
Food Intake and Sleep Disorders in Children and Adolescents with Obesity

 , , ,
, , , 
Abstract
1. Introduction
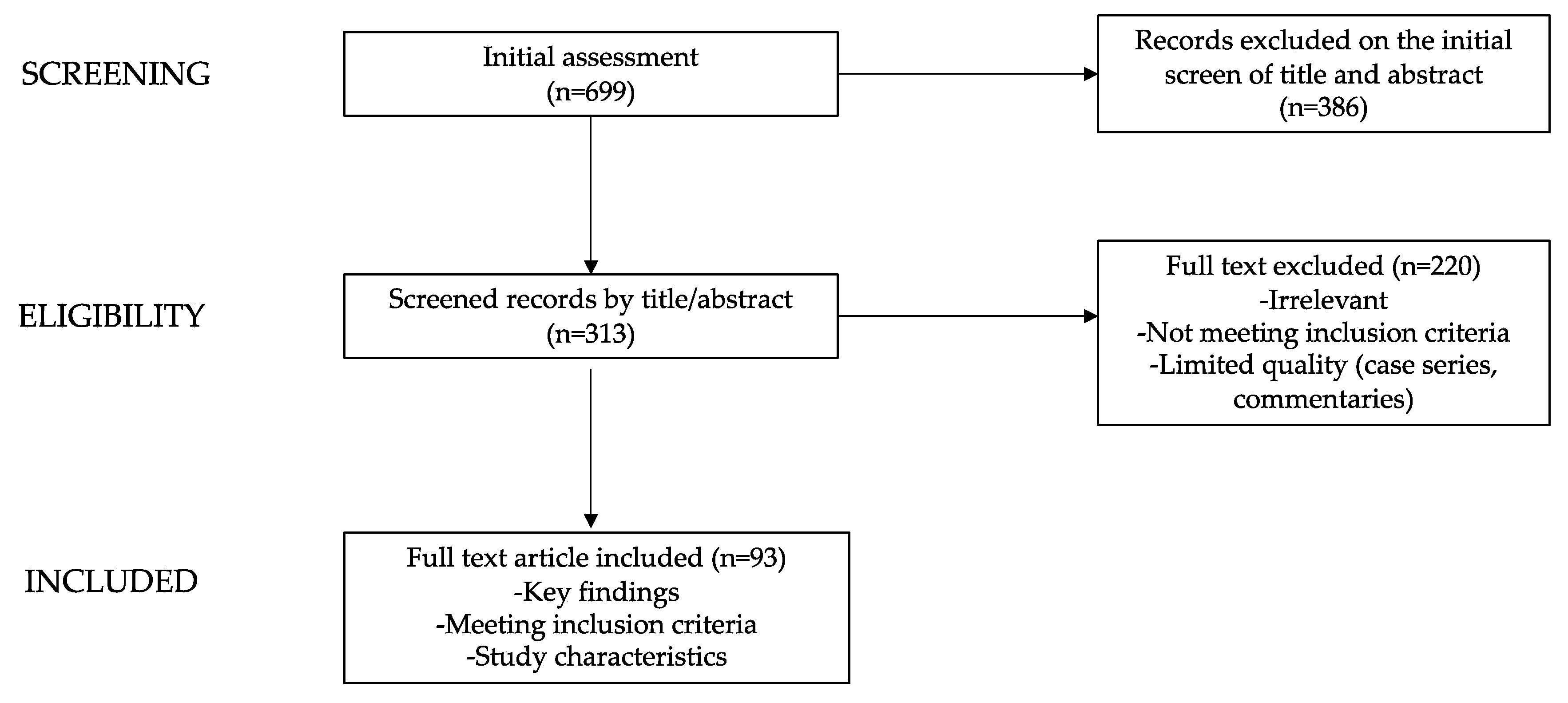
2. Methods
3. Sleep Disturbances and Their Connection to Pediatric Obesity
3.1. Sleep and Overall Well-Being
3.2. Determinants in Disordered Sleep and Obesity
4. Sleep Disorders in Children and Adolescents with Obesity
4.1. Sleep Deprivation in Pediatric Obesity
4.2. Sleep-Disordered Breathing in Pediatric Obesity
5. Dietary Patterns and Sleep Disorders in Pediatric Obesity
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Jebeile, H.; Kelly, A.S.; O’Malley, G.; Baur, L.A. Obesity in Children and Adolescents: Epidemiology, Causes, Assessment, and Management. Lancet Diabetes Endocrinol. 2022, 10, 351–365. [Google Scholar] [CrossRef]
- Woolford, S.J.; Sidell, M.; Li, X.; Else, V.; Young, D.R.; Resnicow, K.; Koebnick, C. Changes in Body Mass Index among Children and Adolescents during the COVID-19 Pandemic. JAMA 2021, 326, 1434. [Google Scholar] [CrossRef]
- Lee, E.Y.; Yoon, K.-H. Epidemic Obesity in Children and Adolescents: Risk Factors and Prevention. Front. Med. 2018, 12, 658–666. [Google Scholar] [CrossRef] [PubMed]
- Koyuncuoğlu Güngör, N. Overweight and Obesity in Children and Adolescents. J. Clin. Res. Pediatr. Endocrinol. 2014, 6, 129–143. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.L.; Lumeng, J.C.; LeBourgeois, M.K. Sleep Patterns and Obesity in Childhood. Curr. Opin. Endocrinol. Diabetes Obes. 2015, 22, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Sluggett, L.; Wagner, S.L.; Harris, R.L. Sleep Duration and Obesity in Children and Adolescents. Can. J. Diabetes 2019, 43, 146–152. [Google Scholar] [CrossRef]
- Paruthi, S.; Brooks, L.J.; D’Ambrosio, C.; Hall, W.A.; Kotagal, S.; Lloyd, R.M.; Malow, B.A.; Maski, K.; Nichols, C.; Quan, S.F.; et al. Recommended Amount of Sleep for Pediatric Populations: A Consensus Statement of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2016, 12, 785–786. [Google Scholar] [CrossRef]
- Felső, R.; Lohner, S.; Hollódy, K.; Erhardt, É.; Molnár, D. Relationship between Sleep Duration and Childhood Obesity: Systematic Review Including the Potential Underlying Mechanisms. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 751–761. [Google Scholar] [CrossRef]
- Hart, C.N.; Carskadon, M.A.; Considine, R.V.; Fava, J.L.; Lawton, J.; Raynor, H.A.; Jelalian, E.; Owens, J.; Wing, R. Changes in Children’s Sleep Duration on Food Intake, Weight, and Leptin. Pediatrics 2013, 132, e1473–e1480. [Google Scholar] [CrossRef]
- Bonanno, L.; Metro, D.; Papa, M.; Finzi, G.; Maviglia, A.; Sottile, F.; Corallo, F.; Manasseri, L. Assessment of Sleep and Obesity in Adults and Children: Observational Study. Medicine 2019, 98, e17642. [Google Scholar] [CrossRef]
- Kumar, S.; Kelly, A.S. Review of Childhood Obesity. Mayo Clin. Proc. 2017, 92, 251–265. [Google Scholar] [CrossRef] [PubMed]
- Zarpellon, R.S.M.; Vilela, D.R.M.; Louzada, F.M.; Radominski, D.R.B.; Crippa, D.A.C.d.S. Association of Food Intake with Sleep Disorders in Children and Adolescents with Obesity. Sleep Med. X 2022, 4, 100053. [Google Scholar] [CrossRef]
- St-Onge, M.-P.; Mikic, A.; Pietrolungo, C.E. Effects of Diet on Sleep Quality. Adv. Nutr. 2016, 7, 938–949. [Google Scholar] [CrossRef] [PubMed]
- Mallampalli, M.P.; Carter, C.L. Exploring Sex and Gender Differences in Sleep Health: A Society for Women’s Health Research Report. J. Womens Health 2014, 23, 553–562. [Google Scholar] [CrossRef]
