
Dietary Intake Is Not Associated with Body Composition nor with Biochemical Tests but with Psychological Status of Cancer Patients Receiving Chemotherapy
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
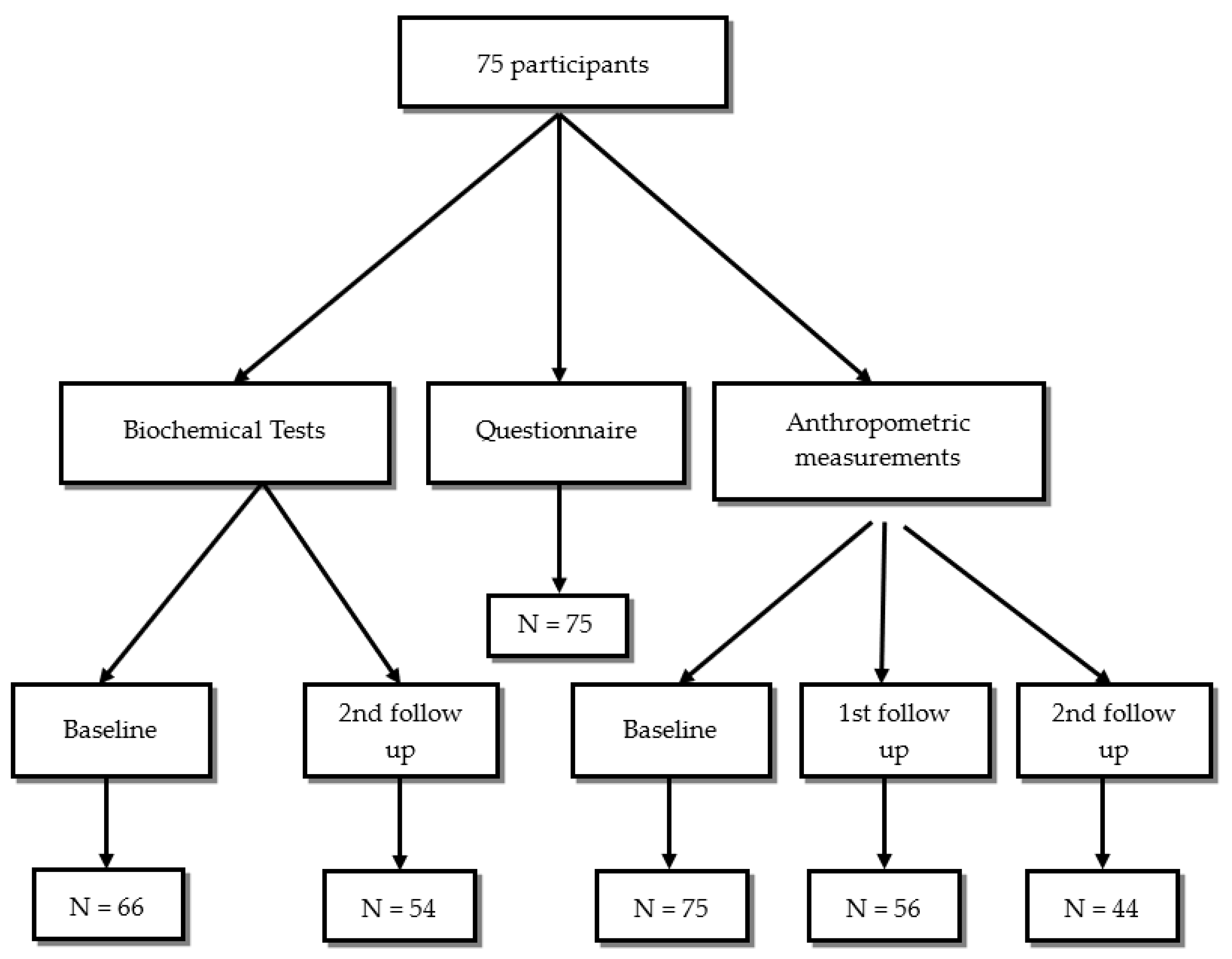
2.1. Study Design, Participants, and Questionnaire
2.2. Psychological Status
2.3. Quality of Life Assessment
2.4. Anthropometric Measurements
2.5. Dietary Intake
2.6. Biochemical Analysis
2.7. Statistical Analyses
3. Results
3.1. Socio-Demographic, Cancer Types, and Cancer-Related Characteristics
3.2. Anthropometric Measurements before the First Cycle of Chemotherapy and after the Third Cycle
3.3. Correlation between Adequate and Inadequate Dietary Intake with Psychological Status, Quality of Life, Anthropometric Measurements, and Biochemical Tests
3.4. Dietary Intake (Macro- and Micronutrients) of Study Sample Compared to Recommended Dietary Intake for Cancer Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Torre, L.A.; Bray, F.; Siegel, R.L.; Ferlay, J.; Lortet-Tieulent, J.; Jemal, A. Global Cancer Statistics, 2012. CA J. Clin. 2015, 65, 87–108. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Global Cancer statistics, 2022. CA J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of incidence and mortality worldwide for 36 Cancers in 185 Countries. CA J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Faller, H.; Schuler, M.; Richard, M.; Heckl, U.; Weis, J.; Küffner, R. Effects of psycho-oncologic interventions on emotional distress and quality of life in adult patients with cancer: Systematic review and meta-Analysis. J. Clin. Oncol. 2013, 31, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, M.G.; Rutten, H.; Rasmussen-Conrad, E.L.; Knuijt, S.; Takes, R.P.; van Herpen, C.M.; Wanten, G.J.; Kaanders, J.H.; Merkx, M.A. Nutritional status, food intake, and dysphagia in long-term survivors with head and neck cancer treated with chemoradiotherapy: A cross-sectional study. Head Neck 2014, 36, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Tomasetti, C.; Li, L.; Vogelstein, B. Stem cell divisions, somatic mutations, cancer etiology, and cancer prevention. Science 2017, 355, 1330–1334. [Google Scholar] [CrossRef]
- Public health round-up. Bull. World Health Organ. 2017, 95, 612–613. [CrossRef]
