
Phase Angle as a Risk Factor for Mortality in Patients Undergoing Peritoneal Dialysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Baseline Characteristics
2.3. Assessment of PhA and Patient or Technique Survivals
2.4. Statistical Analyses
3. Results
3.1. Participants’ Clinical Characteristics
3.2. Patient or Technique Survival according to PhA Tertiles
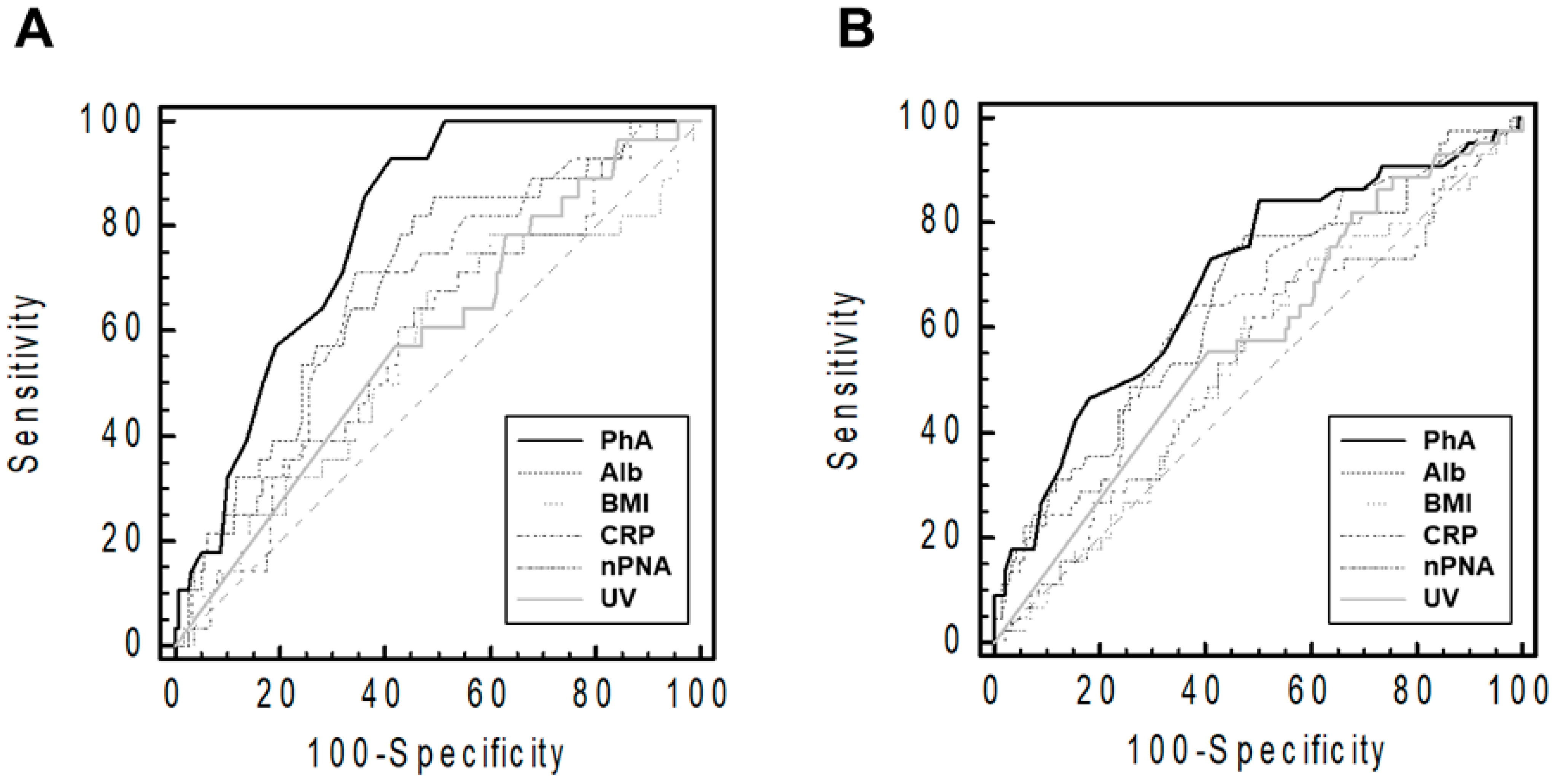
3.3. The Comparison of Patient or Technique Survival among Various Indicators
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- US Renal Data System. USRDS 2020 Annual Data Report: Atlas of Chronic Kidney Disease in the United States; National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2020. Available online: https://adr.usrds.org/2020 (accessed on 1 August 2022).