- Morrissey, B.; Taveras, E.; Allender, S.; Strugnell, C. Sleep and Obesity among Children: A Systematic Review of Multiple Sleep Dimensions. Pediatr. Obes. 2020, 15, e12619. [Google Scholar] [CrossRef] [PubMed]
- Taheri, S. The Link between Short Sleep Duration and Obesity: We Should Recommend More Sleep to Prevent Obesity. Arch. Dis. Child. 2006, 91, 881–884. [Google Scholar] [CrossRef]
- Holliday, E.G.; Magee, C.A.; Kritharides, L.; Banks, E.; Attia, J. Short Sleep Duration Is Associated with Risk of Future Diabetes but Not Cardiovascular Disease: A Prospective Study and Meta-Analysis. PLoS ONE 2013, 8, e82305. [Google Scholar] [CrossRef]
- Sabanayagam, C.; Shankar, A. Sleep Duration and Cardiovascular Disease: Results from the National Health Interview Survey. Sleep 2010, 33, 1037–1042. [Google Scholar] [CrossRef]
- Grandner, M.A.; Hale, L.; Moore, M.; Patel, N.P. Mortality Associated with Short Sleep Duration: The Evidence, the Possible Mechanisms, and the Future. Sleep Med. Rev. 2010, 14, 191–203. [Google Scholar] [CrossRef]
- Van Cauter, E.; Knutson, K.L. Sleep and the Epidemic of Obesity in Children and Adults. Eur. J. Endocrinol. 2008, 159, S59–S66. [Google Scholar] [CrossRef]
- Garaulet, M.; Ortega, F.B.; Ruiz, J.R.; Rey-López, J.P.; Béghin, L.; Manios, Y.; Cuenca-García, M.; Plada, M.; Diethelm, K.; Kafatos, A.; et al. Short Sleep Duration Is Associated with Increased Obesity Markers in European Adolescents: Effect of Physical Activity and Dietary Habits. The HELENA Study. Int. J. Obes. 2011, 35, 1308–1317. [Google Scholar] [CrossRef]
- Patel, S.R.; Hu, F.B. Short Sleep Duration and Weight Gain: A Systematic Review. Obesity 2008, 16, 643–653. [Google Scholar] [CrossRef]
- Spiegel, K.; Tasali, E.; Penev, P.; Van Cauter, E. Brief Communication: Sleep Curtailment in Healthy Young Men Is Associated with Decreased Leptin Levels, Elevated Ghrelin Levels, and Increased Hunger and Appetite. Ann. Intern. Med. 2004, 141, 846–850. [Google Scholar] [CrossRef] [PubMed]
- Landhuis, C.E.; Poulton, R.; Welch, D.; Hancox, R.J. Childhood Sleep Time and Long-Term Risk for Obesity: A 32-Year Prospective Birth Cohort Study. Pediatrics 2008, 122, 955–960. [Google Scholar] [CrossRef]
- Wing, Y.K.; Li, S.X.; Li, A.M.; Zhang, J.; Kong, A.P.S. The Effect of Weekend and Holiday Sleep Compensation on Childhood Overweight and Obesity. Pediatrics 2009, 124, e994–e1000. [Google Scholar] [CrossRef]
- Kim, T.W.; Jeong, J.-H.; Hong, S.-C. The Impact of Sleep and Circadian Disturbance on Hormones and Metabolism. Int. J. Endocrinol. 2015, 2015, 591729. [Google Scholar] [CrossRef] [PubMed]
- Chasens, E.R.; Sereika, S.M.; Weaver, T.E.; Umlauf, M.G. Daytime Sleepiness, Exercise, and Physical Function in Older Adults. J. Sleep Res. 2007, 16, 60–65. [Google Scholar] [CrossRef] [PubMed]
- Gaina, A.; Sekine, M.; Hamanishi, S.; Chen, X.; Wang, H.; Yamagami, T.; Kagamimori, S. Daytime Sleepiness and Associated Factors in Japanese School Children. J. Pediatr. 2007, 151, 518–522.e4. [Google Scholar] [CrossRef]
- Spiegel, K.; Leproult, R.; Colecchia, E.F.; L’Hermite-Balériaux, M.; Nie, Z.; Copinschi, G.; Van Cauter, E. Adaptation of the 24-h Growth Hormone Profile to a State of Sleep Debt. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2000, 279, R874–R883. [Google Scholar] [CrossRef]
- Spiegel, K.; Leproult, R.; Van Cauter, E. Impact of sleep debt on physiological rhythms. Rev. Neurol. 2003, 159, 6S11-20. [Google Scholar] [PubMed]