- Balstad, T.R.; Solheim, T.S.; Strasser, F.; Kaasa, S.; Bye, A. Dietary treatment of weight loss in patients with advanced cancer and cachexia: A systematic literature review. Crit. Rev. Oncol. Hematol. 2014, 91, 210–221. [Google Scholar] [CrossRef]
- Maschke, J.; Kruk, U.; Kastrati, K.; Kleeberg, J.; Buchholz, D.; Erickson, N.; Huebner, J. Nutritional care of cancer patients: A survey on patients’ needs and medical care in reality. Int. J. Clin. Oncol. 2016, 22, 200–206. [Google Scholar] [CrossRef]
- Kwak, M.; Zebrack, B.; Meeske, K.; Embry, L.; Aguilar, C.; Block, R.; Hayes-Lattin, B.; Li, Y.; Butler, M.; Cole, S. Trajectories of psychological distress in adolescent and young adult patients with cancer: A 1-year longitudinal study. J. Clin. Oncol. 2013, 31, 2160–2166. [Google Scholar] [CrossRef]
- Cheville, A.L.; Rhudy, L.; Basford, J.R.; Griffin, J.M.; Flores, A.M. How receptive are patients with late stage cancer to rehabilitation services and what are the sources of their resistance. Arch. Phys. Med. Rehabil. 2017, 98, 203–210. [Google Scholar] [CrossRef] [PubMed]
- Muscaritoli, M.; Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin. Nutr. 2021, 40, 2898–2913. [Google Scholar] [CrossRef] [PubMed]
- Marceca, G.P.; Londhe, P.; Calore, F. Management of cancer cachexia: Attempting to develop new pharmacological agents for new effective therapeutic options. Front. Oncol. 2020, 10, 298. [Google Scholar] [CrossRef]
- van der Meij, B.S.; Teleni, L.; McCarthy, A.L.; Isenring, E.A. Cancer cachexia: An overview of diagnostic criteria and therapeutic approaches for the accredited practicing dietitian. J. Hum. Nutr. Diet. 2020, 34, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Efendioglu, E.M.; Cigiloglu, A.; Turkbeyler, I.H. Malnutrition and depressive symptoms in elderly palliative care patients. J. Palliat. Care 2021, 37, 503–509. [Google Scholar] [CrossRef]
- Stanga, Z.; Field, J.; Iff, S.; Stucki, A.; Lobo, D.N.; Allison, S.P. The effect of nutritional management on the mood of malnourished patients. Clin. Nutr. 2007, 26, 379–382. [Google Scholar] [CrossRef]
- Available online: https://www.svri.org/sites/default/files/attachments/2016-01-13/HADS.pdf (accessed on 8 August 2023).
