
Development and Functionality of a Parsimonious Digital Food Frequency Questionnaire for a Clinical Intervention among an Indigenous Population


Abstract
1. Introduction
2. Materials and Methods
2.1. FFQ Development
2.1.1. Construction of an Appropriate Food List
- Step 1: Access to population-specific dietary intake data. The Australian National Aboriginal and Torres Strait Islander Nutrition and Physical Activity Survey (NATSINPAS) was identified as the primary candidate for population-specific dietary data to inform the development of the FFQ. It included a representative sample of 2300 non-remote and 1800 remote Aboriginal and Torres Strait Islander participants aged ≥ 2 years from 2900 households (one adult and one child per household). The survey was conducted by the Australian Bureau of Statistics (ABS) in 2012–2013 and had a 79% response rate. The ABS published a detailed description of the sampling framework and data collection methodology [28].The NATSINPAS dietary intake data were collected in person by trained interviewers using the US Department of Agriculture’s (USDA’s) Automated Multiple-Pass Method 24HR questionnaire [36,37], adapted to reflect the Australian food supply [38]. A second 24HR was collected by phone in a subsample of volunteer participants. We used the basic Confidentialized Unit Record Files (CURF) data for non-remote participants aged ≥ 18 years (n = 1170) to guide the development of the FFQ food list for the Kaat Koort study. Only data from the first 24HR were used in these analyses because the second 24HR was completed by a self-selected subsample of participants and there is no published information about the response rate or representativeness of this subsample [29].
- Step 2: Data classification. In the ABS dataset, all the foods reported in the 24HR data were classified into major, sub-major and minor food groups, based on the US National Health and Nutrition Examination Survey (NHANES) classification system [39]. For the purposes of creating the FFQ, the >1550 food and beverage items reported on the 24HRs were classified into 205 food groups (Supplemental File S1—Table S1).
- Step 3: Data analysis. These food groups were entered into a stepwise multiple regression model according to their specific nutrient content and their intake quantity from the 24HR [40]. This procedure was conducted for energy and selected nutrients that either determine energy intake or have been associated with cardiovascular health (protein, fat, carbohydrates, fiber, sodium, potassium and magnesium) [41]. To ensure an adequately comprehensive FFQ food list, food groups that accounted for at least 80% of the total intake of these nutrients were considered for inclusion in the FFQ food list. To simultaneously maximize the capacity of the FFQ to rank participants according to nutrient intake levels, the food groups that explained at least 80% of the between-person variability for each of the nutrients of interest were also identified and considered for inclusion in the FFQ. To ensure participants were not overburdened, we aimed to develop a list of less than 100 food and beverage items to be assessed among all participants. Additional items reported by NATSINPAS participants were retained in the food database. They were assigned to the appropriate food group and included in the digital I-ACE FFQ platform as “Extra items” that could be selected and added to the FFQ during the assessment process by participants who consumed them.