- Penev, P.; Spiegel, K.; L’Hermite-Balériaux, M.; Schneider, R.; Van Cauter, E. Relationship between REM Sleep and Testosterone Secretion in Older Men. Ann. Endocrinol. 2003, 64, 157. [Google Scholar]
- Dashti, H.S.; Follis, J.L.; Smith, C.E.; Tanaka, T.; Cade, B.E.; Gottlieb, D.J.; Hruby, A.; Jacques, P.F.; Lamon-Fava, S.; Richardson, K.; et al. Habitual Sleep Duration Is Associated with BMI and Macronutrient Intake and May Be Modified by CLOCK Genetic Variants. Am. J. Clin. Nutr. 2015, 101, 135–143. [Google Scholar] [CrossRef]
- Jansen, E.C.; Peterson, K.E.; Lumeng, J.C.; Kaciroti, N.; LeBourgeois, M.K.; Chen, K.; Miller, A.L. Associations between Sleep and Dietary Patterns among Low-Income Children Attending Preschool. J. Acad. Nutr. Diet. 2019, 119, 1176–1187. [Google Scholar] [CrossRef] [PubMed]
- Scheer, F.A.J.L.; Hilton, M.F.; Mantzoros, C.S.; Shea, S.A. Adverse Metabolic and Cardiovascular Consequences of Circadian Misalignment. Proc. Natl. Acad. Sci. USA 2009, 106, 4453–4458. [Google Scholar] [CrossRef] [PubMed]
- Morin, V.; Hozer, F.; Costemale-Lacoste, J.-F. The Effects of Ghrelin on Sleep, Appetite, and Memory, and Its Possible Role in Depression: A Review of the Literature. L’Encephale 2018, 44, 256–263. [Google Scholar] [CrossRef]
- Peuhkuri, K.; Sihvola, N.; Korpela, R. Diet Promotes Sleep Duration and Quality. Nutr. Res. 2012, 32, 309–319. [Google Scholar] [CrossRef]
- Hermes, F.N.; Nunes, E.E.M.; de Melo, C.M. Sleep, Nutritional Status and Eating Behavior in Children: A Review Study. Rev. Paul. Pediatr. 2022, 40, e2020479. [Google Scholar] [CrossRef]
- Chaput, J.-P.; Katzmarzyk, P.T.; LeBlanc, A.G.; Tremblay, M.S.; Barreira, T.V.; Broyles, S.T.; Fogelholm, M.; Hu, G.; Kuriyan, R.; Kurpad, A.; et al. Associations between Sleep Patterns and Lifestyle Behaviors in Children: An International Comparison. Int. J. Obes. Suppl. 2015, 5, S59–S65. [Google Scholar] [CrossRef]
- Harrington, S.A. Relationships of Objectively Measured Physical Activity and Sleep with BMI and Academic Outcomes in 8-Year-Old Children. Appl. Nurs. Res. 2013, 26, 63–70. [Google Scholar] [CrossRef]
- Williams, S.M.; Farmer, V.L.; Taylor, B.J.; Taylor, R.W. Do More Active Children Sleep More? A Repeated Cross-Sectional Analysis Using Accelerometry. PLoS ONE 2014, 9, e93117. [Google Scholar] [CrossRef]
- Gomes, T.N.; Dos Santos, F.K.; Santos, D.; Pereira, S.; Chaves, R.; Katzmarzyk, P.T.; Maia, J. Correlates of Sedentary Time in Children: A Multilevel Modelling Approach. BMC Public Health 2014, 14, 890. [Google Scholar] [CrossRef] [PubMed]
- Ward, A.L.; Galland, B.C.; Haszard, J.J.; Meredith-Jones, K.; Morrison, S.; McIntosh, D.R.; Jackson, R.; Beebe, D.W.; Fangupo, L.; Richards, R.; et al. The Effect of Mild Sleep Deprivation on Diet and Eating Behaviour in Children: Protocol for the Daily Rest, Eating, and Activity Monitoring (DREAM) Randomized Cross-over Trial. BMC Public Health 2019, 19, 1347. [Google Scholar] [CrossRef] [PubMed]
- Marinelli, M.; Pappa, I.; Bustamante, M.; Bonilla, C.; Suarez, A.; Tiesler, C.M.; Vilor-Tejedor, N.; Zafarmand, M.H.; Alvarez-Pedrerol, M.; Andersson, S.; et al. Heritability and Genome-Wide Association Analyses of Sleep Duration in Children: The EAGLE Consortium. Sleep 2016, 39, 1859–1869. [Google Scholar] [CrossRef] [PubMed]
- Watson, N.F.; Harden, K.P.; Buchwald, D.; Vitiello, M.V.; Pack, A.I.; Weigle, D.S.; Goldberg, J. Sleep Duration and Body Mass Index in Twins: A Gene-Environment Interaction. Sleep 2012, 35, 597–603. [Google Scholar] [CrossRef]
