Figure 1.
The process of selecting matched pairs for the study.
Figure 1.
The process of selecting matched pairs for the study.
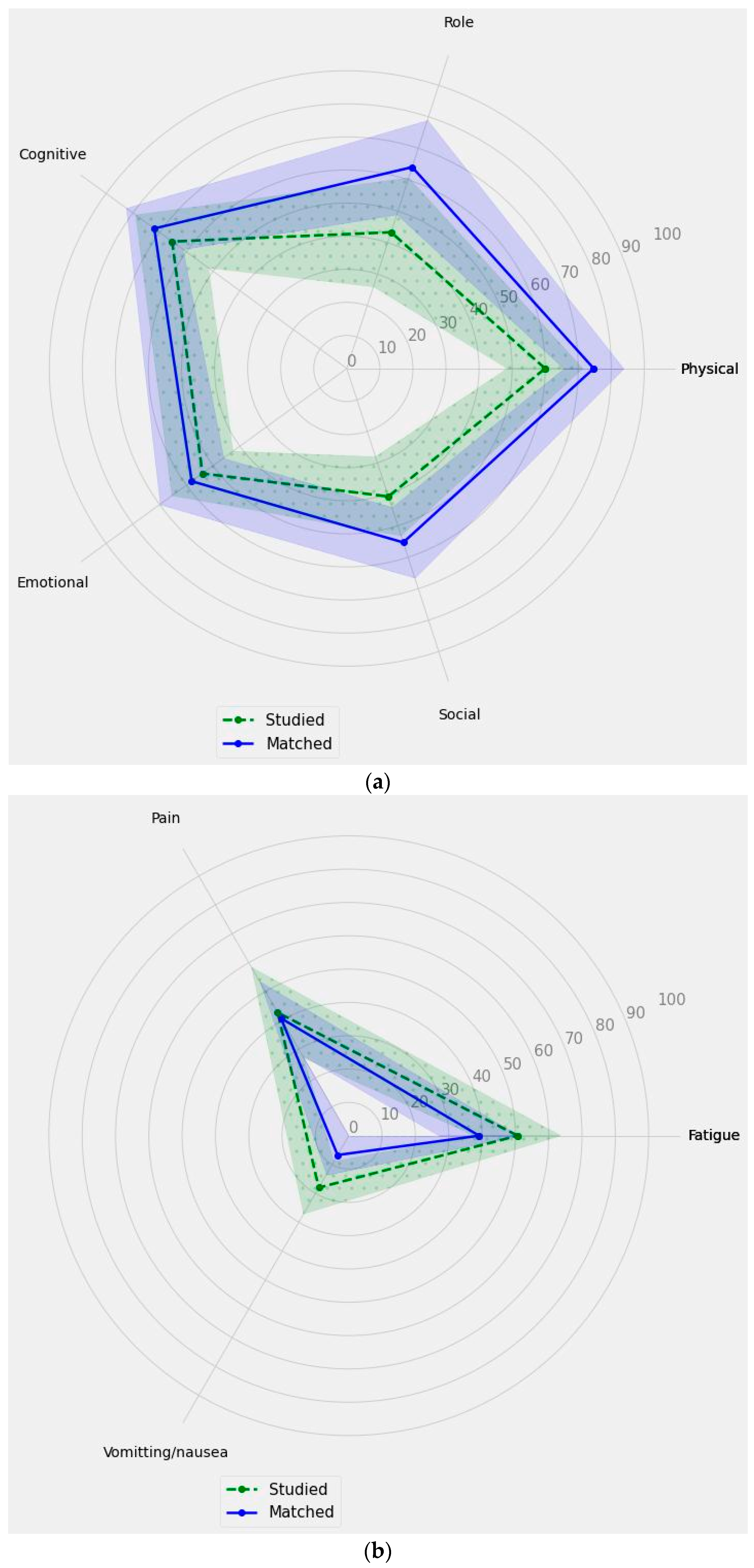
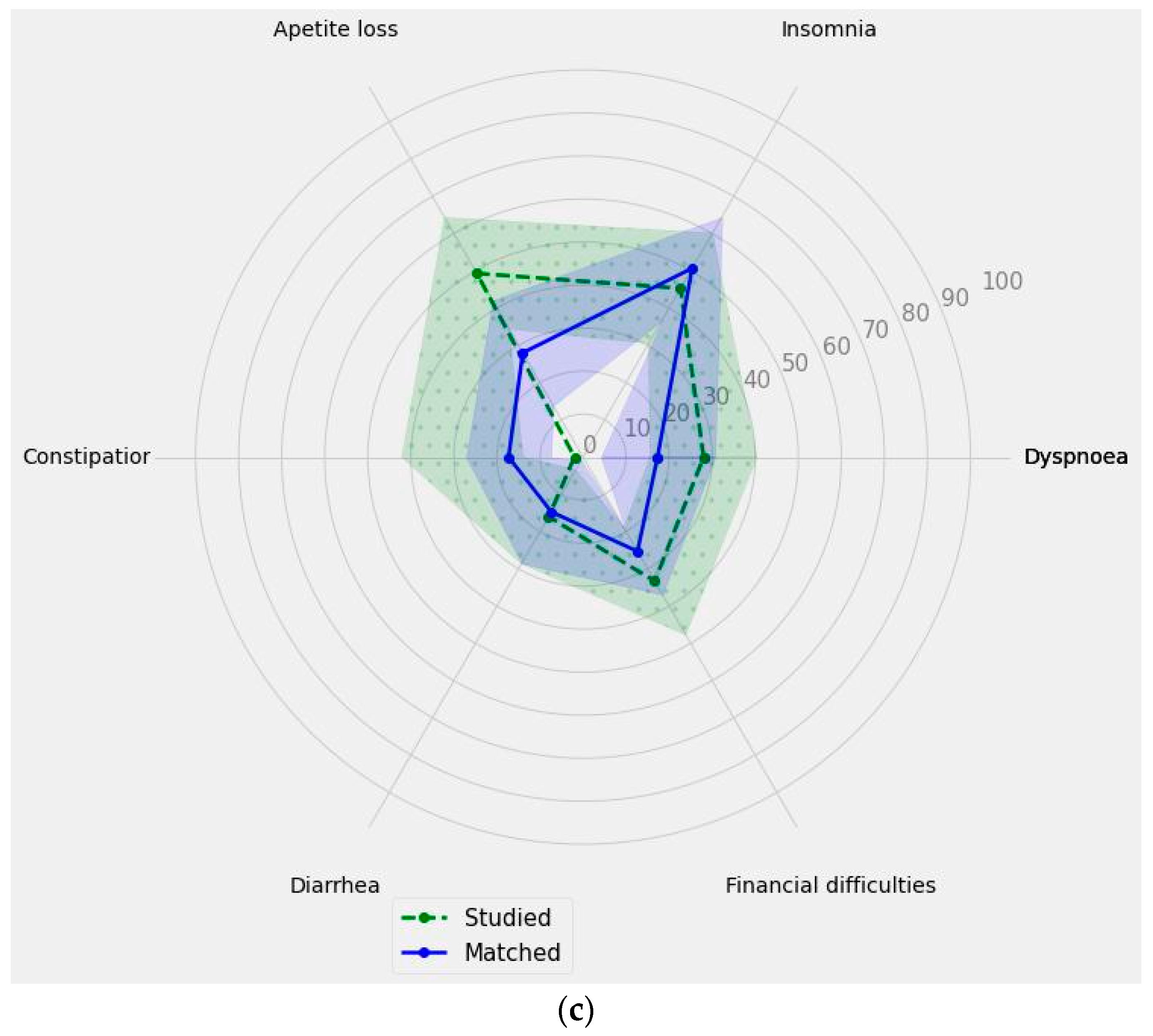
Figure 2.