2.1.2. Refining the List
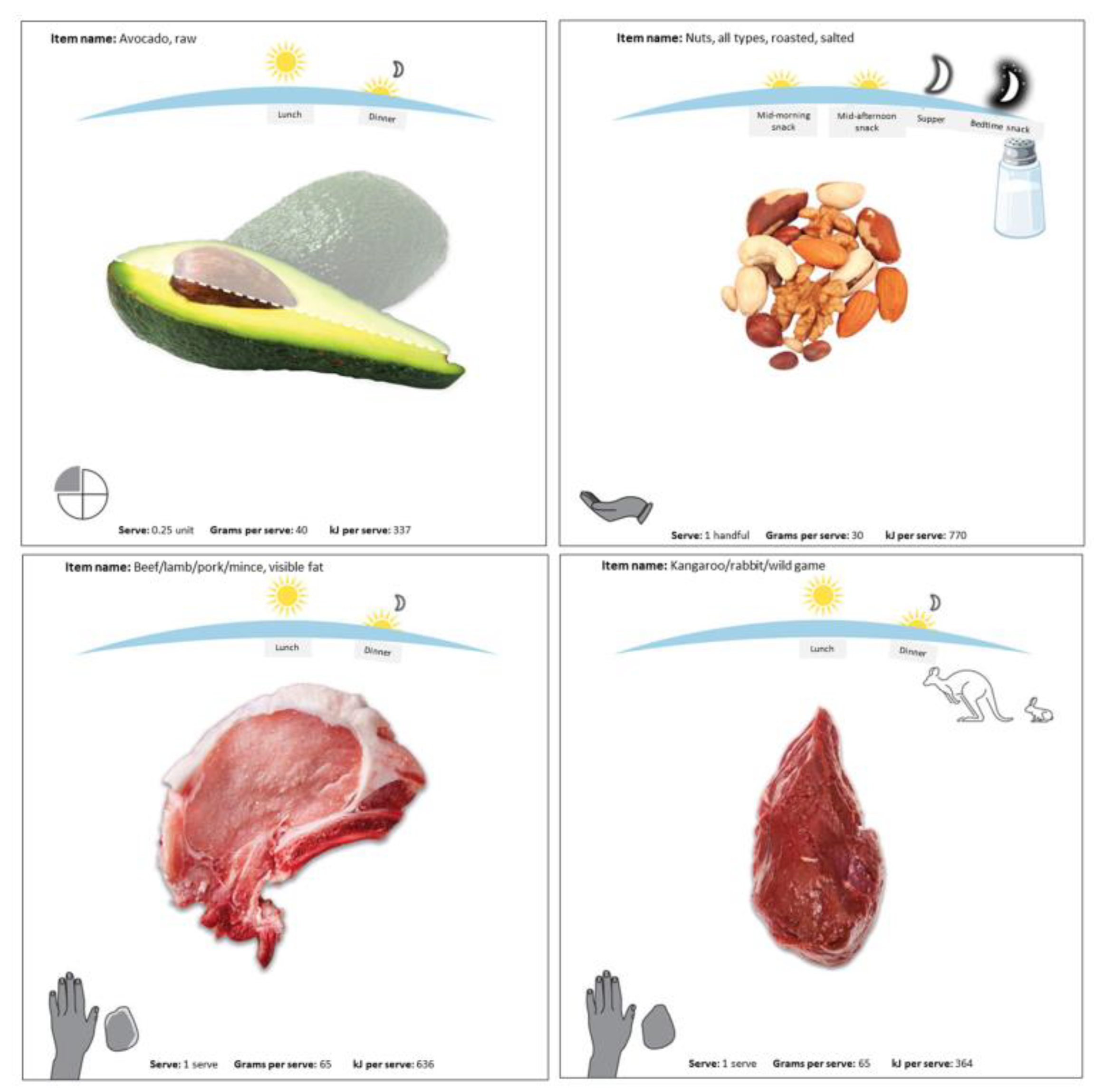
- Step 4: Abbreviation of list items. Since the overall aim of the dietary counseling was to improve adherence to the food-based ADGs [33], this guided the abbreviation of the FFQ food list. For example, starchy vegetables (potatoes, corn, sweet potatoes) were grouped into a single item, as were fresh vegetables. The electronic platform included pictures to inform the user of the foods each FFQ item included (see Figure 2).
- Step 5: Community input. Critically, we obtained community input to refine the data-derived food list and database. An experienced local dietician working with the South West Aboriginal Medical Service in Bunbury, Western Australia (one of the two study sites) assisted with the prioritization of foods to be included in the main FFQ list. She also reviewed and assisted with: (1) defining serving sizes as amounts typically served/eaten/packaged (e.g., 1 slice of bread, 1 flatbread); (2) defining ADG-based serving sizes (e.g., 1 ADG grain serve = 1 slice of bread, ½ flatbread); and (3) reviewing the food database for completeness.
2.2. Developing a Study Food and Nutrient Database
2.3. Assessing FFQ Functionality
2.3.1. Participant Recruitment
2.3.2. FFQ Administration
3. Results
3.1. Analysis of NATSIPAS Nutrition Data and Development of the FFQ
3.2. Test of the FFQ among Kaat Koort Participants
4. Discussion
4.1. FFQ List Development
4.2. Community Input and Meal-Based FFQ
4.3. Advantages of the Digital Platform
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Browne, J.; Lock, M.; Walker, T.; Egan, M.; Backholer, K. Effects of food policy actions on Indigenous Peoples’ nutrition-related outcomes: A systematic review. BMJ Glob. Health 2020, 5, e002442. [Google Scholar] [CrossRef]
- Christidis, R.; Lock, M.; Walker, T.; Egan, M.; Browne, J. Concerns and priorities of Aboriginal and Torres Strait Islander peoples regarding food and nutrition: A systematic review of qualitative evidence. Int. J. Equity Health 2021, 20, 220. [Google Scholar] [CrossRef]
- Goettke, E.; Reynolds, J. “It’s all interconnected… like a spider web”: A qualitative study of the meanings of food and healthy eating in an Indigenous community. Int. J. Circumpolar Health 2019, 78, 1648969. [Google Scholar] [CrossRef]
- Lee, A.; Ride, K. Review of Nutrition among Aboriginal and Torres Strait Islander People. Aust. Indig. Health Bull. 2018, 18, 1–47. Available online: https://healthbulletin.org.au/articles/review-of-nutrition-among-aboriginal-and-torres-strait-islander-people/ (accessed on 11 October 2023).