- Tauman, R.; Gozal, D. Obesity and Obstructive Sleep Apnea in Children. Paediatr. Respir. Rev. 2006, 7, 247–259. [Google Scholar] [CrossRef]
- Bhattacharjee, R.; Kim, J.; Kheirandish-Gozal, L.; Gozal, D. Obesity and Obstructive Sleep Apnea Syndrome in Children: A Tale of Inflammatory Cascades. Pediatr. Pulmonol. 2011, 46, 313–323. [Google Scholar] [CrossRef]
- Fatima, Y.; Doi, S.a.R.; Mamun, A.A. Longitudinal Impact of Sleep on Overweight and Obesity in Children and Adolescents: A Systematic Review and Bias-Adjusted Meta-Analysis. Obes. Rev. 2015, 16, 137–149. [Google Scholar] [CrossRef]
- Su, M.-S.; Zhang, H.-L.; Cai, X.-H.; Lin, Y.; Liu, P.-N.; Zhang, Y.-B.; Hu, W.-Z.; Li, C.-C.; Xiao, Y.-F. Obesity in Children with Different Risk Factors for Obstructive Sleep Apnea: A Community-Based Study. Eur. J. Pediatr. 2016, 175, 211–220. [Google Scholar] [CrossRef]
- Snell, E.K.; Adam, E.K.; Duncan, G.J. Sleep and the Body Mass Index and Overweight Status of Children and Adolescents. Child Dev. 2007, 78, 309–323. [Google Scholar] [CrossRef]
- Touchette, E.; Petit, D.; Tremblay, R.E.; Boivin, M.; Falissard, B.; Genolini, C.; Montplaisir, J.Y. Associations between Sleep Duration Patterns and Overweight/Obesity at Age 6. Sleep 2008, 31, 1507–1514. [Google Scholar] [CrossRef]
- Nixon, G.M.; Thompson, J.M.D.; Han, D.Y.; Becroft, D.M.; Clark, P.M.; Robinson, E.; Waldie, K.E.; Wild, C.J.; Black, P.N.; Mitchell, E.A. Short Sleep Duration in Middle Childhood: Risk Factors and Consequences. Sleep 2008, 31, 71–78. [Google Scholar] [CrossRef]
- Yu, Y.; Lu, B.S.; Wang, B.; Wang, H.; Yang, J.; Li, Z.; Wang, L.; Liu, X.; Tang, G.; Xing, H.; et al. Short Sleep Duration and Adiposity in Chinese Adolescents. Sleep 2007, 30, 1688–1697. [Google Scholar] [CrossRef]
- Hitze, B.; Bosy-Westphal, A.; Bielfeldt, F.; Settler, U.; Plachta-Danielzik, S.; Pfeuffer, M.; Schrezenmeir, J.; Mönig, H.; Müller, M.J. Determinants and Impact of Sleep Duration in Children and Adolescents: Data of the Kiel Obesity Prevention Study. Eur. J. Clin. Nutr. 2009, 63, 739–746. [Google Scholar] [CrossRef] [PubMed]
- Eisenmann, J.C.; Ekkekakis, P.; Holmes, M. Sleep Duration and Overweight among Australian Children and Adolescents. Acta Paediatr. 2006, 95, 956–963. [Google Scholar] [CrossRef] [PubMed]
- Scharf, R.J.; DeBoer, M.D. Sleep Timing and Longitudinal Weight Gain in 4- and 5-Year-Old Children. Pediatr. Obes. 2015, 10, 141–148. [Google Scholar] [CrossRef]
- Boergers, J.; Gable, C.J.; Owens, J.A. Later School Start Time Is Associated with Improved Sleep and Daytime Functioning in Adolescents. J. Dev. Behav. Pediatr. JDBP 2014, 35, 11–17. [Google Scholar] [CrossRef]
- Jarrin, D.C.; McGrath, J.J.; Drake, C.L. Beyond Sleep Duration: Distinct Sleep Dimensions Are Associated with Obesity in Children and Adolescents. Int. J. Obes. 2013, 37, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Busto-Zapico, R.; Amigo-Vázquez, I.; Peña-Suárez, E.; Fernández-Rodríguez, C. Relationships between Sleeping Habits, Sedentary Leisure Activities and Childhood Overweight and Obesity. Psychol. Health Med. 2014, 19, 667–672. [Google Scholar] [CrossRef]
- Sijtsma, A.; Koller, M.; Sauer, P.J.J.; Corpeleijn, E. Television, Sleep, Outdoor Play and BMI in Young Children: The GECKO Drenthe Cohort. Eur. J. Pediatr. 2015, 174, 631–639. [Google Scholar] [CrossRef] [PubMed]
- Consensus Conference Panel; Watson, N.F.; Badr, M.S.; Belenky, G.; Bliwise, D.L.; Buxton, O.M.; Buysse, D.; Dinges, D.F.; Gangwisch, J.; Grandner, M.A.; et al. Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society on the Recommended Amount of Sleep for a Healthy Adult: Methodology and Discussion. J. Clin. Sleep Med. 2015, 11, 931–952. [Google Scholar] [CrossRef] [PubMed]