The comparison of the main subscales’ measurements of the EORTC QLQ C30 for the studied group and matched group. The solid line represents the results obtained in points for individual subscales within the matched group, while the dashed line corresponds to the results obtained in points for individual subscales within the study group. The shaded areas indicate the confidence intervals (CIs): (a) functional scales; (b) symptom scale; (c) single-items measures score.
Figure 2.
The comparison of the main subscales’ measurements of the EORTC QLQ C30 for the studied group and matched group. The solid line represents the results obtained in points for individual subscales within the matched group, while the dashed line corresponds to the results obtained in points for individual subscales within the study group. The shaded areas indicate the confidence intervals (CIs): (a) functional scales; (b) symptom scale; (c) single-items measures score.
Table 1.
The socio-demographic characteristics of patients stratified on studied group and matched group.
Table 1.
The socio-demographic characteristics of patients stratified on studied group and matched group.
| | Total | Studied Group | Matched Group | p |
|---|
| Gender | Male | 26 (52%) | 13 (52%) | 13 (52%) | 0.7773 * |
| Female | 24 (48%) | 12 (48%) | 12 (48%) |
| Level of education | Higher education | 15 (30%) | 5 (20%) | 10 (40%) | 0.6504 |
| Secondary education | 22 (44%) | 12 (48%) | 10 (40%) |
| Vocational education | 13 (26%) | 8 (32%) | 5 (20%) |
| Place of residence | Rural area | 23 (46%) | 11 (44%) | 12 (48%) | 0.4900 |
| Town with up to 20,000 inhabitants | 2 (4%) | 1 (4%) | 1 (4%) |
| City with 20,000 to 100,000 inhabitants | 9 (18%) | 7 (28%) | 2 (8%) |
| City with 100,000 to 500,000 inhabitants | 2 (4%) | 1 (4%) | 1 (4%) |
| City with over 500,000 inhabitants | 14 (28%) | 5 (20%) | 9 (36%) |
| Employment status | Employed full-time | 11 (22%) | 4 (16%) | 7 (28%) | 0.7608 |
| Employed part-time | 1 (2%) | 1 (4%) | 0 (0%) |
| Pension | 3 (6%) | 1 (4%) | 2 (8%) |
| Retirement | 29 (58%) | 14 (56%) | 15 (60%) |
| Unemployed | 6 (12%) | 5 (20%) | 1 (4%) |
| Economic status | Very good | 11 (22%) | 2 (8%) | 9 (36%) | 0.0323 |
| Good | 15 (30%) | 10 (40%) | 5 (20%) |
| Neither good nor bad | 13 (26%) | 9 (36%) | 4 (16%) |
| Bad | 5 (10%) | 4 (16%) | 1 (4%) |
| Very bad | 6 (12%) | 0 (0%) | 6 (24%) |
Table 2.
Age of patients stratified on studied group and matched group.
Table 2.
Age of patients stratified on studied group and matched group.
| | Mean (SD) | 95% CI | Median (IQR) | p |
|---|
| Total | 63.0 (11.8) | 59.64–66.36 | 65.5 (16.0) | |
| Studied group | 62.92 (12.02) | 58.19–67.97 | 66.0 (16.0) | 0.9690 |
| Matched group | 63.1 (11.83) | 57.96–67.88 | 64.0 (14.0) |
Table 3.
Descriptive statistics and scale reliability of the EORTC QLQ C30 compared to reference values for (1) all cancer patients and all stages of cancer [
20] and (2) Polish general population [
21].
Table 3.