- Tanous, O. You, as of now, are someone else!: Minoritzation, settler colonialism, and Indigenous health. J. Pal. Stud. 2023, 52, 68–86. [Google Scholar] [CrossRef]
- Gardiner, F.W.; Rallah-Baker, K.; Dos Santos, A.; Sharma, P.; Churilov, L.; Donnan, G.A.; Davis, S.M.; Quinlan, F.; Worley, P. Indigenous Australians have a greater prevalence of heart, stroke, and vascular disease, are younger at death, with higher hospitalisation and more aeromedical retrievals from remote regions. EClinicalMedicine 2021, 42, 101181. [Google Scholar] [CrossRef]
- Whalan, S.; Farnbach, S.; Volk, L.; Gwynn, J.; Lock, M.; Trieu, K.; Brimblecombe, J.; Webster, J. What do we know about the diets of Aboriginal and Torres Strait Islander peoples in Australia? A systematic literature review. Aust. N. Z. J. Public Health 2017, 41, 579–584. [Google Scholar] [CrossRef]
- Rebuli, M.A.; Hendrie, G.A.; Baird, D.L.; Mahoney, R.; Riley, M.D. Beverage intake and associated nutrient contribution for Aboriginal and Torres Strait Islander Australians: Secondary analysis of a national dietary survey 2012–2013. Nutrients 2022, 14, 507. [Google Scholar] [CrossRef]
- Jernigan, V.B.B.; Huyser, K.R.; Valdes, J.; Simonds, V.W. Food insecurity among American Indians and Alaska Natives: A na-tional profile using the current Population Survey-Food Security Supplement. J. Hunger Environ. Nutr. 2017, 12, 1–10. [Google Scholar] [CrossRef]
- Nikolaus, C.J.; Johnson, S.; Benally, T.; Maudrie, T.; Henderson, A.; Nelson, K.; Lane, T.; Segrest, V.; Ferguson, G.L.; Buchwald, D.; et al. Food insecurity Among American Indian and Alaska Native People: A scoping review to in-form future research and policy needs. Adv. Nutr. 2022, 13, 1566–1583. [Google Scholar] [CrossRef]
- Richmond, C.; Steckley, M.; Neufeld, H.; Kerr, R.B.; Wilson, K.; Dokis, B. First Nations food environments: Exploring the role of place, income, and social connection. Curr. Dev. Nutr. 2020, 4, nzaa108. [Google Scholar] [CrossRef] [PubMed]
- Sherriff, S.; Kalucy, D.; Tong, A.; Naqvi, N.; Nixon, J.; Eades, S.; Ingram, T.; Slater, K.; Dickson, M.; Lee, A.; et al. Murradambirra Dhangaang (make food secure): Aboriginal community and stakeholder perspectives on food insecurity in urban and regional Australia. BMC Public Health 2022, 22, 1066. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. Australian Aboriginal and Torres Strait Islander Health Survey: Nutrition Results—Food and Nutrients, 2012–2013, 4727.0.55.005. 2015. Available online: https://www.ausstats.abs.gov.au/ausstats/subscriber.nsf/0/5D4F0DFD2DC65D9ECA257E0D000ED78F/$File/4727.0.55.005%20australian%20aboriginal%20and%20torres%20strait%20islander%20health%20survey,%20nutrition%20results%20%20-%20food%20and%20nutrients%20.pdf (accessed on 14 November 2023).
- Turrini, A. Perspectives of dietary assessment in human health and disease. Nutrients 2022, 14, 830. [Google Scholar] [CrossRef] [PubMed]
- About the National Aboriginal and Torres Strait Islander Nutrition and Physical Activity Survey. Available online: https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/by%20Subject/4727.0.55.008~2012-13~Main%20Features~About%20the%20National%20Aboriginal%20and%20Torres%20Strait%20Islander%20Nutrition%20and%20Physical%20Activity%20Survey~10001 (accessed on 12 October 2023).
