
The Effects of ESC/ESH-Based Written Generic Lifestyle Advice and a Nutraceutical on 24-Hour Blood Pressure in Patients with High–Normal Office Blood Pressure and Low–Moderate Cardiovascular Risk

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Clinical Parameters
2.3. Blood Pressure Measurements
2.4. Lifestyle Advice, Nutraceutical, and Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics of the Study Population
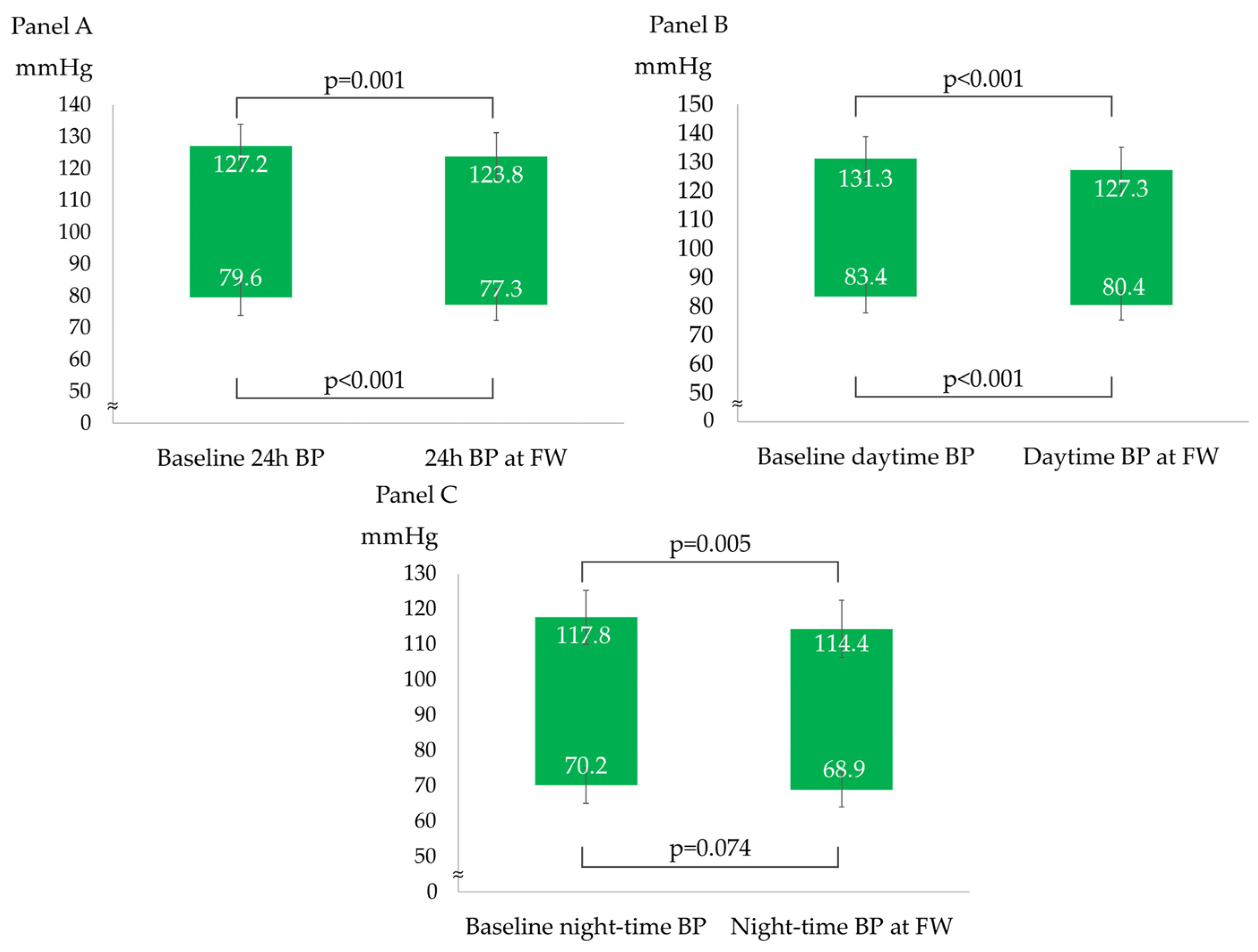
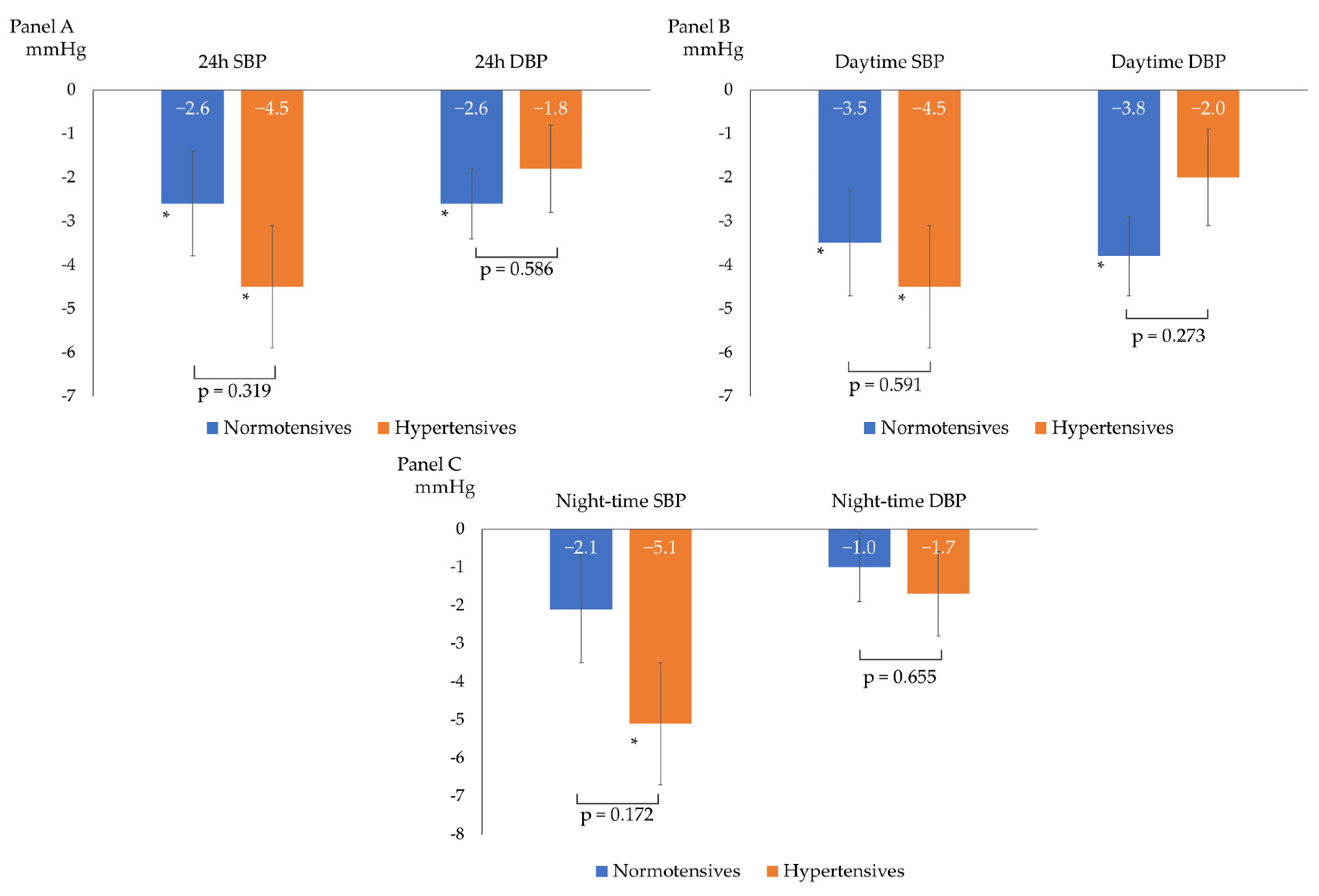
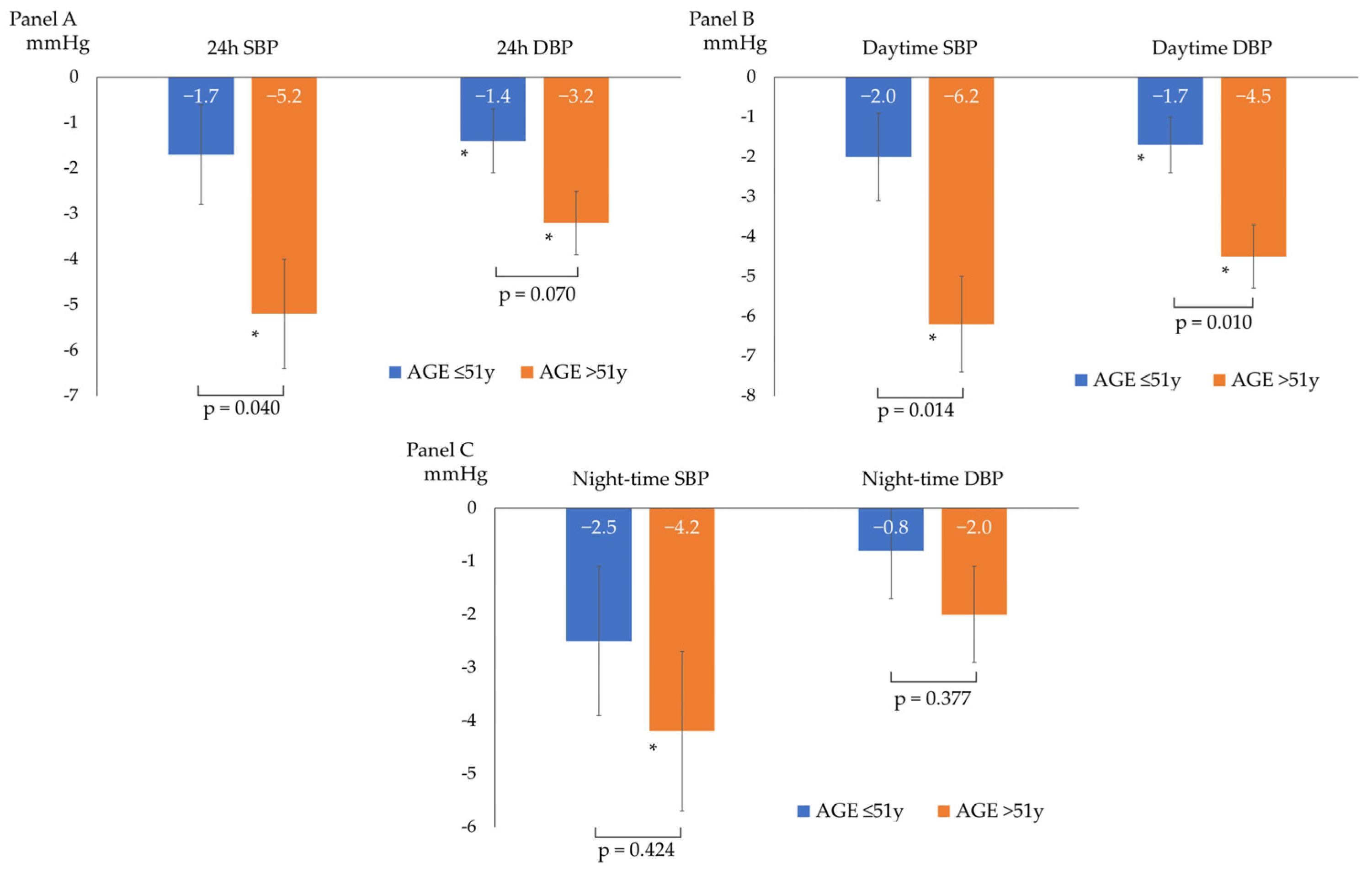
3.2. Changes in ABPM at Follow-Up
4. Discussion
Study Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mancia, G.; Brunström, M.; Burnier, M.; Grassi, G.; Januszewicz, A.; Muiesan, M.L.; Tsioufis, K.; Agabiti-Rosei, E.; Algharably, E.A.E.; Azizi, M.; et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension Endorsed by the European Renal Association (ERA) and the International Society of Hypertension (ISH). J. Hypertens. 2023, 41, 1874–2071. [Google Scholar] [PubMed]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; De Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Liu, Y.; Zhang, L.; Zhou, L.; Li, D.; Quan, H.; Zhu, L.; Hu, F.; Li, X.; Meng, S.; et al. Nonpharmacologic Interventions for Reducing Blood Pressure in Adults with Prehypertension to Established Hypertension. J. Am. Heart Assoc. 2020, 9, e016804. [Google Scholar] [CrossRef] [PubMed]
- Pazoki, R.; Dehghan, A.; Evangelou, E.; Warren, H.; Gao, H.; Caulfield, M.; Elliott, P.; Tzoulaki, I. Genetic Predisposition to High Blood Pressure and Lifestyle Factors: Associations with Midlife Blood Pressure Levels and Cardiovascular Events. Circulation 2018, 137, 653–661. [Google Scholar] [CrossRef] [PubMed]
- Dhakal, A.; KC, T.; Neupane, M. Adherence to lifestyle modifications and its associated factors in hypertensive patients. J. Clin. Nurs. 2022, 31, 2181–2188. [Google Scholar] [CrossRef] [PubMed]