- Available online: https://qol.eortc.org/questionnaire/eortc-qlq-c30/ (accessed on 8 August 2023).
- Parsa, N. Environmental factors inducing human cancers. Iran. J. Public Health 2012, 41, 1–9. [Google Scholar]
- Ravasco, P. Nutrition in cancer patients. J. Clin. Med. 2019, 8, 1211. [Google Scholar] [CrossRef]
- IBM. SPSS Version 22; IBM: Armonk, NY, USA, 2013. [Google Scholar]
- Nho, J.H.; Kim, S.R.; Kwon, Y.S. Depression and appetite: Predictors of malnutrition in gynecologic cancer. Support. Care Cancer 2014, 22, 3081–3088. [Google Scholar] [CrossRef]
- Langius, J.A.E.; Bakker, S.; Rietveld, D.H.F.; Kruizenga, H.M.; Langendijk, J.A.; Weijs, P.J.; Leemans, C.R. Critical weight loss is a major prognostic indicator for disease-specific survival in patients with head and neck cancer receiving radiotherapy. Br. J. Cancer 2013, 109, 1093–1099. [Google Scholar] [CrossRef]
- Clevenger, L.; Schrepf, A.; Degeest, K.; Bender, D.; Goodheart, M.; Ahmed, A.; Dahmoush, L.; Penedo, F.; Lucci, J., 3rd; Thaker, P.H.; et al. Sleep disturbance, distress, and quality of life in ovarian cancer patients during the first year after diagnosis. Cancer 2013, 119, 3234–3241. [Google Scholar] [CrossRef] [PubMed]
- Nikbakhsh, N.; Moudi, S.; Abbasian, S.; Khafri, S. Prevalence of depression and anxiety among cancer patients. Caspian. J. Intern. Med. 2014, 5, 167–170. [Google Scholar] [PubMed]
- Rieke, K.; Schmid, K.; Lydiatt, W.; Houfek, J.; Boilesen, E.; Watanabe-Galloway, S. Depression and survival in head and neck cancer patients. Oral Oncol. 2017, 65, 76–82. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Poulin, P.; Feldstain, A.; Chasen, M. The association between malnutrition and psychological distress in patients with advanced head-and-neck cancer. Curr. Oncol. 2013, 20, 554. [Google Scholar] [CrossRef] [PubMed]
- Kiss, N.K.; Krishnasamy, M.; Isenring, E.A. The effect of mutrition intervention in lung cancer patients undergoing chemotherapy and/or radiotherapy: A Systematic Review. Nutr. Cancer 2013, 66, 47–56. [Google Scholar] [CrossRef] [PubMed]
- Vergara, N.; Montoya, J.E.; Luna, H.G.; Amparo, J.R.; Cristal-Luna, G. Quality of life and nutritional status among cancer patients on chemotherapy. Oman Med. J. 2013, 28, 270–274. [Google Scholar] [CrossRef] [PubMed]