Descriptive statistics and scale reliability of the EORTC QLQ C30 compared to reference values for (1) all cancer patients and all stages of cancer [
20] and (2) Polish general population [
21].
| Measures | Scale | Mean ± SD | Median (IQR) | 95%CI | (1) All Cancer Patients | (2) General Population |
|---|
| Functional scales | Physical | 67.33 ± 25.71 | 80 (40) | (60.03–74.64) | lower | lower |
| Role | 53.67 ± 40.17 | 66.67 (100) | (42.25–65.08) | lower | lower |
| Cognitive | 68.67 ± 29.48 | 83.33 (66.67) | (60.29–77.04) | lower | lower |
| Emotional | 56 ± 27.97 | 58.33 (41.67) | (48.05–63.95) | lower | lower |
| Social | 48 ± 29.48 | 50 (33.34) | (39.62–56.38) | lower | lower |
| Global health status | 39.67 ± 18.79 | 41.67 (25) | (34.33–45.01) | lower | lower |
| Symptom Scales | Fatigue | 44.89 ± 30.45 | 33.33 (33.34) | (36.24–53.54) | similar | higher |
| Pain | 41.67 ± 34.38 | 33.33 (50) | (31.9–51.44) | higher | higher |
| Vomiting/nausea | 12.33 ± 20.15 | 0 (16.67) | (6.61–18.06) | similar | higher |
| Single-item measures | Dyspnoea | 22.67 ± 31.18 | 0 (33.33) | (13.8–31.53) | similar | higher |
| Insomnia | 48 ± 34.44 | 33.33 (33.34) | (38.21–57.79) | similar | higher |
| Appetite loss | 38.67 ± 36.49 | 33.33 (66.67) | (28.3–49.04) | higher | higher |
| Constipation | 22.67 ± 29.69 | 0 (33.33) | (14.23–31.11) | similar | higher |
| Diarrhoea | 15.33 ± 31.74 | 0 (0) | (6.31–24.35) | similar | similar |
| Financial difficulties | 29.33 ± 31.33 | 33.33 (33.33) | (20.43–38.24) | higher | higher |
Table 4.
EORTC QLQ C30: Item-scale correlation matrix.
Table 4.
EORTC QLQ C30: Item-scale correlation matrix.
| | PF | RF | CF | EF | SF | F | P | VN | QoL |
|---|
| Physical functioning (PF) | - | | | | | | | | |
| Role functioning (RF) | 0.53 | - | | | | | | | |
| Cognitive functioning (CF) | 0.56 | 0.56 | - | | | | | | |
| Emotional functioning (EF) | 0.37 | 0.49 | 0.70 | - | | | | | |
| Social functioning (SF) | 0.41 | 0.64 | 0.46 | 0.57 | - | | | | |
| Fatigue (F) | −0.47 | −0.72 | −0.63 | −0.60 | −0.61 | - | | | |
| Pain (P) | −0.53 | −0.48 | −0.62 | −0.49 | −0.54 | 0.62 | - | | |
| Vomiting/nausea (VN) | −0.33 | −0.40 | −0.48 | −0.32 | −0.43 | 0.45 | 0.23 | - | |
| Global health status (QoL) | 0.50 | 0.44 | 0.49 | 0.38 | 0.56 | −0.50 | −0.37 | −0.29 | - |
Table 5.
Results of the stepwise multiple regression analysis for physical scale of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
Table 5.
Results of the stepwise multiple regression analysis for physical scale of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
| | Unstandardized Coefficients | Standardized Coefficients β | p |
|---|
| β | SE |
|---|
| Constant | | | 1.0780 | <0.0001 |
| Weight loss of patients | 0.4195 | 0.1284 | 0.0247 | 0.0020 |
| Economic situation | 0.2795 | 0.1284 | 0.1047 | 0.0345 |
Table 6.
Results of the stepwise multiple regression analysis for emotional scale of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
Table 6.
Results of the stepwise multiple regression analysis for emotional scale of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
| | Unstandardized Coefficients | Standardized Coefficients β | p |
|---|
| β | SE |
|---|
| Constant | | | 2.4912 | <0.0001 |
| Age | −0.3227 | 0.1366 | −0.0129 | 0.0223 |
Table 7.
Results of the stepwise multiple regression analysis for vomiting/nausea scale of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
Table 7.