- Aronson, J.K. Defining ‘nutraceuticals’: Neither nutritious nor pharmaceutical. Br. J. Clin. Pharmacol. 2017, 83, 8–19. [Google Scholar] [CrossRef] [PubMed]
- Penson, P.E.; Banach, M. Natural compounds as anti-atherogenic agents: Clinical evidence for improved cardiovascular outcomes. Atherosclerosis 2021, 316, 58–65. [Google Scholar] [CrossRef]
- Borghi, C.; Tsioufis, K.; Agabiti-Rosei, E.; Burnier, M.; Cicero, A.F.G.; Clement, D.; Coca, A.; Desideri, G.; Grassi, G.; Lovic, D.; et al. Nutraceuticals and blood pressure control: A European Society of Hypertension position document. J. Hypertens. 2020, 38, 799–812. [Google Scholar] [CrossRef]
- Catapano, A.L.; Barrios, V.; Cicero, A.F.; Pirro, M. Lifestyle interventions and nutraceuticals: Guideline-based approach to cardiovascular disease prevention. Atheroscler. Suppl. 2019, 39, 100003. [Google Scholar] [CrossRef]
- Siervo, M.; Lara, J.; Ogbonmwan, I.; Mathers, J.C. Inorganic nitrate and beetroot juice supplementation reduces blood pressure in adults: A systematic review and meta-analysis. J. Nutr. 2013, 143, 818–826. [Google Scholar] [CrossRef]
- Beirne, A.M.; Mitchelmore, O.; Palma, S.; Andiapen, M.; Rathod, K.S.; Hammond, V.; Bellin, A.; Cooper, J.; Wright, P.; Antoniou, S.; et al. NITRATE-CIN Study: Protocol of a Randomized (1:1) Single-Center, U.K. Double-Blind Placebo-Controlled Trial Testing the Effect of Inorganic Nitrate on Contrast-Induced Nephropathy in Patients Undergoing Coronary Angiography for Acute Coronary Syndromes. J. Cardiovasc. Pharmacol. Ther. 2021, 26, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Coles, L.T.; Clifton, P.M. Effect of beetroot juice on lowering blood pressure in free-living, disease-free adults: A randomized, placebo-controlled trial. Nutr. J. 2012, 11, 106. [Google Scholar] [CrossRef] [PubMed]
- Gilchrist, M.; Winyard, P.G.; Aizawa, K.; Anning, C.; Shore, A.; Benjamin, N. Effect of dietary nitrate on blood pressure, endothelial function, and insulin sensitivity in type 2 diabetes. Free Radic. Biol. Med. 2013, 60, 89–97. [Google Scholar] [CrossRef] [PubMed]
