index and Plant-Based Diet with Cognitive Impairment among Older Chinese Adults: A Prospective, Nationwide Cohort Study. Nutrients 2022, 14, 3132. [Google Scholar] [CrossRef]
- Chen, B.; Zeng, J.; Qin, M.; Xu, W.; Zhang, Z.; Li, X.; Xu, S. The Association Between Plant-Based Diet Indices and Obesity and Metabolic Diseases in Chinese Adults: Longitudinal Analyses From the China Health and Nutrition Survey. Front. Nutr. 2022, 9, 881901. [Google Scholar] [CrossRef]
- Chen, Z.; Drouin-Chartier, J.P.; Li, Y.; Baden, M.Y.; Manson, J.E.; Willett, W.C.; Voortman, T.; Hu, H.B.; Bhupathiraju, S.N. Changes in Plant-Based Diet Indices and Subsequent Risk of Type 2 Diabetes in Women and Men: Three U.S. Prospective Cohorts. Diabetes Care 2021, 44, 663–671. [Google Scholar] [CrossRef]
- Dominguez, L.J.; Di Bella, G.; Veronese, N.; Barbagallo, M. Impact of Mediterranean Diet on Chronic Non-Communicable Diseases and Longevity. Nutrients 2021, 13, 2028. [Google Scholar] [CrossRef] [PubMed]
- Rai, S.K.; Fung, T.T.; Lu, N.; Keller, S.F.; Curhan, G.C.; Choi, H.K. The Dietary Approaches to Stop Hypertension (DASH) diet, Western diet, and risk of gout in men: Prospective cohort study. BMJ 2017, 357, j1794. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.; Giovannucci, E. Healthful Plant-Based Diet and Incidence of Type 2 Diabetes in Asian Population. Nutrients 2022, 14, 3078. [Google Scholar] [CrossRef] [PubMed]
- Sotos-Prieto, M.; Struijk, E.A.; Fung, T.T.; Rodríguez-Artalejo, F.; Willett, W.C.; Hu, F.B.; Lopez-Garcia, E. Association between the quality of plant-based diets and risk of frailty. J. Cachexia Sarcopenia Muscle 2022, 13, 2854–2862. [Google Scholar] [CrossRef]
- Maroto-Rodriguez, J.; Delgado-Velandia, M.; Ortolá, R.; Carballo-Casla, A.; García-Esquinas, E.; Rodríguez-Artalejo, F.; Sotos-Prieto, M. Plant-based diets and risk of frailty in community-dwelling older adults: The Seniors-ENRICA-1 cohort. Geroscience 2023, 45, 221–232. [Google Scholar] [CrossRef]
- Duan, Y.; Qi, Q.; Gao, T.; Du, J.; Zhang, M.; Liu, H. Plant-Based Diet and Risk of Frailty in Older Chinese Adults. J. Nutr. Health Aging 2023, 27, 371–377. [Google Scholar] [CrossRef] [PubMed]
- Panza, F.; Lozupone, M.; Solfrizzi, V.; Sardone, R.; Dibello, V.; Di Lena, L.; D’Urso, F.; Stallone, R.; Petruzzi, M.; Giannelli, G.; et al. Different Cognitive Frailty Models and Health- and Cognitive-related Outcomes in Older Age: From Epidemiology to Prevention. J. Alzheimer’s Dis. 2018, 62, 993–1012. [Google Scholar] [CrossRef]
- Bai, W.; Zhang, J.; Smith, R.D.; Cheung, T.; Su, Z.; Ng, C.H.; Zhang, Q.; Xiang, Y.T. Inter-relationship between cognitive performance and depressive symptoms and their association with quality of life in older adults: A network analysis based on the 2017-2018 wave of Chinese Longitudinal Healthy Longevity Survey (CLHLS). J. Affect. Disord. 2023, 320, 621–627. [Google Scholar] [CrossRef]