- Thompson, F.E.; Subar, A.F. Dietary Assessment Methodology. In Nutrition in the Prevention and Treatment of Disease; Coulston, A.M., Rock, C.L., Monsen, E.R., Eds.; Elsevier: Amsterdam, The Netherlands, 2017; pp. 5–48. [Google Scholar]
- Sharma, S. Development and use of FFQ among adults in diverse settings across the globe. Proc. Nutr. Soc. 2011, 70, 232–251. [Google Scholar] [CrossRef] [PubMed]
- Stewart, A.L.; Thrasher, A.D.; Goldberg, J.; Shea, J.A. A framework for understanding modifications to measures for diverse populations. J. Aging Health 2012, 24, 992–1017. [Google Scholar] [CrossRef]
- Tucker, K.L.; Bianchi, L.A.; Maras, J.; Bermudez, O.I. Adaptation of a food frequency questionnaire to assess diets of Puerto Rican and non-Hispanic adults. Am. J. Epidemiol. 1998, 148, 507–518. [Google Scholar] [CrossRef]
- Akbar, J.A.; Jaceldo-Siegl, K.; Fraser, G.; Herring, R.P.; Yancey, A. The contribution of soul and Caribbean foods to nutrient intake in a sample of Blacks of US and Caribbean descent in the Adventist Health Study-2: A pilot study. Ethn. Dis. 2007, 17, 244–249. [Google Scholar] [PubMed]
- Abu-Saad, K.; Shahar, D.R.; Vardi, H.; Fraser, D. Importance of ethnic foods as predictors of and contributors to nutrient intake levels in a minority population. Eur. J. Clin. Nutr. 2010, 64 (Suppl. S3), S88–S94. [Google Scholar] [CrossRef]
- Beukers, M.H.; Dekker, L.H.; de Boer, E.J.; Perenboom, C.W.; Meijboom, S.; Nicolaou, M.; de Vries, J.H.; Brants, H.A. Devel-opment of the HELIUS food frequency questionnaires: Ethnic-specific questionnaires to assess the diet of a multiethnic popu-lation in The Netherlands. Eur. J. Clin. Nutr. 2015, 69, 579–584. [Google Scholar] [CrossRef]
- Bassett, J.K.; English, D.R.; Fahey, M.T.; Forbes, A.B.; Gurrin, L.C.; Simpson, J.A.; Brinkman, M.T.; Giles, G.G.; Hodge, A.M. Validity and calibration of the FFQ used in the Melbourne Collaborative Cohort Study. Public Health Nut. 2016, 19, 2357–2368. [Google Scholar] [CrossRef]
- Collins, C.E.; Boggess, M.M.; Watson, J.F.; Guest, M.; Duncanson, K.; Pezdirc, K.; Rollo, M.; Hutchesson, M.J.; Burrows, T.L. Reproducibility and comparative validity of a food frequency questionnaire for Australian adults. Clin. Nutr. 2014, 33, 906–914. [Google Scholar] [CrossRef] [PubMed]
- Gwynn, J.D.; Flood, V.M.; D’Este, C.A.; Attia, J.R.; Turner, N.; Cochrane, J.; Wiggers, J.H.; Many Rivers Diabetes Prevention Project Study Team. The reliability and validity of a short FFQ among Australian Aboriginal and Torres Strait Islander and non-Indigenous rural children. Public Health Nutr. 2011, 14, 388–401. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.S.; Attia, J.; McEvoy, M.; Hure, A.J. Biochemical validation of the older Australian’s food frequency questionnaire using carotenoids and vitamin E. Nutrients 2014, 6, 4906–4917. [Google Scholar] [CrossRef] [PubMed]
- Watson, J.F.; Collins, C.E.; Sibbritt, D.W.; Dibley, M.J.; Garg, M.L. Reproducibility and comparative validity of a food frequency questionnaire for Australian children and adolescents. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 62. [Google Scholar] [CrossRef] [PubMed]
- Australian Bureau of Statistics. 4727.0.55.002—Australian Aboriginal and Torres Strait Islander Health Survey: Users’ Guide, 2012–2013; Australian Bureau of Statistics: Canberra, Australia, 2013. Available online: https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/C7AE9CD45CBAB87FCA257C2F00146263?opendocument (accessed on 12 October 2023).
- Australian Bureau of Statistics. Australian Aboriginal and Torres Strait Islander Health Survey: Consumption of Food Groups from the Australian Dietary Guidelines, Australia 2012–2013, 4727.0.55.008. 2016. Available online: https://www.ausstats.abs.gov.au/ausstats/subscriber.nsf/0/EBB72D8B7C4C0AD2CA25805E0019CC97/$File/4727.0.55.008%20-%20Consumption%20of%20Food%20Groups%20from%20the%20Australian%20Dietary%20Guidelines%20.pdf (accessed on 14 November 2023).