- Levey, A.S.; Eckardt, K.U.; Dorman, N.M.; Christiansen, S.L.; Cheung, M.; Jadoul, M.; Winkelmayer, W.C. Nomenclature for kidney function and disease: Executive summary and glossary from a Kidney Disease: Improving Global Outcomes (KDIGO) Consensus Conference. Kidney Res. Clin. Pract. 2020, 39, 151–161. [Google Scholar] [CrossRef]
- Sinnakirouchenan, R.; Holley, J.L. Peritoneal dialysis versus hemodialysis: Risks, benefits, and access issues. Adv. Chronic Kidney Dis. 2011, 18, 428–432. [Google Scholar] [CrossRef]
- Hong, Y.A.; Ban, T.H.; Kang, C.Y.; Hwang, S.D.; Choi, S.R.; Lee, H.; Jung, H.-Y.; Kim, K.; Kwon, Y.E.; Kim, S.H.; et al. Trends in epidemiologic characteristics of end-stage renal disease from 2019 Korean Renal Data System (KORDS). Kidney Res. Clin. Pract. 2021, 40, 52–61. [Google Scholar] [CrossRef]
- Zhang, J.; Lu, X.; Li, H.; Wang, S. Risk factors for mortality in patients undergoing peritoneal dialysis: A systematic review and meta-analysis. Ren. Fail. 2021, 43, 743–753. [Google Scholar] [CrossRef]
- Do, J.Y.; Kim, A.Y.; Kang, S.H. Association Between Phase Angle and Sarcopenia in Patients Undergoing Peritoneal Dialysis. Front. Nutr. 2021, 8, 742081. [Google Scholar] [CrossRef]
- Sarmento-Dias, M.; Santos-Araújo, C.; Poínhos, R.; Oliveira, B.; Sousa, M.; Simões-Silva, L.; Soares-Silva, I.; Correia, F.; Pestana, M. Phase Angle Predicts Arterial Stiffness and Vascular Calcification in Peritoneal Dialysis Patients. Perit. Dial. Int. 2017, 37, 451–457. [Google Scholar] [CrossRef]
- Han, B.G.; Lee, J.Y.; Kim, J.S.; Yang, J.W. Clinical Significance of Phase Angle in Non-Dialysis CKD Stage 5 and Peritoneal Dialysis Patients. Nutrients 2018, 10, 1331. [Google Scholar] [CrossRef]
- Abad, S.; Sotomayor, G.; Vega, A.; Pérez de José, A.; Verdalles, U.; Jofré, R.; López-Gómez, J.M. The phase angle of the electrical impedance is a predictor of long-term survival in dialysis patients. Nefrologia 2011, 31, 670–676. [Google Scholar]
- Huang, R.; Wu, M.; Wu, H.; Ye, H.; Peng, Y.; Yi, C.; Yu, X.; Yang, X. Lower Phase Angle Measured by Bioelectrical Impedance Analysis Is a Marker for Increased Mortality in Incident Continuous Ambulatory Peritoneal Dialysis Patients. J. Ren. Nutr. 2020, 30, 119–125. [Google Scholar] [CrossRef]
- Mushnick, R.; Fein, P.A.; Mittman, N.; Goel, N.; Chattopadhyay, J.; Avram, M.M. Relationship of bioelectrical impedance parameters to nutrition and survival in peritoneal dialysis patients. Kidney Int. Suppl. 2003, 87, S53–S56. [Google Scholar] [CrossRef]
- Davies, S.J.; Phillips, L.; Naish, P.F.; Russell, G.I. Quantifying comorbidity in peritoneal dialysis patients and its relationship to other predictors of survival. Nephrol. Dial. Transplant. 2002, 17, 1085–1092. [Google Scholar] [CrossRef]
- Kang, S.H.; Do, J.Y. Effects of volume status on body composition in incident peritoneal dialysis patients. Eur. J. Clin. Nutr. 2020, 74, 633–641. [Google Scholar] [CrossRef]