- Pei, Z.; Zhang, J.; Qin, W.; Hu, F.; Zhao, Y.; Zhang, X.; Cong, X.; Liu, C.; Xu, L. Association between Dietary Patterns and Depression in Chinese Older Adults: A Longitudinal Study Based on CLHLS. Nutrients 2022, 14, 5230. [Google Scholar] [CrossRef]
- Fu, Y.C.; Pei, M.Y.; Liao, J.J.; Li, N.; Zhang, F.C.; Liu, H.L. Prevalence and correlates of elder neglect in the community-dwelling Chinese population: New evidence from the CLHLS study. Front. Public Health 2023, 11, 1123835. [Google Scholar] [CrossRef]
- Chen, H.; Shen, J.; Xuan, J.; Zhu, A.; Ji, J.S.; Liu, X.; Cao, Y.; Zong, G.; Zeng, Y.; Wang, X.; et al. Plant-based dietary patterns in relation to mortality among older adults in China. Nat. Aging 2022, 2, 224–230. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.; Chen, H.; Shen, J.; Wang, X.; Li, Z.; Zhao, A.; Shi, X.; Yan, L.; Zeng, Y.; Yuan, C.; et al. Interaction between plant-based dietary pattern and air pollution on cognitive function: A prospective cohort analysis of Chinese older adults. Lancet Reg. Health West. Pac. 2022, 20, 100372. [Google Scholar] [CrossRef] [PubMed]
- Qi, R.; Sheng, B.; Zhou, L.; Chen, Y.; Sun, L.; Zhang, X. Association of Plant-Based Diet Indices and Abdominal Obesity with Mental Disorders among Older Chinese Adults. Nutrients 2023, 15, 2721. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q.; Tang, B.; Zhai, Y.; Chen, Y.; Jin, Z.; Han, H.; Gao, Y.; Wu, C.; Chen, T.; He, J. Dynamic statistical model for predicting the risk of death among older Chinese people, using longitudinal repeated measures of the frailty index: A prospective cohort study. Age Ageing 2020, 49, 966–973. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; Zhou, Y.; Liu, H.; Shi, M.; Wei, Y.; Xia, Y. Bidirectional Longitudinal Study of Frailty and Depressive Symptoms Among Older Chinese Adults. Front. Aging Neurosci. 2022, 14, 791971. [Google Scholar] [CrossRef] [PubMed]
- Haghighatdoost, F.; Mahdavi, A.; Mohammadifard, N.; Hassannejad, R.; Najafi, F.; Farshidi, H.; Lotfizadeh, M.; Kazemi, T.; Karimi, S.; Roohafza, H.; et al. The relationship between a plant-based diet and mental health: Evidence from a cross-sectional multicentric community trial (LIPOKAP study). PLoS ONE 2023, 18, e0284446. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Gu, Y.; Meng, G.; Wu, H.; Zhang, S.; Wang, X.; Zhang, J.; Huang, T.; Niu, K. Quality of plant-based diet and the risk of dementia and depression among middle-aged and older population. Age Ageing 2023, 52, afad070. [Google Scholar] [CrossRef]
- Satija, A.; Bhupathiraju, S.N.; Rimm, E.B.; Spiegelman, D.; Chiuve, S.E.; Borgi, L.; Willett, W.C.; Manson, J.E.; Sun, Q.; Hu, F.B. Plant-Based Dietary Patterns and Incidence of Type 2 Diabetes in US Men and Women: Results from Three Prospective Cohort Studies. PLoS Med. 2016, 13, e1002039. [Google Scholar] [CrossRef]
- Trautwein, E.A.; Mckay, S. The Role of Specific Components of a Plant-Based Diet in Management of Dyslipidemia and the Impact on Cardiovascular Risk. Nutrients 2020, 12, 2671. [Google Scholar] [CrossRef]