- Willett, W. Food frequency methods. In Nutritional Epidemiology, 3rd ed.; Willett, W., Ed.; Oxford University Press: New York, NY, USA, 2012; pp. 70–95. [Google Scholar]
- Australia New Zealand Clinical Trials Registry (ANZCTR). Kaat Koort: Examining the Impact of a Program Targeting cardio-Metabolic Risk and Lifestyle Changes on Heart and Brain Health among Aboriginal and Torres Strait Islander People, Regis-tration No. ACTRN12621001022853. Available online: https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=382003&isReview=true (accessed on 12 October 2023).
- van den Brink, A.C.; Brouwer-Brolsma, E.M.; Berendsen, A.A.M.; van de Rest, O. The Mediterranean, Dietary Approaches to Stop Hypertension (DASH), and Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) diets are associated with less cognitive decline and a lower risk of alzheimer’s disease-A review. Adv. Nutr. 2019, 10, 1040–1065. [Google Scholar] [CrossRef] [PubMed]
- National Health and Medical Research Council (NHMRC). Australian Dietary Guidelines; National Health and Medical Research Council: Canberra, Australia, 2013. Available online: https://www.nhmrc.gov.au/adg (accessed on 12 October 2023).
- Kalter-Leibovici, O.; Younis-Zeidan, N.; Atamna, A.; Lubin, F.; Alpert, G.; Chetrit, A.; Novikov, I.; Daoud, N.; Freedman, L.S. Lifestyle intervention in obese Arab women: A randomized controlled trial. Arch. Intern. Med. 2010, 170, 970–976. [Google Scholar] [CrossRef][Green Version]
- Abu-Saad, K.; Murad, H.; Barid, R.; Olmer, L.; Ziv, A.; Younis-Zeidan, N.; Kaufman-Shriqui, V.; Gillon-Keren, M.; Rigler, S.; Berchenko, Y.; et al. Development and efficacy of an electronic, culturally adapted lifestyle counseling tool for improving diabetes-related dietary knowledge: Randomized controlled trial among ethnic minority adults with type 2 diabetes mellitus. J. Med. Internet Res. 2019, 21, e13674. [Google Scholar] [CrossRef]
- McMahon, E.; Wycherley, T.; O’Dea, K.; Brimblecombe, J. A comparison of dietary estimates from the National Aboriginal and Torres Strait Islander Health Survey to food and beverage purchase data. Aust. N. Z. J. Public Health 2017, 41, 598–603. [Google Scholar] [CrossRef]
- Raper, N.; Perloff, B.; Ingwersen, L.; Steinfeldt, L.; Anand, J. An overview of USDA’s Dietary Intake Data System. J. Food Comp. Anal. 2004, 17, 545–555. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. Nutrition, in 4363.0.55.001—Australian Health Survey: Users’ Guide, 2011–2013. Available online: https://www.abs.gov.au/ausstats/abs@.nsf/Lookup/6CB038300A8571F7CA257CD2001CA0EF?opendocument (accessed on 12 October 2023).
- Food Standards Australia New Zealand (FSANZ). AUSNUT 2011–13—Australian Food Composition Database; FSANZ: Canberra, Australia, 2014. Available online: https://www.foodstandards.gov.au/science/monitoringnutrients/ausnut/pages/default.aspx (accessed on 12 October 2023).