- Arroyo, D.; Panizo, N.; Abad, S.; Vega, A.; Rincón, A.; de José, A.P.; López-Gómez, J.M. Intraperitoneal fluid overestimates hydration status assessment by bioimpedance spectroscopy. Perit. Dial. Int. 2015, 35, 85–89. [Google Scholar] [CrossRef]
- Lan, P.G.; Clayton, P.A.; Johnson, D.W. Duration of hemodialysis following peritoneal dialysis cessation in Australia and New Zealand: Proposal for a standardized definition of technique failure. Perit. Dial. Int. 2016, 36, 623–630. [Google Scholar] [CrossRef]
- Pencina, M.J.; D’Agostino, R.B., Sr.; D’Agostino, R.B., Jr.; Vasan, R.S. Evaluating the added predictive ability of a new marker: From area under the ROC curve to reclassification and beyond. Stat. Med. 2008, 27, 157–172. [Google Scholar] [CrossRef]
- Pencina, M.J.; D’Agostino, R.B., Sr.; Steyerberg, E.W. Extensions of net reclassification improvement calculations to measure usefulness of new biomarkers. Stat. Med. 2011, 30, 11–21. [Google Scholar] [CrossRef]
- Norman, K.; Stobäus, N.; Pirlich, M.; Bosy-Westphal, A. Bioelectrical phase angle and impedance vector analysis--clinical relevance and applicability of impedance parameters. Clin. Nutr. 2012, 31, 854–861. [Google Scholar] [CrossRef]
- Enia, G.; Sicuso, C.; Alati, G.; Zoccali, C. Subjective global assessment of nutrition in dialysis patients. Nephrol. Dial. Transplant. 1993, 8, 1094–1098. [Google Scholar]
- Passadakis, P.; Sud, K.; Dutta, A.; Singhal, M.; Pettit, J.; Chatalalsingh, C.; Thodis, E.; Vargemezis, V.; Oreopoulos, D. Bioelectrical impedance analysis in the evaluation of the nutritional status of continuous ambulatory peritoneal dialysis patients. Adv. Perit. Dial. 1999, 15, 147–152. [Google Scholar]
- Edefonti, A.; Picca, M.; Damiani, B.; Garavaglia, R.; Loi, S.; Ardissino, G.; Marra, G.; Ghio, L. Prevalence of malnutrition assessed by bioimpedance analysis and anthropometry in children on peritoneal dialysis. Perit. Dial. Int. 2001, 21, 172–179. [Google Scholar] [CrossRef]
- Fein, P.A.; Gundumalla, G.; Jorden, A.; Matza, B.; Chattopadhyay, J.; Avram, M.M. Usefulness of bioelectrical impedance analysis in monitoring nutrition status and survival of peritoneal dialysis patients. Adv. Perit. Dial. 2002, 18, 195–199. [Google Scholar] [PubMed]
- Cigarran, S.; Barril, G.; Cirugeda, A.; Bernis, C.; Aguilera, A.; Sanz, P.; Herraez, I.; Alegre, L.; Selgas, R. Hypoalbuminemia is also a marker of fluid excess determined by bioelectrical impedance parameters in dialysis patients. Ther. Apher. Dial. 2007, 11, 114–120. [Google Scholar] [CrossRef] [PubMed]