- Coelho-Junior, H.J.; Calvani, R.; Picca, A.; Gonçalves, I.O.; Landi, F.; Bernabei, R.; Cesari, M.; Uchida, M.C.; Marzetti, E. Association between Dietary Habits and Physical Function in Brazilian and Italian Older Women. Nutrients 2020, 12, 1635. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, Q.; Hao, W.; Zhu, D. Long-Term Food Variety and Dietary Patterns Are Associated with Frailty among Chinese Older Adults: A Cohort Study Based on CLHLS from 2014 to 2018. Nutrients 2022, 14, 4279. [Google Scholar] [CrossRef] [PubMed]
- Ygnatios, N.T.M.; Lima-Costa, M.F.; Torres, J.L. Food consumption is associated with frailty in edentulous older adults: Evidence from the ELSI-Brazil study. Cien. Saude Colet. 2023, 28, 1891–1902. [Google Scholar] [CrossRef] [PubMed]
- Sandoval-Insausti, H.; Blanco-Rojo, R.; Graciani, A.; López-García, E.; Moreno-Franco, B.; Laclaustra, M.; Donat-Vargas, C.; Ordovás, J.M.; Rodríguez-Artalejo, F.; Guallar-Castillón, P. Ultra-processed Food Consumption and Incident Frailty: A Prospective Cohort Study of Older Adults. J. Gerontol. A Biol. Sci. Med. Sci. 2020, 75, 1126–1133. [Google Scholar] [CrossRef] [PubMed]
- Soysal, P.; Stubbs, B.; Lucato, P.; Luchini, C.; Solmi, M.; Peluso, R.; Sergi, G.; Isik, A.T.; Manzato, E.; Maggi, S.; et al. Inflammation and frailty in the elderly: A systematic review and meta-analysis. Ageing Res. Rev. 2016, 31, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Jazwinski, S.M. The Gut Microbiota and Healthy Aging: A Mini-Review. Gerontology 2018, 64, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Abbatecola, A.M.; Paolisso, G. Is there a relationship between insulin resistance and frailty syndrome? Curr. Pharm. Des. 2008, 14, 405–410. [Google Scholar] [PubMed]
- Cleasby, M.E.; Jamieson, P.M.; Atherton, P.J. Insulin resistance and sarcopenia: Mechanistic links between common co-morbidities. J. Endocrinol. 2016, 229, R67–R81. [Google Scholar] [CrossRef]
- Soysal, P.; Arik, F.; Smith, L.; Jackson, S.E.; Isik, A.T. Inflammation, Frailty and Cardiovascular Disease. Adv. Exp. Med. Biol. 2020, 1216, 55–64. [Google Scholar]
- Krentz, A.J.; Viljoen, A.; Sinclair, A. Insulin resistance: A risk marker for disease and disability in the older person. Diabet. Med. 2013, 30, 535–548. [Google Scholar] [CrossRef]
- Bao, B.; Prasad, A.S.; Beck, F.W.; Fitzgerald, J.T.; Snell, D.; Bao, G.W.; Singh, T.; Cardozo, L.J. Zinc decreases C-reactive protein, lipid peroxidation, and inflammatory cytokines in elderly subjects: A potential implication of zinc as an atheroprotective agent. Am. J. Clin. Nutr. 2010, 91, 1634–1641. [Google Scholar] [CrossRef]
- Michelon, E.; Blaum, C.; Semba, R.D.; Xue, Q.-L.; Ricks, M.O.; Fried, L.P. Vitamin and carotenoid status in older women: Associations with the frailty syndrome. J. Gerontol. A Biol. Sci. Med. Sci. 2006, 61, 600–607. [Google Scholar] [CrossRef] [PubMed]