- Mardas, M.; Jamka, M.; Mądry, R.; Walkowiak, J.; Krótkopad, M.; Stelmach-Mardas, M. Dietary habits changes and quality of life in patients undergoing chemotherapy for epithelial ovarian cancer. Support. Care Cancer 2014, 23, 1015–1023. [Google Scholar] [CrossRef]
- Solheim, T.S.; Blum, D.; Fayers, P.M.; Hjermstad, M.J.; Stene, G.B.; Strasser, F.; Kaasa, S. Weight loss, appetite loss and food intake in cancer patients with cancer cachexia: Three peas in a pod?—Analysis from a multicenter cross sectional study. Acta Oncol. 2013, 53, 539–546. [Google Scholar] [CrossRef]
- Stene, G.B.; Helbostad, J.L.; Amundsen, T.; Sørhaug, S.; Hjelde, H.; Kaasa, S.; Grønberg, B.H. Changes in skeletal muscle mass during palliative chemotherapy in patients with advanced lung cancer. Acta Oncol. 2014, 54, 340–348. [Google Scholar] [CrossRef]
- Malihi, Z.; Kandiah, M.; Chan, Y.; Esfandbod, M.; Vakili, M.; Hosseinzadeh, M.; Zarif Yeganeh, M. The effect of dietary intake changes on nutritional status in acute leukaemia patients after first induction chemotherapy. Eur. J. Cancer Care 2014, 24, 542–552. [Google Scholar] [CrossRef]

{kind=link}
| Initial Mean (SD) | Final Mean (SD) | p-Value | |
|---|---|---|---|
| Weight (kg) | 76.8 (18.2) | 66.8 (13.9) | 0.00 |
| Height (cm) | 163.2 (8.2) | 163.2 (8.2) | ND * |
| Muscles mass (kg) | 26.7 (6.7) | 23.4 (5.7) | 0.00 |
| Fat mass (kg) | 28.2 (11.8) | 23.2 (8.2) | 0.00 |
| Minerals (kg) | 3.4 (0.7) | 3.0 (0.7) | 0.00 |
| Body water (L) | 35.7 (8.1) | 32.1 (7.3) | 0.00 |
| Waist/hip ratio | 0.9 (0.1) | 0.9 (0.1) | 0.48 |
| Fat% | 36.1 (9.0) | 32.7 (9.2) | 0.01 |
| BMI ** (kg/m2) | 28.9 (6.5) | 25.2 (4.8) | 0.00 |
| Basel metabolic rate (kcal) | 1419.7 (238.8) | 1293.3 (217.9) | 0.00 |
| Protein (kg) | 9.5 (2.2) | 8.5 (2.0) | 0.00 |
| Visceral fat (level) | 12.7 (4.6) | 10.4 (4.4) | 0.00 |
| Variables | Dietary Intake | p-Value | |
|---|---|---|---|
| Inadequate n (%) | Adequate n (%) | ||
| Psychological status | |||
| Depression | 0.00 | ||
| Normal | 3 (5.4) | 7 (36.8) | |
| Borderline abnormal | 23 (41) | 7(36.8) | |
| Abnormal | 30 (53.6) | 5 (26.3) | |
| Anxiety | 0.25 | ||
| Normal | 8 (14.3) | 4 (21.1) | |
| Borderline abnormal | 15 (26.8) | 8 (42.1) | |
| Abnormal | 33 (58.9) | 7 (36.8) | |
| Quality of life | |||
| Healthcare scale | 0.00 | ||
| Bad | 44 (78.6) | 8 (42.1) | |
| Good | 12 (21.4) | 11 (57.9) | |
| Functional scale | 0.01 | ||
| Bad | 13 (68.4) | 20 (35.7) | |
| Good | 6 (31.6) | 36 (64.3) | |
| Symptom’s scale | 0.64 | ||
| Bad | 21 (37.5) | 6 (31.6) | |