- Hobbs, D.A.; Kaffa, N.; George, T.W.; Methven, L.; Lovegrove, J.A. Blood pressure-lowering effects of beetroot juice and novel beetroot-enriched bread products in normotensive male subjects. Br. J. Nutr. 2012, 108, 2066–2074. [Google Scholar] [CrossRef] [PubMed]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Landolfo, M.; Allevi, M.; Spannella, F.; Giulietti, F.; Gezzi, A.; Sarzani, R. Cardiovascular Risk Assessment and Control in Outpatients Evaluated by 24-hour Ambulatory Blood Pressure and Different LDL-C Equations. High. Blood Press. Cardiovasc. Prev. 2023, 30, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Giulietti, F.; Filipponi, A.; Rosettani, G.; Giordano, P.; Iacoacci, C.; Spannella, F.; Sarzani, R. Pharmacological Approach to Smoking Cessation: An Updated Review for Daily Clinical Practice. High. Blood Press. Cardiovasc. Prev. 2020, 27, 349–362. [Google Scholar] [CrossRef] [PubMed]
- Martin, S.S.; Blaha, M.J.; Elshazly, M.B.; Toth, P.P.; Kwiterovich, P.O.; Blumenthal, R.S.; Jones, S.R. Comparison of a novel method vs. the Friedewald equation for estimating low-density lipoprotein cholesterol levels from the standard lipid profile. JAMA 2013, 310, 2061–2068. [Google Scholar] [CrossRef]
- Spannella, F.; Giulietti, F.; Fedecostante, M.; Ricci, M.; Balietti, P.; Cocci, G.; Landi, L.; Bonfigli, A.R.; Boemi, M.; Espinosa, E.; et al. Interarm blood pressure differences predict target organ damage in type 2 diabetes. J. Clin. Hypertens. 2017, 19, 472–478. [Google Scholar] [CrossRef]
- Omboni, S.; Palatini, P.; Parati, G. Standards for ambulatory blood pressure monitoring clinical reporting in daily practice: Recommendations from the Italian Society of Hypertension. Blood Press. Monit. 2015, 20, 241–244. [Google Scholar] [CrossRef]
- Egan, B.M.; Stevens-Fabry, S. Prehypertension—prevalence, health risks, and management strategies. Nat. Rev. Cardiol. 2015, 12, 289–300. [Google Scholar] [CrossRef] [PubMed]