- Park, S.-J.; Park, J.; Won, C.W.; Lee, H.-J. The Inverse Association of Sarcopenia and Protein-Source Food and Vegetable Intakes in the Korean Elderly: The Korean Frailty and Aging Cohort Study. Nutrients 2022, 14, 1375. [Google Scholar] [CrossRef] [PubMed]
- Tomata, Y.; Wang, Y.; Hägg, S.; Jylhävä, J. Protein Nutritional Status and Frailty: A Mendelian Randomization Study. J. Nutr. 2022, 152, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Isanejad, M.; Sirola, J.; Rikkonen, T.; Mursu, J.; Kröger, H.; Qazi, S.L.; Tuppurainen, M.; Erkkilä, A.T. Higher protein intake is associated with a lower likelihood of frailty among older women, Kuopio OSTPRE-Fracture Prevention Study. Eur. J. Nutr. 2020, 59, 1181–1189. [Google Scholar] [CrossRef] [PubMed]
- Ley, S.H.; Sun, Q.; Willett, W.C.; Eliassen, A.H.; Wu, K.; Pan, A.; Grodstein, F.; Hu, F.B. Associations between red meat intake and biomarkers of inflammation and glucose metabolism in women. Am. J. Clin. Nutr. 2014, 99, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Würtz, A.M.L.; Jakobsen, M.U.; Bertoia, M.L.; Hou, T.; Schmidt, E.B.; Willett, W.C.; Overvad, K.; Sun, Q.; E Manson, J.; Hu, F.B.; et al. Replacing the consumption of red meat with other major dietary protein sources and risk of type 2 diabetes mellitus: A prospective cohort study. Am. J. Clin. Nutr. 2021, 113, 612–621. [Google Scholar] [CrossRef] [PubMed]
- Gordon, E.H.; Hubbard, R.E. Do sex differences in chronic disease underpin the sex-frailty paradox? Mech. Ageing Dev. 2019, 179, 44–50. [Google Scholar] [CrossRef]
- Reid, N.; Young, A.; Hanjani, L.S.; Hubbard, R.E.; Gordon, E.H. Sex-specific interventions to prevent and manage frailty. Maturitas 2022, 164, 23–30. [Google Scholar] [CrossRef]
- Holsen, L.M.; Huang, G.; Cherkerzian, S.; Aroner, S.; Loucks, E.B.; Buka, S.; Handa, R.J.; Goldstein, J.M. Sex Differences in Hemoglobin A1c Levels Related to the Comorbidity of Obesity and Depression. J. Women’s Health 2021, 30, 1303–1312. [Google Scholar] [CrossRef]
- Bedaso, A.; Adams, J.; Peng, W.; Sibbritt, D. The relationship between social support and mental health problems during pregnancy: A systematic review and meta-analysis. Reprod. Health 2021, 18, 162. [Google Scholar] [CrossRef]
- Cho, H.; Lee, K.; Choi, E.; Cho, H.N.; Park, B.; Suh, M.; Rhee, Y.; Choi, K.S. Association between social support and postpartum depression. Sci. Rep. 2022, 12, 3128. [Google Scholar] [CrossRef] [PubMed]
- Geronikola, N.; Zalonis, I.; Ntanasi, E.; Charisis, S.; Kosmidis, M.H.; Anastasiou, C.A.; Dardiotis, E.; Hadjigeorgiou, G.; Megalou, M.; Velonakis, G.; et al. Sex Differences in Frailty Incidence in Greek Community-Dwelling Older People: The HELIAD Study. J. Frailty Aging 2022, 11, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Park, C.; Ko, F.C. The Science of Frailty: Sex Differences. Clin. Geriatr. Med. 2021, 37, 625–638. [Google Scholar] [CrossRef] [PubMed]