Results of the stepwise multiple regression analysis for vomiting/nausea scale of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
| | Unstandardized Coefficients | Standardized Coefficients β | p |
|---|
| β | SE |
|---|
| Constant | | | 1.1600 | <0.0001 |
| Type of group (studied/matched) | 0.3333 | 0.1361 | 0.3200 | 0.0180 |
Table 8.
Results of the stepwise multiple regression analysis for dyspnoea scale of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
Table 8.
Results of the stepwise multiple regression analysis for dyspnoea scale of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
| | Unstandardized Coefficients | Standardized Coefficients β | p |
|---|
| β | SE |
|---|
| Constant | | | 1.1600 | <0.0001 |
| Type of group (studied/matched) | 0.2837 | 0.1384 | 0.2800 | 0.0459 |
Table 9.
Results of the stepwise multiple regression analysis for insomnia scale of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
Table 9.
Results of the stepwise multiple regression analysis for insomnia scale of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
| | Unstandardized Coefficients | Standardized Coefficients β | p |
|---|
| β | SE |
|---|
| Constant | | | 0.5286 | 0.0963 |
| Age | 0.3097 | 0.1372 | 0.0110 | 0.0286 |
Table 10.
Results of the stepwise multiple regression analysis for appetite loss scale in of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
Table 10.
Results of the stepwise multiple regression analysis for appetite loss scale in of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
| | Unstandardized Coefficients | Standardized Coefficients β | p |
|---|
| β | SE |
|---|
| Constant | | | 1.5804 | <0.0001 |
| Weight loss of patients | −0.2945 | 0.1379 | −0.0176 | 0.0379 |
Table 11.
Results of the stepwise multiple regression analysis for constipation scale of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
Table 11.
Results of the stepwise multiple regression analysis for constipation scale of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
| | Unstandardized Coefficients | Standardized Coefficients β | p |
|---|
| β | SE |
|---|
| Constant | | | 1.2930 | <0.0001 |
| Weight loss of patients | 0.3450 | 0.1355 | 0.0213 | 0.0141 |
Table 12.
Results of the stepwise multiple regression analysis for diarrhoea scale of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
Table 12.
Results of the stepwise multiple regression analysis for diarrhoea scale of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
| | Unstandardized Coefficients | Standardized Coefficients β | p |
|---|
| β | SE |
|---|
| Constant | | | 1.4427 | <0.0001 |
| Education level | 0.2833 | 0.1384 | 0.1619 | 0.0462 |
Table 13.
Results of the stepwise multiple regression analysis for financial difficulties scale of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
Table 13.
Results of the stepwise multiple regression analysis for financial difficulties scale of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
| | Unstandardized Coefficients | Standardized Coefficients β | p |
|---|
| β | SE |
|---|
| Constant | | | 1.7250 | <0.0001 |
| Economic situation | −0.3227 | 0.1366 | −0.1250 | 0.0223 |
Table 14.
Results of the stepwise multiple regression analysis for Global Health Status (QoL) of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
Table 14.
Results of the stepwise multiple regression analysis for Global Health Status (QoL) of EORTC QLQ C30 in a model including type of group (studied or matched group), gender, age, body mass index, place of residence, level of education, employment status, economic situation, and weight loss of patients as variables within the population of combined studied and matched groups (n = 50).
| | Unstandardized Coefficients | Standardized Coefficients β | p |
|---|
| β | SE |
|---|
| Constant | | | 0.2306 | 0.4754 |
| Functional scales—Emotional functioning | 0.3192 | 0.1208 | 0.2224 | 0.0113 |
| Functional scales—Social functioning | 0.3490 | 0.1218 | 0.2835 | 0.0063 |
| Functional scales—Physical functioning | 0.3867 | 0.1220 | 0.2653 | 0.0027 |
| Symptom scales—Vomiting/nausea | 0.2928 | 0.1264 | 0.1983 | 0.0251 |



 ,
, 






{kind=link}
{kind=link}
{kind=link}