- Willett, W.C.; Sampson, L.; Stampfer, M.J.; Rosner, B.; Bain, C.; Witschi, J.; Hennekens, C.H.; Speizer, F.E. Reproducibility and validity of a semiquantitative food frequency questionnaire. Am. J. Epidemiol. 1985, 122, 51–65. [Google Scholar] [CrossRef]
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics—2022 Update: A Report From the American Heart Association. Circulation 2022, 145, e153–e639. [Google Scholar] [CrossRef] [PubMed]
- Bessarab, D.; Ng’Andu, B. Yarning about yarning as a legitimate method in Indigenous research. Int. J. Crit. Indig. Stud. 2010, 3, 37–50. [Google Scholar] [CrossRef]
- Hallett, J.; Held, S.; McCormick, A.K.H.G.; Simonds, V.; Real Bird, S.; Martin, C.; Simpson, C.; Schure, M.; Turnsplenty, N.; Trottier, C. What touched your heart? Collaborative story analysis emerging from an Apsáalooke cultural context. Qual. Health Res. 2016, 27, 1267–1277. [Google Scholar] [CrossRef] [PubMed]
- Wain, T.; Sim, M.; Bessarab, D.; Mak, D.; Hayward, C.; Rudd, C. Engaging Australian Aboriginal narratives to challenge attitudes and create empathy in health care: A methodological perspective. BMC Med. Educ. 2016, 16, 156. [Google Scholar] [CrossRef] [PubMed]
- Walker, M.; Fredericks, B.; Mills, K.; Anderson, D. “Yarning” as a method for community-based health research with Indigenous women: The Indigenous Women’s Wellness Research Program. Health Care Women Int. 2014, 35, 1216–1226. [Google Scholar] [CrossRef]
- Institute of Medicine. Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids; The National Academies Press: Washington, DC, USA, 2005; p. 10490. [Google Scholar] [CrossRef]
- Buchowski, M.S.; Schlundt, D.G.; Hargreaves, M.K.; Hankin, J.H.; Signorello, L.B.; Blot, W.J. Development of a culturally sen-sitive food frequency questionnaire for use in the Southern Community Cohort Study. Cell Mol. Biol. 2003, 49, 1295–1304. [Google Scholar]
- Chen, J.; Grech, A.; Allman-Farinelli, M. Using popular foods consumed to inform development of digital tools for dietary assessment and monitoring. Nutrients 2022, 14, 4822. [Google Scholar] [CrossRef]
- El Mesmoudi, N.; Al Dhaheri, A.S.; Feehan, J.; Stojanovska, L.; Ali, H.I. Validation of a quantitative web-based food frequency questionnaire to assess dietary intake in the adult Emirati population. PLoS ONE 2022, 17, e0262150. [Google Scholar] [CrossRef]
- Neelakantan, N.; Whitton, C.; Seah, S.; Koh, H.; Rebello, S.A.; Lim, J.Y.; Chen, S.; Chan, M.F.; Chew, L.; Van Dam, R.M. Development of a semi-quantitative food frequency questionnaire to assess the dietary intake of a multi-ethnic urban Asian population. Nutrients 2016, 8, 528. [Google Scholar] [CrossRef]
- Shai, I.; Shahar, D.R.; Vardi, H.; Fraser, D. Selection of food items for inclusion in a newly developed food-frequency ques-tionnaire. Public Health Nutr. 2004, 7, 745–749. [Google Scholar] [CrossRef]
- Zheng, M.; Campbell, K.J.; Scanlan, E.; McNaughton, S.A. Development and evaluation of a food frequency questionnaire for use among young children. PLoS ONE 2020, 15, e0230669. [Google Scholar] [CrossRef]
- Pannen, S.T.; Gassmann, R.; Vorburger, R.; Rohrmann, S.; Sych, J.; Steinemann, N. Development of a multilingual web-based food frequency questionnaire for adults in Switzerland. Nutrients 2023, 15, 4359. [Google Scholar] [CrossRef]
- Drawson, A.S.; Toombs, E.; Mushquash, C.J. Indigenous research methods: A systematic review. Int. Indig. Policy J. 2017, 8, 5. [Google Scholar] [CrossRef]
- Christensen, S.E.; Möller, E.; Bonn, S.E.; Ploner, A.; Wright, A.; Sjölander, A.; Bälter, O.; Lissner, L.; Bälter, K. Two new meal- and web-based interactive food frequency questionnaires: Validation of energy and macronutrient intake. J. Med. Internet Res. 2013, 15, e109. [Google Scholar] [CrossRef]
- Fregapane, G.; Asensio-García, C. Dietary assessment of an educated young Spanish population using a self-administered meal-based food frequency questionnaire. Eur. J. Epidemiol. 2000, 16, 183–191. [Google Scholar] [CrossRef]
- Quandt, S.A.; Vitolins, M.Z.; Smith, S.L.; Tooze, J.A.; Bell, R.A.; Davis, C.C.; DeVellis, R.F.; Arcury, T.A. Comparative validation of standard, picture-sort and meal-based food-frequency questionnaires adapted for an elderly population of low so-cio-economic status. Public Health Nutr. 2007, 10, 524–532. [Google Scholar] [CrossRef]
- Block, G.; Hartman, A.M.; Dresser, C.M.; Carroll, M.D.; Gannon, J.; Gardner, L. A data-based approach to diet questionnaire design and testing. Am. J. Epidemiol. 1986, 124, 453–469. [Google Scholar] [CrossRef]
- EPIC-Norfolk Study Food Frequency Questionnaire. Available online: https://www.epic-norfolk.org.uk/about-epic-norfolk/nutritional-methods/ffq/ (accessed on 14 November 2023).