- Wang, P.; Song, M.; Eliassen, A.H.; Wang, M.; Fung, T.T.; Clinton, S.K.; Rimm, E.B.; Hu, F.B.; Willett, W.C.; Tabung, F.K.; et al. Optimal dietary patterns for prevention of chronic disease. Nat. Med. 2023, 29, 719–728. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Characteristics | N(%) | PDI | p-Value | hPDI | p-Value | uPDI | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| T1 | T2 | T3 | T1 | T2 | T3 | T1 | T2 | T3 | |||||
| Age (years) | 2883 (100) | 82 (11) | 81 (11) | 79 (10) | <0.001 | 83 (11) | 80 (11) | 80 (10) | <0.001 | 80 (11) | 81 (11) | 82 (11) | <0.001 |
| Sex | <0.05 | <0.001 | <0.001 | ||||||||||
| Male | 1552 (53.8) | 562 (36.2) | 469 (30.2) | 521 (33.6) | 479 (30.9) | 567 (37.1) | 497 (32.0) | 622 (40.1) | 525 (33.8) | 405 (26.1) | |||
| Female | 1331 (46.2) | 506 (38.0) | 439 (33.0) | 386 (29.0) | 486 (36.5) | 508 (38.2) | 337 (25.3) | 403 (30.3) | 497 (37.3) | 431 (32.4) | |||
| Resdic | <0.01 | 0.09 | <0.001 | ||||||||||
| Urban | 361 (12.5) | 122 (33.8) | 142 (39.3) | 97 (26.9) | 103 (28.5) | 142 (39.3) | 116 (32.1) | 235 (65.1) | 78 (21.6) | 48 (13.3) | |||
| Town | 2522 (87.5) | 946 (37.5) | 766 (30.4) | 810 (32.1) | 862 (34.2) | 942 (37.4) | 718 (28.5) | 790 (31.3) | 944 (37.4) | 788 (31.2) | |||
| Economic situation | 0.23 | 0.31 | <0.001 | ||||||||||
| Wealthy | 483 (16.8) | 189 (39.1) | 158 (32.7) | 136 (28.2) | 162 (33.5) | 169 (35.0) | 152 (31.5) | 257 (53.2) | 145 (30.0) | 81 (16.8) | |||
| Not wealthy | 2400 (83.2) | 879 (36.6) | 750 (31.2) | 771 (32.1) | 803 (33.5) | 915 (38.1) | 682 (28.4) | 768 (32.0) | 877 (36.5) | 755 (31.5) | |||
| Cohabitation status | 0.15 | 0.62 | <0.001 | ||||||||||
| Solitude | 544 (18.9) | 220 (40.4) | 168 (30.9) | 156 (28.7) | 190 (34.9) | 205 (37.7) | 149 (27.4) | 140 (25.7) | 189 (34.7) | 215 (39.5) | |||
| Not living alone | 2339 (81.1) | 848 (36.3) | 740 (31.6) | 751 (32.1) | 775 (33.1) | 879 (37.6) | 685 (29.3) | 885 (37.8) | 833 (35.6) | 621 (26.5) | |||
| Marital status | <0.001 | <0.001 | <0.001 | ||||||||||
| Married/cohabitating | 1306 (45.3) | 415 (31.8) | 400 (30.6) | 491 (37.6) | 363 (27.8) | 508 (38.9) | 435 (33.3) | 539 (41.3) | 451 (34.5) | 316 (24.2) | |||
| Others | 1577 (54.7) | 653 (41.4) | 508 (32.2) | 416 (26.4) | 602 (38.2) | 576 (36.5) | 399 (25.3) | 486 (30.8) | 571 (36.2) | 520 (33.0) | |||
| Smoking status | <0.01 | <0.01 | <0.01 | ||||||||||
| never | 1718 (59.6) | 675 (39.3) | 542 (31.5) | 501 (29.2) | 613 (35.7) | 630 (36.7) | 475 (27.6) | 576 (33.5) | 608 (35.4) | 534 (31.1) | |||
| former | 429 (14.9) | 153 (35.7) | 134 (31.2) | 142 (33.1) | 132 (30.8) | 180 (42.0) | 117 (27.3) | 177 (71.3) | 151 (35.2) | 101 (23.5) | |||
| now | 736 (25.5) | 240 (32.6) | 232 (31.5) | 264 (35.9) | 220 (29.9) | 274 (37.2) | 242 (32.9) | 272 (37.0) | 263 (35.7) | 201 (27.3) | |||
| Alcohol consumption | 0.53 | 0.12 | <0.001 | ||||||||||
| never | 1813 (62.9) | 687 (37.9) | 573 (31.6) | 553 (30.5) | 619 (34.1) | 694 (38.3) | 500 (27.6) | 598 (33.0) | 646 (35.6) | 569 (31.4) | |||