- Vasan, R.S.; Larson, M.G.; Leip, E.P.; Evans, J.C.; O’Donnell, C.J.; Kannel, W.B.; Levy, D. Impact of high-normal blood pressure on the risk of cardiovascular disease. N. Engl. J. Med. 2001, 345, 1291–1297. [Google Scholar] [CrossRef] [PubMed]
- Cuspidi, C.; Sala, C.; Tadic, M.; Gherbesi, E.; Facchetti, R.; Grassi, G.; Mancia, G. High-normal blood pressure and abnormal left ventricular geometric patterns: A meta-analysis. J. Hypertens. 2019, 37, 1312–1319. [Google Scholar] [CrossRef] [PubMed]
- Nicoll, R.; Henein, M.Y. Hypertension and lifestyle modification: How useful are the guidelines? Br. J. Gen. Pract. 2010, 60, 879–880. [Google Scholar] [CrossRef]
- Filippou, C.D.; Thomopoulos, C.G.; Kouremeti, M.M.; Sotiropoulou, L.I.; Nihoyannopoulos, P.I.; Tousoulis, D.M.; Tsioufis, C.P. Mediterranean diet and blood pressure reduction in adults with and without hypertension: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. 2021, 40, 3191–3200. [Google Scholar] [CrossRef] [PubMed]
- Kapil, V.; Khambata, R.S.; Robertson, A.; Caulfield, M.J.; Ahluwalia, A. Dietary nitrate provides sustained blood pressure lowering in hypertensive patients: A randomized, phase 2, double-blind, placebo-controlled study. Hypertension 2015, 65, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Webb, A.J.; Patel, N.; Loukogeorgakis, S.; Okorie, M.; Aboud, Z.; Misra, S.; Rashid, R.; Miall, P.; Deanfield, J.; Benjamin, N.; et al. Acute blood pressure lowering, vasoprotective, and antiplatelet properties of dietary nitrate via bioconversion to nitrite. Hypertension 2008, 51, 784–790. [Google Scholar] [CrossRef]
- Hobbs, D.A.; Goulding, M.G.; Nguyen, A.; Malaver, T.; Walker, C.F.; George, T.W.; Methven, L.; Lovegrove, J.A. Acute ingestion of beetroot bread increases endothelium-independent vasodilation and lowers diastolic blood pressure in healthy men: A randomized controlled trial. J. Nutr. 2013, 143, 1399–1405. [Google Scholar] [CrossRef]