- Thivel, D.; Isacco, L.; Aucouturier, J.; Pereira, B.; Lazaar, N.; Ratel, S.; Doré, E.; Duché, P. Bedtime and Sleep Timing but Not Sleep Duration Are Associated with Eating Habits in Primary School Children. J. Dev. Behav. Pediatr. JDBP 2015, 36, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Bagley, E.J.; El-Sheikh, M. Relations between Daytime Pre-Ejection Period Reactivity and Sleep in Late Childhood. J. Sleep Res. 2014, 23, 335–338. [Google Scholar] [CrossRef] [PubMed]
- Hart, C.N.; Cairns, A.; Jelalian, E. Sleep and Obesity in Children and Adolescents. Pediatr. Clin. N. Am. 2011, 58, 715–733. [Google Scholar] [CrossRef]
- Roche, J.; Corgosinho, F.C.; Dâmaso, A.R.; Isacco, L.; Miguet, M.; Fillon, A.; Guyon, A.; Moreira, G.A.; Pradella-Hallinan, M.; Tufik, S.; et al. Sleep-Disordered Breathing in Adolescents with Obesity: When Does It Start to Affect Cardiometabolic Health? Nutr. Metab. Cardiovasc. Dis. NMCD 2020, 30, 683–693. [Google Scholar] [CrossRef]
- Kalra, M.; Inge, T.; Garcia, V.; Daniels, S.; Lawson, L.; Curti, R.; Cohen, A.; Amin, R. Obstructive Sleep Apnea in Extremely Overweight Adolescents Undergoing Bariatric Surgery. Obes. Res. 2005, 13, 1175–1179. [Google Scholar] [CrossRef]
- Grime, C.; Tan, H. Sleep Disordered Breathing in Children. Indian J. Pediatr. 2015, 82, 945–955. [Google Scholar] [CrossRef]
- Canapari, C.A.; Hoppin, A.G.; Kinane, T.B.; Thomas, B.J.; Torriani, M.; Katz, E.S. Relationship between Sleep Apnea, Fat Distribution, and Insulin Resistance in Obese Children. J. Clin. Sleep Med. 2011, 7, 268–273. [Google Scholar] [CrossRef]
- Arens, R.; Sin, S.; Nandalike, K.; Rieder, J.; Khan, U.I.; Freeman, K.; Wylie-Rosett, J.; Lipton, M.L.; Wootton, D.M.; McDonough, J.M.; et al. Upper Airway Structure and Body Fat Composition in Obese Children with Obstructive Sleep Apnea Syndrome. Am. J. Respir. Crit. Care Med. 2011, 183, 782–787. [Google Scholar] [CrossRef] [PubMed]
- Marcus, C.L.; Brooks, L.J.; Draper, K.A.; Gozal, D.; Halbower, A.C.; Jones, J.; Schechter, M.S.; Sheldon, S.H.; Spruyt, K.; Ward, S.D.; et al. Diagnosis and Management of Childhood Obstructive Sleep Apnea Syndrome. Pediatrics 2012, 130, 576–584. [Google Scholar] [CrossRef]
- Scholle, S.; Wiater, A.; Scholle, H.C. Normative Values of Polysomnographic Parameters in Childhood and Adolescence: Arousal Events. Sleep Med. 2012, 13, 243–251. [Google Scholar] [CrossRef] [PubMed]
- Chamorro, R.; Algarín, C.; Garrido, M.; Causa, L.; Held, C.; Lozoff, B.; Peirano, P. Night Time Sleep Macrostructure Is Altered in Otherwise Healthy 10-Year-Old Overweight Children. Int. J. Obes. 2014, 38, 1120–1125. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Olson, C.A.; Hamilton, N.A.; Somers, V.K. Percentage of REM Sleep Is Associated with Overnight Change in Leptin. J. Sleep Res. 2016, 25, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Skjåkødegård, H.F.; Danielsen, Y.S.; Frisk, B.; Hystad, S.W.; Roelants, M.; Pallesen, S.; Conlon, R.P.K.; Wilfley, D.E.; Juliusson, P.B. Beyond Sleep Duration: Sleep Timing as a Risk Factor for Childhood Obesity. Pediatr. Obes. 2021, 16, e12698. [Google Scholar] [CrossRef] [PubMed]
- Polak, J.; Shimoda, L.A.; Drager, L.F.; Undem, C.; McHugh, H.; Polotsky, V.Y.; Punjabi, N.M. Intermittent Hypoxia Impairs Glucose Homeostasis in C57BL6/J Mice: Partial Improvement with Cessation of the Exposure. Sleep 2013, 36, 1483–1490. [Google Scholar] [CrossRef] [PubMed]