| former | 357 (12.4) | 124 (34.7) | 118 (33.1) | 115 (32.2) | 126 (35.3) | 118 (33.1) | 113 (31.7) | 134 (37.5) | 122 (34.2) | 101 (28.3) | |||
| now | 713 (24.7) | 257 (36.0) | 217 (30.4) | 239 (33.5) | 220 (30.9) | 272 (38.1) | 221 (31.0) | 293 (41.1) | 254 (35.6) | 166 (23.3) | |||
| Physical exercise | 0.18 | 0.09 | <0.001 | ||||||||||
| never | 1611 (55.9) | 622 (38.6) | 494 (30.7) | 495 (30.7) | 569 (35.3) | 602 (37.4) | 440 (27.3) | 470 (29.2) | 618 (38.4) | 523 (32.5) | |||
| former | 255 (8.8) | 97 (38.0) | 73 (28.6) | 85 (33.3) | 73 (28.6) | 99 (38.8) | 83 (32.5) | 90 (35.3) | 92 (36.1) | 73 (28.6) | |||
| now | 1017 (35.3) | 349 (34.3) | 341 (333.5) | 327 (32.2) | 323 (31.8) | 383 (37.7) | 311 (30.6) | 465 (45.7) | 312 (30.7) | 240 (23.6) | |||
| BMI (kg/m2) | <0.001 | <0.001 | |||||||||||
| low | 696 (24.1) | 317 (45.5) | 214 (30.7) | 165 (23.7) | 283 (40.7) | 238 (34.2) | 175 (25.1) | 212 (30.5) | 258 (37.1) | 226 (32.5) | <0.001 | ||
| nomal | 1749 (60.7) | 619 (35.4) | 549 (31.4) | 581 (33.2) | 575 (32.9) | 664 (38.0) | 510 (29.2) | 610 (34.9) | 624 (35.7) | 515 (29.4) | |||
| overweight | 355 (12.3) | 112 (31.5) | 116 (32.7) | 127 (35.8) | 89 (25.1) | 146 (41.1) | 120 (33.8) | 157 (44.2) | 120 (33.8) | 78 (22.0) | |||
| Obesity | 83 (2.9) | 20 (24.1) | 29 (34.9) | 34 (41.0) | 18 (21.7) | 36 (43.4) | 29 (34.9) | 46 (55.4) | 20 (24.1) | 17 (20.5) | |||
| T1 | T2 | T3 | |||
|---|---|---|---|---|---|
| HR (95% CI) | p-Value | HR (95% CI) | p-Value | ||
| PDI | |||||
| Model 1 | 1 | 0.93 (0.84–1.04) | 0.21 | 0.85 (0.77–0.95) | <0.01 |
| Model 2 | 1 | 0.93 (0.83–1.04) | 0.19 | 0.86 (0.77–0.95) | <0.01 |
| hPDI | |||||
| Model 1 | 1 | 0.87 (0.79–0.97) | <0.05 | 0.82 (0.73–0.92) | <0.001 |
| Model 2 | 1 | 0.87 (0.79–0.97) | <0.05 | 0.83 (0.74–0.93) | <0.001 |
| uPDI | |||||
| Model 1 | 1 | 1.07 (0.96–1.19) | 0.21 | 1.23 (1.10–1.38) | <0.001 |
| Model 2 | 1 | 1.05 (0.94–1.18) | 0.37 | 1.21 (1.08–1.36) | <0.01 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qi, R.; Yang, Y.; Sheng, B.; Li, H.; Zhang, X. Plant-Based Diet Indices and Their Association with Frailty in Older Adults: A CLHLS-Based Cohort Study. Nutrients 2023, 15, 5120. https://doi.org/10.3390/nu15245120
Qi R, Yang Y, Sheng B, Li H, Zhang X. Plant-Based Diet Indices and Their Association with Frailty in Older Adults: A CLHLS-Based Cohort Study. Nutrients. 2023; 15(24):5120. https://doi.org/10.3390/nu15245120
Chicago/Turabian StyleQi, Ran, Yun Yang, Baihe Sheng, Huiping Li, and Xinyu Zhang. 2023. "Plant-Based Diet Indices and Their Association with Frailty in Older Adults: A CLHLS-Based Cohort Study" Nutrients 15, no. 24: 5120. https://doi.org/10.3390/nu15245120
APA StyleQi, R., Yang, Y., Sheng, B., Li, H., & Zhang, X. (2023). Plant-Based Diet Indices and Their Association with Frailty in Older Adults: A CLHLS-Based Cohort Study. Nutrients, 15(24), 5120. https://doi.org/10.3390/nu15245120