| Good | 35 (62.5) | 13 (68.4) | |
| Anthropometric measurements and body composition (Mean ± SD) | |||
| Fat (%) | 32.6 ± 9.9 | 32.6 ± 7.5 | 0.74 |
| Waist/hip ratio | 0.9 ± 0.1 | 0.9 ± 0.1 | 0.66 |
| BMI (kg/m2) | 25.5 ± 5.3 | 24.6 ± 3.6 | 0.23 |
| Body water (L) | 32.3 ± 7.6 | 31.7 ± 6.6 | 0.81 |
| Minerals (kg) | 2.9 ± 0.7 | 3 ± 0.5 | 0.93 |
| Fat mass (kg) | 23.4 ± 8.5 | 22.9 ± 7.6 | 0.46 |
| Muscle mass (kg) | 23.4 ± 5.8 | 23.4 ± 5.4 | 0.64 |
| Biochemical Tests | Dietary Intake | p-Value | |||
|---|---|---|---|---|---|
| Inadequate | Adequate | ||||
| Median | Range | Median | Range | ||
| WBC | 5.7 | 0.1–36.5 | 6.2 | 1.3–11.4 | 0.83 |
| RBC | 4.12 | 1.09–5.29 | 3.9 | 3.3–5.89 | 0.86 |
| MCV | 86.3 | 73.8–97.6 | 81.2 | 35.8–99.8 | 0.42 |
| MCH | 29.1 | 24.2–33.6 | 30 | 15.5–33.1 | 0.81 |
| MCHC | 34 | 32.4–36 | 33.8 | 30.5–35.2 | 0.18 |
| RDW | 16.8 | 12.2–22.6 | 18.4 | 13.7–27.2 | 0.11 |
| Platelet count | 271 | 20–566 | 248 | 129–455 | 0.91 |
| MPV | 8.5 | 4.8–11.4 | 8.8 | 7.9–17.5 | 0.16 |
| Lymphocyte | 23.8 | 3.2–54.3 | 26.6 | 8.5–48.7 | 0.98 |
| Monocytes | 9.7 | 0.9–41.8 | 9.3 | 1.5–42.4 | 0.97 |
| Eosinophile | 1.3 | 0–9 | 0.4 | 0–6.9 | 0.25 |
| Basophile | 0.7 | 0–1.5 | 0.7 | 0.2–1.4 | 0.82 |
| HB | 12 | 7–15.9 | 11.2 | 8.1–15.1 | 0.17 |
| Neutrophils | 62.4 | 19–95 | 64.5 | 5–87 | 0.86 |
| PCV | 35.9 | 21–44.3 | 33.9 | 26.7–46.3 | 0.26 |
| Serum creatinine level | 0.61 | 0.1–1.34 | 0.6 | 0.44–1.04 | 0.37 |
| Sodium serum level | 140 | 133–143 | 140 | 136–142 | 0.79 |
| Potassium | 4.56 | 3.74–5.52 | 4.4 | 3.63–5.2 | 0.51 |
| Chloride serum level | 101.7 | 91.7–106.4 | 101.4 | 94.7–103.7 | 0.79 |
| Uric acid serum | 4.78 | 1.6–7.7 | 4.46 | 3.25–6.48 | 0.30 |
| Albumin serum level | 4.3 | 2.56–5 | 4.355 | 3.64–5.13 | 0.44 |
| Bilirubin serum level | 0.32 | 0.15–1.41 | 0.465 | 0.18–24 | 0.10 |
| Alkaline phosphatase | 83 | 40–924 | 68 | 50–94 | 0.08 |
| AST | 18.8 | 0–129 | 17.4 | 0–43 | 0.57 |
| ALT | 16.8 | 0–109 | 13 | 0–47 | 0.78 |
| Bilirubin direct | 0.11 | 0–0.37 | 0.135 | 0–0.27 | 0.57 |
| Total protein serum | 6.74 | 0–8.6 | 6.85 | 0–7.64 | 0.94 |
| Urea serum level | 21 | 0–48 | 17.5 | 0–38 | 0.55 |
| Mean ± SD | RDA * | p-Value | |
|---|---|---|---|
| Calories (kcal) | 1452 ± 1061.1 | 30 kcal/kg/day | 0.00 |
| Protein (g) | 57 ± 52.0 | 2 g/kg | 0.00 |
| Carbohydrate (g) | 173 ± 127.2 | 100 g/day | 0.00 |
| Fiber (g) | 15 ± 21.1 | 30 g/day | 0.00 |