- Ota, H.; Tamaki, S.; Itaya-Hironaka, A.; Yamauchi, A.; Sakuramoto-Tsuchida, S.; Morioka, T.; Takasawa, S.; Kimura, H. Attenuation of Glucose-Induced Insulin Secretion by Intermittent Hypoxia via down-Regulation of CD38. Life Sci. 2012, 90, 206–211. [Google Scholar] [CrossRef]
- Makar, A.B.; McMartin, K.E.; Palese, M.; Tephly, T.R. Formate Assay in Body Fluids: Application in Methanol Poisoning. Biochem. Med. 1975, 13, 117–126. [Google Scholar] [CrossRef]
- DeBoer, M.D. Obesity, Systemic Inflammation, and Increased Risk for Cardiovascular Disease and Diabetes among Adolescents: A Need for Screening Tools to Target Interventions. Nutrition 2013, 29, 379–386. [Google Scholar] [CrossRef]
- Wilson, K.; St-Onge, M.-P.; Tasali, E. Diet Composition and Objectively Assessed Sleep Quality: A Narrative Review. J. Acad. Nutr. Diet. 2022, 122, 1182–1195. [Google Scholar] [CrossRef]
- Weiss, A.; Xu, F.; Storfer-Isser, A.; Thomas, A.; Ievers-Landis, C.E.; Redline, S. The Association of Sleep Duration with Adolescents’ Fat and Carbohydrate Consumption. Sleep 2010, 33, 1201–1209. [Google Scholar] [CrossRef]
- Imaki, M.; Hatanaka, Y.; Ogawa, Y.; Yoshida, Y.; Tanada, S. An Epidemiological Study on Relationship between the Hours of Sleep and Life Style Factors in Japanese Factory Workers. J. Physiol. Anthropol. Appl. Human Sci. 2002, 21, 115–120. [Google Scholar] [CrossRef]
- Shechter, A.; O’Keeffe, M.; Roberts, A.L.; Zammit, G.K.; RoyChoudhury, A.; St-Onge, M.-P. Alterations in Sleep Architecture in Response to Experimental Sleep Curtailment Are Associated with Signs of Positive Energy Balance. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 2012, 303, R883–R889. [Google Scholar] [CrossRef]
- Godos, J.; Grosso, G.; Castellano, S.; Galvano, F.; Caraci, F.; Ferri, R. Association between Diet and Sleep Quality: A Systematic Review. Sleep Med. Rev. 2021, 57, 101430. [Google Scholar] [CrossRef]
- Grandner, M.A.; Kripke, D.F.; Naidoo, N.; Langer, R.D. Relationships among Dietary Nutrients and Subjective Sleep, Objective Sleep, and Napping in Women. Sleep Med. 2010, 11, 180–184. [Google Scholar] [CrossRef]
- Tanaka, E.; Yatsuya, H.; Uemura, M.; Murata, C.; Otsuka, R.; Toyoshima, H.; Tamakoshi, K.; Sasaki, S.; Kawaguchi, L.; Aoyama, A. Associations of Protein, Fat, and Carbohydrate Intakes with Insomnia Symptoms among Middle-Aged Japanese Workers. J. Epidemiol. 2013, 23, 132–138. [Google Scholar] [CrossRef] [PubMed]
- Holmes, J.F.; St. Laurent, C.W.; Spencer, R.M.C. Unhealthy Diet Is Associated with Poor Sleep in Preschool-Aged Children. J. Genet. Psychol. 2021, 182, 289–303. [Google Scholar] [CrossRef]
- Tomanic, M.; Paunovic, K.; Lackovic, M.; Djurdjevic, K.; Nestorovic, M.; Jakovljevic, A.; Markovic, M. Energy Drinks and Sleep among Adolescents. Nutrients 2022, 14, 3813. [Google Scholar] [CrossRef]
- Spaeth, A.M.; Hawley, N.L.; Raynor, H.A.; Jelalian, E.; Greer, A.; Crouter, S.E.; Coffman, D.L.; Carskadon, M.A.; Owens, J.A.; Wing, R.R.; et al. Sleep, Energy Balance, and Meal Timing in School-Aged Children. Sleep Med. 2019, 60, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Golley, R.K.; Maher, C.A.; Matricciani, L.; Olds, T.S. Sleep Duration or Bedtime? Exploring the Association between Sleep Timing Behaviour, Diet and BMI in Children and Adolescents. Int. J. Obes. 2013, 37, 546–551. [Google Scholar] [CrossRef] [PubMed]