- The Nurses’ Health Study Food Frequency Questionnaire. 1984. Available online: https://nurseshealthstudy.org/sites/default/files/questionnaires/1984long.pdf (accessed on 13 November 2023).
- The Health Professionals Follow-up Study Food Frequency Questionnaire. 1986. Available online: https://www.hsph.harvard.edu/hpfs/wp-content/uploads/sites/2471/2017/09/86L.pdf (accessed on 13 November 2023).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Food Groups | Percent Contribution to Total Energy Intake |
|---|---|
| Main contributors to energy intake 1 | |
| Breads, white | 6.45 |
| Beef, lamb, pork | 4.70 |
| Soft drinks | 3.75 |
| Processed meat | 3.47 |
| Hot potato chips | 3.40 |
| Milk, full fat | 3.13 |
| Mixed poultry dishes | 3.08 |
| Savory pasta/rice dishes | 3.06 |
| Cakes | 2.71 |
| Poultry | 2.69 |
| Burgers | 2.63 |
| Savory pastry | 2.52 |
| Sugar | 2.18 |
| Mixed red meat dishes | 2.17 |
| Beers, regular | 2.01 |
| Pizza | 1.79 |
| Wine | 1.66 |
| Cheese, ripened, high fat | 1.61 |
| Beers, lite | 1.54 |
| Potatoes | 1.49 |
| Fin fish, fried | 1.32 |
| Breads, whole grain | 1.27 |
| Breads, mixed grain | 1.21 |
| Ice cream, full fat | 1.19 |
| Breakfast cereal, whole grain, low sugar | 1.17 |
| Cordials | 1.15 |
| Chocolate, filled | 1.07 |
| Rice | 1.02 |
| Margarine | 0.97 |
| Eggs | 0.94 |
| Milk drinks, full fat | 0.92 |
| Bananas | 0.92 |
| Butter | 0.89 |
| Breakfast cereal, muesli | 0.83 |
| Sweet biscuits, filled | 0.82 |
| Spiked soft drinks | 0.79 |
| Chocolate, plain | 0.78 |
| Milk, low fat | 0.78 |
| Fruit drinks | 0.75 |
| Sandwiches | 0.74 |
| Potato crisps | 0.74 |
| Porridge | 0.72 |
| Pasta and noodles | 0.69 |
| Fruit juices | 0.68 |
| Pome fruit | 0.66 |
| Egg dishes, savory | 0.60 |
| Coffee with milk | 0.60 |
| Subtotal % (number of groups) | 80.25 (47) |
| Main contributors to other nutrients 2 | |
| Cocktails | 0.59 |
| Gravies | 0.58 |
| Electrolyte drinks (sports drinks) | 0.56 |
| Other nuts | 0.53 |
| Salad dressing, full fat | 0.53 |
| Doughnut/crepe/pancake | 0.47 |
| Dairy desserts | 0.47 |
| Salads, vegetable based | 0.47 |
| Squash | 0.40 |
| Candies, sugar sweetened | 0.36 |
| Fin fish, fresh | 0.34 |
| Soup with meat, homemade | 0.34 |
| Fin fish, preserved | 0.33 |
| Mixed vegetables | 0.30 |
| Fortified beverage | 0.29 |
| Other fruit | 0.29 |
| Honey and sugar syrups | 0.29 |
| Sports/protein beverage | 0.27 |
| Citrus fruit | 0.26 |
| Legume products | 0.20 |
| Other root vegetables | 0.19 |
| Sweetcorn | 0.18 |
| Stone fruit | 0.17 |
| Carrots | 0.15 |
| Tomato | 0.15 |
| Peas and edible podded peas | 0.10 |
| Brassica vegetables | 0.07 |
| Subtotal % (number of groups) | 8.88 (27) |
| Additional contributors to between-person variation 3 | |
| Peanut products | 0.23 |
| Spirits/liquors | 0.25 |
| Tropical fruit | 0.11 |
| Subtotal % (number of groups) | 0.59 (3) |
| Total contribution of all food groups | 89.72 (77) |
| 24HR Food Groups (% Contribution to Total Energy) | Items Representing Food Group in Digital FFQ Platform |
|---|---|
| Breads, white (6.4%) | Bread/toast, white flour |
| Bread, damper, white flour | |
| Bread roll, white flour | |
| Bread, tortilla/flat wrap, white flour | |
| Soft drinks/cordials (4.9%) | Soft drink/fruit drink/cordial/slushie, regular |
| Beef, lamb, pork (4.7%) | Beef/lamb/pork/mince, visible fat |