- Gu, Y.; Cheng, L.T.; Chen, H.M.; Sun, X.Y.; Tang, L.J.; Guo, L.J.; Axelsson, J.; Wang, T. Strong association between nutritional markers and arterial stiffness in continuous ambulatory peritoneal dialysis patients. Blood Purif. 2008, 26, 340–346. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Do, J.Y.; Kim, J.C. Impedance-derived phase angle is associated with muscle mass, strength, quality of life, and clinical outcomes in maintenance hemodialysis patients. PLoS ONE 2022, 17, e0261070. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.; Hwang, J.H.; Han, M.; Cha, R.H.; Kang, S.H.; An, W.S.; Kim, J.C.; Kim, S.H. Phase angle as a marker for muscle health and quality of life in patients with chronic kidney disease. Clin. Nutr. 2022, 41, 1651–1659. [Google Scholar] [CrossRef] [PubMed]
- Rinaldi, S.; Gilliland, J.; O’Connor, C.; Chesworth, B.; Madill, J. Is phase angle an appropriate indicator of malnutrition in different disease states? A systematic review. Clin. Nutr. ESPEN 2019, 29, 1–14. [Google Scholar] [CrossRef]
- Shu, Y.; Liu, J.; Zeng, X.; Hong, H.G.; Li, Y.; Zhong, H.; Ma, L.; Fu, P. The Effect of Overhydration on Mortality and Technique Failure Among Peritoneal Dialysis Patients: A Systematic Review and Meta-Analysis. Blood Purif. 2018, 46, 350–358. [Google Scholar] [CrossRef]
- Bellido, D.; García-García, C.; Talluri, A.; Lukaski, H.C.; García-Almeida, J.M. Future lines of research on phase angle: Strengths and limitations. Rev. Endocr. Metab. Disord. 2023, 24, 563–583. [Google Scholar] [CrossRef]
- Shizgal, H.M. The effect of malnutrition on body composition. Surg. Gynecol. Obstet. 1981, 152, 22–26. [Google Scholar]
- Selberg, O.; Selberg, D. Norms and correlates of bioimpedance phase angle in healthy human subjects, hospitalized patients, and patients with liver cirrhosis. Eur. J. Appl. Physiol. 2002, 86, 509–516. [Google Scholar] [CrossRef]
- Dumler, F.; Kilates, C. Body composition analysis by bioelectrical impedance in chronic maintenance dialysis patients: Comparisons to the National Health and Nutrition Examination Survey III. J. Ren. Nutr. 2003, 13, 166–172. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Characteristics | Low Tertile (n = 66) | Middle Tertile (n = 68) | High Tertile (n = 65) | p-Value |
|---|---|---|---|---|
| Age (years) | 59.4 ± 11.7 | 57.3 ± 11.2 | 49.8 ± 11.9 a,b | <0.001 |
| Sex (male) | 30 (45.5%) | 35 (51.5%) | 48 (73.8%) | 0.003 |
| Davies comorbidity index | <0.001 | |||
| Low-risk group | 19 (28.8%) | 20 (29.4%) | 40 (61.5%) | |
| Intermediate-risk group | 37 (56.1%) | 45 (66.2%) | 24 (36.9%) | |
| High-risk group | 10 (15.2%) | 3 (4.4%) | 1 (1.5%) | |
| Automated peritoneal dialysis (%) | 14 (21.2%) | 21 (30.9%) | 22 (33.8%) | 0.245 |
| Dialysis vintage (months) | 64 (37–108) | 51 (26–80) | 48 (25–86) | 0.367 |
| Body mass index (kg/m2) | 23.9 (21.9–26.2) | 23.9 (21.7–25.6) | 24.8 (22.5–27.9) b | 0.025 |
| Weekly Kt/Vurea | 1.93 ± 0.43 | 1.87 ± 0.43 | 1.96 ± 0.51 | 0.454 |
| C-reactive protein (mg/dL) | 0.14 (0.06–0.45) | 0.18 (0.06–0.46) | 0.17 (0.04–0.34) | 0.519 |
| Urine volume (mL/day) | 0 (0–500) | 0 (0–310) | 355 (0–1200) a,b | 0.001 |
| DP4Cr | 0.69 ± 0.16 | 0.64 ± 0.11 | 0.65 ± 0.12 | 0.509 |
| Phosphorus (mg/dL) | 4.7 ± 1.4 | 5.0 ± 1.3 | 5.0 ± 1.5 | 0.597 |
| Calcium (mg/dL) | 8.3 ± 0.9 | 8.3 ± 1.0 | 8.3 ± 1.0 | 0.980 |