- King, C. Soft Drinks Consumption and Child Behaviour Problems: The Role of Food Insecurity and Sleep Patterns. Public Health Nutr. 2017, 20, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Na, M.; Eagleton, S.G.; Jomaa, L.; Lawton, K.; Savage, J.S. Food Insecurity Is Associated with Suboptimal Sleep Quality, but Not Sleep Duration, among Low-Income Head Start Children of Pre-School Age. Public Health Nutr. 2020, 23, 701–710. [Google Scholar] [CrossRef] [PubMed]
- de Jong, E.; Stocks, T.; Visscher, T.L.S.; HiraSing, R.A.; Seidell, J.C.; Renders, C.M. Association between Sleep Duration and Overweight: The Importance of Parenting. Int. J. Obes. 2012, 36, 1278–1284. [Google Scholar] [CrossRef]
- Kordas, K.; Casavantes, K.M.; Mendoza, C.; Lopez, P.; Ronquillo, D.; Rosado, J.L.; Vargas, G.G.; Stoltzfus, R.J. The Association between Lead and Micronutrient Status, and Children’s Sleep, Classroom Behavior, and Activity. Arch. Environ. Occup. Health 2007, 62, 105–112. [Google Scholar] [CrossRef]
- Landis, A.M.; Parker, K.P.; Dunbar, S.B. Sleep, Hunger, Satiety, Food Cravings, and Caloric Intake in Adolescents. J. Nurs. Scholarsh. 2009, 41, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Westerlund, L.; Ray, C.; Roos, E. Associations between Sleeping Habits and Food Consumption Patterns among 10-11-Year-Old Children in Finland. Br. J. Nutr. 2009, 102, 1531–1537. [Google Scholar] [CrossRef]
- Khan, M.K.A.; Faught, E.L.; Chu, Y.L.; Ekwaru, J.P.; Storey, K.E.; Veugelers, P.J. Is It Nutrients, Food Items, Diet Quality or Eating Behaviours That Are Responsible for the Association of Children’s Diet with Sleep? J. Sleep Res. 2017, 26, 468–476. [Google Scholar] [CrossRef]
- Min, C.; Kim, H.-J.; Park, I.-S.; Park, B.; Kim, J.-H.; Sim, S.; Choi, H.G. The Association between Sleep Duration, Sleep Quality, and Food Consumption in Adolescents: A Cross-Sectional Study Using the Korea Youth Risk Behavior Web-Based Survey. BMJ Open 2018, 8, e022848. [Google Scholar] [CrossRef] [PubMed]
- Kjeldsen, J.S.; Hjorth, M.F.; Andersen, R.; Michaelsen, K.F.; Tetens, I.; Astrup, A.; Chaput, J.-P.; Sjödin, A. Short Sleep Duration and Large Variability in Sleep Duration Are Independently Associated with Dietary Risk Factors for Obesity in Danish School Children. Int. J. Obes. 2014, 38, 32–39. [Google Scholar] [CrossRef]
- Córdova, F.V.; Barja, S.; Brockmann, P.E. Consequences of Short Sleep Duration on the Dietary Intake in Children: A Systematic Review and Metanalysis. Sleep Med. Rev. 2018, 42, 68–84. [Google Scholar] [CrossRef] [PubMed]
- Tatone-Tokuda, F.; Dubois, L.; Ramsay, T.; Girard, M.; Touchette, E.; Petit, D.; Montplaisir, J.Y. Sex Differences in the Association between Sleep Duration, Diet and Body Mass Index: A Birth Cohort Study: Sleep, Diet and BMI. J. Sleep Res. 2012, 21, 448–460. [Google Scholar] [CrossRef]
- Franckle, R.L.; Falbe, J.; Gortmaker, S.; Ganter, C.; Taveras, E.M.; Land, T.; Davison, K.K. Insufficient Sleep among Elementary and Middle School Students Is Linked with Elevated Soda Consumption and Other Unhealthy Dietary Behaviors. Prev. Med. 2015, 74, 36–41. [Google Scholar] [CrossRef]
- Ramírez-Contreras, C.; Santamaría-Orleans, A.; Izquierdo-Pulido, M.; Zerón-Rugerio, M.F. Sleep Dimensions Are Associated with Obesity, Poor Diet Quality and Eating Behaviors in School-Aged Children. Front. Nutr. 2022, 9, 959503. [Google Scholar] [CrossRef] [PubMed]