- Penson, P.E.; Mancini, G.B.J.; Toth, P.P.; Martin, S.S.; Watts, G.F.; Sahebkar, A.; Mikhailidis, D.P.; Banach, M.; Lipid and Blood Pressure Meta-Analysis Collaboration (LBPMC) Group & International Lipid Expert Panel (ILEP). Introducing the ‘Drucebo’ effect in statin therapy: A systematic review of studies comparing reported rates of statin-associated muscle symptoms, under blinded and open-label conditions. J. Cachexia Sarcopenia Muscle 2018, 9, 1023–1033. [Google Scholar] [CrossRef]
- Galletti, F.; Agabiti-Rosei, E.; Bernini, G.; Boero, R.; Desideri, G.; Fallo, F.; Mallamaci, F.; Morganti, A.; Castellano, M.; Nazzaro, P.; et al. Excess dietary sodium and inadequate potassium intake by hypertensive patients in Italy: Results of the MINISAL-SIIA study program. J. Hypertens. 2014, 32, 48–56. [Google Scholar] [CrossRef]
- Gupta, D.K.; Lewis, C.E.; Varady, K.A.; Su, Y.R.; Madhur, M.S.; Lackland, D.T.; Reis, J.P.; Wang, T.J.; Lloyd-Jones, D.M.; Allen, N.B. Effect of Dietary Sodium on Blood Pressure: A Crossover Trial. JAMA 2023, e2323651. [Google Scholar] [CrossRef] [PubMed]
- Hansen, D.; Abreu, A.; Ambrosetti, M.; Cornelissen, V.; Gevaert, A.; Kemps, H.; Laukkanen, J.A.; Pedretti, R.; Simonenko, M.; Wilhelm, M.; et al. Exercise intensity assessment and prescription in cardiovascular rehabilitation and beyond: Why and how: A position statement from the Secondary Prevention and Rehabilitation Section of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2022, 29, 230–245. [Google Scholar] [CrossRef] [PubMed]
- Panayotov, V.S. Studying a Possible Placebo Effect of an Imaginary Low-Calorie Diet. Front. Psychiatry. 2019, 10, 550. [Google Scholar] [CrossRef] [PubMed]
- Dickinson, S.L.; Foote, G.; Allison, D.B. Commentary: Studying a Possible Placebo Effect of an Imaginary Low-Calorie Diet. Front. Psychiatry. 2020, 11, 329. [Google Scholar] [CrossRef] [PubMed]
- Virdis, A.; Giannarelli, C.; Neves, M.F.; Taddei, S.; Ghiadoni, L. Cigarette smoking and hypertension. Curr. Pharm. Des. 2010, 16, 2518–2525. [Google Scholar] [CrossRef] [PubMed]