| Beef/lamb/pork/mince, lean | |
| Processed meat (3.5%) | Bacon |
| Sausage | |
| Sausage, lean | |
| Ham | |
| Spam/polony/processed luncheon meat | |
| Corned beef | |
| Cheese sausage | |
| Hot potato chips (3.4%) | Hot potato chips/fries/hash browns, takeaway |
| Hot potato chips/fries, homemade |
| Characteristic | Total (n = 60) | Women (n = 42) | Men (n = 18) |
|---|---|---|---|
| Age (years), median (IQR) | 48 (42–55) | 48.0 (42.0–55.0) | 48.5 (42.0–54.0) |
| Self-reported chronic morbidity | |||
| Hypercholesterolaemia, n (%) | 23 (38.3) | 16 (38.1) | 7 (38.8) |
| Hypertension, n (%) | 13 (21.7) | 7 (16.7) | 6 (33.3) |
| Type 2 diabetes, n (%) | 25 (41.7) | 17 (40.5) | 8 (44.4) |
| Coronary artery disease, n (%) | 6 (11.5) | 3 (7.1) | 3 (16.7) |
| BMI (kg/m2), median (IQR) | 34.0 (29.0–58.4) | 35.0 (29.3–41.7) | 31.7 (28.1–39.8) |
| Reported energy intake per day (kJ), median (IQR) | 10,042 (6968–12,175) | 9226 (6645–11,770) | 11,200 (8605–13,738) |
| Estimated total energy expenditure per day (kJ), median (IQR) | 10,197 (8636–11,551) | 9010 (8223–10,789) | 12,413 (10,798–13,564) |
| Percent Contribution to Total Intake | ||
|---|---|---|
| Nutrient or Food Group | Main Items | Extra Items |
| 4a. Energy and nutrients | ||
| Energy (kJ) | 69.9 | 30.1 |
| Protein (g) | 66.8 | 33.2 |
| Total fat (g) | 66.0 | 34.0 |
| Fiber (g) | 81.3 | 18.7 |
| Carbohydrates (g) | 74.2 | 25.8 |
| Total sugar (g) | 75.7 | 24.3 |
| Free sugar (g) | 77.3 | 22.7 |
| Calcium (mg) | 65.9 | 34.1 |
| Sodium (mg) | 68.8 | 31.2 |
| Magnesium (mg) | 68.9 | 31.1 |
| Potassium (mg) | 69.9 | 30.1 |
| 4b. Food groups (serves) | ||
| Total grains | 79.7 | 20.3 |
| Whole grains | 84.5 | 15.5 |
| Total Vegetables | 90.4 | 9.6 |
| Fruit | 92.3 | 7.7 |
| Total dairy | 56.8 | 43.2 |
| Low fat dairy | 50.7 | 49.3 |
| Meats and alternative protein sources 2 | 53.8 | 46.2 |
| Fast/fried food | 61.4 | 38.6 |
| Processed/salty food | 61.4 | 38.6 |
| Alcoholic drinks | 69.1 | 30.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu-Saad, K.; Accos, M.; Ziv, A.; Collins, F.; Shepherd, C.; Eades, S.; Kalter-Leibovici, O. Development and Functionality of a Parsimonious Digital Food Frequency Questionnaire for a Clinical Intervention among an Indigenous Population. Nutrients 2023, 15, 5012. https://doi.org/10.3390/nu15235012
Abu-Saad K, Accos M, Ziv A, Collins F, Shepherd C, Eades S, Kalter-Leibovici O. Development and Functionality of a Parsimonious Digital Food Frequency Questionnaire for a Clinical Intervention among an Indigenous Population. Nutrients. 2023; 15(23):5012. https://doi.org/10.3390/nu15235012
Chicago/Turabian StyleAbu-Saad, Kathleen, Moran Accos, Arnona Ziv, Fiona Collins, Carrington Shepherd, Sandra Eades, and Ofra Kalter-Leibovici. 2023. "Development and Functionality of a Parsimonious Digital Food Frequency Questionnaire for a Clinical Intervention among an Indigenous Population" Nutrients 15, no. 23: 5012. https://doi.org/10.3390/nu15235012
APA StyleAbu-Saad, K., Accos, M., Ziv, A., Collins, F., Shepherd, C., Eades, S., & Kalter-Leibovici, O. (2023). Development and Functionality of a Parsimonious Digital Food Frequency Questionnaire for a Clinical Intervention among an Indigenous Population. Nutrients, 15(23), 5012. https://doi.org/10.3390/nu15235012