- Agostini, A.; Lushington, K.; Kohler, M.; Dorrian, J. Associations between Self-reported Sleep Measures and Dietary Behaviours in a Large Sample of Australian School Students (n = 28,010). J. Sleep Res. 2018, 27, e12682. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, G.P.; Mota, M.C.; Crispim, C.A. Eveningness Is Associated with Skipping Breakfast and Poor Nutritional Intake in Brazilian Undergraduate Students. Chronobiol. Int. 2018, 35, 358–367. [Google Scholar] [CrossRef]
- Kawai, M. Disruption of the Circadian Rhythms and Its Relationship with Pediatric Obesity. Pediatr. Int. 2022, 64, e14992. [Google Scholar] [CrossRef] [PubMed]
- Plancoulaine, S.; Reynaud, E.; Forhan, A.; Lioret, S.; Heude, B.; Charles, M.-A.; Annesi-Maesano, I.; Bernard, J.Y.; Botton, J.; Charles, M.A.; et al. Night Sleep Duration Trajectories and Associated Factors among Preschool Children from the EDEN Cohort. Sleep Med. 2018, 48, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Ríos-Hernández, A.; Gilchrist, C.; Chelimo, C.; Castro, T.G.; Izquierdo-Pulido, M.; Wall, C.; Thabrew, H.; Berry, S.; Morton, S.; Grant, C. The Relationship between Diet and Sleep in 2-y-Old Children: Results from Growing Up in New Zealand. Nutrition 2022, 95, 111560. [Google Scholar] [CrossRef]
- Stifter, C.A.; Anzman-Frasca, S.; Birch, L.L.; Voegtline, K. Parent Use of Food to Soothe Infant/Toddler Distress and Child Weight Status. An Exploratory Study. Appetite 2011, 57, 693–699. [Google Scholar] [CrossRef]
- Castellucci, B.; Barrea, L.; Laudisio, D.; Aprano, S.; Pugliese, G.; Savastano, S.; Colao, A.; Muscogiuri, G. Improving Sleep Disturbances in Obesity by Nutritional Strategies: Review of Current Evidence and Practical Guide. Int. J. Food Sci. Nutr. 2021, 72, 579–591. [Google Scholar] [CrossRef]
- Zuraikat, F.M.; Wood, R.A.; Barragán, R.; St-Onge, M.-P. Sleep and Diet: Mounting Evidence of a Cyclical Relationship. Annu. Rev. Nutr. 2021, 41, 309–332. [Google Scholar] [CrossRef]
- Binks, H.; Vincent, G.E.; Gupta, C.; Irwin, C.; Khalesi, S. Effects of Diet on Sleep: A Narrative Review. Nutrients 2020, 12, 936. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Paragraph | Keywords | Total Number of Articles Found | Relevant Articles (Fully Read) |
|---|---|---|---|
| Sleep disturbances in pediatric obesity | “pediatric obesity” AND “sleep” OR “sleep disorders” OR “sleep apnea syndrome” | 242 | 133 (36) |
| Diet and Sleep | “children” OR “adolescents” AND “sleep” AND “diet” OR “food” | 214 | 83 (25) |
| Food intake and sleep disorders in children and adolescents with obesity | “pediatric obesity” AND “food intake” AND “sleep” OR “sleep disorders” | 243 | 97 (32) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calcaterra, V.; Rossi, V.; Tagi, V.M.; Baldassarre, P.; Grazi, R.; Taranto, S.; Zuccotti, G. Food Intake and Sleep Disorders in Children and Adolescents with Obesity. Nutrients 2023, 15, 4736. https://doi.org/10.3390/nu15224736
Calcaterra V, Rossi V, Tagi VM, Baldassarre P, Grazi R, Taranto S, Zuccotti G. Food Intake and Sleep Disorders in Children and Adolescents with Obesity. Nutrients. 2023; 15(22):4736. https://doi.org/10.3390/nu15224736
Chicago/Turabian StyleCalcaterra, Valeria, Virginia Rossi, Veronica Maria Tagi, Paola Baldassarre, Roberta Grazi, Silvia Taranto, and Gianvincenzo Zuccotti. 2023. "Food Intake and Sleep Disorders in Children and Adolescents with Obesity" Nutrients 15, no. 22: 4736. https://doi.org/10.3390/nu15224736
APA StyleCalcaterra, V., Rossi, V., Tagi, V. M., Baldassarre, P., Grazi, R., Taranto, S., & Zuccotti, G. (2023). Food Intake and Sleep Disorders in Children and Adolescents with Obesity. Nutrients, 15(22), 4736. https://doi.org/10.3390/nu15224736