- Tawa, M.; Nakagawa, K.; Ohkita, M. Effects of beetroot juice supplementation on vascular functional and structural changes in aged mice. Physiol. Rep. 2023, 11, e15755. [Google Scholar] [CrossRef] [PubMed]
- De Jongh, R.T.; Serné, E.H.; IJzerman, R.G.; de Vries, G.; Stehouwer, C.D. Impaired microvascular function in obesity: Implications for obesity-associated microangiopathy, hypertension, and insulin resistance. Circulation 2004, 109, 2529–2535. [Google Scholar] [CrossRef] [PubMed]
- Van der Avoort, C.M.T.; Ten Haaf, D.S.M.; Bongers, C.; van Oorschot, F.; Verdijk, L.B.; van Loon, L.J.C.; Hopman, M.T. Increasing Nitrate-Rich Vegetable Intake Lowers Ambulatory Blood Pressure in (pre)Hypertensive Middle-Aged and Older Adults: A 12-Wk Randomized Controlled Trial. J. Nutr. 2021, 151, 2667–2679. [Google Scholar] [CrossRef]
- Cicero, A.F.; Derosa, G.; Parini, A.; Baronio, C.; Borghi, C. Factors associated with 2-year persistence in fully non reimbursed lipid-lowering treatments. Atherosclerosis 2014, 235, 81–83. [Google Scholar] [CrossRef]
- Balietti, P.; Spannella, F.; Giulietti, F.; Rosettani, G.; Bernardi, B.; Cocci, G.; Bonfigli, A.R.; Sarzani, R. Ten-year changes in ambulatory blood pressure: The prognostic value of ambulatory pulse pressure. J. Clin. Hypertens. 2018, 20, 1230–1237. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| All Population (n° 43) | Normotensives at ABPM 1 (n° 25) | Hypertensives at ABPM 1 (n° 18) | p (Normotensives vs. Hypertensives) | |
|---|---|---|---|---|
| Age (years) | 49.9 ± 10.8 | 50.4 ± 10.7 | 49.2 ± 11.0 | 0.726 |
| Sex (male) | 23 (53.5%) | 13 (52.0%) | 10 (55.6%) | 0.818 |
| BMI 2 (kg/m2) | 25.1 ± 3.2 | 25.0 ± 3.0 | 25.4 ± 43.5 | 0.708 |
| Weight (kg) | 73.0 ± 11.4 | 72.6 ± 11.2 | 73.5 ± 11.9 | 0.802 |
| Office SBP 3 (mmHg) | 135.4 ± 3.9 | 135.3 ± 2.6 | 135.6 ± 3.5 | 0.829 |
| Office DBP 4 (mmHg) | 85.1 ± 3.1 | 84.7 ± 2.9 | 85.9 ± 3.7 | 0.356 |