| Fat (g) | 61 ± 66.2 | 55 g/day | 0.40 |
| Saturated fat % | 7 ± 3.5 | 7 | 0.09 |
| Unsaturated fat% | 12 ± 10.8 | 15 | 0.02 |
| Omega 3 and omega 6 (g) | 8 ± 26.7 | 250 mg | 0.01 |
| Protein % | 17 ± 7.1 | 30 | 0.00 |
| Carbohydrate % | 49 ± 12.8 | 45 | 0.00 |
| Fat % | 34 ± 13.9 | 25 | 0.00 |
| Vitamins and Minerals | Mean ± SD | Recommended Dietary Allowance * | p-Value |
|---|---|---|---|
| Vitamin B1 (mg) | 0.5 ± 0.4 | 1.5 | 0.00 |
| Vitamin B2 (mg) | 0.6 ± 0.5 | 1.7 | 0.00 |
| Vitamin A (IU) | 3059.1 ± 3194.1 | 40,000 | 0.00 |
| Vitamin B12 (mcg) | 1.1 ± 2.7 | 6 | 0.00 |
| Folate (mcg) | 134.0 ± 123.7 | 400 | 0.00 |
| Vitamin E (mg) | 2.8 ± 5.3 | 15 | 0.00 |
| Vitamin D (IU) | 30.2 ± 52.1 | 400 | 0.00 |
| Vitamin B3 (mg) | 7.1 ± 6.0 | 20 | 0.00 |
| Vitamin B6 (mg) | 0.5 ± 0.4 | 100 | 0.00 |
| Vitamin C (mg) | 33.2 ± 25.7 | 2000 | 0.00 |
| Sodium (mg) | 3426.5 ± 3400.8 | 1500 | 0.00 |
| Magnesium (mg) | 77.9 ± 52.4 | 370 | 0.00 |
| Selenium (mcg) | 18.3 ± 18.8 | 55 | 0.00 |
| Zinc (mg) | 2.8 ± 2.4 | 90 | 0.00 |
| Iron(mg) | 9.1 ± 9.5 | 11 | 0.09 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Subih, H.S.; Al-Shwaiyat, E.A.; Al-Bayyari, N.; Obeidat, B.S.; Abu-Farsakh, F.; Bawadi, H. Dietary Intake Is Not Associated with Body Composition nor with Biochemical Tests but with Psychological Status of Cancer Patients Receiving Chemotherapy. Nutrients 2023, 15, 5087. https://doi.org/10.3390/nu15245087
Subih HS, Al-Shwaiyat EA, Al-Bayyari N, Obeidat BS, Abu-Farsakh F, Bawadi H. Dietary Intake Is Not Associated with Body Composition nor with Biochemical Tests but with Psychological Status of Cancer Patients Receiving Chemotherapy. Nutrients. 2023; 15(24):5087. https://doi.org/10.3390/nu15245087
Chicago/Turabian StyleSubih, Hadil S., Esraa A. Al-Shwaiyat, Nahla Al-Bayyari, Belal S. Obeidat, Fadi Abu-Farsakh, and Hiba Bawadi. 2023. "Dietary Intake Is Not Associated with Body Composition nor with Biochemical Tests but with Psychological Status of Cancer Patients Receiving Chemotherapy" Nutrients 15, no. 24: 5087. https://doi.org/10.3390/nu15245087
APA StyleSubih, H. S., Al-Shwaiyat, E. A., Al-Bayyari, N., Obeidat, B. S., Abu-Farsakh, F., & Bawadi, H. (2023). Dietary Intake Is Not Associated with Body Composition nor with Biochemical Tests but with Psychological Status of Cancer Patients Receiving Chemotherapy. Nutrients, 15(24), 5087. https://doi.org/10.3390/nu15245087