| Potassium (mEq/L) | 4.5 ± 0.8 | 4.6 ± 0.6 | 4.6 ± 0.6 | 0.432 |
| Sodium (mEq/L) | 137 (134–139) | 136 (134–139) | 137 (134–139) | 0.615 |
| Albumin (g/dL) | 3.3 ± 0.5 | 3.6 ± 0.4 a | 3.8 ± 0.4 a,b | <0.001 |
| nPNA (g/kg/day) | 0.78 ± 0.21 | 0.85 ± 0.23 | 0.88 ± 0.17 a | 0.028 |
| Alkaline phosphatase (IU/L) | 109 (86–148) | 112 (76–148) | 102 (76–135) | 0.147 |
| Intact parathyroid hormone (pg/mL) | 269 (126–431) | 285 (152–438) | 314 (176–555) | 0.235 |
| Duration of follow-up (months) | 41 (12–86) | 55 (16–90) | 59 (37–96) | 0.241 |
| Patient Survival | Technique Survival | |||||||
|---|---|---|---|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | |||||
| HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | HR (95% CI) | p | |
| Tertile of PhA (decrease 1 tertile) | 3.25 (1.81–5.84) | <0.001 | 2.48 (1.32–4.66) | 0.005 | 1.88 (1.28–2.77) | 0.001 | 1.42 (0.92–2.17) | 0.100 |
| Age (ref: <65 years) | 4.16 (2.00–8.62) | <0.001 | 3.60 (1.72–7.55) | 0.001 | 2.60 (1.43–4.73) | 0.002 | 2.31 (1.26–4.22) | 0.007 |
| Sex (ref: male) | 1.71 (0.82–3.56) | 0.150 | 1.15 (0.64–2.06) | 0.640 | ||||
| BMI (increased 1 kg/m2) | 1.03 (0.94–1.12) | 0.586 | 1.01 (0.94–1.09) | 0.772 | ||||
| UV (increase 1 mL/day) | 1.00 (1.00–1.00) | 0.112 | 1.00 (1.00–1.00) | 0.158 | ||||
| Albumin (increase 1 g/dL) | 0.36 (0.19–0.69) | 0.002 | 0.68 (0.34–1.37) | 0.281 | 0.41 (0.24–0.70) | 0.001 | 0.60 (0.33–1.06) | 0.077 |
| nPNA (increase 1 g/kg/day) | 0.28 (0.05–1.77) | 0.177 | 0.62 (0.15–2.65) | 0.523 | ||||
| Davies risk index (increase 1 grade) | 2.45 (1.35–4.46) | 0.003 | 2.01 (1.10–3.65) | 0.023 | 1.95 (1.21–3.14) | 0.006 | 1.63 (1.00–2.65) | 0.051 |
| Models | AUC | Difference between AUCs | Relative IDI | Category-Free NRI | ||
|---|---|---|---|---|---|---|
| Values | Values | p-Value | Values | p-Value | ||
| Patient death | ||||||
| Multivariate model | 0.79 | – | – | – | – | |
| Multivariate model with PhA | 0.85 | 0.05 | 0.56 | 0.010 | 0.58 | 0.004 |
| Technique failure | ||||||
| Multivariate model | 0.71 | – | – | – | – | |
| Multivariate model with PhA | 0.73 | 0.02 | 0.19 | 0.051 | 0.28 | 0.090 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, S.-H.; Do, J.-Y. Phase Angle as a Risk Factor for Mortality in Patients Undergoing Peritoneal Dialysis. Nutrients 2023, 15, 4991. https://doi.org/10.3390/nu15234991
Kang S-H, Do J-Y. Phase Angle as a Risk Factor for Mortality in Patients Undergoing Peritoneal Dialysis. Nutrients. 2023; 15(23):4991. https://doi.org/10.3390/nu15234991
Chicago/Turabian StyleKang, Seok-Hui, and Jun-Young Do. 2023. "Phase Angle as a Risk Factor for Mortality in Patients Undergoing Peritoneal Dialysis" Nutrients 15, no. 23: 4991. https://doi.org/10.3390/nu15234991
APA StyleKang, S.-H., & Do, J.-Y. (2023). Phase Angle as a Risk Factor for Mortality in Patients Undergoing Peritoneal Dialysis. Nutrients, 15(23), 4991. https://doi.org/10.3390/nu15234991