| 24 h SBP 3 (mmHg) | 127.2 ± 6.8 | 124.8 ± 5.6 | 130.6 ± 7.0 | 0.005 |
| 24 h DBP 4 (mmHg) | 79.6 ± 5.6 | 76.2 ± 3.3 | 84.3 ± 4.5 | <0.001 |
| Daytime SBP 3 (mmHg) | 131.3 ± 7.5 | 128.9 ± 6.7 | 134.5 ± 7.5 | 0.015 |
| Daytime DBP 4 (mmHg) | 83.4 ± 5.5 | 80.1 ± 3.3 | 88.0 ± 4.7 | <0.001 |
| Night-time SBP 3 (mmHg) | 117.8 ± 7.7 | 116.1 ± 6.2 | 120.1 ± 9.1 | 0.091 |
| Night-time DBP 4 (mmHg) | 70.2 ± 5.0 | 68.0 ± 2.9 | 73.2 ± 5.6 | 0.002 |
| Glucose (mmol/L) | 5.11 ± 0.50 | 5.24 ± 0.46 | 4.93 ± 0.53 | 0.104 |
| Creatinine (µmol/L) | 77.4 ± 16.7 | 73.0 ± 14.1 | 83.6 ± 18.5 | 0.063 |
| eGFR 5 (mL/min/1.73 m2) | 94.9 ± 13.0 | 97.6 ± 11.6 | 90.9 ± 14.3 | 0.139 |
| TC 6 (mmol/L) | 5.15 ± 0.39 | 5.30 ± 0.35 | 4.92 ± 0.33 | 0.004 |
| HDL-C 7 (mmol/L) | 1.53 ± 0.31 | 1.54 ± 0.37 | 1.52 ± 0.26 | 0.856 |
| LDL-C 8 (mmol/L) | 3.13 ± 0.47 | 3.24 ± 0.48 | 2.96 ± 0.39 | 0.088 |
| TG 9 (mmol/L) | 0.99 (0.84–1.21) | 1.08 (0.90–1.35) | 0.92 (0.77–1.08) | 0.111 |
| ABPM 1 (mmHg) | Sex | Baseline BMI 2 (kg/m2) | Smoking Status | |||
|---|---|---|---|---|---|---|
| Male (n° 23) | Female (n° 20) | <25 (n° 18) | ≥25 (n° 25) | No (n° 29) | Yes (n° 14) | |
| 24 h SBP 3 | −3.5 ± 1.2 * | −3.2 ± 1.3 * | −3.9 ± 1.3 * | −3.0 ± 1.1 * | −4.0 ± 1.0 * | −2.1 ± 1.5 |
| p for interaction 0.873 | p for interaction 0.635 | p for interaction 0.311 | ||||
| 24 h DBP 4 | −2.2 ± 0.7 * | −2.2 ± 0.7 * | −2.2 ± 0.8 * | −2.2 ± 0.7 * | −2.6 ± 0.6 * | −1.5 ± 0.9 |
| p for interaction 0.991 | p for interaction 0.997 | p for interaction 0.312 | ||||
| Daytime SBP | −4.1 ± 1.2 * | −3.8 ± 1.3 * | −4.2 ± 1.4 * | −3.7 ± 1.2 * | −4.7 ± 1.0 * | −2.4 ± 1.5 |
| p for interaction 0.862 | p for interaction 0.798 | p for interaction 0.229 | ||||
| Daytime DBP | −3.0 ± 0.8 * | −3.1 ± 0.8 * | −3.1 ± 0.9 * | −3.0 ± 0.7 * | −3.6 ± 0.7 * | −1.9 ± 1.0 |
| p for interaction 0.909 | p for interaction 0.900 | p for interaction 0.151 | ||||
| Night-time SBP | −3.4 ± 1.4 * | −3.3 ± 1.5 * | −4.0 ± 1.6 * | −2.8 ± 1.4 * | −3.9 ± 1.3 * | −2.2 ± 1.8 |
| p for interaction 0.965 | p for interaction 0.595 | p for interaction 0.447 | ||||
| Night-time DBP | −1.1 ± 0.9 | −1.5 ± 1.0 | −1.3 ± 1.0 | −1.3 ± 0.8 | −1.4 ± 0.8 | −1.1 ± 1.1 |
| p for interaction 0.772 | p for interaction 0.981 | p for interaction 0.808 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Landolfo, M.; Spannella, F.; Poliseno, C.; Massacesi, A.; Giulietti, F.; Festa, R.; Cavazzin, E.; Sasso, G.; Mazza, A.; Sarzani, R. The Effects of ESC/ESH-Based Written Generic Lifestyle Advice and a Nutraceutical on 24-Hour Blood Pressure in Patients with High–Normal Office Blood Pressure and Low–Moderate Cardiovascular Risk. Nutrients 2023, 15, 5099. https://doi.org/10.3390/nu15245099
Landolfo M, Spannella F, Poliseno C, Massacesi A, Giulietti F, Festa R, Cavazzin E, Sasso G, Mazza A, Sarzani R. The Effects of ESC/ESH-Based Written Generic Lifestyle Advice and a Nutraceutical on 24-Hour Blood Pressure in Patients with High–Normal Office Blood Pressure and Low–Moderate Cardiovascular Risk. Nutrients. 2023; 15(24):5099. https://doi.org/10.3390/nu15245099
Chicago/Turabian StyleLandolfo, Matteo, Francesco Spannella, Chiara Poliseno, Adriano Massacesi, Federico Giulietti, Roberto Festa, Enrico Cavazzin, Giulio Sasso, Alberto Mazza, and Riccardo Sarzani. 2023. "The Effects of ESC/ESH-Based Written Generic Lifestyle Advice and a Nutraceutical on 24-Hour Blood Pressure in Patients with High–Normal Office Blood Pressure and Low–Moderate Cardiovascular Risk" Nutrients 15, no. 24: 5099. https://doi.org/10.3390/nu15245099
APA StyleLandolfo, M., Spannella, F., Poliseno, C., Massacesi, A., Giulietti, F., Festa, R., Cavazzin, E., Sasso, G., Mazza, A., & Sarzani, R. (2023). The Effects of ESC/ESH-Based Written Generic Lifestyle Advice and a Nutraceutical on 24-Hour Blood Pressure in Patients with High–Normal Office Blood Pressure and Low–Moderate Cardiovascular Risk. Nutrients, 15(24), 5099. https://doi.org/10.3390/nu15245099